
An Open Source GIS Application for Spatial Assessment of Health Care Quality Indicators

 ,
,  ,
,  , , and
, , and
Abstract
:1. Background
2. Materials and Methods
2.1. Database
2.2. Health Care Quality Indicators (HCQIs) GIS Application
2.3. Web Map Development
2.4. Ethical Statement/Considerations
3. Results
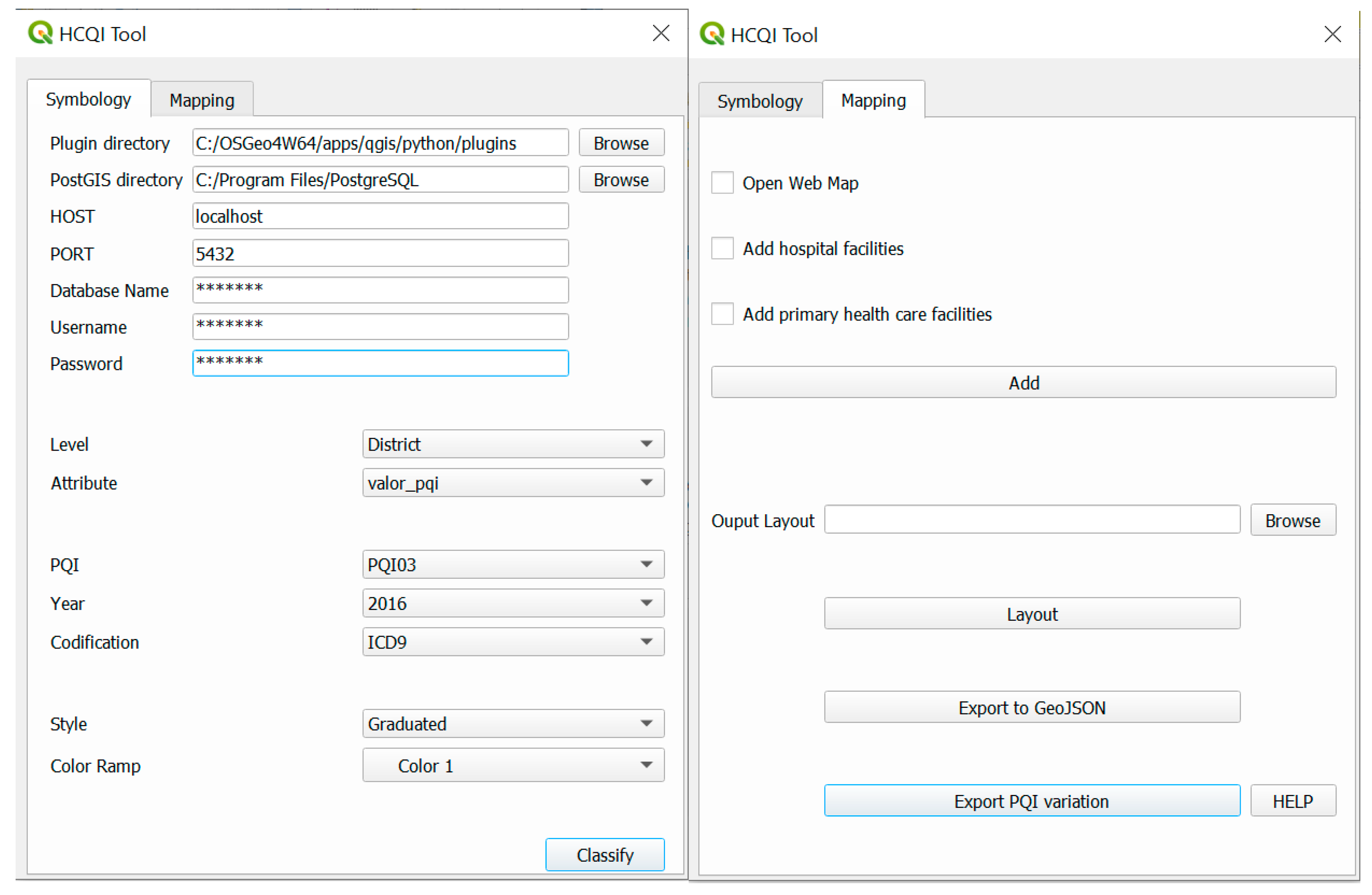
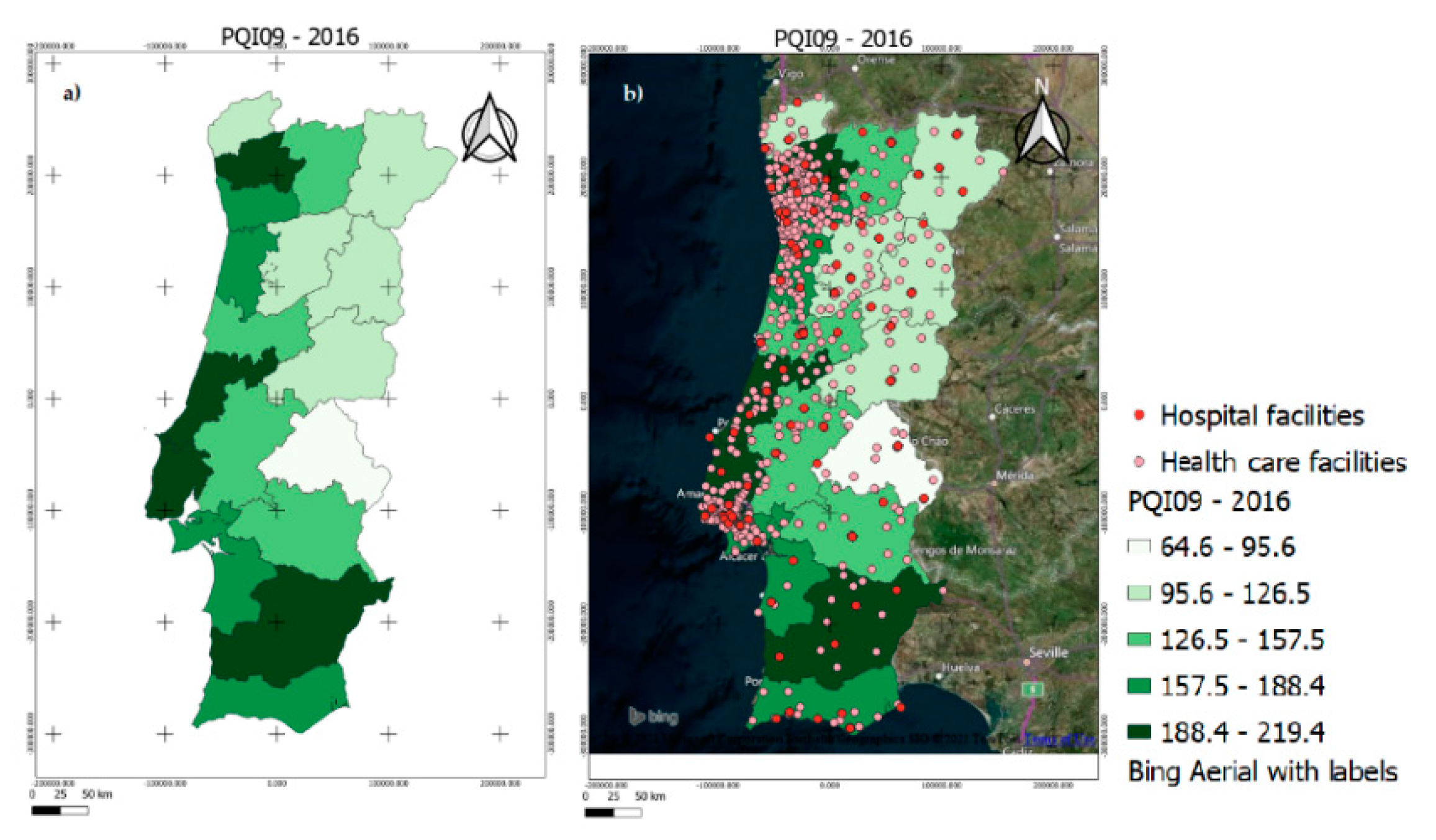
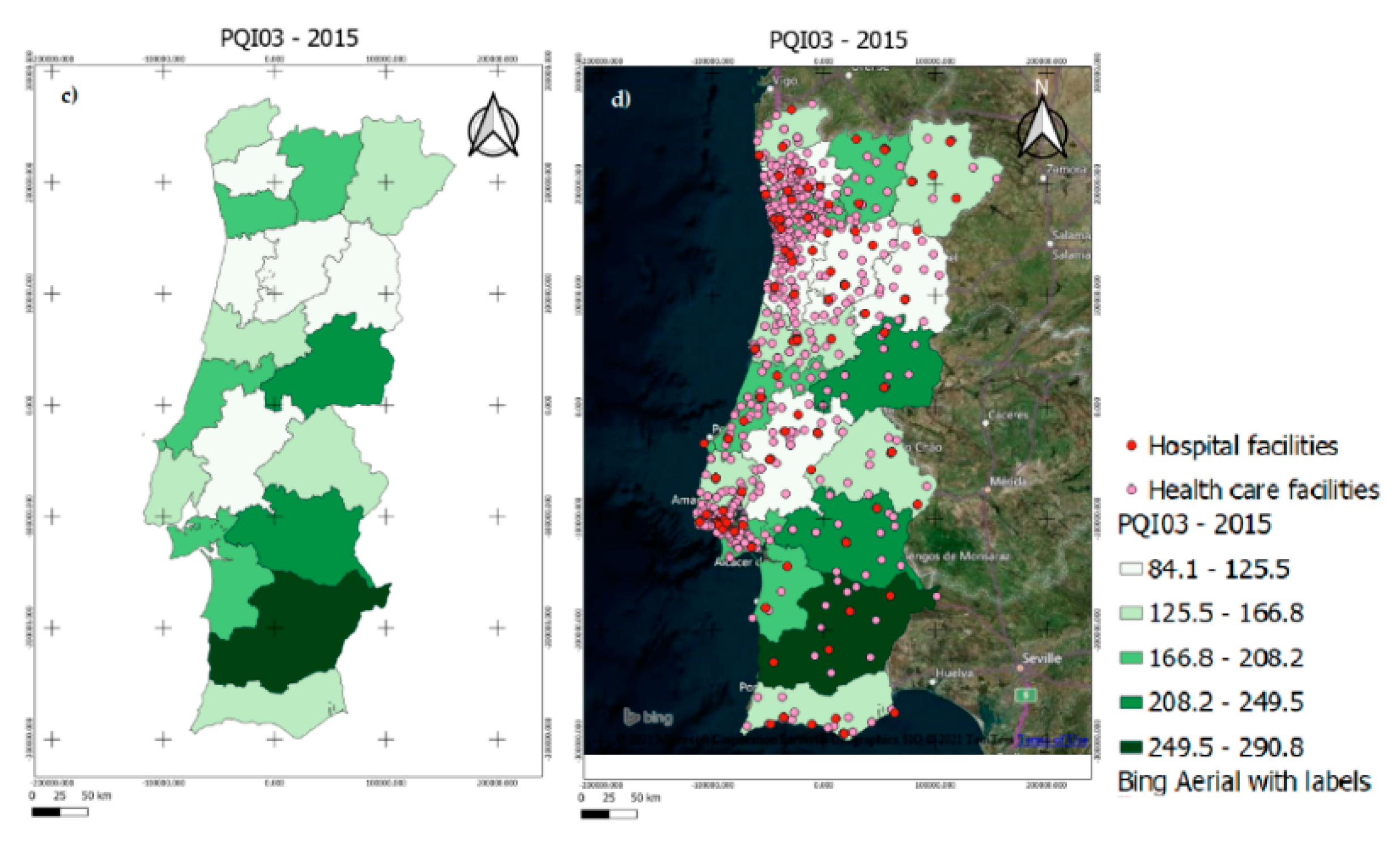
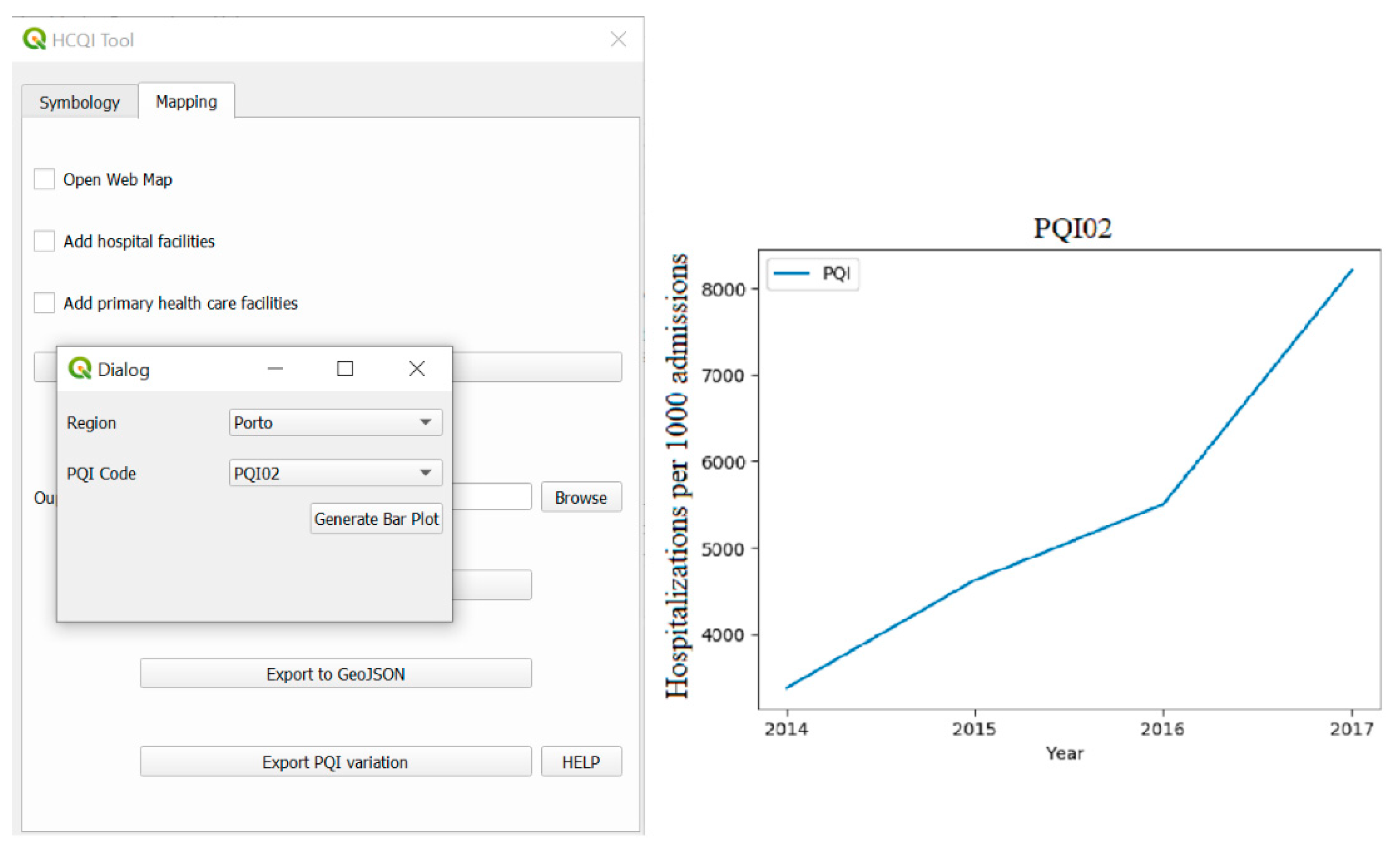
3.1. GIS Open Source Application
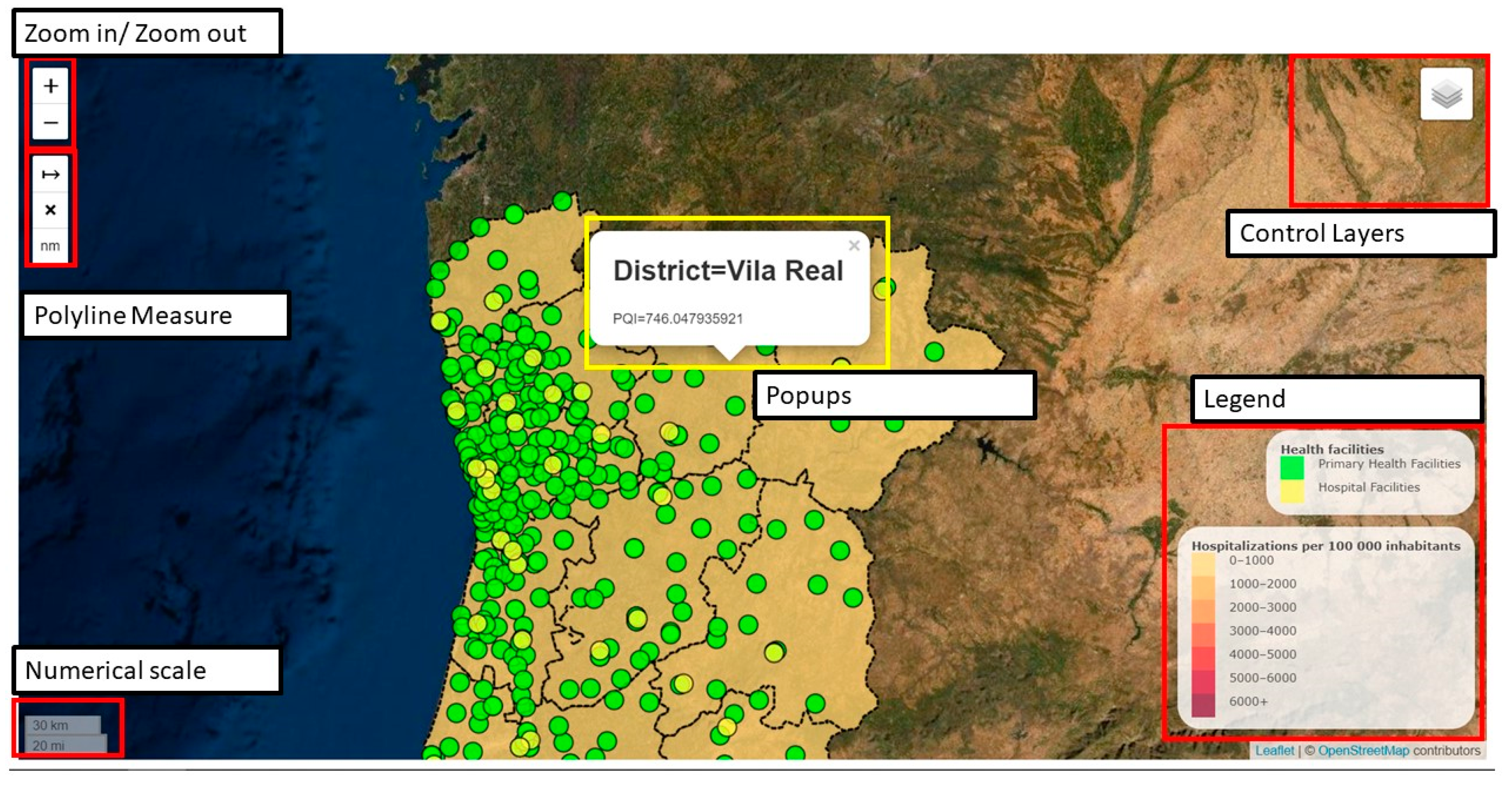
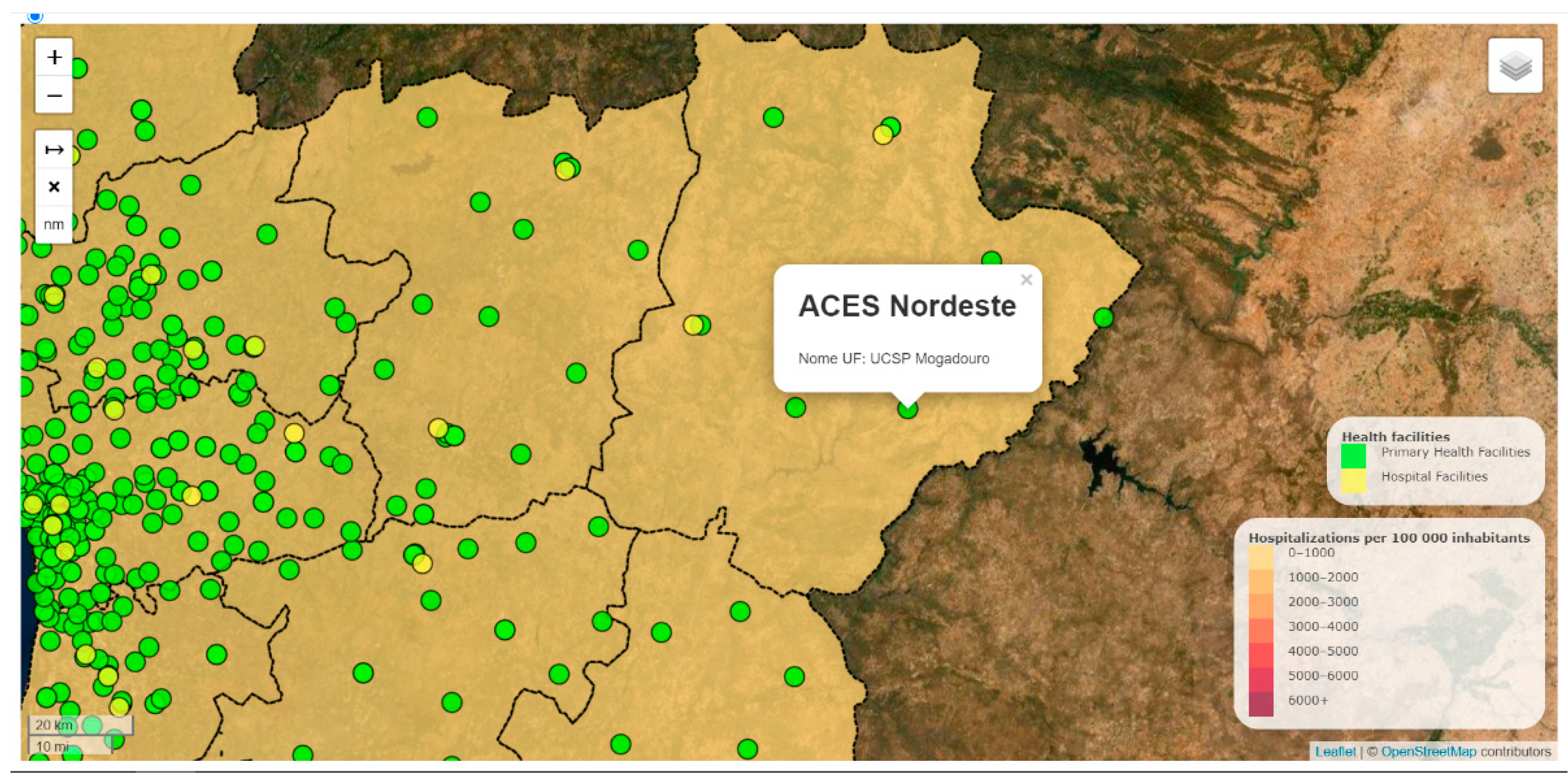
3.2. Web Map
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Muenchow, J.; Schäfer, S.; Krüger, E. Reviewing qualitative GIS research—Toward a wider usage of open-source GIS and reproducible research practices. Geogr. Compass 2019, 13, e12441. [Google Scholar] [CrossRef]
- Khan, M.A.; UrRehman, F. Free and Open Source Software: Evolution, Benefits and Characteristics. Int. J. Emerg. Trends Technol. Comput. Sci. 2012, 1, 1–7. [Google Scholar]
- Chand, J. Free and Open Source Software’s for Geographic Information System (GIS). Available online: https://1library.net/document/y4386v9z-free-open-source-software-s-geographic-information-gis.html?utm_source=related_list (accessed on 30 March 2021).
- Richard Satllman. Available online: https://stallman.org/ (accessed on 30 March 2021).
- Jayawardhana, U.K.; Gorsevski, P.V. An ontology-based framework for extracting spatio-temporal influenza data using Twitter. Int. J. Digit. Earth 2017, 12, 2–24. [Google Scholar] [CrossRef]
- AHRQ Quality Indicators. Guide to Prevention Quality Indicators: Hospital Admission for Ambulatory Care Sensitive Conditions. Available online: https://www.qualityindicators.ahrq.gov/modules/pqi_overview.aspx (accessed on 10 January 2020).
- Helmer, D.A.; Tseng, C.-L.; Brimacombe, M.; Rajan, M.; Stiptzarov, N.; Pogach, L. Applying diabetes-related Prevention Quality Indicators to a national cohort of veterans with diabetes. Diabetes Care 2003, 26, 3017–3023. [Google Scholar] [CrossRef] [Green Version]
- Manzoli, L.; Flacco, M.E.; De Vito, C.; Arcà, S.; Carle, F.; Capasso, L.; Marzuillo, C.; Muraglia, A.; Samani, F.; Villari, P. AHRQ prevention quality indicators to assess the quality of primary care of local providers: A pilot study from Italy. Eur. J. Public Health 2014, 24, 745–750. [Google Scholar] [CrossRef] [Green Version]
- Rocha, J.V.M.; Nunes, C.; Santana, R. Avoidable hospitalizations in Brazil and Portugal: Identifying and comparing critical areas through spatial analysis. PLoS ONE 2019, 14, e0219262. [Google Scholar] [CrossRef] [PubMed]
- Kelen, P.T.V.; Downs, J.A.; Stark, L.M.; Loraamm, R.W.; Andreson, J.H.; Unnasch, T.R. Spatial epidemiology of eastern equine encephalitis in Florida. Int. J. Health Geogr. 2012, 11, 47. [Google Scholar] [CrossRef] [Green Version]
- Veenendaal, B.; Brovelli, M.A.; Li, S. Review of Web Mapping: Eras, Trends and Directions. ISPRS Int. J. Geo Inf. 2017, 6, 317. [Google Scholar] [CrossRef]
- Franch-Pardo, I.; Napoletano, B.M.; Rosete-Verges, F.; Billa, L. Spatial analysis and GIS in the study of COVID-19. A review. Sci. Total Environ. 2020, 739, 140033. [Google Scholar] [CrossRef]
- Dubowitz, T.D.; Williams, M.; Steiner, E.D.; Weden, M.M.; Miyashiro, L.; Jacobson, D.; Lurie, N. Using Geographic Infor-mation Systems to Match Local Health Needs With Public Health Services and Programs. Am. J. Public Health 2011, 101, 1664–1665. [Google Scholar] [CrossRef]
- Dulin, M.F.; Ludden, T.M.; Tapp, H.; Blackwell, J.; de Hernandez, B.U.; Smith, H.A.; Furuseth, O.J. Using Geographic Infor-mation Systems (GIS) to Understand a Community’s Primary Care Needs. J. Am. Board Family Med. 2010, 23, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Shaw, N.; McGuire, S. Understanding the use of geographical information systems (GIS) in health informatics research: A review. J. Innov. Health Inf. 2017, 24, 228–233. [Google Scholar] [CrossRef]
- Alvarez-Mendoza, C.I.; Teodoro, A.C.; Torres, N.; Vivanco, V. Assessment of Remote Sensing Data to Model PM10 Estimation in Cities with a Low Number of Air Quality Stations: A Case of Study in Quito, Ecuador. Environments 2019, 6, 85. [Google Scholar] [CrossRef] [Green Version]
- GIS & Mapping for Public Health: Mapping Websites & Applications. Available online: https://guides.lib.berkeley.edu/publichealth/phgis/mapping (accessed on 1 July 2020).
- Centers for Disease Control and Prevention. Available online: https://nccd.cdc.gov/cdi/rdPage.aspx?rdReport=DPH_CDI.ExploreByTopic&islTopic=AST&islYear=9999&go=GO (accessed on 1 July 2020).
- GEOSAUDE. Available online: http://www.geosaude.dgs.pt/ (accessed on 1 July 2020).
- PORDATA. Available online: https://www.pordata.pt/ (accessed on 1 July 2020).
- Instituto Nacional de Estatística (INE). Available online: Ine.pt (accessed on 1 July 2020).
- BI-CSP. Available online: https://bicsp.min-saude.pt/pt/Paginas/default.aspx (accessed on 1 July 2020).
- Administração Central do Sistema de Saúde, IP. Available online: https://benchmarking-acss.min-saude.pt/ (accessed on 1 July 2020).
- Serviço Nacional de Saúde (Health Nacional Service). Available online: https://www.sns.gov.pt/transparencia/ (accessed on 30 March 2021).
- Eurostat. Income Poverty Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Income_poverty_statistics (accessed on 1 July 2020).
- Campos-Matos, I.; Russo, G.; Perelman, J. Connecting the dots on health inequalities—A systematic review on the social determinants of health in Portugal. Int. J. Equity Health 2016, 15, 26. [Google Scholar] [CrossRef] [Green Version]
- Dimitrovová, K.; Costa, C.; Santana, P.; Perelman, J. Evolution and financial cost of socioeconomic inequalities in ambulatory care sensitive conditions: An ecological study for Portugal, 2000–2014. Int. J. Equity Health 2017, 16, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AHRQ. Agency for Healthcare Research and Quality, “Prevention Quality Indicators Technical Specifications Updates—Version 6.0 (ICD-9-CM). Available online: https://www.qualityindicators.ahrq.gov/Archive/PQI_TechSpec_ICD09_v60.aspx (accessed on 10 April 2020).
- AHRQ. Agency for Healthcare Research and Quality, “Prevention Quality Indicators Technical Specifications Updates—Version v2018.0.1. Available online: https://www.qualityindicators.ahrq.gov/Archive/PQI_TechSpec_ICD10_v60.aspx (accessed on 10 April 2020).
- ACSS. Administração Central do Sistema de Saúde. Available online: http://www.acss.min-saude.pt/ (accessed on 1 March 2020).
- Freitas, A.; Gaspar, J.; Rocha, N.; Marreiros, G.; Da Costa-Pereira, A. Quality in Hospital Administrative Databases. Appl. Math. Inf. Sci. 2014, 8, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Sarmento, J.; Rocha, J.V.M.; Santana, R. Defining ambulatory care sensitive conditions for adults in Portugal. BMC Health Serv. Res. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Ramalho, A.; Lobo, M.; Duarte, L.; Souza, J.; Santos, P.; Freitas, A. Landscapes on Prevention Quality Indicators: A Spatial Analysis of Diabetes Preventable Hospitalizations in Portugal (2016–2017). Int. J. Environ. Res. Public Health 2020, 17, 8387. [Google Scholar] [CrossRef]
- DGT. Direção Geral do Território. Available online: http://www.dgterritorio.pt/ (accessed on 10 March 2020).
- PostGIS. Spatial and Geographic Objects for PostgreSQL. Available online: https://postgis.net/ (accessed on 10 January 2020).
- QGIS. Welcome to the QGIS Project! Qgis. 2016. Available online: http://www.qgis.org/ (accessed on 25 September 2020).
- Duarte, L.; Lobo, M.; Viana, J.; Freitas, A.; Teodoro, A. A GIS Open Source Application to Perform the Spatial Distribution of Prevention Quality Indicators (PQIs). In Proceedings of the 6th International Conference on Geographical Information Systems Theory, Applications and Management, Prague, Czech Republic, 7–9 May 2020; Volume 1, pp. 129–134. [Google Scholar]
- Qt Documentation. Available online: https://doc.qt.io/qt-5/reference-overview.html (accessed on 23 March 2020).
- PyQGIS Developer Cookbook. Available online: https://docs.qgis.org/testing/en/docs/pyqgis_developer_cookbook/ (accessed on 23 March 2020).
- MatPlotLib. Available online: https://matplotlib.org/ (accessed on 25 September 2020).
- Bhatia, T.S.; Singh, H.; Litoria, P.K.; Pateriya, B. Web GIS Development using Open Source Leaflet and Geoserver Toolkit. IJCST 2018, 9, 29–33. [Google Scholar]
- Horbiński, T.; Lorek, D. The use of Leaflet and GeoJSON files for creating the interactive web map of the preindustrial state of the natural environment. J. Spat. Sci. 2020, 1–17. [Google Scholar] [CrossRef]
- Apeh, O.I.; Nwaka, O.C.; Ndukwu, R.I.; Maduako, I.; Arilewola, O. E-beacon: A web-based survey control finder application. S. Afr. J. Geomat. 2019, 8, 178–190. [Google Scholar]
- Kim, J. Web-based Geovisualization System of Oceanographic Information using Dynamic particles and HTML5. J. Coast. Res. 2018, 85, 1491. [Google Scholar] [CrossRef]
- Olyazadeh, R.; Sudmeier-Rieux, K.; Jaboyedoff, M.; Derron, M.-H.; Devkota, S. An offline–onlineWeb-GIS Android application for fast data acquisition of landslide hazard and risk. Nat. Hazards Earth Syst. Sci. 2017, 17, 549–561. [Google Scholar] [CrossRef] [Green Version]
- Tayebi, A.; Gomez, J.; De Adana, F.S.; Gutierrez, O.; De Sevilla, M.F. Development of a Web-Based Simulation Tool to Estimate the Path Loss in Outdoor Environments using OpenStreetMaps [Wireless Corner]. IEEE Antennas Propag. Mag. 2019, 61, 123–129. [Google Scholar] [CrossRef]
- JavaScript. Available online: https://www.javascript.com/ (accessed on 10 March 2020).
- Farkas, G. Applicability of open-source web mapping libraries for building massive Web GIS clients. J. Geogr. Syst. 2017, 19, 273–295. [Google Scholar] [CrossRef]
- Leaflet. Leaflet—A JavaScript Library for Interactive Maps. Available online: http://leafletjs.com/ (accessed on 25 September 2020).
- Geoserver. Geoserver. Available online: http://geoserver.org/ (accessed on 14 March 2020).
- Switch2OSM. Available online: https://switch2osm.org/using-tiles/getting-started-with-leaflet/ (accessed on 23 March 2020).
- ArcGIS. Available online: https://www.esri.com/en-us/arcgis/about-arcgis/overview (accessed on 23 March 2021).
- WHOROE (World Health Organization Regional Office for Europe). Assessing Health Services Delivery Performance with Hospitalizations for Ambulatory Care Sensitive Conditions. Available online: https://www.euro.who.int/__data/assets/pdf_file/0010/305875/Assessing-HSD-performance-with-ACSH.pdf (accessed on 1 July 2020).
- McLafferty, S.L. GIS and Health Care. Annu. Rev. Public Health 2003, 24, 25–42. [Google Scholar] [CrossRef]
- Jack, K.; Holt, M. Community profiling as part of a health needs assessment. Nurs. Stand. 2008, 22, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, C. Hospitalisation of ambulatory care sensitive conditions and access to primary care in Portugal. Public Health 2018, 165, 117–124. [Google Scholar] [CrossRef]
- Santos, J.V.; Viana, J.; Souza, J.; Lobo, M.; Ramalho, A.; Gonçalves-Pinho, M.; Freitas, A. Time trends of primary care quality across Portuguese regions: Using prevention quality indicators. Eur. J. Public Health 2019, 29, ckz186–ckz383. [Google Scholar] [CrossRef] [Green Version]
- Alonso, V.; Santos, J.V.; Pinto, M.; Ferreira, J.; Lema, I.; Lopes, F.; Freitas, A. Problems and Barriers in the Transition to ICD-10-CM/PCS: A Qualitative Study of Medical Coders’ Perceptions. In Proceedings of the World Conference on Information Systems and Technologies; Springer: Cham, Switzerland, 2019; pp. 72–82. [Google Scholar] [CrossRef]
- Paramasivam, C. Merits and Demerits of GIS and Geostatistical Techniques. Available online: https://www.researchgate.net/publication/333510563_Merits_and_Demerits_of_GIS_and_Geostatistical_Techniques (accessed on 23 March 2021).
- Stevens, R.; Ahmedzai, S.H.; Hughes, P.; Noble, B.; Ahmed, N. Geographical Information Systems (GIS) in Palliative Care: A Systematic Review; University of Sheffield: Sheffield, UK, 2010. [Google Scholar]
- Van Loenen, T.; Berg, M.J.V.D.; Westert, G.P.; Faber, M.J. Organizational aspects of primary care related to avoidable hospitalization: A systematic review. Fam. Pract. 2014, 31, 502–516. [Google Scholar] [CrossRef]
- Olvingson, C.; Hallberg, J.; Timpka, T.; Lindqvist, K. Ethical issues in public health informatics: Implications for system design when sharing geographic information. J. Biomed. Inf. 2002, 35, 178–185. [Google Scholar] [CrossRef] [Green Version]
- Tranmer, M.; Pickles, A.; Fieldhouse, E.; Elliot, M.; Dale, A.; Brown, M.; Martin, D.; Steel, D.; Gardiner, C. The case for small area microdata. J. R. Stat. Soc. Ser. A Stat. Soc. 2004, 168, 29–49. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PQI Code | Description |
|---|---|
| PQI01 | Diabetes Short-Term Complications |
| PQI02 | Perforated Appendix |
| PQI03 | Diabetes Long-Term Complications |
| PQI05 | COPD or Asthma in Older Adults |
| PQI07 | Hypertension |
| PQI08 | Heart Failure |
| PQI09 | Low Birth Weight |
| PQI10 | Dehydration |
| PQI11 | Bacterial Pneumonia |
| PQI12 | Urinary Tract Infection |
| PQI14 | Uncontrolled Diabetes |
| PQI15 | Asthma in Younger Adults |
| PQI16 | Lower-Extremity Amputation Among Patients with Diabetes |
| PQI90 | Prevention Quality Overall Composite |
| PQI91 | Prevention Quality Acute Composite (PQI11, PQI12) |
| PQI92 | Prevention Quality Chronic Composite (PQI1, PQI3, PQI5, PQI7, PQI8, PQI14, PQI15, PQI16) |
| PQI93 | Prevention Quality Diabetes Composite (PQI1, PQI3, PQI14, PQI16) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duarte, L.; Teodoro, A.C.; Lobo, M.; Viana, J.; Pinheiro, V.; Freitas, A. An Open Source GIS Application for Spatial Assessment of Health Care Quality Indicators. ISPRS Int. J. Geo-Inf. 2021, 10, 264. https://doi.org/10.3390/ijgi10040264
Duarte L, Teodoro AC, Lobo M, Viana J, Pinheiro V, Freitas A. An Open Source GIS Application for Spatial Assessment of Health Care Quality Indicators. ISPRS International Journal of Geo-Information. 2021; 10(4):264. https://doi.org/10.3390/ijgi10040264
Chicago/Turabian StyleDuarte, Lia, Ana Cláudia Teodoro, Mariana Lobo, João Viana, Vera Pinheiro, and Alberto Freitas. 2021. "An Open Source GIS Application for Spatial Assessment of Health Care Quality Indicators" ISPRS International Journal of Geo-Information 10, no. 4: 264. https://doi.org/10.3390/ijgi10040264
APA StyleDuarte, L., Teodoro, A. C., Lobo, M., Viana, J., Pinheiro, V., & Freitas, A. (2021). An Open Source GIS Application for Spatial Assessment of Health Care Quality Indicators. ISPRS International Journal of Geo-Information, 10(4), 264. https://doi.org/10.3390/ijgi10040264