

Administration of Warfarin Inhibits the Development of Cerulein-Induced Edematous Acute Pancreatitis in Rats


 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals and Treatment
- (1)
- Saline-treated control rats without induction of AP (Control—C);
- (2)
- Rats without induction of AP pretreated with warfarin administered at a dose of 90 µg/kg/dose (WF 90 + Saline);
- (3)
- Rats without induction of AP pretreated with warfarin administered at a dose of 180 µg/kg/dose (WF 180 + Saline);
- (4)
- Rats without induction of AP pretreated with warfarin administered at a dose of 270 µg/kg/dose (WF 270 + Saline);
- (5)
- Rats with cerulein-induced AP pretreated with saline (Saline + CIAP);
- (6)
- Rats pretreated with warfarin administered at a dose of 90 µg/kg/dose before induction of cerulein-induced AP (WF 90 + CIAP);
- (7)
- Rats pretreated with warfarin administered at a dose of 180 µg/kg/dose before induction of cerulein-induced AP (WF 180 + CIAP);
- (8)
- Rats pretreated with warfarin administered at a dose of 270 µg/kg/dose before induction of cerulein-induced AP (WF 270 + CIAP).
2.2. Measurement of the Pancreatic Blood Flow
2.3. Biochemical Analysis
2.4. Measurement of the Pancreatic Weight and Pancreatic Histology
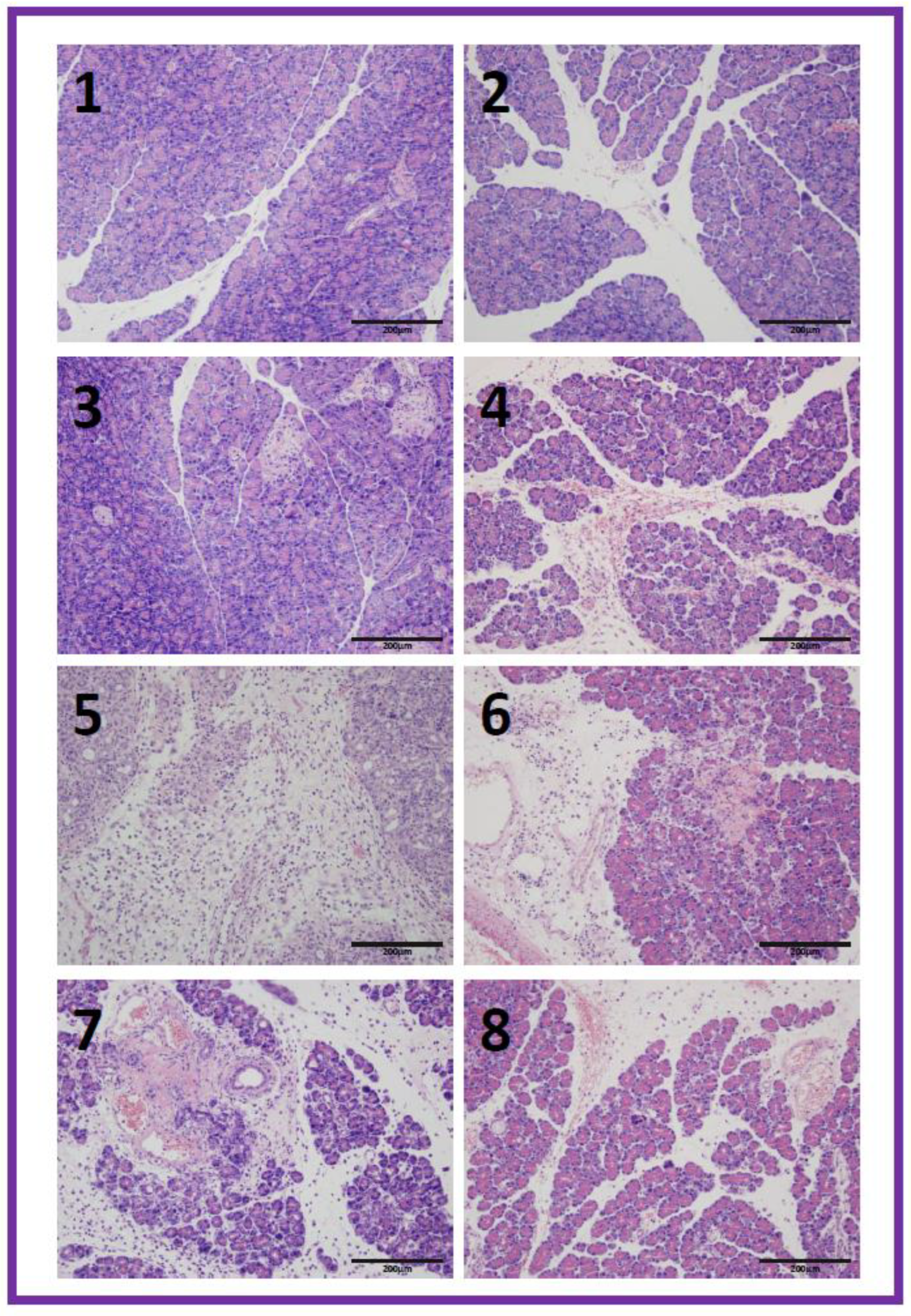
- Pancreatic edema: 0 = no edema, 1 = interlobular edema, 2 = interlobular and moderate intralobular edema, and 3 = severe interlobular and intralobular edema.
- Hemorrhages: 0 = absent, 1 = from one to two foci per slide, 2 = from three to five foci per slide, and 3 = more than five foci per slide.
- Leukocyte infiltration: 0 = absent, 1 = scarce perivascular infiltration, 2 = moderate perivascular and scarce diffuse infiltration, and 3 = abundant diffuse infiltration.
- Acinar necrosis: 0 = absent, 1 = less than 15% of cells involved, 2 = from 15% to 35% of cells involved, and 3 = more than 35% of cells involved.
- Vacuolization of acinar cells: 0 = absent, 1 = less than 25%, 2 = 25–50%, and 3 = more than 50%.
2.5. Statistical Analysis
3. Results
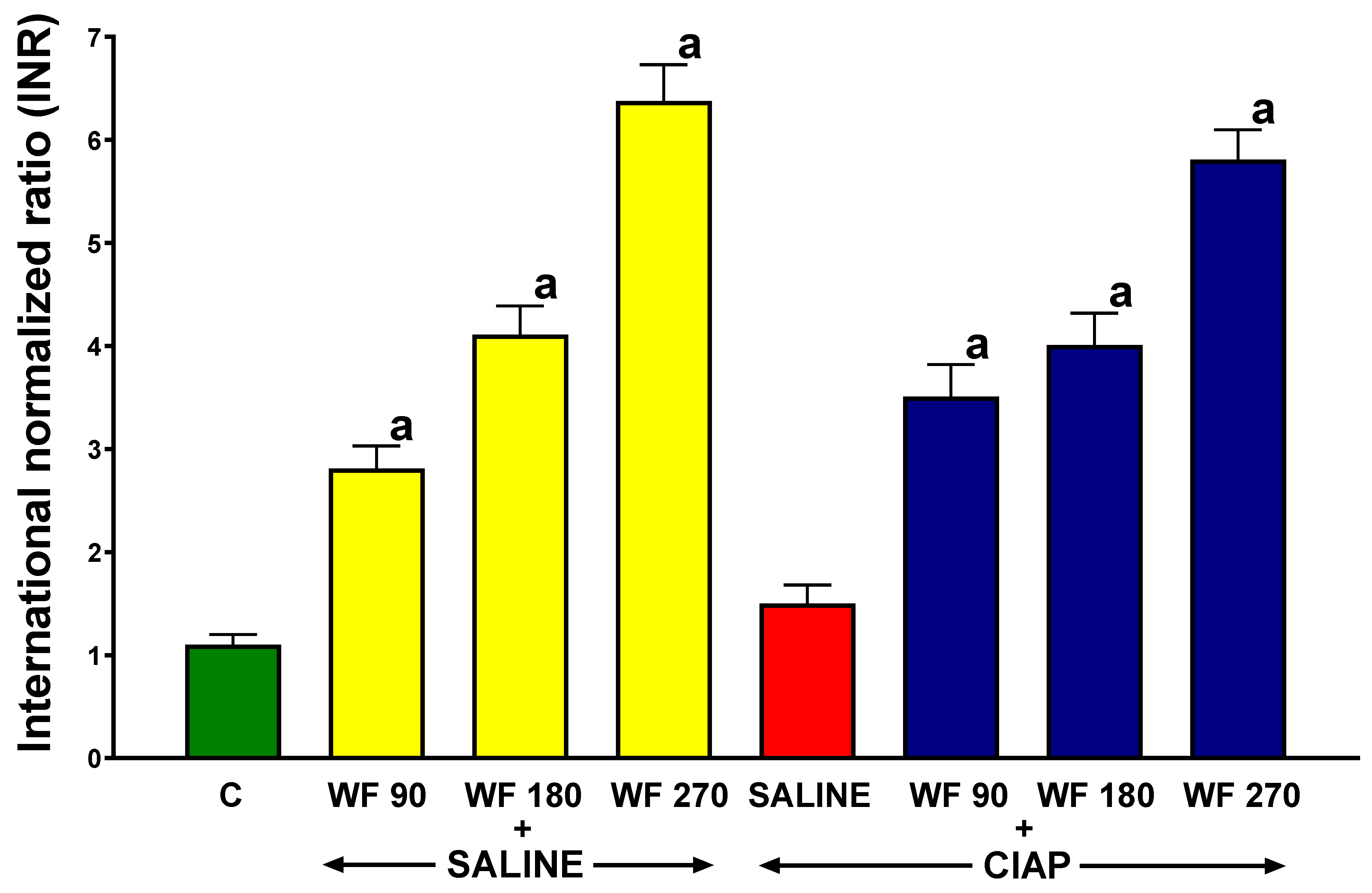
3.1. International Normalized Ratio
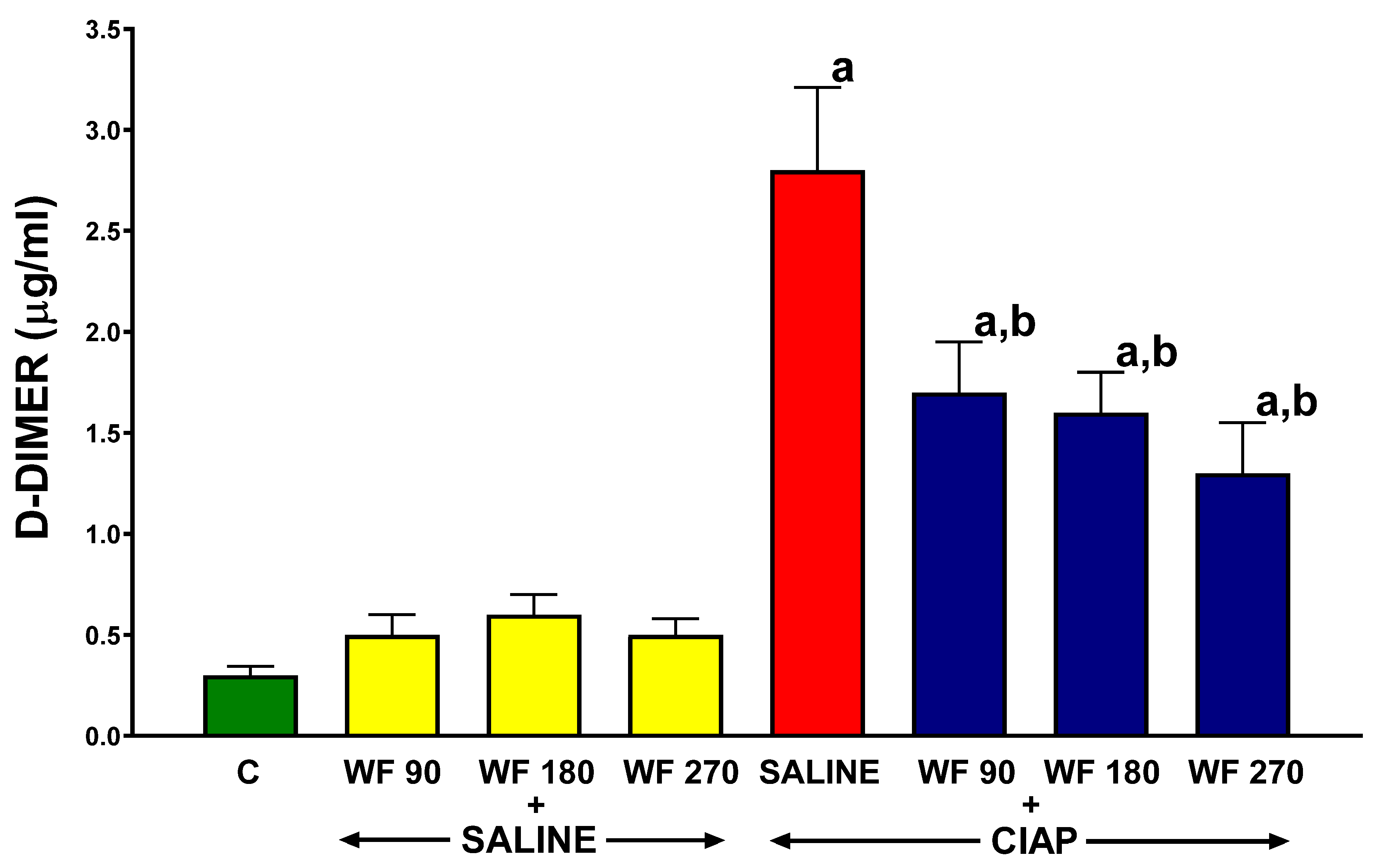
3.2. Serum Concentration of D-Dimer
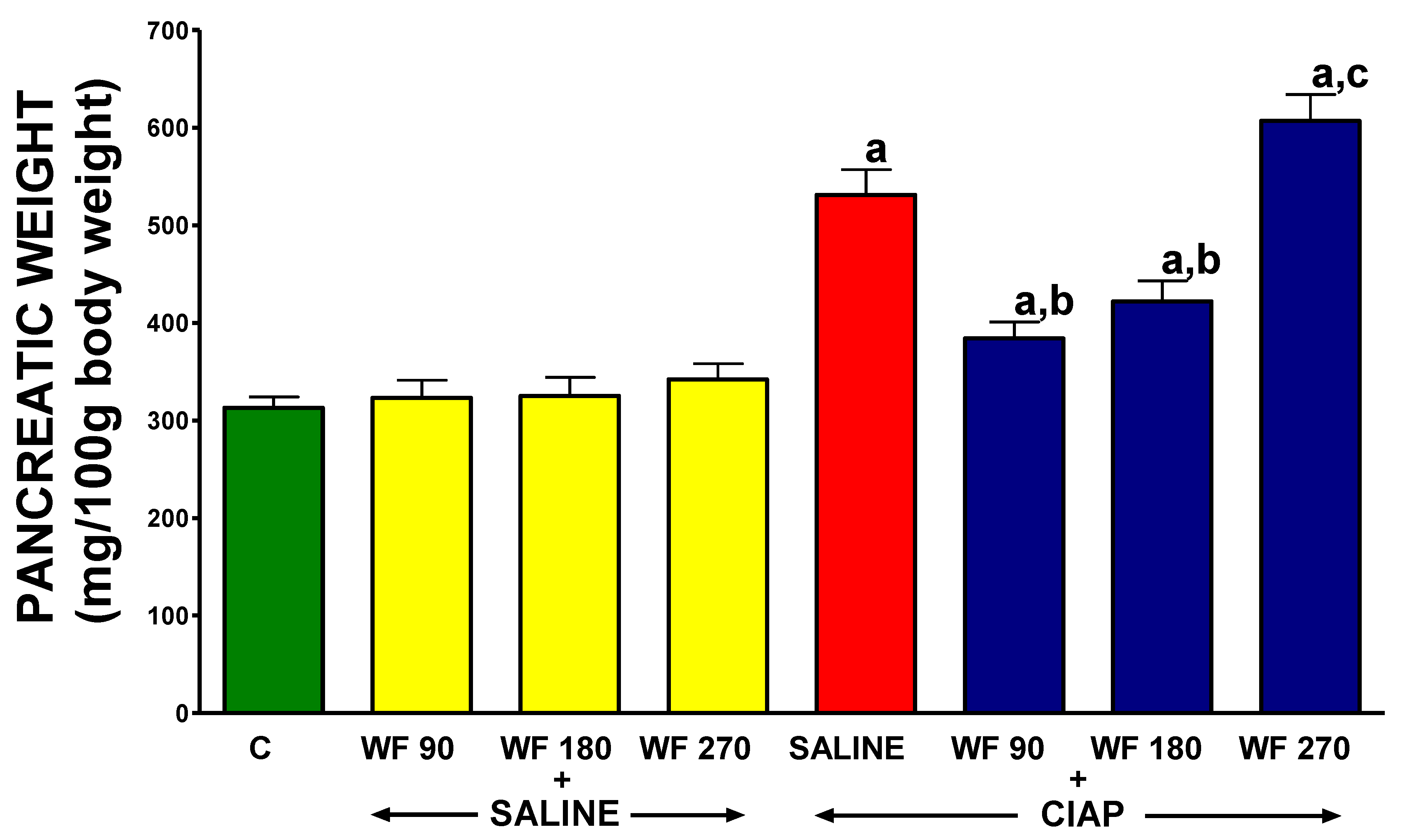
3.3. Pancreatic Weight
3.4. Histological Examination
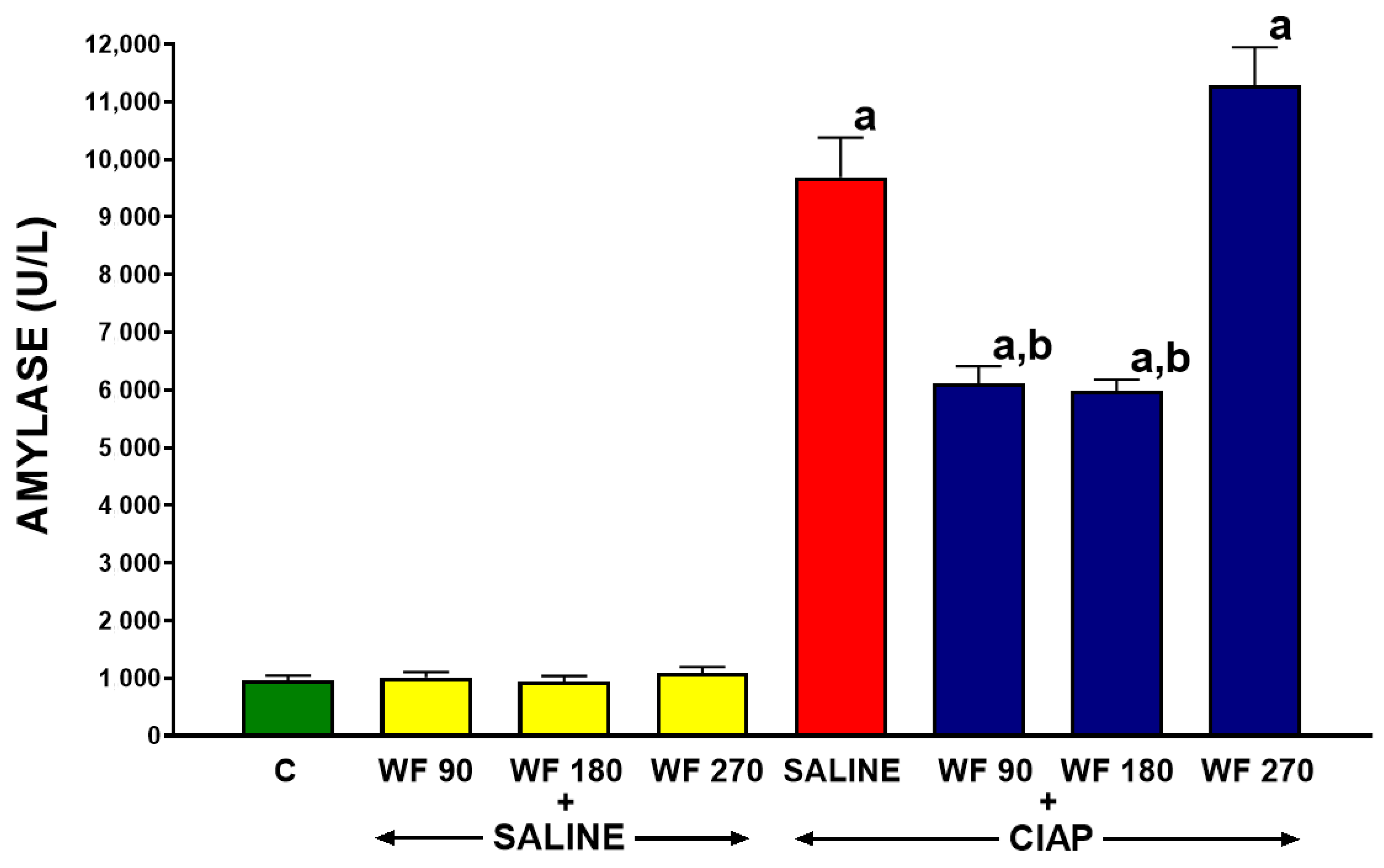
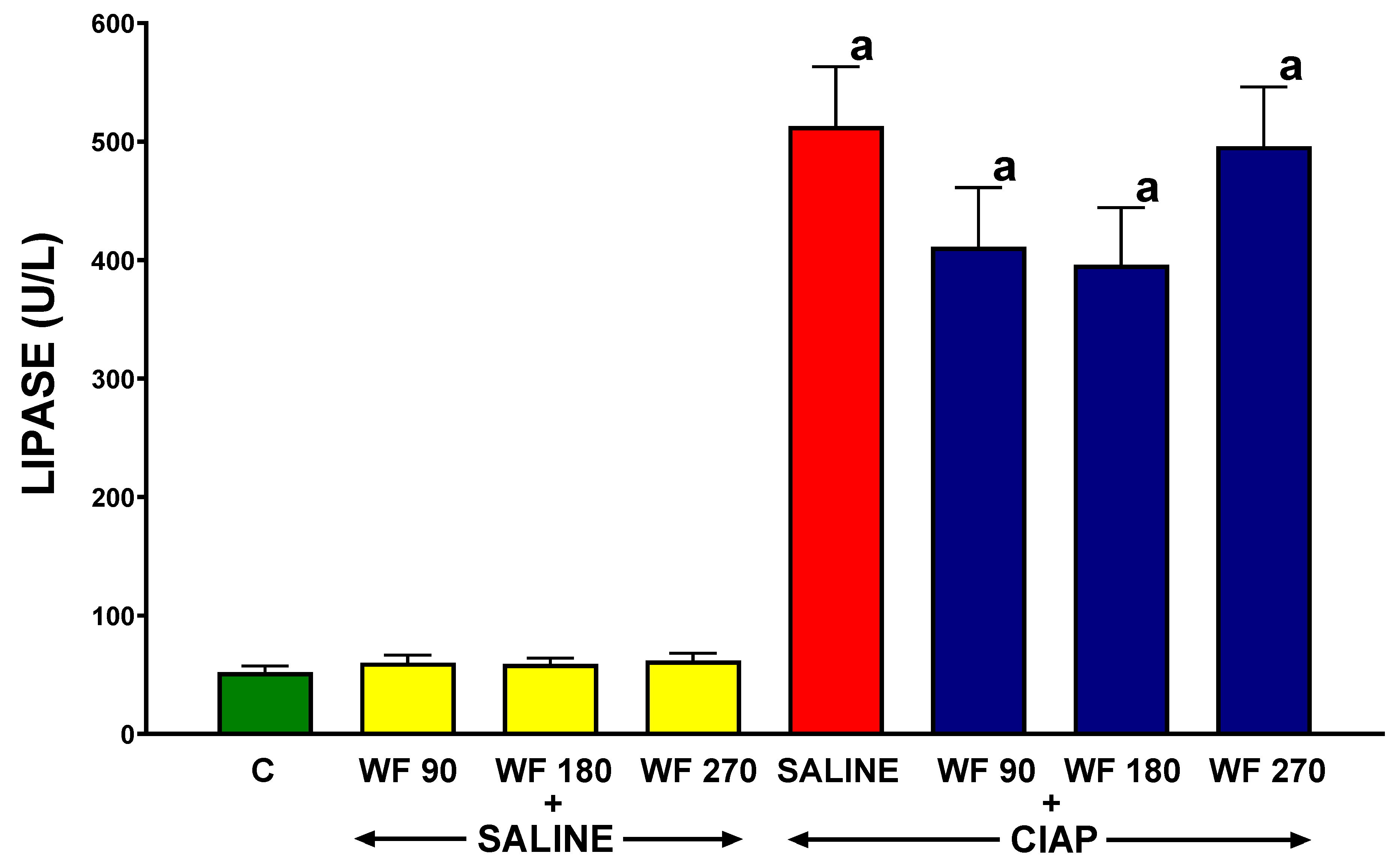
3.5. Serum Activity of Pancreatic Enzymes
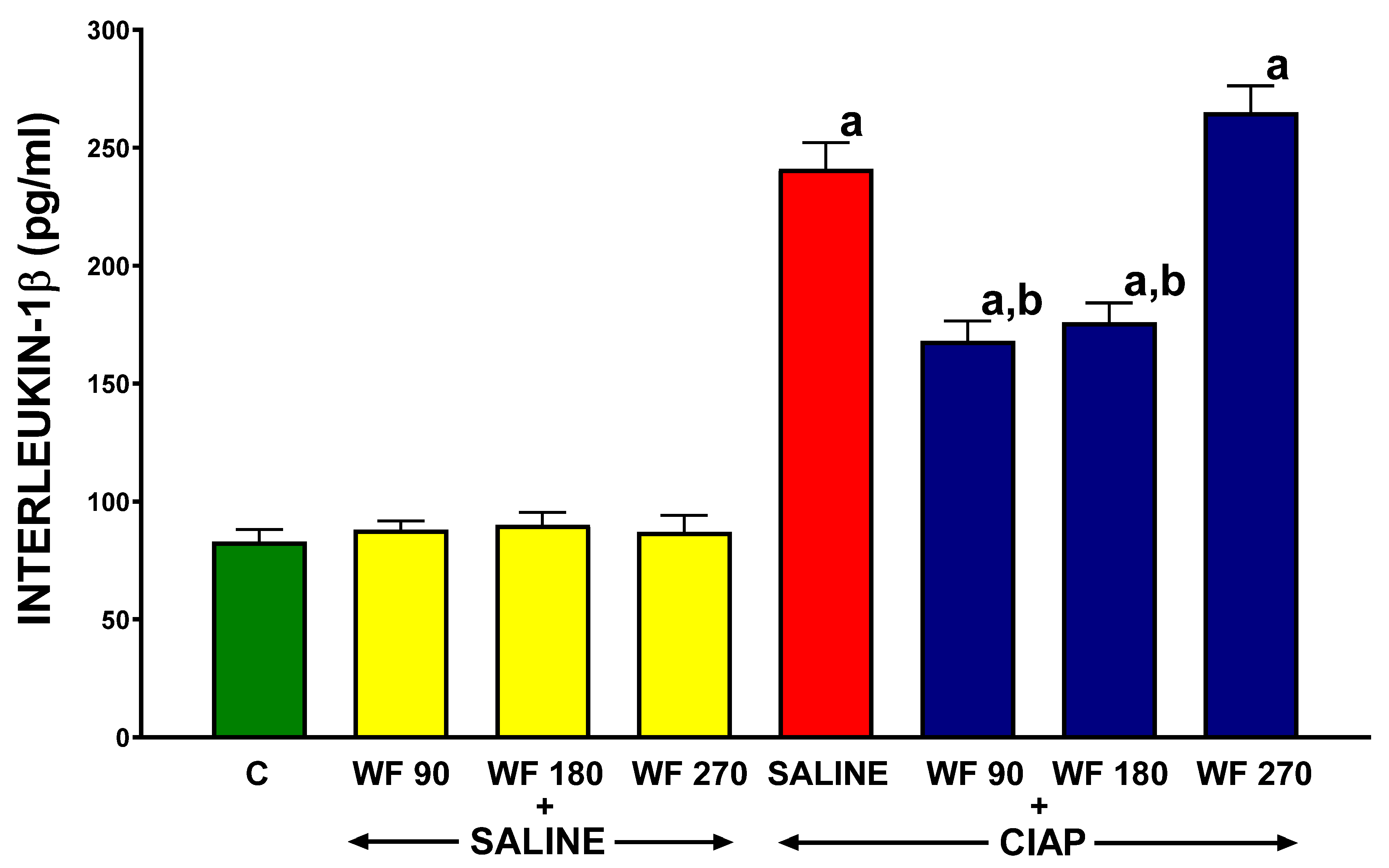
3.6. Serum Concentration of Interleukin-1β
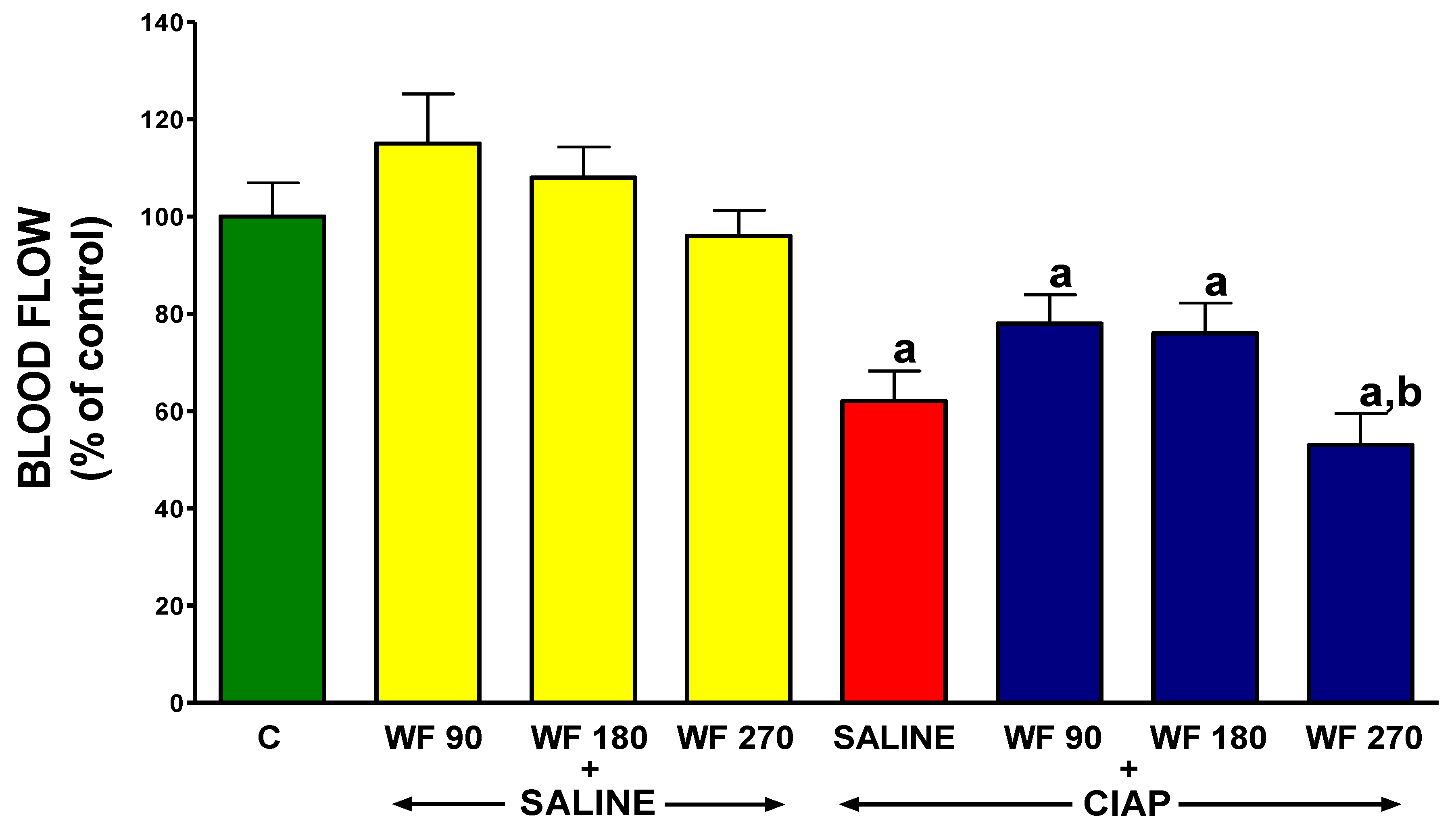
3.7. Pancreatic Blood Flow
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sinha, A.; Ma, Y.; Scherzer, R.; Hur, S.; Li, D.; Ganz, P.; Deeks, S.G.; Hsue, P.Y. Role of T-Cell Dysfunction, Inflammation, and Coagulation in Microvascular Disease in HIV. J. Am. Heart Assoc. Cardiovasc. Cerebrovasc. Dis. 2016, 5, e004243. [Google Scholar] [CrossRef]
- Lazzaroni, M.G.; Piantoni, S.; Masneri, S.; Garrafa, E.; Martini, G.; Tincani, A.; Andreoli, L.; Franceschini, F. Coagulation Dysfunction in COVID-19: The Interplay between Inflammation, Viral Infection and the Coagulation System. Blood Rev. 2020, 46, 100745. [Google Scholar] [CrossRef]
- Magro, G. COVID-19: Review on Latest Available Drugs and Therapies against SARS-CoV-2. Coagulation and Inflammation Cross-Talking. Virus Res. 2020, 286, 198070. [Google Scholar] [CrossRef]
- Panova-Noeva, M.; Schulz, A.; Arnold, N.; Hermanns, M.I.; Prochaska, J.H.; Laubert-Reh, D.; Spronk, H.M.; Blettner, M.; Beutel, M.; Pfeiffer, N.; et al. Coagulation and Inflammation in Long-Term Cancer Survivors: Results from the Adult Population. J. Thromb. Haemost. 2018, 16, 699–708. [Google Scholar] [CrossRef] [Green Version]
- Danese, S.; Papa, A.; Saibeni, S.; Repici, A.; Malesci, A.; Vecchi, M. Inflammation and Coagulation in Inflammatory Bowel Disease: The Clot Thickens. Am. J. Gastroenterol. 2007, 102, 174–186. [Google Scholar] [CrossRef]
- Dumnicka, P.; Maduzia, D.; Ceranowicz, P.; Olszanecki, R.; Drożdż, R.; Kuśnierz-Cabala, B. The Interplay between Inflammation, Coagulation and Endothelial Injury in the Early Phase of Acute Pancreatitis: Clinical Implications. Int. J. Mol. Sci. 2017, 18, 354. [Google Scholar] [CrossRef] [Green Version]
- Levi, M.; van der Poll, T. Inflammation and Coagulation. Crit. Care Med. 2010, 38, S26–S34. [Google Scholar] [CrossRef]
- Esmon, C.T. The Interactions between Inflammation and Coagulation. Br. J. Haematol. 2005, 131, 417–430. [Google Scholar] [CrossRef]
- Esmon, C.T. Crosstalk between Inflammation and Thrombosis. Maturitas 2008, 61, 122–131. [Google Scholar] [CrossRef]
- Esmon, C.T. Possible Involvement of Cytokines in Diffuse Intravascular Coagulation and Thrombosis. Baillieres Best Pract. Res. Clin. Haematol. 1999, 12, 343–359. [Google Scholar] [CrossRef]
- Levi, M.; van der Poll, T.; Schultz, M. New Insights into Pathways That Determine the Link between Infection and Thrombosis. Neth. J. Med. 2012, 70, 114–120. [Google Scholar] [PubMed]
- Morrissey, J.H. Tissue Factor: An Enzyme Cofactor and a True Receptor. Thromb. Haemost. 2001, 86, 66–74. [Google Scholar] [CrossRef] [Green Version]
- Grover, S.P.; Mackman, N. Tissue Factor: An Essential Mediator of Hemostasis and Trigger of Thrombosis. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 709–725. [Google Scholar] [CrossRef] [Green Version]
- Levi, M.; Keller, T.T.; van Gorp, E.; ten Cate, H. Infection and Inflammation and the Coagulation System. Cardiovasc. Res. 2003, 60, 26–39. [Google Scholar] [CrossRef]
- Gando, S.; Levi, M.; Toh, C.-H. Disseminated Intravascular Coagulation. Nat. Rev. Dis. Primer 2016, 2, 16037. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; van der Poll, T. Coagulation and Sepsis. Thromb. Res. 2017, 149, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Bach Ronald, R. Tissue Factor Encryption. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 456–461. [Google Scholar] [CrossRef] [Green Version]
- Morrissey, J.H. Tissue Factor Interactions with Factor VII: Measurement and Clinical Significance of Factor VIIa in Plasma. Blood Coagul. Fibrinolysis 1995, 6, S14. [Google Scholar] [CrossRef]
- Danckwardt, S.; Hentze, M.W.; Kulozik, A.E. Pathologies at the Nexus of Blood Coagulation and Inflammation: Thrombin in Hemostasis, Cancer, and Beyond. J. Mol. Med. Berl. Ger. 2013, 91, 1257–1271. [Google Scholar] [CrossRef] [Green Version]
- Fang, X.; Liao, R.; Yu, Y.; Li, J.; Guo, Z.; Zhu, T. Thrombin Induces Secretion of Multiple Cytokines and Expression of Protease-Activated Receptors in Mouse Mast Cell Line. Mediat. Inflamm. 2019, 2019, 4952131. [Google Scholar] [CrossRef] [Green Version]
- Rezaie, A.R. Protease-Activated Receptor Signalling by Coagulation Proteases in Endothelial Cells. Thromb. Haemost. 2014, 112, 876–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.; Dorling, A. The Roles of Thrombin and Protease-Activated Receptors in Inflammation. Semin. Immunopathol. 2012, 34, 63–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, Y.; Nonoyama, S.; Morio, T.; Imai, K.; Ochs, H.D.; Mizutani, S. Characterization of Soluble CD40 Ligand Released from Human Activated Platelets. J. Med. Dent. Sci. 2001, 48, 23–27. [Google Scholar] [PubMed]
- Rizvi, M.; Pathak, D.; Freedman, J.E.; Chakrabarti, S. CD40-CD40 Ligand Interactions in Oxidative Stress, Inflammation and Vascular Disease. Trends Mol. Med. 2008, 14, 530–538. [Google Scholar] [CrossRef]
- Schönbeck, U.; Mach, F.; Libby, P. CD154 (CD40 Ligand). Int. J. Biochem. Cell Biol. 2000, 32, 687–693. [Google Scholar] [CrossRef]
- Feldman, B.F.; Attix, E.A.; Strombeck, D.R.; O’Neill, S. Biochemical and Coagulation Changes in a Canine Model of Acute Necrotizing Pancreatitis. Am. J. Vet. Res. 1981, 42, 805–809. [Google Scholar]
- Rydzewska, G.; Kosidlo, S.; Gabryelewicz, A.; Rydzewski, A. Tissue Plasminogen Activator, Plasminogen Activator Inhibitor, and Other Parameters of Fibrinolysis in the Early Stages of Taurocholate Acute Pancreatitis in Rats. Int. J. Pancreatol. Off. J. Int. Assoc. Pancreatol. 1992, 11, 161–168. [Google Scholar] [CrossRef]
- Lasson, A.; Ohlsson, K. Consumptive Coagulopathy, Fibrinolysis and Protease-Antiprotease Interactions during Acute Human Pancreatitis. Thromb. Res. 1986, 41, 167–183. [Google Scholar] [CrossRef]
- Maeda, K.; Hirota, M.; Ichihara, A.; Ohmuraya, M.; Hashimoto, D.; Sugita, H.; Takamori, H.; Kanemitsu, K.; Baba, H. Applicability of Disseminated Intravascular Coagulation Parameters in the Assessment of the Severity of Acute Pancreatitis. Pancreas 2006, 32, 87–92. [Google Scholar] [CrossRef]
- Domínguez-Muñoz, J.E.; Viedma, J.A.; Pérez-Mateo, M.; Carballo, F.; García Fe, M. Inflammatory Response in the Initial Phase of Acute Pancreatitis: Relationship to the Onset and Severity of the Disease. Rev. Esp. Enferm. Dig. Organo Of. Soc. Esp. Patol. Dig. 1995, 87, 225–246. [Google Scholar]
- Ranson, J.H.; Lackner, H.; Berman, I.R.; Schinella, R. The Relationship of Coagulation Factors to Clinical Complications of Acute Pancreatitis. Surgery 1977, 81, 502–511. [Google Scholar] [PubMed]
- Kakafika, A.; Papadopoulos, V.; Mimidis, K.; Mikhailidis, D.P. Coagulation, Platelets, and Acute Pancreatitis. Pancreas 2007, 34, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Hamada, S.; Masamune, A.; Kikuta, K.; Shimosegawa, T. Disseminated Intravascular Coagulation on Admission Predicts Complications and Poor Prognosis of Acute Pancreatitis: Analysis of the Nationwide Epidemiological Survey in Japan. Pancreas 2017, 46, e15. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Zhou, X.; Ling, L.; Chen, S.; Zhou, J. Prediction of Mortality and Organ Failure Based on Coagulation and Fibrinolysis Markers in Patients with Acute Pancreatitis: A Retrospective Study. Medicine 2019, 98, e15648. [Google Scholar] [CrossRef] [PubMed]
- Staubli, S.M.; Oertli, D.; Nebiker, C.A. Laboratory Markers Predicting Severity of Acute Pancreatitis. Crit. Rev. Clin. Lab. Sci. 2015, 52, 273–283. [Google Scholar] [CrossRef]
- Gurda-Duda, A.; Kuśnierz-Cabala, B.; Nowak, W.; Naskalski, J.W.; Kulig, J. Assessment of the Prognostic Value of Certain Acute-Phase Proteins and Procalcitonin in the Prognosis of Acute Pancreatitis. Pancreas 2008, 37, 449–453. [Google Scholar] [CrossRef]
- Bal Dit Sollier, C.; Dillinger, J.-G.; Drouet, L. Anticoagulant Activity and Pleiotropic Effects of Heparin. J. Med. Vasc. 2020, 45, 147–157. [Google Scholar] [CrossRef]
- Gabryelewicz, A.; Niewiarowski, S.; Prokopowicz, J.; Chlebowski, J. Heparin and Protease Inhibitors in the Prevention of Experimental Acute Pancreatic Necrosis in Dogs. Digestion 1969, 2, 7–16. [Google Scholar] [CrossRef]
- Dobosz, M.; Wajda, Z.; Hac, S.; Mysliwska, J.; Mionskowska, L.; Bryl, E.; Roszkiewicz, A.; Mysliwski, A. Heparin and Nitric Oxide Treatment in Experimental Acute Pancreatitis in Rats. Forum 1998, 8, 303–310. [Google Scholar]
- Ceranowicz, P.; Dembinski, A.; Warzecha, Z.; Dembinski, M.; Cieszkowski, J.; Rembisz, K.; Konturek, S.J.; Kusnierz-Cabala, B.; Tomaszewska, R.; Pawlik, W.W. Protective and Therapeutic Effect of Heparin in Acute Pancreatitis. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2008, 59 (Suppl. 4), 103–125. [Google Scholar]
- Rabenstein, T.; Roggenbuck, S.; Framke, B.; Martus, P.; Fischer, B.; Nusko, G.; Muehldorfer, S.; Hochberger, J.; Ell, C.; Hahn, E.G.; et al. Complications of Endoscopic Sphincterotomy: Can Heparin Prevent Acute Pancreatitis after ERCP? Gastrointest. Endosc. 2002, 55, 476–483. [Google Scholar] [CrossRef]
- Twilla, J.D.; Mancell, J. Hypertriglyceridemia-Induced Acute Pancreatitis Treated with Insulin and Heparin. Am. J. Health-Syst. Pharm. AJHP Off. J. Am. Soc. Health-Syst. Pharm. 2012, 69, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.; Peng, J.M.; Zhu, H.D.; Zhang, H.M.; Lu, B.; Li, Y.; Qian, J.M.; Yu, X.Z.; Yang, H. Continuous Intravenous Infusion of Insulin and Heparin vs Plasma Exchange in Hypertriglyceridemia-Induced Acute Pancreatitis. J. Dig. Dis. 2018, 19, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Qiu, F.; Lü, X.; Huang, Y. Effect of Low Molecular Weight Heparin on Pancreatic Micro-Circulation in Severe Acute Pancreatitis in a Rodent Model. Chin. Med. J. 2007, 120, 2260–2263. [Google Scholar] [CrossRef] [PubMed]
- Yamenel, L.; Mas, M.R.; Comert, B.; Isik, A.T.; Aydin, S.; Mas, N.; Deveci, S.; Ozyurt, M.; Tasci, I.; Unal, T. The Effect of Activated Protein C on Experimental Acute Necrotizing Pancreatitis. Crit. Care 2005, 9, R184–R190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, X.-S.; Qiu, F.; Li, J.-Q.; Fan, Q.-Q.; Zhou, R.-G.; Ai, Y.-H.; Zhang, K.-C.; Li, Y.-X. Low Molecular Weight Heparin in the Treatment of Severe Acute Pancreatitis: A Multiple Centre Prospective Clinical Study. Asian J. Surg. 2009, 32, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Tozlu, M.; Kayar, Y.; İnce, A.T.; Baysal, B.; Şentürk, H. Low Molecular Weight Heparin Treatment of Acute Moderate and Severe Pancreatitis: A Randomized, Controlled,Open-Label Study. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2019, 30, 81–87. [Google Scholar] [CrossRef]
- Eguchi, T.; Tsuji, Y.; Yamashita, H.; Fukuchi, T.; Kanamori, A.; Matsumoto, K.; Hasegawa, T.; Koizumi, A.; Kitada, R.; Tsujimae, M.; et al. Efficacy of Recombinant Human Soluble Thrombomodulin in Preventing Walled-off Necrosis in Severe Acute Pancreatitis Patients. Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 2015, 15, 485–490. [Google Scholar] [CrossRef] [Green Version]
- Lyseng-Williamson, K.A.; Perry, C.M. Drotrecogin Alfa (Activated). Drugs 2002, 62, 617–630; discussion 631–632. [Google Scholar] [CrossRef]
- Alsfasser, G.; Warshaw, A.L.; Thayer, S.P.; Antoniu, B.; Laposata, M.; Lewandrowski, K.B.; Fernández-del Castillo, C. Decreased Inflammation and Improved Survival with Recombinant Human Activated Protein C Treatment in Experimental Acute Pancreatitis. Arch. Surg. Chic. Ill 1960 2006, 141, 670–676; discussion 676–677. [Google Scholar] [CrossRef] [Green Version]
- Ping, C.; Yongping, Z.; Minmin, Q.; Weiyan, Y.; Yaozong, Y. Activated Protein C Improves the Severity of Severe Acute Pancreatitis via Up-Regulating the Expressions of Endothelial Cell Protein C Receptor and Thrombomodulin. Dig. Dis. Sci. 2010, 55, 1599–1609. [Google Scholar] [CrossRef] [PubMed]
- Pettilä, V.; Kyhälä, L.; Kylänpää, M.-L.; Leppäniemi, A.; Tallgren, M.; Markkola, A.; Puolakkainen, P.; Repo, H.; Kemppainen, E. APCAP--Activated Protein C in Acute Pancreatitis: A Double-Blind Randomized Human Pilot Trial. Crit. Care Lond. Engl. 2010, 14, R139. [Google Scholar] [CrossRef] [Green Version]
- Miranda, C.J.; Mason, J.M.; Babu, B.I.; Sheen, A.J.; Eddleston, J.M.; Parker, M.J.; Pemberton, P.; Siriwardena, A.K. Twenty-Four Hour Infusion of Human Recombinant Activated Protein C (Xigris) Early in Severe Acute Pancreatitis: The XIG-AP 1 Trial. Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 2015, 15, 635–641. [Google Scholar] [CrossRef] [PubMed]
- van Rijn, J.L.M.L.; Zwaal, R.F.A.; Hemker, H.C.; Rosing, J. Role of Accessory Components in the Activation of Vitamin K-Dependent Coagulation Factors. Pathophysiol. Haemost. Thromb. 1986, 16, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Warzecha, Z.; Sendur, P.; Ceranowicz, P.; Dembinski, M.; Cieszkowski, J.; Kusnierz-Cabala, B.; Tomaszewska, R.; Dembinski, A. Pretreatment with Low Doses of Acenocoumarol Inhibits the Development of Acute Ischemia/Reperfusion-Induced Pancreatitis. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2015, 66, 731–740. [Google Scholar]
- Warzecha, Z.; Sendur, P.; Ceranowicz, P.; Dembiński, M.; Cieszkowski, J.; Kuśnierz-Cabala, B.; Olszanecki, R.; Tomaszewska, R.; Ambroży, T.; Dembiński, A. Protective Effect of Pretreatment with Acenocoumarol in Cerulein-Induced Acute Pancreatitis. Int. J. Mol. Sci. 2016, 17, 1709. [Google Scholar] [CrossRef] [Green Version]
- Warzecha, Z.; Sendur, P.; Ceranowicz, P.; Cieszkowski, J.; Dembiński, M.; Sendur, R.; Bonior, J.; Jaworek, J.; Ambroży, T.; Olszanecki, R.; et al. Therapeutic Effect of Low Doses of Acenocoumarol in the Course of Ischemia/Reperfusion-Induced Acute Pancreatitis in Rats. Int. J. Mol. Sci. 2017, 18, 882. [Google Scholar] [CrossRef] [Green Version]
- Barcellona, D.; Vannini, M.L.; Fenu, L.; Balestrieri, C.; Marongiu, F. Warfarin or Acenocoumarol: Which Is Better in the Management of Oral Anticoagulants? Thromb. Haemost. 1998, 80, 899–902. [Google Scholar] [CrossRef]
- Maduzia, D.; Ceranowicz, P.; Cieszkowski, J.; Chmura, A.; Galazka, K.; Kusnierz-Cabala, B.; Warzecha, Z. Administration of Warfarin Accelerates the Recovery in Ischemia/Reperfusion-Induced Acute Pancreatitis. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2020, 71, 417–427. [Google Scholar] [CrossRef]
- Maduzia, D.; Ceranowicz, P.; Cieszkowski, J.; Gałązka, K.; Kuśnierz-Cabala, B.; Warzecha, Z. Pretreatment with Warfarin Attenuates the Development of Ischemia/Reperfusion-Induced Acute Pancreatitis in Rats. Mol. Basel Switz. 2020, 25, E2493. [Google Scholar] [CrossRef]
- Warzecha, Z.; Kownacki, P.; Ceranowicz, P.; Dembinski, M.; Cieszkowski, J.; Dembinski, A. Ghrelin Accelerates the Healing of Oral Ulcers in Non-Sialoadenectomized and Sialoadenectomized Rats. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2013, 64, 657–668. [Google Scholar]
- Konturek, S.J.; Szlachcic, A.; Dembinski, A.; Warzecha, Z.; Jaworek, J.; Stachura, J. Nitric Oxide in Pancreatic Secretion and Hormone-Induced Pancreatitis in Rats. Int. J. Pancreatol. Off. J. Int. Assoc. Pancreatol. 1994, 15, 19–28. [Google Scholar] [CrossRef]
- Dembiński, A.; Warzecha, Z.; Ceranowicz, P.; Tomaszewska, R.; Dembiński, M.; Pabiańczyk, M.; Stachura, J.; Konturek, S.J. Ischemic Preconditioning Reduces the Severity of Ischemia/Reperfusion-Induced Pancreatitis. Eur. J. Pharmacol. 2003, 473, 207–216. [Google Scholar] [CrossRef]
- Ceranowicz, P.; Cieszkowski, J.; Warzecha, Z.; Dembiński, A. Experimental models of acute pancreatitis. Postep. Hig. Med. Dosw. Online 2015, 69, 264–269. [Google Scholar] [CrossRef]
- Vollmar, B.; Menger, M.D. Microcirculatory Dysfunction in Acute Pancreatitis. A New Concept of Pathogenesis Involving Vasomotion-Associated Arteriolar Constriction and Dilation. Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 2003, 3, 181–190. [Google Scholar] [CrossRef]
- Panek, J.; Zasada, J.; Poźniczek, M. Microcirculatory disturbance in the course of acute pancreatitis. Przegl. Lek. 2007, 64, 435–437. [Google Scholar] [PubMed]
- Wang, X.; Liu, M.; Hu, W.; Cui, T.; Yu, X.; Liu, R.; Yin, C. Angiotensin-(1-7) Treatment Restores Pancreatic Microcirculation Profiles: A New Story in Acute Pancreatitis. Pancreas 2020, 49, 960–966. [Google Scholar] [CrossRef] [PubMed]
- Cuthbertson, C.M.; Christophi, C. Disturbances of the Microcirculation in Acute Pancreatitis. Br. J. Surg. 2006, 93, 518–530. [Google Scholar] [CrossRef]
- Komara, N.L.; Paragomi, P.; Greer, P.J.; Wilson, A.S.; Breze, C.; Papachristou, G.I.; Whitcomb, D.C. Severe Acute Pancreatitis: Capillary Permeability Model Linking Systemic Inflammation to Multiorgan Failure. Am. J. Physiol. Gastrointest. Liver Physiol. 2020, 319, G573–G583. [Google Scholar] [CrossRef]
- Ge, P.; Luo, Y.; Okoye, C.S.; Chen, H.; Liu, J.; Zhang, G.; Xu, C.; Chen, H. Intestinal Barrier Damage, Systemic Inflammatory Response Syndrome, and Acute Lung Injury: A Troublesome Trio for Acute Pancreatitis. Biomed. Pharmacother. Biomed. Pharmacother. 2020, 132, 110770. [Google Scholar] [CrossRef]
- Luo, Y.; Li, Z.; Ge, P.; Guo, H.; Li, L.; Zhang, G.; Xu, C.; Chen, H. Comprehensive Mechanism, Novel Markers and Multidisciplinary Treatment of Severe Acute Pancreatitis-Associated Cardiac Injury-A Narrative Review. J. Inflamm. Res. 2021, 14, 3145–3169. [Google Scholar] [CrossRef] [PubMed]
- Warzecha, Z.; Ceranowicz, P.; Dembinski, M.; Cieszkowski, J.; Ginter, G.; Ptak-Belowska, A.; Dembinski, A. Involvement of Cyclooxygenase-1 and Cyclooxygenase-2 Activity in the Therapeutic Effect of Ghrelin in the Course of Ethanol-Induced Gastric Ulcers in Rats. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2014, 65, 95–106. [Google Scholar]
- Ceranowicz, P.; Warzecha, Z.; Dembinski, A.; Sendur, R.; Cieszkowski, J.; Ceranowicz, D.; Pawlik, W.W.; Kuwahara, A.; Kato, I.; Konturek, P.C. Treatment with Ghrelin Accelerates the Healing of Acetic Acid-Induced Gastric and Duodenal Ulcers in Rats. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2009, 60, 87–98. [Google Scholar]
- Dembiński, A.; Warzecha, Z.; Ceranowicz, P.; Cieszkowski, J.; Dembiński, M.; Ptak-Belowska, A.; Kuwahara, A.; Kato, I. Administration of Obestatin Accelerates the Healing of Chronic Gastric Ulcers in Rats. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2011, 17, BR196–BR200. [Google Scholar] [CrossRef] [Green Version]
- Maduzia, D.; Matuszyk, A.; Ceranowicz, D.; Warzecha, Z.; Ceranowicz, P.; Fyderek, K.; Galazka, K.; Dembinski, A. The Influence of Pretreatment with Ghrelin on the Development of Acetic-Acid-Induced Colitis in Rats. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2015, 66, 875–885. [Google Scholar]
- Matuszyk, A.; Ceranowicz, D.; Warzecha, Z.; Ceranowicz, P.; Fyderek, K.; Gałązka, K.; Cieszkowski, J.; Bonior, J.; Jaworek, J.; Pihut, M.; et al. The Influence of Ghrelin on the Development of Dextran Sodium Sulfate-Induced Colitis in Rats. BioMed Res. Int. 2015, 2015, 718314. [Google Scholar] [CrossRef] [Green Version]
- Matuszyk, A.; Ceranowicz, P.; Warzecha, Z.; Cieszkowski, J.; Bonior, J.; Jaworek, J.; Kuśnierz-Cabala, B.; Konturek, P.; Ambroży, T.; Dembiński, A. Obestatin Accelerates the Healing of Acetic Acid-Induced Colitis in Rats. Oxid. Med. Cell. Longev. 2016, 2016, 2834386. [Google Scholar] [CrossRef] [Green Version]
- Ceranowicz, P.; Warzecha, Z.; Cieszkowski, J.; Ceranowicz, D.; Kuśnierz-Cabala, B.; Bonior, J.; Jaworek, J.; Ambroży, T.; Gil, K.; Olszanecki, R.; et al. Essential Role of Growth Hormone and IGF-1 in Therapeutic Effect of Ghrelin in the Course of Acetic Acid-Induced Colitis. Int. J. Mol. Sci. 2017, 18, 1118. [Google Scholar] [CrossRef] [Green Version]
- Dembiński, A.; Warzecha, Z.; Ceranowicz, P.; Dembiński, M.; Cieszkowski, J.; Gosiewski, T.; Bulanda, M.; Kuśnierz-Cabala, B.; Gałązka, K.; Konturek, P.C. Synergic Interaction of Rifaximin and Mutaflor (Escherichia Coli Nissle 1917) in the Treatment of Acetic Acid-Induced Colitis in Rats. Gastroenterol. Res. Pract. 2016, 2016, 3126280. [Google Scholar] [CrossRef] [Green Version]
- Warzecha, Z.; Dembiński, A.; Ceranowicz, P.; Dembiński, M.; Cieszkowski, J.; Kuśnierz-Cabala, B.; Naskalski, J.W.; Jaworek, J.; Konturek, S.J.; Pawlik, W.W.; et al. Influence of ischemic preconditioning on blood coagulation, fibrinolytic activity and pancreatic repair in the course of caerulein-induced acute pancreatitis in rats. J. Physiol. Pharmacol. 2007, 58, 303–319. [Google Scholar]
- Ceranowicz, P.; Dembińsk, M.; Warzecha, Z.; Cieszkowski, J.; Kuśnierz-Cabala, B.; Tomaszewska, R.; Dembiński, A. Healing Effect of Heparin in the Course of Acute Cerulein-Induced Pancreatitis. Gastroenterol. Rev. Gastroenterol. 2009, 4, 199–205. [Google Scholar]
- Vogel, A. Darstellung von Benzoesäure aus der Tonka-Bohne und aus den Meliloten-oder Steinklee-Blumen. Ann. Phys. 1820, 64, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Whitlon, D.S.; Sadowski, J.A.; Suttie, J.W. Mechanism of Coumarin Action: Significance of Vitamin K Epoxide Reductase Inhibition. Biochemistry 1978, 17, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Wittkowsky, A.K. Warfarin and Other Coumarin Derivatives: Pharmacokinetics, Pharmacodynamics, and Drug Interactions. Semin. Vasc. Med. 2003, 3, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Chen, X.; Jin, D.-Y.; Stafford, D.W.; Pedersen, L.G.; Tie, J.-K. Warfarin and Vitamin K Epoxide Reductase: A Molecular Accounting for Observed Inhibition. Blood 2018, 132, 647–657. [Google Scholar] [CrossRef] [Green Version]
- Undas, A.; Zabczyk, M. Antithrombotic Medications and Their Impact on Fibrin Clot Structure and Function. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2018, 69. [Google Scholar] [CrossRef]
- Johnson, J.A.; Cavallari, L.H. Warfarin Pharmacogenetics. Trends Cardiovasc. Med. 2015, 25, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Oliva Berini, E.; Galán Alvarez, P.; Pacheco Onrubia, A.M. Comparison of quality and hemorragic risk of oral anticoagulant therapy using acenocoumarol versus warfarin. Med. Clin. 2008, 131, 96–97. [Google Scholar] [CrossRef]
- Menichelli, D.; Poli, D.; Antonucci, E.; Cammisotto, V.; Testa, S.; Pignatelli, P.; Palareti, G.; Pastori, D. The Italian Federation Of Anticoagulation Clinics Fcsa, null Comparison of Anticoagulation Quality between Acenocoumarol and Warfarin in Patients with Mechanical Prosthetic Heart Valves: Insights from the Nationwide PLECTRUM Study. Mol. Basel Switz. 2021, 26, 1425. [Google Scholar] [CrossRef]
- Ismail, O.Z.; Bhayana, V. Lipase or Amylase for the Diagnosis of Acute Pancreatitis? Clin. Biochem. 2017, 50, 1275–1280. [Google Scholar] [CrossRef]
- Leppäniemi, A.; Tolonen, M.; Tarasconi, A.; Segovia-Lohse, H.; Gamberini, E.; Kirkpatrick, A.W.; Ball, C.G.; Parry, N.; Sartelli, M.; Wolbrink, D.; et al. 2019 WSES Guidelines for the Management of Severe Acute Pancreatitis. World J. Emerg. Surg. WJES 2019, 14, 27. [Google Scholar] [CrossRef]
- Keck, T.; Friebe, V.; Warshaw, A.L.; Antoniu, B.A.; Waneck, G.; Benz, S.; Hopt, U.T.; Fernández-del-Castillo, C. Pancreatic Proteases in Serum Induce Leukocyte-Endothelial Adhesion and Pancreatic Microcirculatory Failure. Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 2005, 5, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Baczyńska, A. Doustne leki przeciwkrzepliwe w różnych stanach klinicznych–praktyczny poradnik. Chor. Serca I Naczyń 2004, 1, 27–36. Available online: https://journals.viamedica.pl/choroby_serca_i_naczyn/article/view/12239 (accessed on 2 October 2021).
- Osman, M.O.; Lausten, S.B.; Jakobsen, N.O.; Kristensen, J.U.; Deleuran, B.; Larsen, C.G.; Jensen, S.L. Graded Experimental Acute Pancreatitis: Monitoring of a Renewed Rabbit Model Focusing on the Production of Interleukin-8 (IL-8) and CD11b/CD18. Eur. J. Gastroenterol. Hepatol. 1999, 11, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Vonlaufen, A.; Apte, M.V.; Imhof, B.A.; Frossard, J.L. The Role of Inflammatory and Parenchymal Cells in Acute Pancreatitis. J. Pathol. 2007, 213, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Grady, T.; Liang, P.; Ernst, S.A.; Logsdon, C.D. Chemokine Gene Expression in Rat Pancreatic Acinar Cells Is an Early Event Associated with Acute Pancreatitis. Gastroenterology 1997, 113, 1966–1975. [Google Scholar] [CrossRef]
- Gukovskaya, A.S.; Gukovsky, I.; Zaninovic, V.; Song, M.; Sandoval, D.; Gukovsky, S.; Pandol, S.J. Pancreatic Acinar Cells Produce, Release, and Respond to Tumor Necrosis Factor-Alpha. Role in Regulating Cell Death and Pancreatitis. J. Clin. Investig. 1997, 100, 1853–1862. [Google Scholar] [CrossRef] [Green Version]
- Gu, H.; Werner, J.; Bergmann, F.; Whitcomb, D.C.; Büchler, M.W.; Fortunato, F. Necro-Inflammatory Response of Pancreatic Acinar Cells in the Pathogenesis of Acute Alcoholic Pancreatitis. Cell Death Dis. 2013, 4, e816. [Google Scholar] [CrossRef] [Green Version]
- Ara, T.; DeClerck, Y.A. Interleukin-6 in Bone Metastasis and Cancer Progression. Eur. J. Cancer Oxf. Engl. 1990 2010, 46, 1223–1231. [Google Scholar] [CrossRef] [Green Version]
- Mentula, P.; Kylänpää, M.-L.; Kemppainen, E.; Jansson, S.-E.; Sarna, S.; Puolakkainen, P.; Haapiainen, R.; Repo, H. Plasma Anti-inflammatory Cytokines and Monocyte Human Leucocyte Antigen-DR Expression in Patients with Acute Pancreatitis. Scand. J. Gastroenterol. 2004, 39, 178–187. [Google Scholar] [CrossRef]
- Marrache, F.; Tu, S.P.; Bhagat, G.; Pendyala, S.; Osterreicher, C.H.; Gordon, S.; Ramanathan, V.; Penz-Osterreicher, M.; Betz, K.S.; Song, Z.; et al. Overexpression of Interleukin-1beta in the Murine Pancreas Results in Chronic Pancreatitis. Gastroenterology 2008, 135, 1277–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotton, P.B. Are Low-Volume ERCPists a Problem in the United States? A Plea to Examine and Improve ERCP Practice-NOW. Gastrointest. Endosc. 2011, 74, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Peery, A.F.; Crockett, S.D.; Murphy, C.C.; Lund, J.L.; Dellon, E.S.; Williams, J.L.; Jensen, E.T.; Shaheen, N.J.; Barritt, A.S.; Lieber, S.R.; et al. Burden and Cost of Gastrointestinal, Liver, and Pancreatic Diseases in the United States: Update 2018. Gastroenterology 2019, 156, 254–272.e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, A.L.; McNabb-Baltar, J. Hypertriglyceridemia and Acute Pancreatitis. Pancreatol. Off. J. Int. Assoc. Pancreatol. IAP Al 2020, 20, 795–800. [Google Scholar] [CrossRef]
- Adiamah, A.; Kushairi, A.; Tumilty, S.; Na, Y.; Crook, M.; Brooks, A.J.; Lobo, D.N. Hypertriglyceridaemia as a Risk Factor for Critical Care Admission in Acute Pancreatitis: A Prospective Study. Clin. Nutr. Espen 2020, 39, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.-Y.; Li, H.-X.; Zhang, Y.; He, W.-H. Hypertriglyceridemia-Induced Acute Pancreatitis: Progress on Disease Mechanisms and Treatment Modalities. Discov. Med. 2019, 27, 101–109. [Google Scholar]
- Okamura, D.; Starr, M.E.; Lee, E.Y.; Stromberg, A.J.; Evers, B.M.; Saito, H. Age-dependent vulnerability to experimental acute pancreatitis is associated with increased systemic inflammation and thrombosis. Aging Cell. 2012, 11, 760–769. [Google Scholar] [CrossRef] [Green Version]
- Systemic Anticoagulation Found to Benefit Acute Pancreatitis Patients. Available online: https://www.mdedge.com/internalmedicine/article/201168/gastroenterology/systemic-anticoagulation-found-benefit-acute (accessed on 2 October 2021).
- Budnitz, D.S.; Lovegrove, M.C.; Shehab, N.; Richards, C.L. Emergency Hospitalizations for Adverse Drug Events in Older Americans. N. Engl. J. Med. 2011, 365, 2002–2012. [Google Scholar] [CrossRef]
- Couris, R.; Tataronis, G.; McCloskey, W.; Oertel, L.; Dallal, G.; Dwyer, J.; Blumberg, J.B. Dietary Vitamin K Variability Affects International Normalized Ratio (INR) Coagulation Indices. Int. J. Vitam. Nutr. Res. Int. Z. Vitam. Ernahr. J. Int. Vitaminol. Nutr. 2006, 76, 65–74. [Google Scholar] [CrossRef]
- Shields, L.B.E.; Fowler, P.; Siemens, D.M.; Lorenz, D.J.; Wilson, K.C.; Hester, S.T.; Honaker, J.T. Standardized Warfarin Monitoring Decreases Adverse Drug Reactions. BMC Fam. Pract. 2019, 20, 151. [Google Scholar] [CrossRef] [Green Version]
- Garcia, D.; Ageno, W.; Bussey, H.; Eikelboom, J.; Margaglione, M.; Marongiu, F.; Moia, M.; Palareti, G.; Pengo, V.; Poli, D.; et al. Prevention and Treatment of Bleeding Complications in Patients Receiving Vitamin K Antagonists, Part 1: Prevention. Am. J. Hematol. 2009, 84, 579–583. [Google Scholar] [CrossRef]
- Ageno, W.; Garcia, D.; Aguilar, M.I.; Douketis, J.; Finazzi, G.; Imberti, D.; Iorio, A.; Key, N.S.; Lim, W.; Marietta, M.; et al. Prevention and Treatment of Bleeding Complications in Patients Receiving Vitamin K Antagonists, Part 2: Treatment. Am. J. Hematol. 2009, 84, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Limdi, N.A.; McGwin, G.; Goldstein, J.A.; Beasley, T.M.; Arnett, D.K.; Adler, B.K.; Baird, M.F.; Acton, R.T. Influence of CYP2C9 and VKORC1 1173C/T Genotype on the Risk of Hemorrhagic Complications in African-American and European-American Patients on Warfarin. Clin. Pharmacol. Ther. 2008, 83, 312–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baranova, E.V.; Verhoef, T.I.; Asselbergs, F.W.; de Boer, A.; Maitland-van der Zee, A.-H. Genotype-Guided Coumarin Dosing: Where Are We Now and Where Do We Need to Go Next? Expert Opin. Drug Metab. Toxicol. 2015, 11, 509–522. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EDEMA (0–3) | INFLAMMATORY INFILTRATION (0–3) | VACUOLIZATION (0–3) | NECROSIS (0–3) | HEMORRHAGES (0–3) | |
|---|---|---|---|---|---|
| CONTROL | 0 | 0 | 0 | 0 | 0 |
| WARFARIN 90 + saline | 0–1 | 0 | 0 | 0 | 0 |
| WARFARIN 180 + saline | 0 | 0 | 0 | 0 | 0 |
| WARFARIN 270 + saline | 0–1 | 0 | 0 | 0 | 0–1 |
| CIAP | 2–3 | 2 | 2–3 | 0 | 0 |
| WARFARIN 90 + CIAP | 1–2 | 1–2 | 2 | 0 | 0 |
| WARFARIN 180 + CIAP | 1–2 | 1 | 2 | 0 | 0 |
| WARFARIN 270 + CIAP | 2–3 | 1–2 | 2 | 0 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konarska-Bajda, K.; Ceranowicz, P.; Cieszkowski, J.; Ginter, G.; Stempniewicz, A.; Gałązka, K.; Kuśnierz-Cabala, B.; Dumnicka, P.; Bonior, J.; Warzecha, Z. Administration of Warfarin Inhibits the Development of Cerulein-Induced Edematous Acute Pancreatitis in Rats. Biomolecules 2023, 13, 948. https://doi.org/10.3390/biom13060948
Konarska-Bajda K, Ceranowicz P, Cieszkowski J, Ginter G, Stempniewicz A, Gałązka K, Kuśnierz-Cabala B, Dumnicka P, Bonior J, Warzecha Z. Administration of Warfarin Inhibits the Development of Cerulein-Induced Edematous Acute Pancreatitis in Rats. Biomolecules. 2023; 13(6):948. https://doi.org/10.3390/biom13060948
Chicago/Turabian StyleKonarska-Bajda, Katarzyna, Piotr Ceranowicz, Jakub Cieszkowski, Grzegorz Ginter, Agnieszka Stempniewicz, Krystyna Gałązka, Beata Kuśnierz-Cabala, Paulina Dumnicka, Joanna Bonior, and Zygmunt Warzecha. 2023. "Administration of Warfarin Inhibits the Development of Cerulein-Induced Edematous Acute Pancreatitis in Rats" Biomolecules 13, no. 6: 948. https://doi.org/10.3390/biom13060948
APA StyleKonarska-Bajda, K., Ceranowicz, P., Cieszkowski, J., Ginter, G., Stempniewicz, A., Gałązka, K., Kuśnierz-Cabala, B., Dumnicka, P., Bonior, J., & Warzecha, Z. (2023). Administration of Warfarin Inhibits the Development of Cerulein-Induced Edematous Acute Pancreatitis in Rats. Biomolecules, 13(6), 948. https://doi.org/10.3390/biom13060948