Optimization-Based Constrained Trajectory Generation for Robot-Assisted Stitching in Endonasal Surgery



Abstract
:1. Introduction
1.1. Related Work
- An online optimization-based needle trajectory generation method that is used as a reference for a smooth guidance virtual fixture.
- Constrained motion planning based on dual concurrent inverse kinematics (IK) solver that integrates a task-priority based IK and a nonlinear optimization based IK.
- Experimental comparison between the proposed method in a robot-assisted mode and an autonomous mode with the use of a conventional surgical tool.
2. Materials and Methods
2.1. System Overview
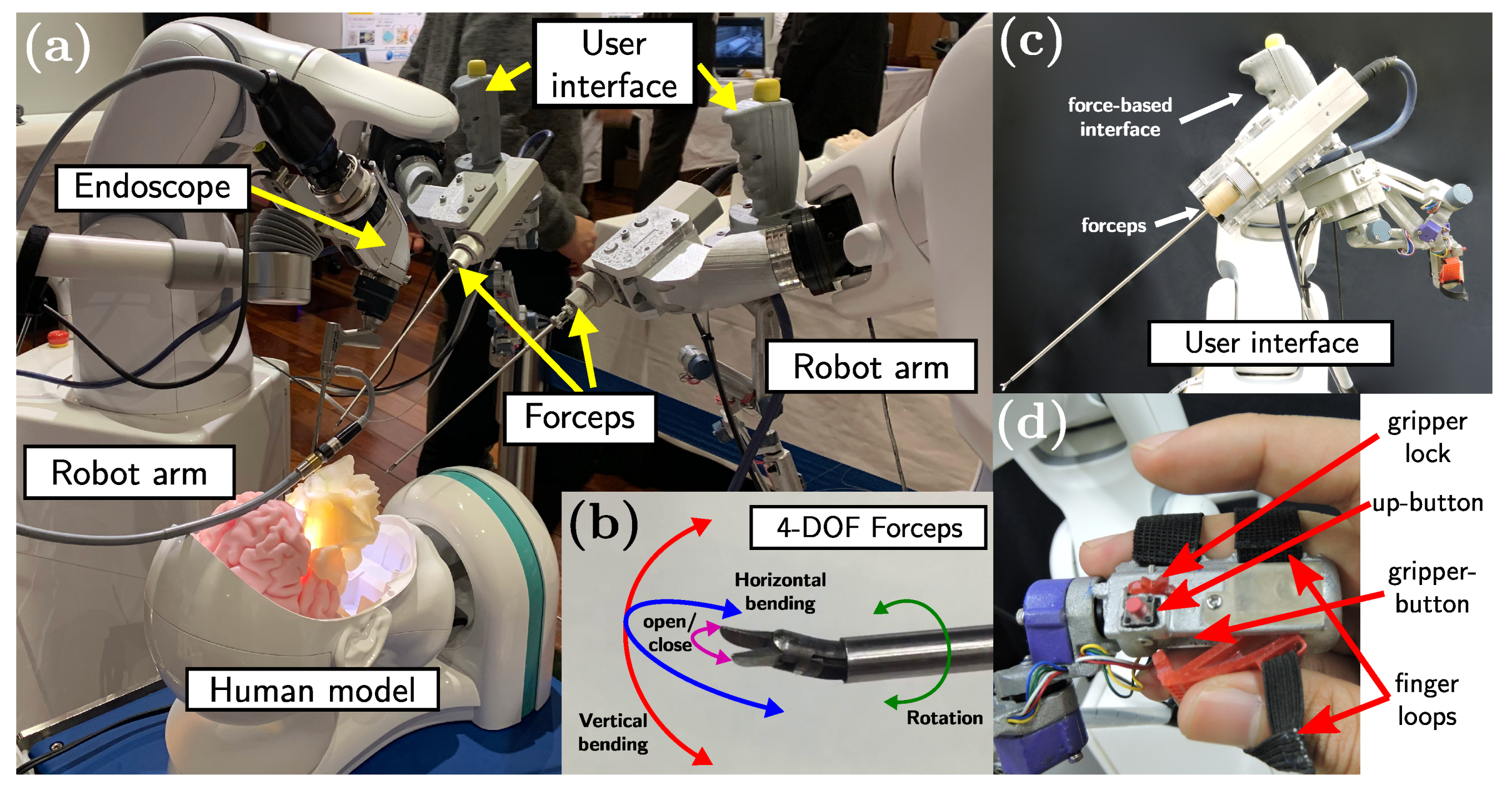
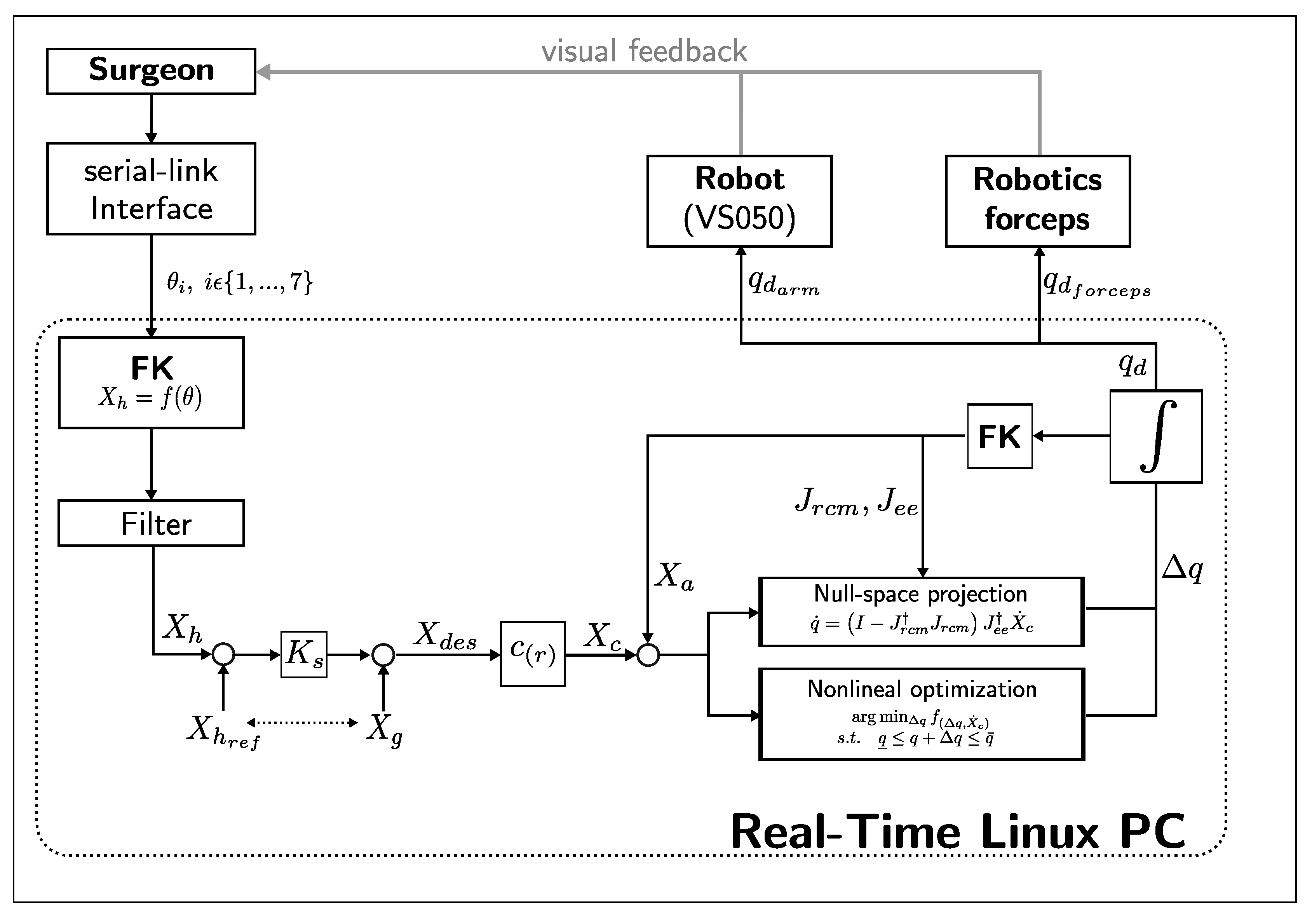
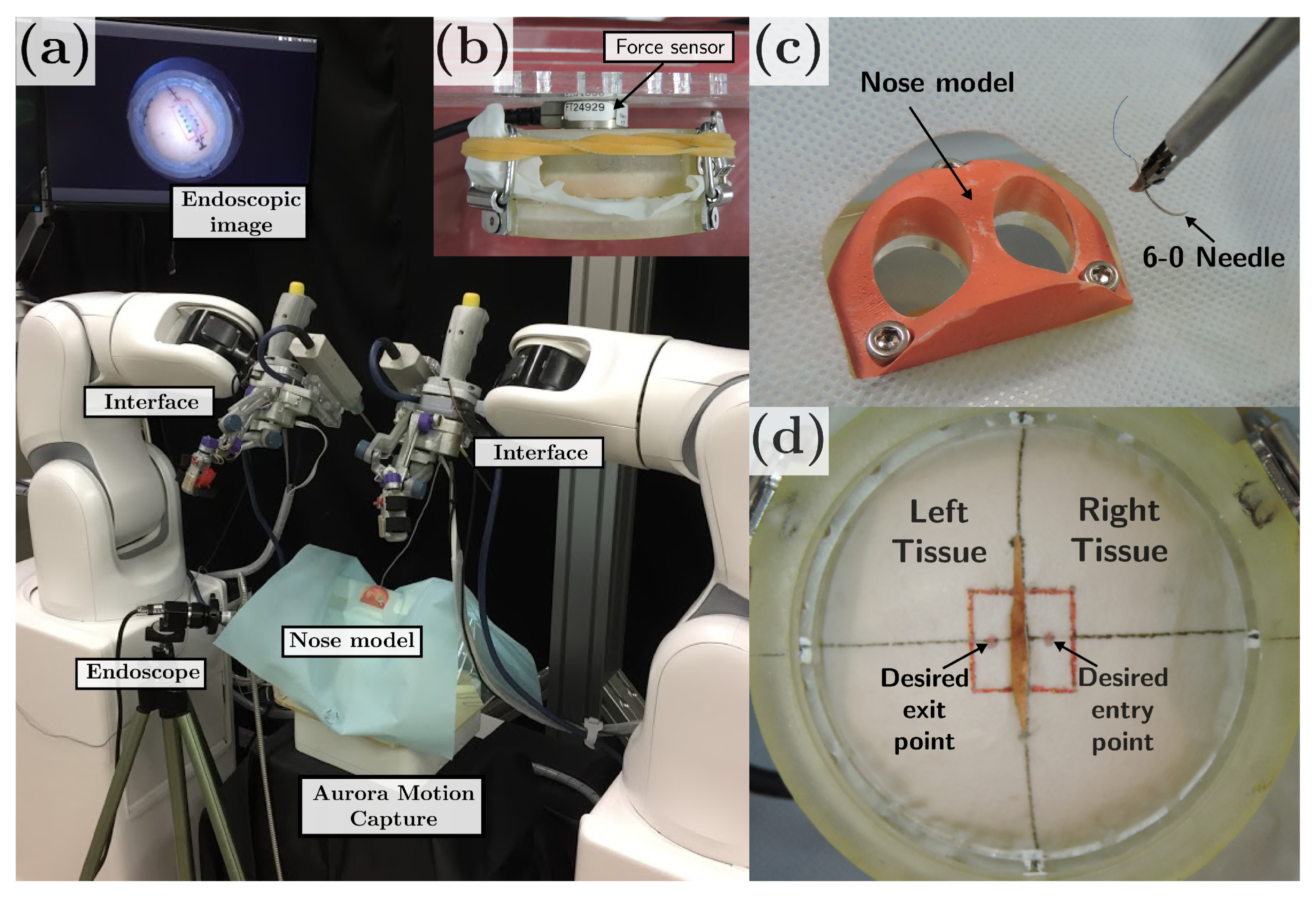
2.1.1. Robotic Surgical System
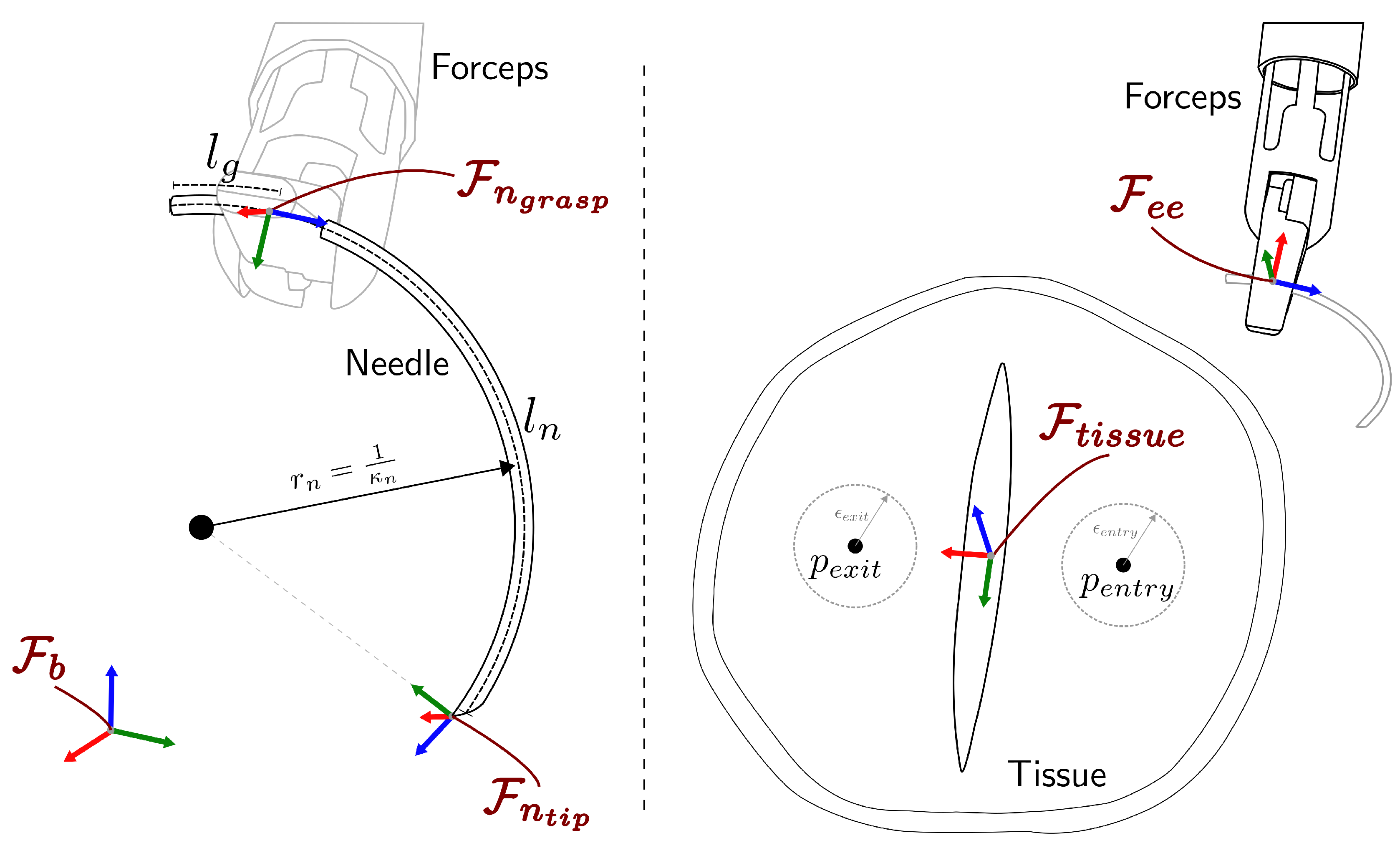
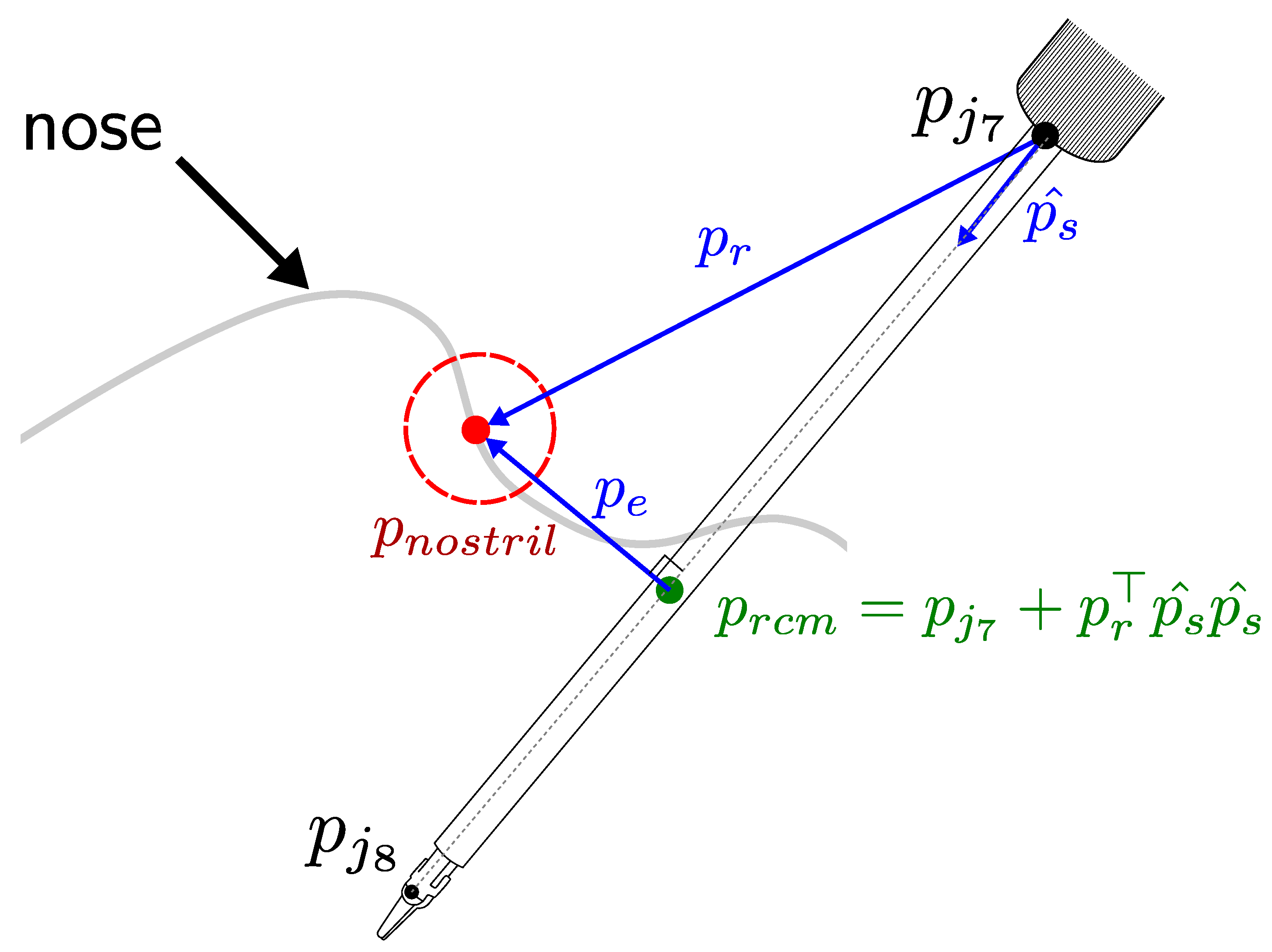
2.1.2. Description of the Stitching Workspace Frames
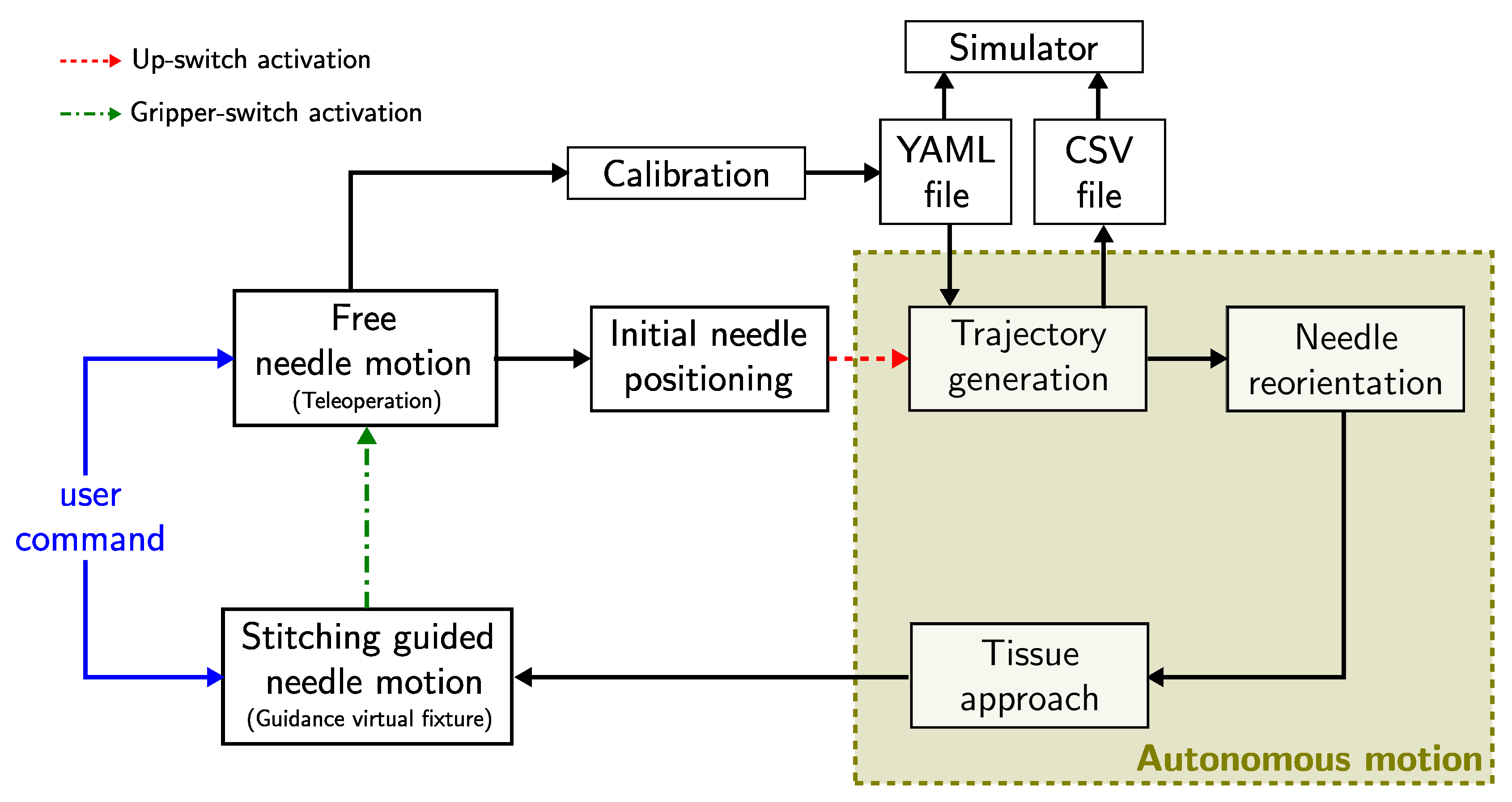
2.1.3. Algorithm Overview
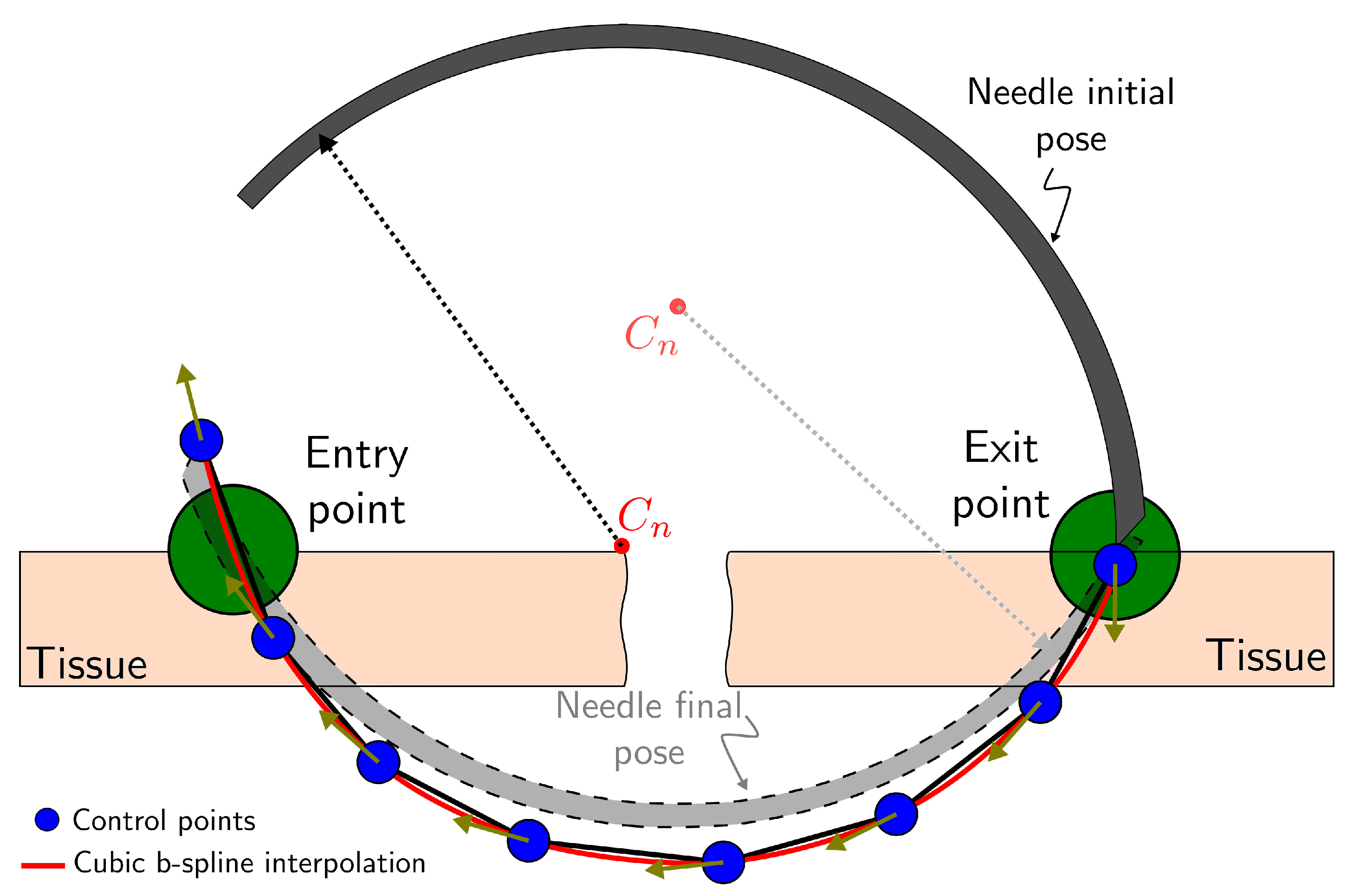
2.2. Online Optimization-Based Trajectory Generation
2.2.1. Sequential Convex Programming
| Algorithm 1: penalty trust region based sequential optimization. |
 |
2.2.2. Problem Definition
2.2.3. Optimization Model
Costs (Equation (7)):
Stitching kinematic constraints (Equation (8)):
Desired Entry/Exit Port Constraints (Equations (9) and (10)):
Needle Constraints (Equation (11)):
Suture depth constraint (Equation (12)):
Needle reorientation constraints (Equations (13)–(15)):
2.3. Constrained Motion Planning
2.3.1. Guidance Virtual Fixture
2.3.2. Task-Priority Inverse Kinematics
2.3.3. Nonlinear Optimization Inverse Kinematics
3. Experiments and Discussion
3.1. Implementation Details
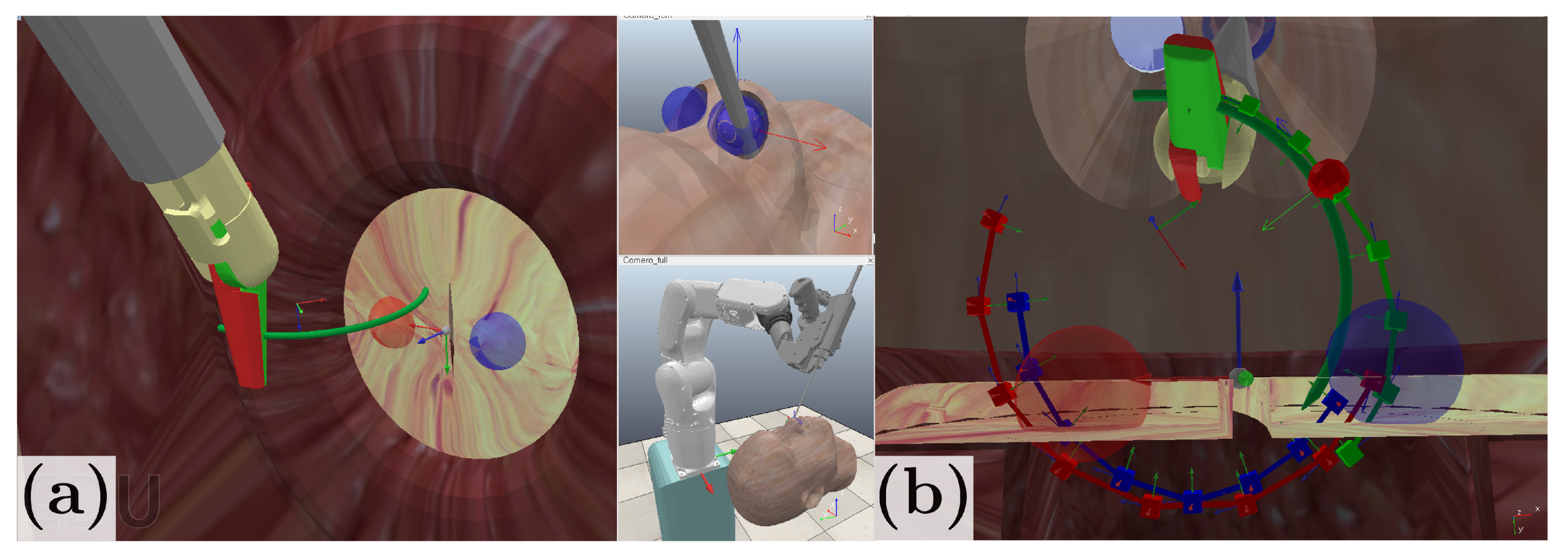
3.2. Simulation Environment
3.3. Stitching Experiments
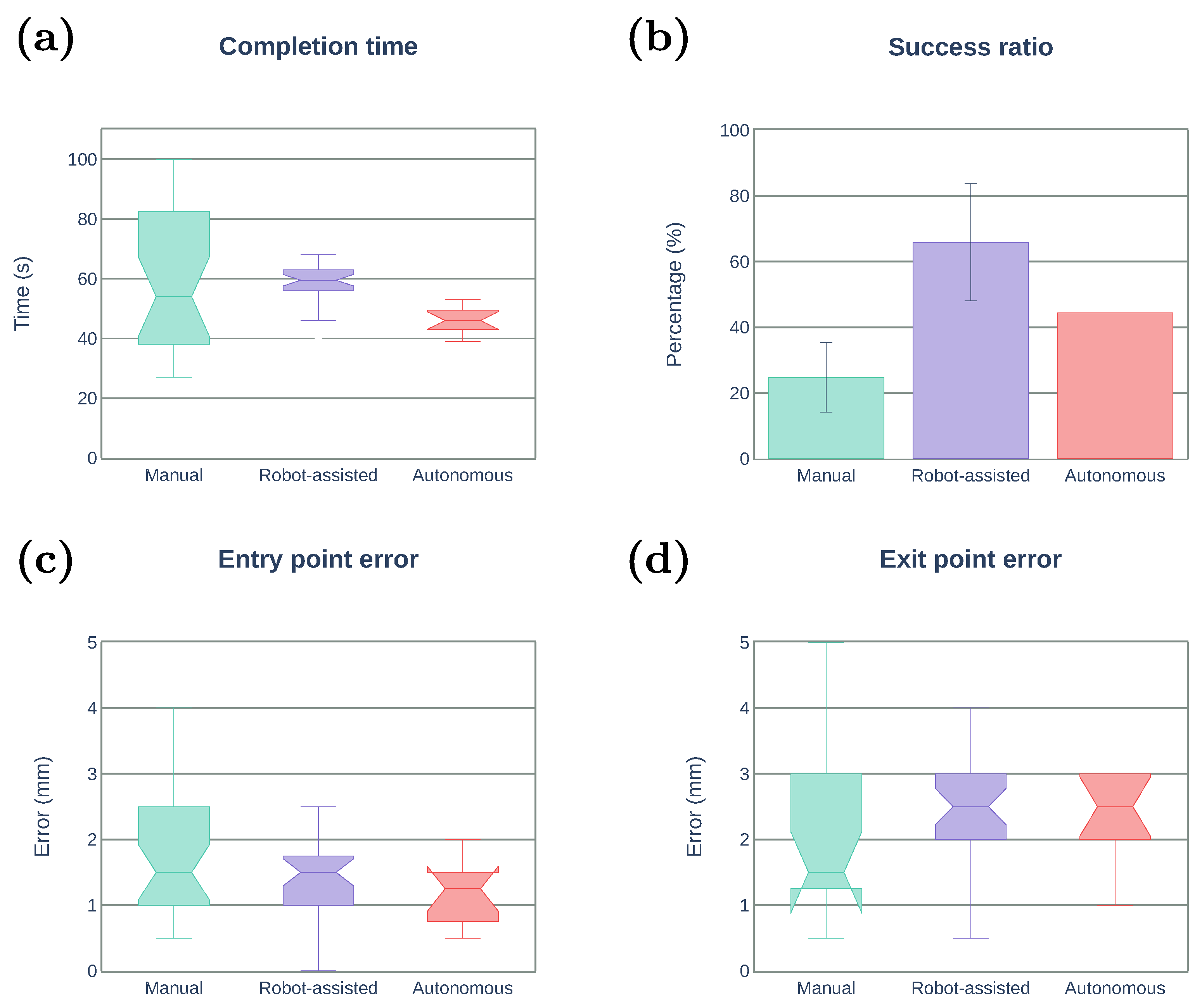
- Manual: by using conventional forceps for endoscopic endonasal surgery.
- Robot-assisted: by using the proposed method. The system generates the optimal trajectory and constrains the needle pose.
- Autonomous: the robot starts in a fixed initial pose and executes the stitching task without human assistance.
- Task completion time (s): the total time in which participants performed the task.
- Success ratio (%): the percentage of succeed stitching from the total number of attempts.
- Entry point error (mm): the Euclidean distance between the desired entry point and the actual entry point.
- Exit point error (mm): the Euclidean distance between the desired exit point and the actual exit point.
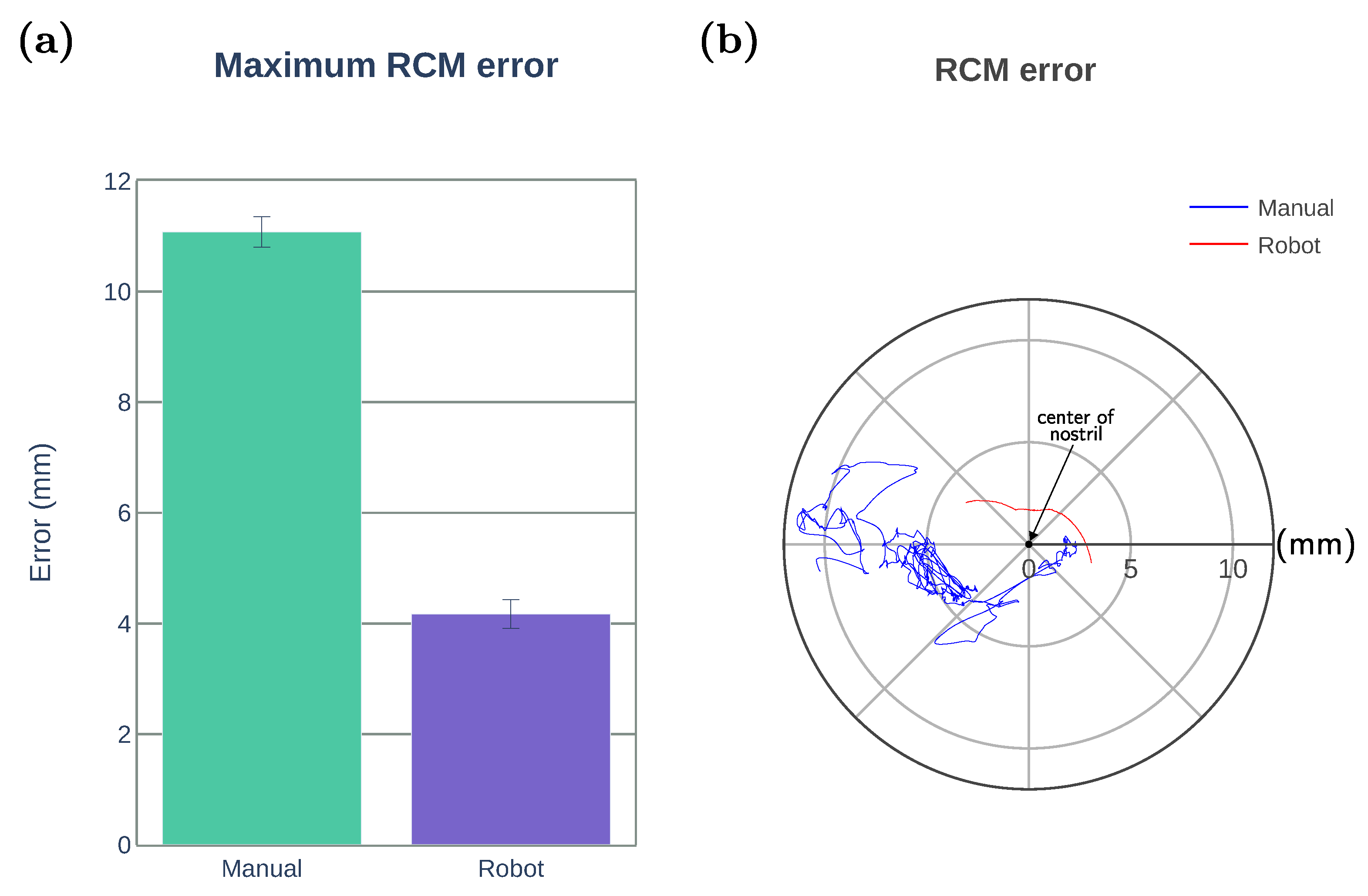
- Maximum RCM error (mm): the maximum Euclidean distance between the RCM position and the center of the nostril.
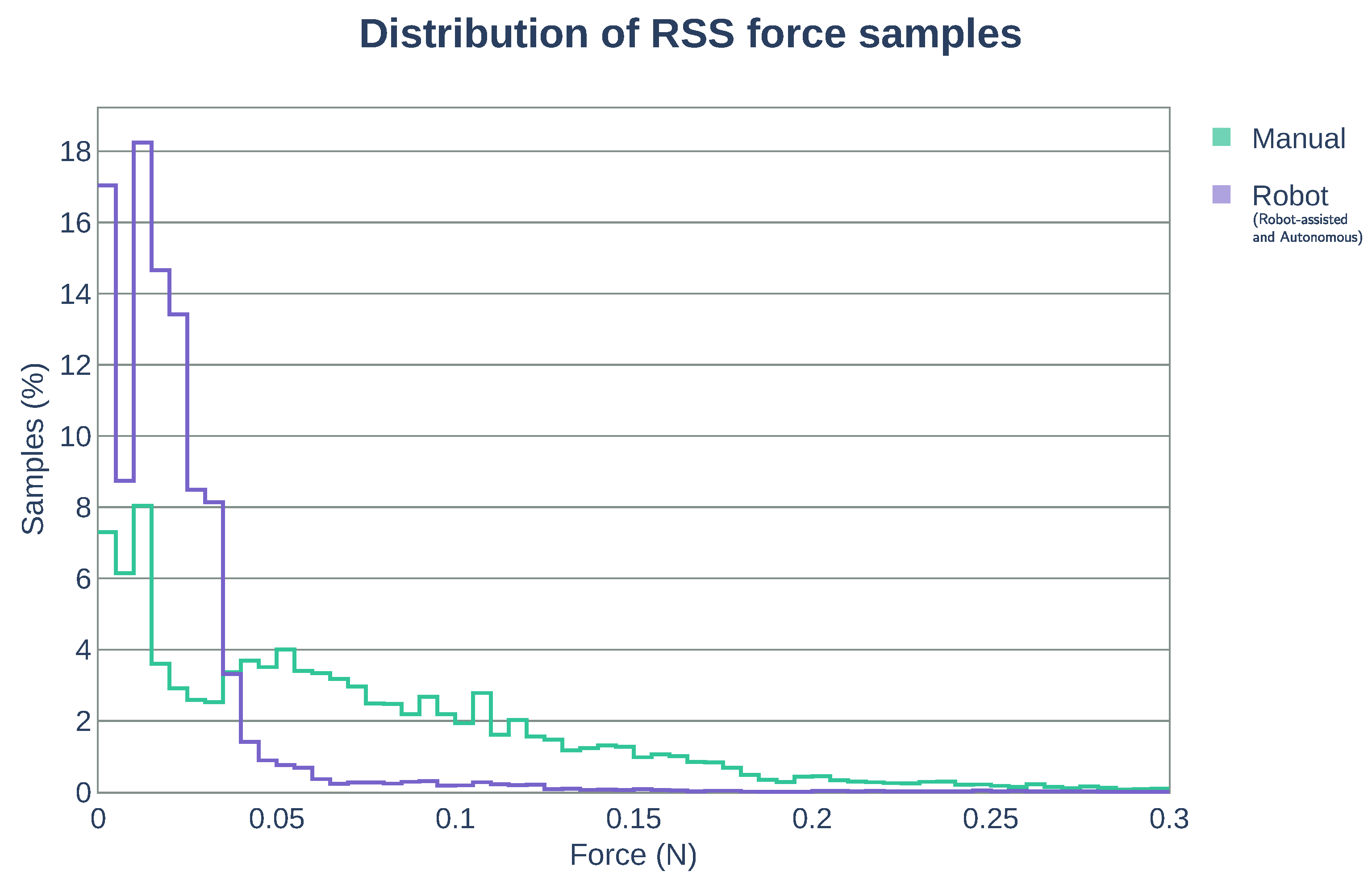
- Maximum RSS force (N): the maximum RSS force applied on the tissue.
- Distribution of RSS force samples: graphical representation of the number of RSS force measurements within equally distributed force intervals with respect to the total number of RSS force samples obtained during the stitching task.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garcia-Ruiz, A.; Gagner, M.; Miller, J.H.; Steiner, C.P.; Hahn, J.F. Manual vs Robotically Assisted Laparoscopic Surgery in the Performance of Basic Manipulation and Suturing Tasks. Arch. Surg. Chic. 1998, 133, 957–961. [Google Scholar] [CrossRef]
- Ruurda, J.P.; Broeders, I.A.M.J.; Pulles, B.; Kappelhof, F.M.; van der Werken, C. Manual robot assisted endoscopic suturing: Time-action analysis in an experimental model. Surg. Endosc. 2004, 18, 1249–1252. [Google Scholar] [CrossRef]
- Kranzfelder, M.; Staub, C.; Fiolka, A.; Schneider, A.; Gillen, S.; Wilhelm, D.; Friess, H.; Knoll, A.; Feussner, H. Toward increased autonomy in the surgical OR: Needs, requests, and expectations. Surg. Endosc. 2013, 27, 1681–1688. [Google Scholar] [CrossRef] [Green Version]
- Colan, J.; Nakanishi, J.; Aoyama, T.; Hasegawa, Y. A Cooperative Human-Robot Interface for Constrained Manipulation in Robot-Assisted Endonasal Surgery. Appl. Sci. 2020, 10, 4809. [Google Scholar] [CrossRef]
- Kapoor, A.; Li, M.; Taylor, R.H. Spatial Motion Constraints for Robot Assisted Suturing Using Virtual Fixtures. In Proceedings of the 2005 International Conference on Medical Image Computing and Computer-Assisted Intervention, Palm Springs, CA, USA, 26–29 October 2005; pp. 89–96. [Google Scholar] [CrossRef] [Green Version]
- Knoll, A.; Mayer, H.; Staub, C.; Bauernschmitt, R. Selective automation and skill transfer in medical robotics: A demonstration on surgical knot-tying. Int. J. Med. Robot. Comput. Assist. Surg. 2012, 8, 384–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osa, T.; Sugita, N.; Mitsuishi, M. Online Trajectory Planning in Dynamic Environments for Surgical Task Automation. In Proceedings of the 2014 Robotics: Science and Systems Conference, Berkeley, CA, USA, 12–16 July 2014; pp. 1–9. [Google Scholar] [CrossRef]
- Van den Berg, J.; Miller, S.; Duckworth, D.; Hu, H.; Wan, A.; Fu, X.-Y.; Goldberg, K.; Abbeel, P. Superhuman Performance of Surgical Tasks by Robots using Iterative Learning from Human-Guided Demonstrations. In Proceedings of the 2010 IEEE International Conference on Robotics and Automation, Anchorage, AK, USA, 3–7 May 2010; pp. 2074–2081. [Google Scholar] [CrossRef]
- Kang, H.; Wen, J.T. Autonomous suturing using minimally invasive surgical robots. In Proceedings of the 2000 IEEE International Conference on Control Applications, Anchorage, AK, USA, 27 September 2000; pp. 742–747. [Google Scholar] [CrossRef]
- Chow, D.-L.; Newman, W. Trajectory Optimization of Robotic Suturing. In Proceedings of the 2015 IEEE International Conference on Technologies for Practical Robot Applications, Woburn, MA, USA, 11–12 May 2015; pp. 1–6. [Google Scholar] [CrossRef]
- Nageotte, F.; Zanne, P.; Doignon, C.; de Mathelin, M. Stitching Planning in Laparoscopic Surgery: Towards Robot-assisted Suturing. Int. J. Robot. Res. 2009, 28, 1303–1321. [Google Scholar] [CrossRef]
- Liu, T.; Cavusoglu, M.C. Needle Grasp and Entry Port Selection for Automatic Execution of Suturing Tasks in Robotic Minimally Invasive Surgery. IEEE Trans. Autom. Sci. Eng. 2016, 13, 552–563. [Google Scholar] [CrossRef] [PubMed]
- Staub, C.; Osa, T.; Knoll, A.; Bauernschmitt, R. Automation of Tissue Piercing using Circular Needles and Vision Guidance for Computer Aided Laparoscopic Surgery. In Proceedings of the 2010 IEEE International Conference on Robotics and Automation, Anchorage, AK, USA, 3–7 May 2010; pp. 4585–4590. [Google Scholar] [CrossRef] [Green Version]
- D’Ettorre, C.; Dwyer, G.; Du, X.; Chadebecq, F.; Vasconcelos, F.; Momi, E.D.; Stoyanov, D. Automated pick-up of suturing needles for robotic surgical assistance. In Proceedings of the 2018 IEEE International Conference on Robotics and Automation, Brisbane, QLD, Australia, 21–25 May 2018; pp. 1370–1377. [Google Scholar] [CrossRef] [Green Version]
- Iyer, S.; Looi, T.; Drake, J. A Single Arm, Single Camera System for Automated Suturing. In Proceedings of the 2013 IEEE International Conference on Robotics and Automation, Karlsruhe, Germany, 6–10 May 2013; pp. 239–244. [Google Scholar] [CrossRef]
- Pedram, S.A.; Ferguson, P.; Ma, J.; Dutson, E.; Rosen, J. Autonomous Suturing via Surgical Robot: An Algorithm for Optimal Selection of Needle Diameter, Shape, and Path. In Proceedings of the 2017 IEEE International Conference on Robotics and Automation, Singapore, 29 May–3 June 2017; pp. 2391–2398. [Google Scholar] [CrossRef]
- Sen, S.; Garg, A.; Gealy, D.V.; McKinley, S.; Jen, Y.; Goldberg, K. Automating Multi-Throw Multilateral Surgical Suturing with a Mechanical Needle Guide and Sequential Convex Optimization. In Proceedings of the 2016 IEEE International Conference on Robotics and Automation, Stockholm, Sweden, 16–21 May 2016; pp. 4178–4185. [Google Scholar] [CrossRef] [Green Version]
- Jackson, R.C.; Cavusoglu, M.C. Needle Path Planning for Autonomous Robotic Surgical Suturing. In Proceedings of the 2013 IEEE International Conference on Robotics and Automation, Karlsruhe, Germany, 6–10 May 2013; pp. 1669–1675. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, K.; Kanno, T.; Ito, K.; Kawashima, K. Single-Master Dual-Slave Surgical Robot With Automated Relay of Suture Needle. IEEE Trans. Ind. Electron. 2018, 65, 6343–6351. [Google Scholar] [CrossRef]
- Adhami, L.; Coste-Maniere, E. Optimal planning for minimally invasive surgical robots. IEEE Trans. Robot. Autom. 2003, 19, 854–863. [Google Scholar] [CrossRef]
- Kehoe, B.; Kahn, G.; Mahler, J.; Kim, J.; Lee, A.; Lee, A.; Nakagawa, K.; Patil, S.; Boyd, W.D.; Abbeel, P.; et al. Autonomous Multilateral Debridement with the Raven Surgical Robot. In Proceedings of the 2014 IEEE International Conference on Robotics and Automation, Hong Kong, China, 31 May–7 June 2014; pp. 1432–1439. [Google Scholar] [CrossRef] [Green Version]
- Murali, A.; Sen, S.; Kehoe, B.; Garz, A.; McFarland, S.; Patil, S.; Boyd, W.D.; Lim, S.; Abbeel, P.; Goldberg, K. Learning by Observation for Surgical Subtasks: Multilateral Cutting of 3D Viscoelastic and 2D Orthotropic Tissue Phantoms. In Proceedings of the 2015 IEEE International Conference on Robotics and Automation, Seattle, WA, USA, 26–30 May 2015; pp. 1202–1209. [Google Scholar] [CrossRef] [Green Version]
- Thananjeyan, B.; Garg, A.; Krishnan, S.; Chen, C.; Miller, L.; Goldberg, K. Multilateral Surgical Pattern Cutting in 2D Orthotropic Gauze with Deep Reinforcement Learning Policies for Tensioning. In Proceedings of the 2017 IEEE International Conference on Robotics and Automation, Singapore, 29 May–3 June 2017; pp. 2371–2378. [Google Scholar] [CrossRef]
- Javdani, S.; Tandon, S.; Tang, J.; O’Brien, J.F.; Abbeel, P. Modeling and Perception of Deformable One-Dimensional Objects. In Proceedings of the 2011 IEEE International Conference on Robotics and Automation, Shanghai, China, 9–13 May 2011; pp. 1607–1614. [Google Scholar] [CrossRef] [Green Version]
- Jackson, R.C.; Yuan, R.; Chow, D.-L.; Newman, W.S.; Avuolu, M.C. Real-Time Visual Tracking of Dynamic Surgical Suture Threads. IEEE Trans. Autom. Sci. Eng. 2018, 15, 1078–1090. [Google Scholar] [CrossRef] [PubMed]
- Padoy, N.; Hager, G.D. Human-Machine Collaborative Surgery Using Learned Models. In Proceedings of the 2011 IEEE International Conference on Robotics and Automation, Shanghai, China, 9–13 May 2011; pp. 5285–5292. [Google Scholar] [CrossRef] [Green Version]
- Reed, K.B.; Majewicz, A.; Kallem, V.; Alterovitz, R.; Goldberg, K.; Cowan, N.J.; Okamura, A.M. Robot-Assisted Needle Steering. IEEE Robot. Autom. Mag. 2011, 18, 35–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Malpani, A.; Chalasani, P.; Deguet, A.; Vedula, S.S.; Kazanzides, P.; Taylor, R.H. Virtual Fixture Assistance for Needle Passing and Knot Tying. In Proceedings of the 2016 IEEE/RSJ International Conference on Intelligent Robots and Systems, Daejeon, Korea, 9–14 October 2016; pp. 2343–2350. [Google Scholar] [CrossRef]
- Selvaggio, M.; Ghalamzan Esfahani, A.; Moccia, R.; Ficuciello, F.; Siciliano, B. Haptic-guided shared control for needle grasping optimization in minimally invasive robotic surgery. In Proceedings of the 2019 IEEE/RSJ International Conference on Intelligent Robots and Systems, Macau, China, 3–8 November 2019; pp. 3617–3623. [Google Scholar] [CrossRef] [Green Version]
- Marinho, M.M.; Ishida, H.; Harada, K.; Deie, K.; Mitsuishi, M. Virtual Fixture Assistance for Suturing in Robot-Aided Pediatric Endoscopic Surgery. IEEE Robot. Autom. Lett. 2019, 5, 524–531. [Google Scholar] [CrossRef]
- Fontanelli, G.A.; Yang, G.-Z.; Siciliano, B. A Comparison of Assistive Methods for Suturing in MIRS. In Proceedings of the 2018 IEEE/RSJ International Conference on Intelligent Robots and Systems, Madrid, Spain, 1–5 October 2018; pp. 4389–4395. [Google Scholar] [CrossRef]
- Arata, J.; Fujisawa, Y.; Nakadate, R.; Kiguchi, K.; Harada, K.; Mitsuishi, M.; Hashizume, M. Compliant four degree-of-freedom manipulator with locally deformable elastic elements for minimally invasive surgery. In Proceedings of the 2019 IEEE International Conference on Robotics and Automation, Montreal, QC, Canada, 20–24 May 2019; pp. 2663–2669. [Google Scholar] [CrossRef]
- Schulman, J.; Duan, Y.; Ho, J.; Lee, A.; Awwal, I.; Bradlow, H.; Pan, J.; Patil, S.; Goldberg, K.; Abbeel, P. Motion planning with sequential convex optimization and convex collision checking. Int. J. Robot. Res. 2014, 33, 1251–1270. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, R. Practical Methods of Optimization; John Wiley & Sons: Hoboken, NJ, USA, 1987. [Google Scholar]
- Nocedal, J.; Wright, S.J. Numerical Optimization; Springer Science & Business Media: New York, NY, USA, 2006. [Google Scholar]
- Murray, R.M.; Li, Z.; Sastry, S.S. A Mathematical Introduction to Robotic Manipulation; CRC Press: Boca Raton, FL, USA, 1994. [Google Scholar]
- Bettini, A.; Marayong, P.; Lang, S.; Okamura, A.M.; Hager, G.D. Vision-Assisted Control for Manipulation Using Virtual Fixtures. IEEE Trans. Robot. 2004, 20, 953–966. [Google Scholar] [CrossRef] [Green Version]
- Chiaverini, S. Singularity-robust task-priority redundancy resolution for real-time kinematic control of robot manipulators. IEEE Trans. Robot. Autom. 1997, 13, 398–410. [Google Scholar] [CrossRef] [Green Version]
- Azimian, H.; Patel, R.V.; Naish, M.D. On Constrained Manipulation in Robotics-Assisted Minimally Invasive Surgery. In Proceedings of the 2010 IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, Tokyo, Japan, 26–29 September 2010; pp. 650–655. [Google Scholar] [CrossRef]
- Sandoval, J.; Poisson, G.; Vieyres, P. A New Kinematic Formulation of the RCM Constraint for Redundant Torque-Controlled Robots. In Proceedings of the 2017 IEEE/RSJ International Conference on Intelligent Robots and Systems, Vancouver, BC, Canada, 24–28 September 2017; pp. 4576–4581. [Google Scholar] [CrossRef]
- Beeson, P.; Ames, B. TRAC-IK: An open-source library for improved solving of generic inverse kinematics. In Proceedings of the IEEE-RAS 15th International Conference on Humanoid Robots, Seoul, Korea, 3–5 November 2015; pp. 928–935. [Google Scholar] [CrossRef]
- Carpentier, J.; Saurel, G.; Buondonno, G.; Mirabel, J.; Lamiraux, F.; Stasse, O.; Mansard, N. The Pinocchio C++ library. In Proceedings of the 2019 IEEE/SICE International Symposium on System Integration, Paris, France, 14–16 January 2019; pp. 614–619. [Google Scholar] [CrossRef] [Green Version]
- Andersson, J.A.E.; Gillis, J.; Horn, G.; Rawlings, J.B.; Diehl, M. CasADi: A software framework for nonlinear optimization and optimal control. Math. Program. Comput. 2019, 11, 1–36. [Google Scholar] [CrossRef]
- Gurobi Optimizer. Available online: https://www.gurobi.com/ (accessed on 15 November 2020).
- Wächter, A.; Biegler, L.T. On the implementation of an interior-point filter line-search algorithm for large-scale nonlinear programming. Math. Program. 2006, 106, 25–27. [Google Scholar] [CrossRef]
- Rohmer, E.; Singh, S.P.N.; Freese, M. V-REP: A Versatile and Scalable Robot Simulation Framework. In Proceedings of the 2013 IEEE/RSJ International Conference on Intelligent Robots and Systems, Tokyo, Japan, 3–7 November 2013; pp. 1321–1326. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Notation | Description |
|---|---|
| k-iteration penalty | |
| k-iteration trust region size | |
| k-iteration control variable | |
| step rejection threshold | |
| step acceptance threshold | |
| trust region shrinkage factor | |
| trust region expansion factor | |
| penalty scaling factor | |
| convergence threshold for merit | |
| convergence threshold for control variable | |
| constraint satisfaction threshold | |
| needle pose at step t | |
| N | number of trajectory steps |
| b | needle insertion distance at each step |
| twist applied at step t | |
| needle deviation at step t | |
| max. needle deviation | |
| needle length free for grasping | |
| needle length | |
| needle natural curvature | |
| entry position tolerance | |
| exit position tolerance |
| Subject | # of Trials | # of Success | Success Ratio (%) |
|---|---|---|---|
| 1 | 12 | 4 | 33.3 |
| 2 | 15 | 4 | 26.7 |
| 3 | 12 | 4 | 33.3 |
| 4 | 8 | 2 | 25.0 |
| 5 | 15 | 2 | 13.3 |
| 6 | 12 | 1 | 8.3 |
| 7 | 8 | 3 | 37.5 |
| Total | 82 | 20 | |
| Mean Success Ratio (%) | 25.4 |
| Subject | # of Trials | # of Success | Success Ratio (%) |
|---|---|---|---|
| 1 | 12 | 5 | 41.7 |
| 2 | 10 | 5 | 50.0 |
| 3 | 8 | 5 | 62.5 |
| 4 | 8 | 5 | 62.5 |
| 5 | 7 | 4 | 57.1 |
| 6 | 6 | 6 | 100.0 |
| 7 | 6 | 5 | 83.3 |
| Total | 57 | 35 | |
| Mean Success Ratio (%) | 65.3 |
| # of Trials | # of Success | Success Ratio (%) |
|---|---|---|
| 16 | 7 | 43.8 |
| Mean (N) | SD (N) | |
|---|---|---|
| Manual operation | 0.349 | 0.178 |
| Robotic system | 0.096 | 0.046 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colan, J.; Nakanishi, J.; Aoyama, T.; Hasegawa, Y. Optimization-Based Constrained Trajectory Generation for Robot-Assisted Stitching in Endonasal Surgery. Robotics 2021, 10, 27. https://doi.org/10.3390/robotics10010027
Colan J, Nakanishi J, Aoyama T, Hasegawa Y. Optimization-Based Constrained Trajectory Generation for Robot-Assisted Stitching in Endonasal Surgery. Robotics. 2021; 10(1):27. https://doi.org/10.3390/robotics10010027
Chicago/Turabian StyleColan, Jacinto, Jun Nakanishi, Tadayoshi Aoyama, and Yasuhisa Hasegawa. 2021. "Optimization-Based Constrained Trajectory Generation for Robot-Assisted Stitching in Endonasal Surgery" Robotics 10, no. 1: 27. https://doi.org/10.3390/robotics10010027
APA StyleColan, J., Nakanishi, J., Aoyama, T., & Hasegawa, Y. (2021). Optimization-Based Constrained Trajectory Generation for Robot-Assisted Stitching in Endonasal Surgery. Robotics, 10(1), 27. https://doi.org/10.3390/robotics10010027