Winter Is Coming: A Socio-Environmental Monitoring and Spatiotemporal Modelling Approach for Better Understanding a Respiratory Disease


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Spatial and Spatiotemporal Patterns
2.3. Correlations, Similarities, and Clustering
2.4. Geographically Weighted Poisson Regression
3. Results
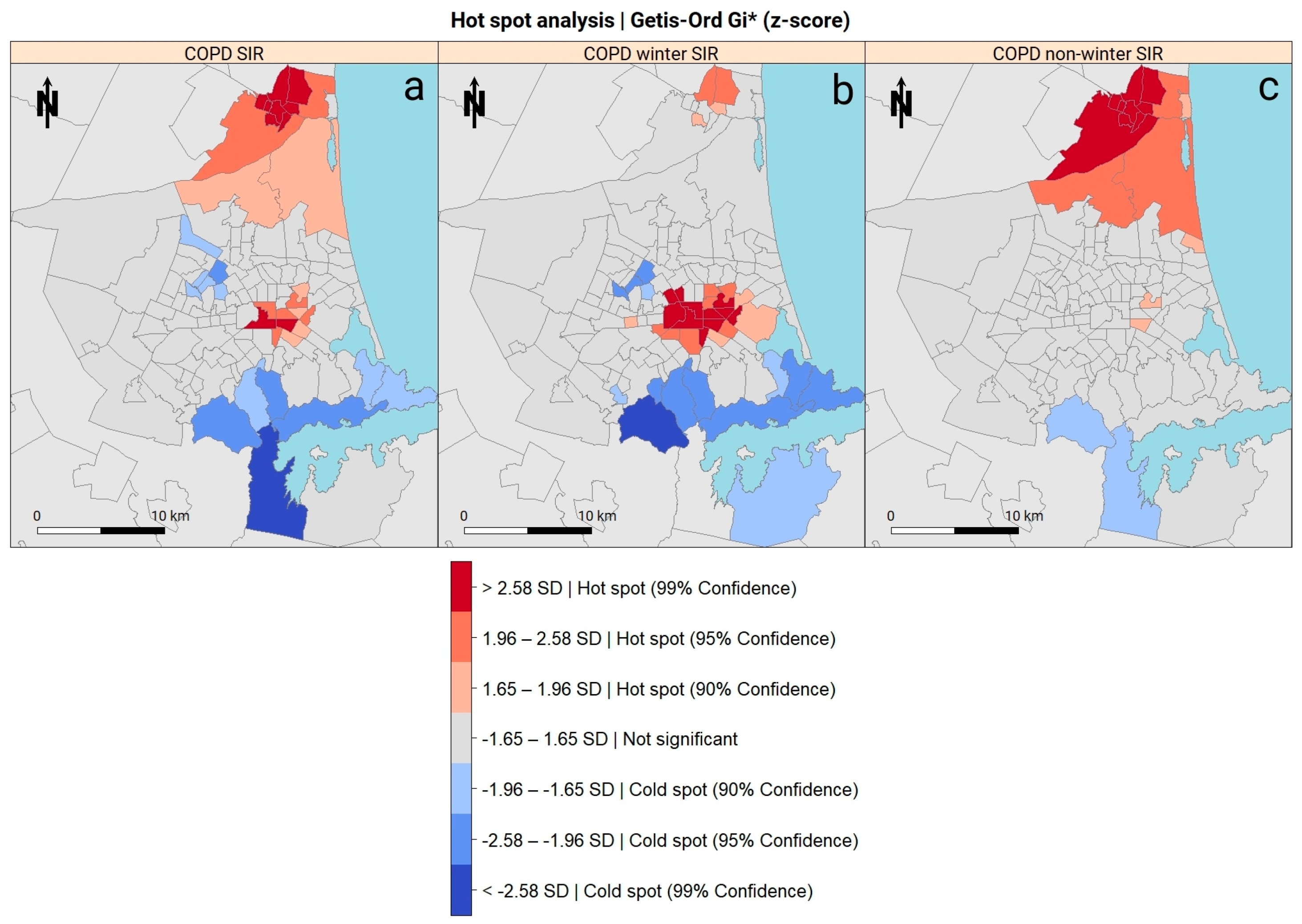
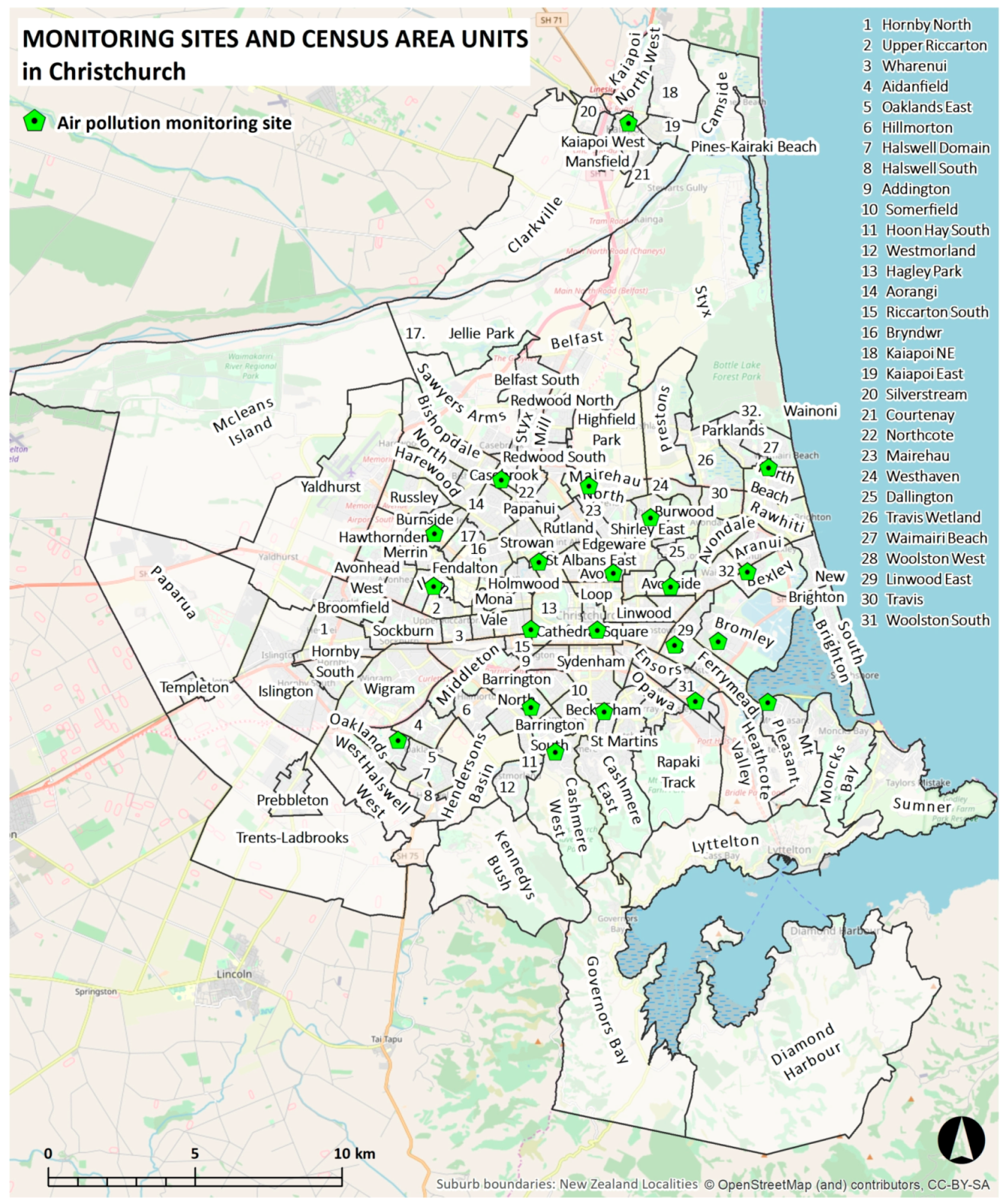
3.1. Mapping
3.2. Spatial and Spatio-Temporal Patterns
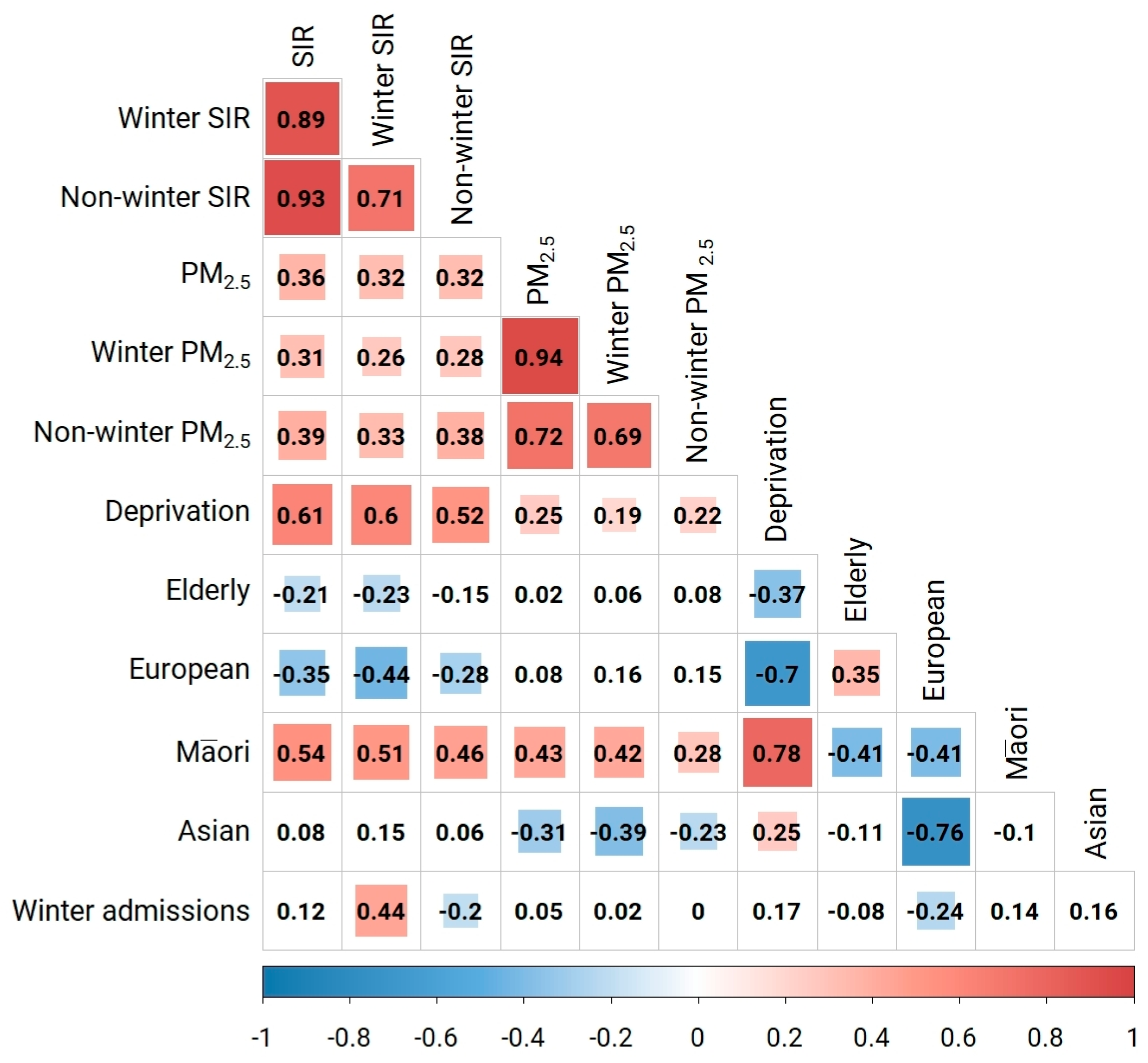
3.3. Correlations and Similarities
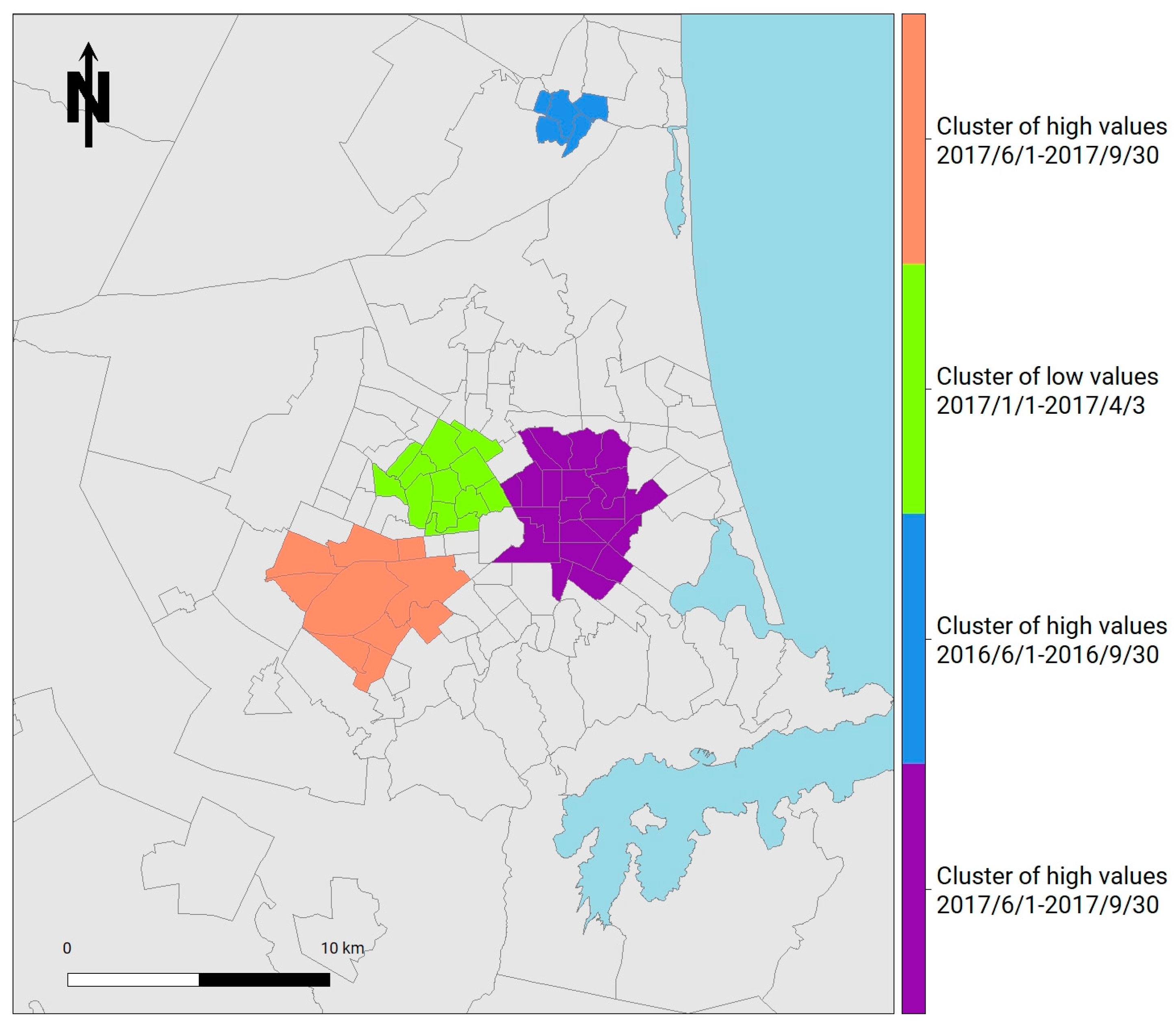
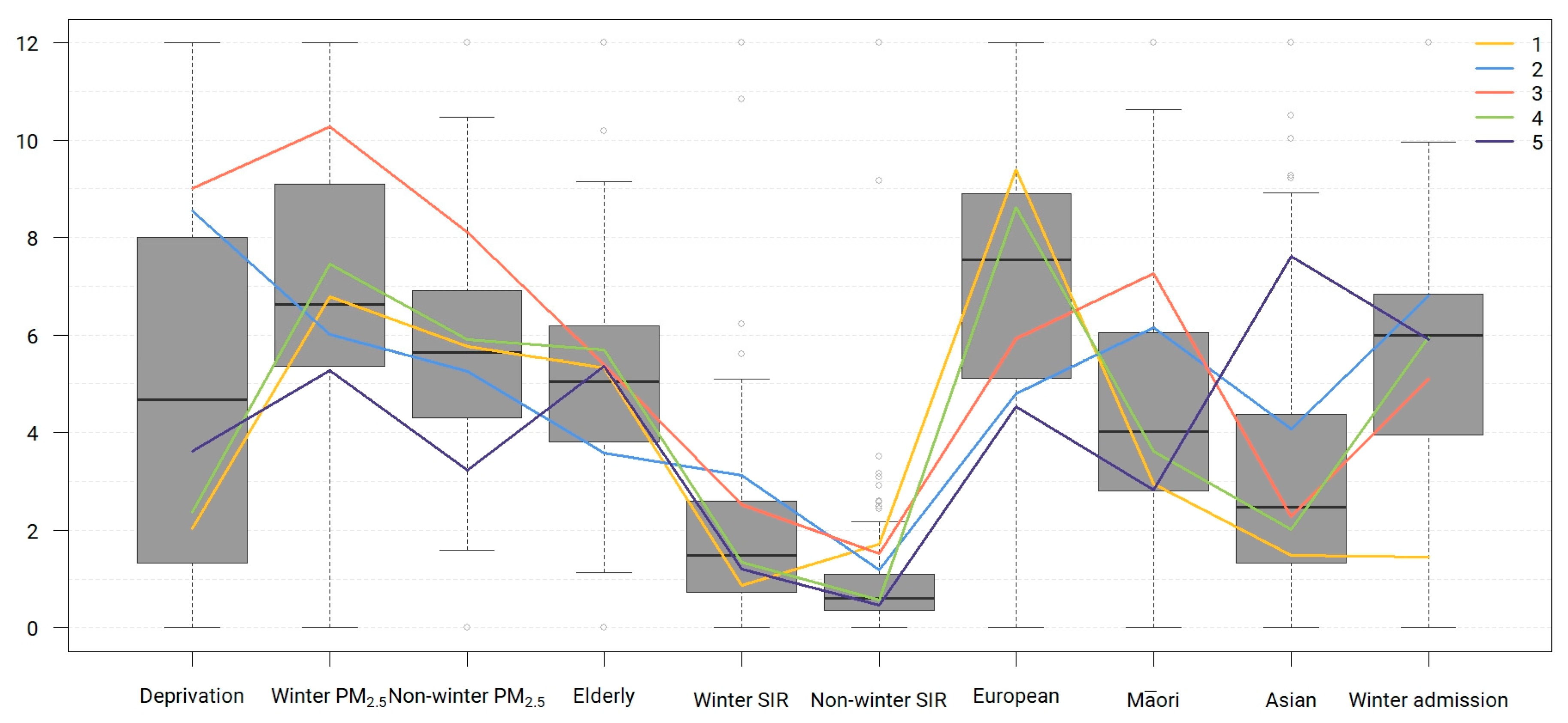
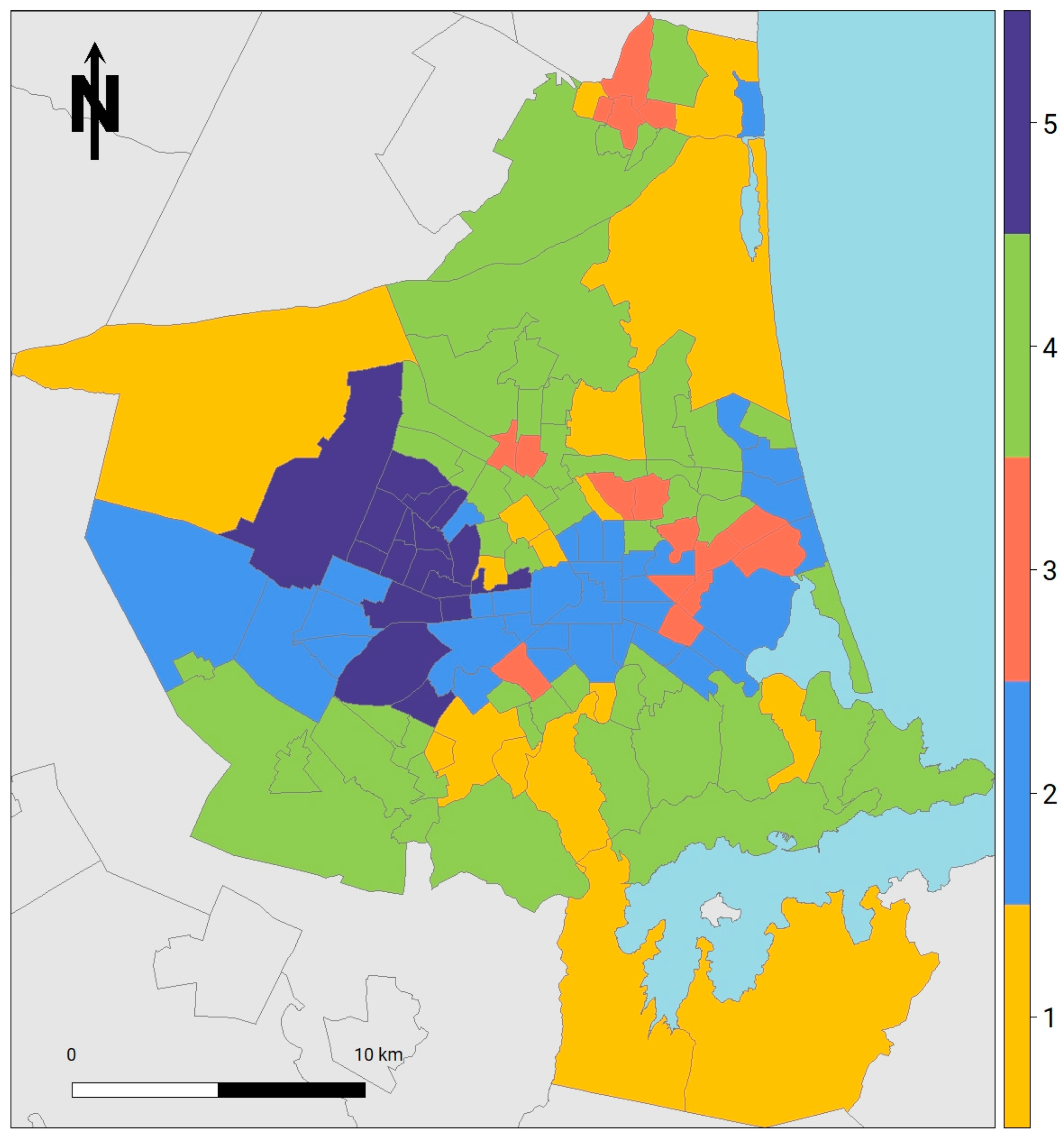
3.4. Clustering
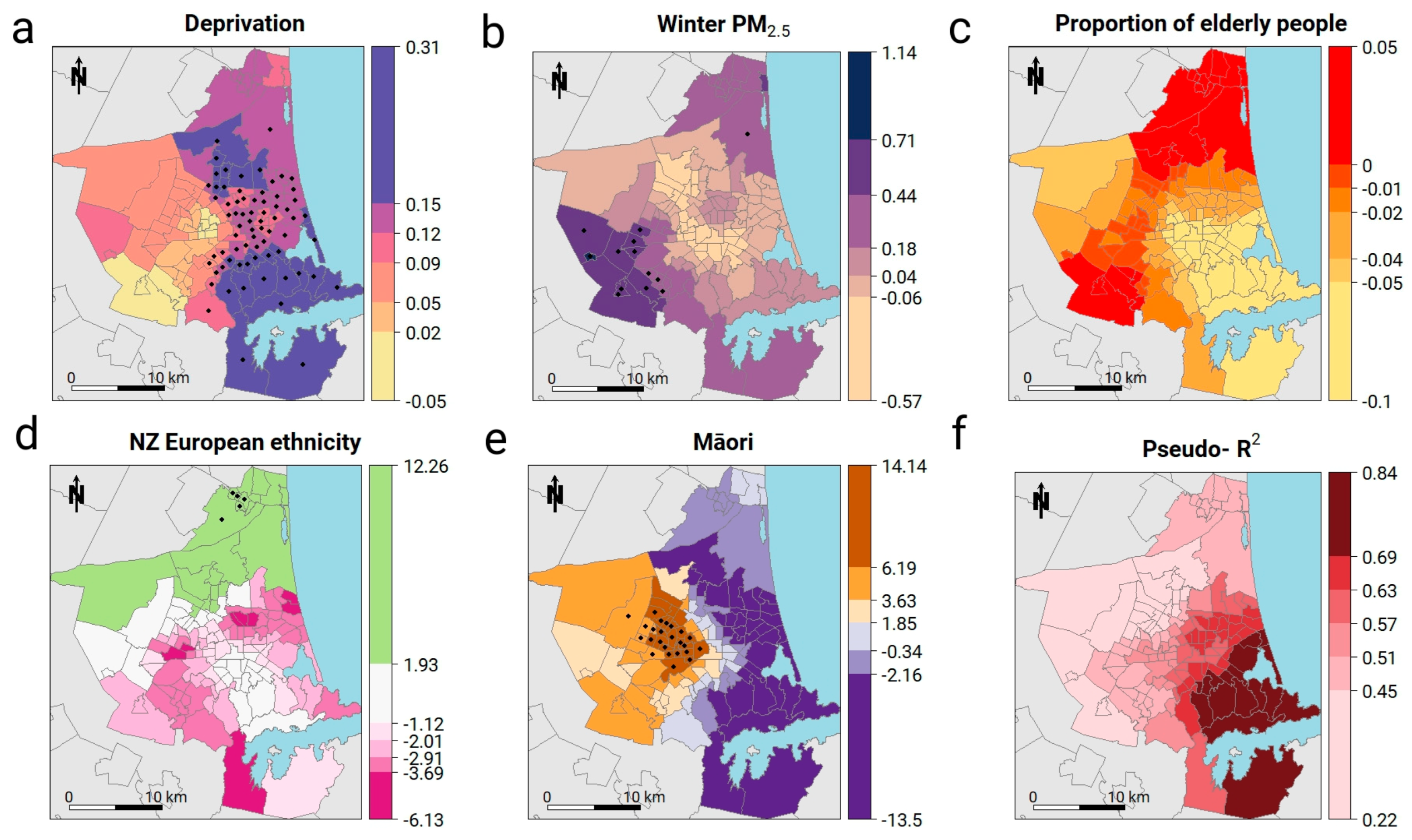
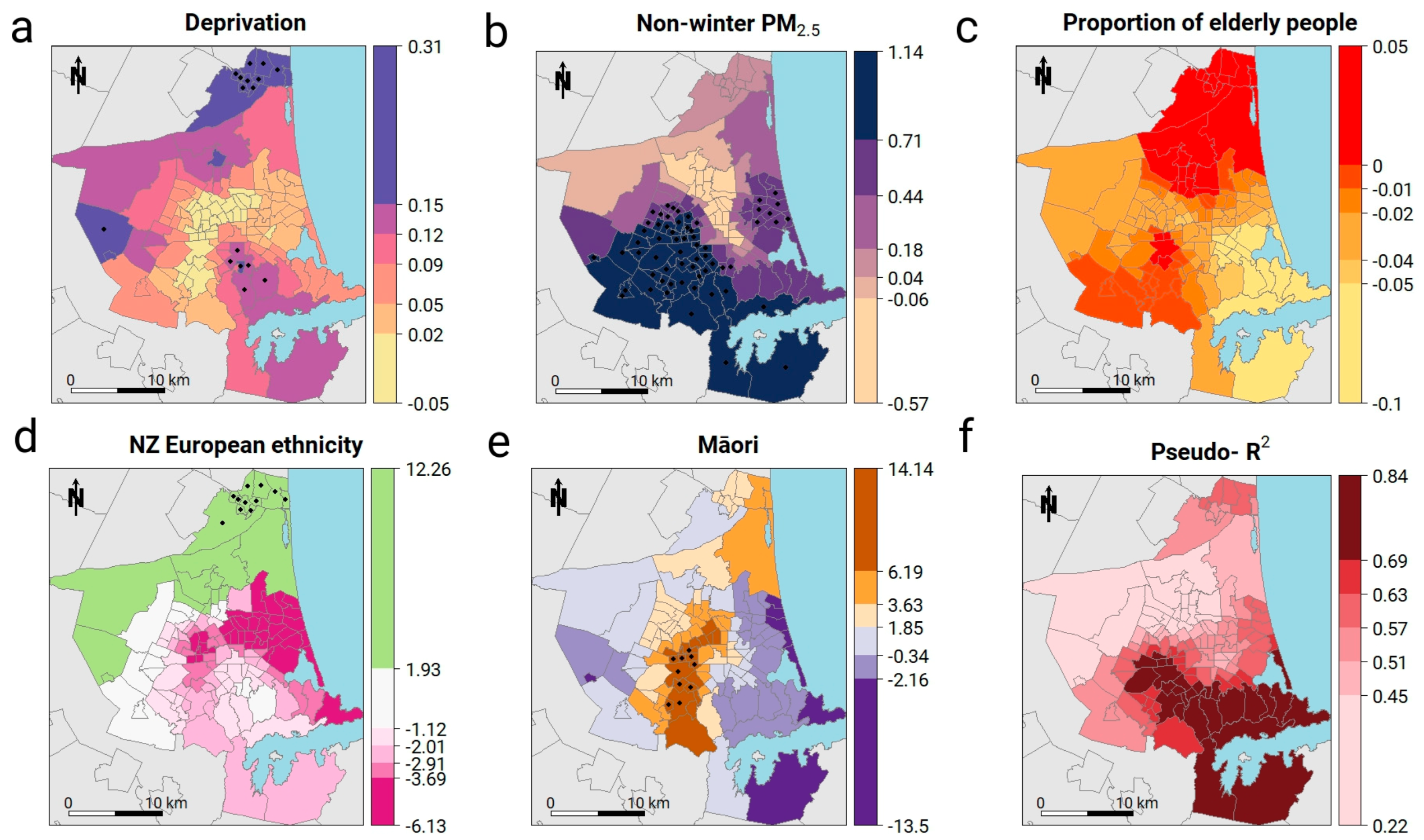
3.5. Geographically Weighted Poisson Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 (n = 17) | Group 2 (n = 34) | Group 3 (n = 16) | Group 4 (n = 48) | Group 5 (n = 17) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | Mean | SD | Median | Mean | SD | Median | Mean | SD | Median | Mean | SD | Median | |
| Deprivation | 2.53 | 1.94 | 1.00 | 7.41 | 1.02 | 7.00 | 7.75 | 1.24 | 8.00 | 2.77 | 1.48 | 2.50 | 3.71 | 1.96 | 3.00 |
| PM2.5 winter | 9.21 | 0.86 | 9.24 | 8.92 | 0.81 | 8.98 | 10.54 | 0.41 | 10.52 | 9.46 | 0.78 | 9.47 | 8.63 | 0.35 | 8.65 |
| PM2.5 non-winter | 5.54 | 0.33 | 5.44 | 5.44 | 0.23 | 5.43 | 5.98 | 0.32 | 5.92 | 5.56 | 0.32 | 5.57 | 5.07 | 0.27 | 5.08 |
| Elderly proportion | 16.02 | 4.10 | 15.38 | 11.74 | 3.96 | 11.48 | 16.18 | 3.46 | 16.66 | 16.91 | 4.21 | 16.46 | 16.08 | 3.15 | 16.26 |
| SIR winter | 0.71 | 2.13 | 0.00 | 2.57 | 1.72 | 2.24 | 2.07 | 0.89 | 2.06 | 1.11 | 0.66 | 0.96 | 0.98 | 0.88 | 0.62 |
| SIR non-winter | 1.65 | 3.31 | 0.58 | 1.15 | 0.83 | 0.94 | 1.47 | 0.91 | 1.25 | 0.55 | 0.33 | 0.47 | 0.46 | 0.29 | 0.42 |
| European | 0.91 | 0.04 | 0.89 | 0.74 | 0.08 | 0.75 | 0.78 | 0.07 | 0.78 | 0.88 | 0.03 | 0.88 | 0.73 | 0.05 | 0.75 |
| Māori | 0.05 | 0.03 | 0.05 | 0.11 | 0.03 | 0.11 | 0.13 | 0.03 | 0.13 | 0.06 | 0.02 | 0.07 | 0.05 | 0.01 | 0.05 |
| Asian | 0.04 | 0.03 | 0.04 | 0.10 | 0.06 | 0.09 | 0.06 | 0.04 | 0.06 | 0.05 | 0.03 | 0.04 | 0.19 | 0.04 | 0.19 |
| Winter admissions | 0.12 | 0.14 | 0.00 | 0.57 | 0.17 | 0.54 | 0.42 | 0.14 | 0.43 | 0.50 | 0.11 | 0.50 | 0.49 | 0.15 | 0.53 |
References
- Milne, R.J.; Beasley, R.; Milne, R.J.; Beasley, R. Hospital admissions for chronic obstructive pulmonary disease in New Zealand. N. Z. Med. J. 2014, 128, 23–35. [Google Scholar]
- Pauwels, R.A.; Buist, A.S.; Calverley, P.M.A.; Jenkins, C.R.; Hurd, S.S. NHLBI/WHO Workshop Summary Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop Summary. Am. J. Respir. Crit. Care Med. 2012, 163, 1256–1276. [Google Scholar] [CrossRef] [PubMed]
- Bentayeb, M.; Simoni, M.; Baiz, N.; Norback, D.; Baldacci, S.; Maio, S.; Viegi, G.; Annesi-Maesano, I. Geriatric Study in Europe on Health Effects of Air Quality in Nursing Homes Group. Adverse respiratory effects of outdoor air pollution in the elderly. Int. J. Tuberc. Lung Dis. 2012, 16, 1149–1161. [Google Scholar] [CrossRef] [PubMed]
- Ko, F.W.S.; Hui, D.S.C. Air pollution and chronic obstructive pulmonary disease. Respirology 2012, 17, 395–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.; Zhou, Y.; Liu, S.; Chen, X.; Zou, W.; Zhao, D.; Li, X.; Pu, J.; Huang, L.; Chen, J.; et al. Association between exposure to ambient particulate matter and chronic obstructive pulmonary disease: Results from a cross-sectional study in China. Thorax 2017, 72, 788–795. [Google Scholar] [CrossRef] [PubMed]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA 2006, 295, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, A.; Bind, M.-A.C.; Schwartz, J. Particulate air pollution and survival in a COPD cohort. Environ. Health 2008, 7, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raherison, C.; Girodet, P.O. Epidemiology of COPD. Eur. Respir. Rev. 2009, 18, 213–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, T.-C.; Chiang, P.H.; Su, M.D.; Wang, H.W.; Liu, M.S.Y. Geographic disparity in chronic obstructive pulmonary disease (COPD) mortality rates among the Taiwan population. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, G.; Wedzicha, J. The causes and consequences of seasonal variation in COPD exacerbations. Int. J. Chronic Obstr. Pulm. Dis. 2014, 39, 1101. [Google Scholar] [CrossRef] [PubMed]
- McAllister, D.A.; Morling, J.R.; Fischbacher, C.M.; MacNee, W.; Wild, S.H. Socioeconomic deprivation increases the effect of winter on admissions to hospital with COPD: Retrospective analysis of 10 years of national hospitalisation data. Prim. Care Respir. J. 2013, 22, 296–299. [Google Scholar] [CrossRef] [PubMed]
- McCormack, M.C.; Paulin, L.M.; Gummerson, C.E.; Peng, R.D.; Diette, G.B.; Hansel, N.N. Colder temperature is associated with increased COPD morbidity. Eur. Respir. J. 2017, 49, 1601501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halbert, R.J.; Natoli, J.L.; Gano, A.; Badamgarav, E.; Buist, A.S.; Mannino, D.M. Global burden of COPD: Systematic review and meta-analysis. Eur. Respir. J. 2006, 28, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Calderon-Larranaga, A.; Carney, L.; Soljak, M.; Bottle, A.; Partridge, M.; Bell, D.; Abi-Aad, G.; Aylin, P.; Majeed, A. Association of population and primary healthcare factors with hospital admission rates for chronic obstructive pulmonary disease in England: National cross-sectional study. Thorax 2011, 66, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Lamprecht, B.; McBurnie, M.A.; Vollmer, W.M.; Gudmundsson, G.; Welte, T.; Nizankowska-Mogilnicka, E.; Studnicka, M.; Bateman, E.; Anto, J.M.; Burney, P.; et al. COPD in never smokers: Results from the population-based burden of obstructive lung disease study. Chest 2011, 139, 752–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, T.-C.; Wang, H.-W.; Tseng, T.-J.; Chiang, P.-H. Spatial Clustering and Local Risk Factors of Chronic Obstructive Pulmonary Disease (COPD). Int. J. Environ. Res. Public Health 2015, 12, 15716–15727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crighton, E.J.; Ragetlie, R.; Luo, J.; To, T.; Gershon, A. A spatial analysis of COPD prevalence, incidence, mortality and health service use in Ontario. Health Rep. 2015, 26, 10–18. [Google Scholar] [PubMed]
- Hnizdo, E.; Sullivan, P.A.; Bang, K.M.; Wagner, G. Airflow obstruction attributable to work in industry and occupation among U.S. race/ethnic groups: A study of NHANES III data. Am. J. Ind. Med. 2004, 46, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, T.; Martinussen, P.E. The geography of chronic obstructive pulmonary disease: A population-based study of Norway. Soc. Sci. Med. 2014, 111, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.; Kingham, S.; Zawar-Reza, P. Every breath you take? Environmental justice and air pollution in Christchurch, New Zealand. Environ. Plan. A 2006, 38, 919–938. [Google Scholar] [CrossRef]
- Lipton, R.; Banerjee, A.; Dowling, K.C.; Treno, A.J. The geography of COPD hospitalization in California. COPD J. Chronic Obstr. Pulm. Dis. 2005, 2, 435–444. [Google Scholar] [CrossRef]
- Lipton, R.; Banerjee, A. The geography of chronic obstructive pulmonary disease across time: California in 1993 and 1999. Int. J. Med. Sci. 2007, 4, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Fisk, W.J.; Lei-Gomez, Q.; Mendell, M.J. Meta-analyses of the associations of respiratory health effects with dampness and mold in homes. Indoor Air 2007, 17, 284–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrett, M.H.; Rayment, P.R.; Hooper, M.A.; Abramson, M.J.; Hooper, B.M. Indoor airborne fungal spores, house dampness and associations with environmental factors and respiratory health in children. Clin. Exp. Allergy 1998, 28, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Statistics New Zealand. Estimated Resident Population for Territorial Authority Areas at 30 June (1996+) (Annual-Jun); Statistics New Zealand: Wellington, New Zealand, 2017; p. 4.
- World Health Organization. WHO Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide: Global Update 2005: Summary of Risk Assessment; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Behrendt, C.E. Mild and moderate-to-severe COPD in nonsmokers: Distinct demographic profiles. Chest 2005, 128, 1239–1244. [Google Scholar] [CrossRef] [PubMed]
- Peruzza, S.; Sergi, G.; Vianello, A.; Pisent, C.; Tiozzo, F.; Manzan, A.; Coin, A.; Inelmen, E.M.; Enzi, G. Chronic obstructive pulmonary disease (COPD) in elderly subjects: Impact on functional status and quality of life. Respir. Med. 2003, 97, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Wakefield, J.C.; Best, N.G.; Briggs, D.J. Spatial Epidemiology: Methods and Applications; Oxford University Press: Oxford, UK, 2000. [Google Scholar]
- Atkinson, J.; Salmond, C.; Crampton, P. NZDep2013 Index of Deprivation; Department of Public Health, University of Otago: Wellington, New Zealand, 2014. [Google Scholar]
- Marek, L.; Campbell, M.; Bui, L. Shaking for innovation: The (re)building of a (smart) city in a post disaster environment. Cities 2017, 63, 41–50. [Google Scholar] [CrossRef]
- Marek, L.; Campbell, M.; Epton, M.; Storer, M.; Kingham, S. Real-time environmental sensors to improve health in the Sensing City. ISPRS Int. Arch. Photogramm. Remote Sens. Spat. Inf. Sci. 2016, XLI-B2, 729–733. [Google Scholar] [CrossRef]
- Gräler, B.; Gerharz, L.; Pebesma, E. Spatio-Temporal Analysis and Interpolation of PM10 Measurements in Europe; ETC/ACM Technical Paper 2011/10; ETC/ACM: Bilthoven, The Netherlands, 2011; p. 37. [Google Scholar]
- Graler, B.; Pebesma, E.; Heuvelink, G. Spatio-Temporal Interpolation using gstat. R J. 2016, 8, 204–218. [Google Scholar]
- Getis, A.; Ord, J.K. The Analysis of Spatial Association by Use of Distance Statistics. Geogr. Anal. 1992, 24, 189–206. [Google Scholar] [CrossRef]
- Pfeiffer, D.U.; Stevenson, M.D.; Robinson, T.; Rogers, D. Spatial Analysis in Epidemiology; Oxford University Press: Oxford, UK, 2008; ISBN 978-0-19-850988-2. [Google Scholar]
- Bivand, R.S.; Altman, M.; Anselin, L.; Assunção, R.; Berke, O.; Bernat, A.; Blanchet, G.; Blankmeyer, E.; Carvalho, M.; Christensen, B.; et al. spdep: Spatial Dependence: Weighting Schemes, Statistics and Models; R-Package Version 0.7-4. 2017. Available online: https://CRAN.R-project.org/package=spdep (accessed on 5 October 2018).
- Kulldorff, M. Information Management Services Inc SaTScan v9.3: Software for the Spatial and Space-Time Scan Statistics; StatScan: Boston, MA, USA, 2009; p. 109. [Google Scholar]
- Kleinman, K. rsatscan: Tools, Classes, and Methods for Interfacing with SaTScan Stand-Alone Software. 2015. Available online: https://CRAN.R-project.org/package=rsatscan (accessed on 5 October 2018).
- Kalogirou, S. Testing local versions of correlation coefficients. Jahrbuch für Regionalwissenschaft 2011, 32, 45–61. [Google Scholar] [CrossRef] [Green Version]
- Kalogirou, S. lctools: Local Correlation, Spatial Inequalities and Other Tools. 2015. Available online: https://CRAN.R-project.org/package=lctools (accessed on 5 October 2018).
- Pánek, J.; Pászto, V.; Marek, L. Mapping Emotions: Spatial Distribution of Safety Perception in the City of Olomouc. In The Rise of Big Spatial Data; Ivan, I., Singleton, A., Horák, J., Inspektor, T., Eds.; Springer: Cham, Switzerland, 2017; pp. 211–224. ISBN 978-3-319-45122-0. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Pearson: London, UK, 2008. [Google Scholar]
- Carvalho, A.; Albuquerque, P.; de Almeida Junior, G.; Guimaraes, R. Spatial Hierarchical clustering. Rev. Bras. Biom. 2009, 27, 411–442. [Google Scholar] [CrossRef]
- Horák, J.; Ivan, I.; Inspektor, T. Spatial hierarchy clustering (Prostorové hierarchické shlukování). In GIS Ostrava 2012; VŠB-TU Ostrava, HGF; Institut Geoinformatiky: Ostrava, Czech Republic, 2012; p. 10. [Google Scholar]
- Walesiak, M.; Dudek, A. Symulacyjna optymalizacja wyboru procedury klasyfikacyjnej dla danego typu danych—Charakterystyka problemu (Determination of optimal clustering procedure for a data set—The characterisation of the problem). Zeszyty Naukowe Uniwersytetu Szczecińskiego 2006, NR450, 636–646. [Google Scholar]
- Murtagh, F.; Legendre, P. Ward’s Hierarchical Agglomerative Clustering Method: Which Algorithms Implement Ward’s Criterion? J. Classif. 2014, 31, 274–295. [Google Scholar] [CrossRef] [Green Version]
- Alves, A.T.J.; Nobre, F.F.; Waller, L.A. Exploring spatial patterns in the associations between local AIDS incidence and socioeconomic and demographic variables in the state of Rio de Janeiro, Brazil. Spat. Spatio-Temporal Epidemiol. 2016, 17, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Fotheringham, A.S.; Brunsdon, C.; Charlton, M. Geographically Weighted Regression: The Analysis of Spatially Varying Relationships; John Wiley & Sons: Hoboken, NJ, USA, 2002; ISBN 0471496162. [Google Scholar]
- Feuillet, T.; Charreire, H.; Menai, M.; Salze, P.; Simon, C.; Dugas, J.; Hercberg, S.; Andreeva, V.A.; Enaux, C.; Weber, C.; et al. Spatial heterogeneity of the relationships between environmental characteristics and active commuting: Towards a locally varying social ecological model. Int. J. Health Geogr. 2015, 14, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Cheng, E.M.Y.; Atkinson, P.M.; Shahani, A.K. Elucidating the spatially varying relation between cervical cancer and socio-economic conditions in England. Int. J. Health Geogr. 2011, 10, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakaya, T.; Charlton, M.; Brunsdon, C.; Lewis, P.; Yao, J.; Fotheringham, A.S. Semiparametric Geographically Weighted Regression, Release 1.0.90 (GWR 4.0.90). 2015. Available online: http://gwr.maynoothuniversity.ie/gwr4-software/ (accessed on 5 October 2018).
- Bivand, R.S.; Yu, D. spgwr: Geographically Weighted Regression. R Package Version 0.6-32. 2017. Available online: https://CRAN.R-project.org/package=spgwr (accessed on 5 October 2018).
- Gollini, I.; Lu, B.; Charlton, M.; Brunsdon, C.; Harris, P. GWmodel: An R package for exploring spatial heterogeneity. J. Stat. Softw. 2015, 63, 1–50. [Google Scholar] [CrossRef]
- Nakaya, T.; Fotheringham, A.S.; Brunsdon, C.; Charlton, M. Geographically weighted Poisson regression for disease association mapping. Stat. Med. 2005, 24, 2695–2717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Wang, W.; Liu, P.; Bigham, J.M.; Ragland, D.R. Using Geographically Weighted Poisson Regression for county-level crash modeling in California. Saf. Sci. 2013, 58, 89–97. [Google Scholar] [CrossRef]
- Alin, A. Multicollinearity. Wiley Interdiscip. Rev. Comput. Stat. 2010, 2, 370–374. [Google Scholar] [CrossRef]
- Poynter, R.A. Assessing the Influence of Environment and Socio-Economics on Spatial and Temporal Patterns of COPD Hospitalisation in Christchurch: A GIS Approach; University of Canterbury: Christchurch, New Zealand, 2016. [Google Scholar]
- Harré, E.S.M.; Price, P.D.; Ayrey, R.B.; Toop, L.J.; Martin, I.R.; Town, G.I. Respiratory effects of air pollution in chronic obstructive pulmonary disease: A three month prospective study. Thorax 1997, 52, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, G.C.; Wedzicha, J.A. Deprivation, winter season, and COPD exacerbations. Prim. Care Respir. J. 2013, 22, 264–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanbari Ghozikali, M.; Heibati, B.; Naddafi, K.; Kloog, I.; Oliveri Conti, G.; Polosa, R.; Ferrante, M. Evaluation of Chronic Obstructive Pulmonary Disease (COPD) attributed to atmospheric O3, NO2, and SO2 using Air Q Model (2011-2012 year). Environ. Res. 2016, 144, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.B.; Marsh, R.L.; Upham, J.W.; Hoffman, L.R.; Smith-Vaughan, H.; Holt, D.; Toombs, M.; Byrnes, C.; Yerkovich, S.T.; Torzillo, P.J.; et al. Toward Making Inroads in Reducing the Disparity of Lung Health in Australian Indigenous and New Zealand Māori Children. Front. Pediatr. 2015, 3, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harwood, M.; Martin, P.; Reid, J. Diagnosis and management of COPD in Māori and Pacific peoples. Best Pract. J. 2012, 43, 14–25. [Google Scholar]
- Levack, W.M.M.; Weatherall, M.; Reeve, J.C.; Mans, C.; Mauro, A. Uptake of pulmonary rehabilitation in New Zealand by people with chronic obstructive pulmonary disease in 2009. N. Z. Med. J. 2012, 125, 23–33. [Google Scholar] [PubMed]
- Czarnota, J.; Wheeler, D.C.; Gennings, C. Evaluating geographically weighted regression models for environmental chemical risk analysis. Cancer Inform. 2015, 14, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, D.; Tiefelsdorf, M. Multicollinearity and correlation among local regression coefficients in geographically weighted regression. J. Geogr. Syst. 2005, 7, 161–187. [Google Scholar] [CrossRef]
- Wheeler, D.C.; Calder, C.A. An assessment of coefficient accuracy in linear regression models with spatially varying coefficients. J. Geogr. Syst. 2007, 9, 145–166. [Google Scholar] [CrossRef]
- Spronken-Smith, R.A.; Sturman, A.P.; Wilton, E. V The air pollution problem in Christchurch, New Zealand—Progress and prospects. Clean Air Environ. Qual. 2002, 36, 23–29. [Google Scholar]
- Kingham, S.; Pattinson, W.; Shrestha, K.; Longley, I.; Salmond, J. Determination of Personal Exposure to Traffic Pollution While Travelling by Different Modes; NZ Transport Agency: Wellington, New Zealand, 2011; ISBN 9780478380576.
- Mallet, T. Air Quality Status Report: Christchurch Airshed; Environment Canterbury: Christchurch, New Zealand, 2014.












| Independent Variable | Global Model GLM Poisson Winter | Global Model GLM Poisson Non-winter | GWR Poisson (n = 52) Winter | GWR Poisson (n = 52) Non-winter | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Est. | Std. Error | z-Value | Pr (>|t|) | Est. | Std. Error | z-Value | Pr (>|t|) | Min. | Q1 | Median | Q3 | Max. | Min. | Q1 | Median | Q3 | Max. | |
| (Intercept) | −3.92 | 0.46 | −8.47 | 0.00 | −6.57 | 0.68 | −9.68 | 0.00 | −12.83 | −5.59 | −3.06 | −1.69 | −0.77 | −17.29 | −8.05 | −6.35 | −3.18 | 2.34 |
| Deprivation | 0.14 | 0.02 | 6.32 | 0.00 | 0.09 | 0.03 | 2.83 | 0.00 | −0.02 | 0.07 | 0.12 | 0.14 | 0.30 | −0.04 | 0.02 | 0.05 | 0.11 | 0.25 |
| PM2.5 | 0.03 | 0.05 | 0.59 | 0.56 | 0.56 | 0.12 | 4.61 | 0.00 | −0.17 | −0.04 | 0.04 | 0.21 | 0.74 | −0.56 | 0.14 | 0.57 | 0.82 | 1.13 |
| Elderly ratio | −0.03 | 0.01 | −3.72 | 0.00 | −0.04 | 0.01 | −3.24 | 0.01 | −0.09 | −0.05 | −0.03 | −0.01 | 0.04 | −0.07 | −0.03 | −0.02 | −0.01 | 0.03 |
| European | −0.61 | 0.54 | −1.12 | 0.26 | −1.22 | 0.72 | −1.69 | 0.09 | −4.58 | −3.01 | −1.74 | −0.26 | 5.72 | −6.12 | −3.89 | −2.22 | −0.66 | 12.25 |
| Maori | 1.05 | 1.38 | 0.76 | 0.44 | 2.39 | 1.56 | 1.53 | 0.08 | −13.49 | −2.95 | 0.62 | 4.67 | 14.13 | −3.97 | −0.24 | 2.21 | 4.79 | 10.69 |
| (pseudo) R2 | 0.44 | 0.48 | 0.62 | 0.65 | ||||||||||||||
| AICc | 365.17 | 196.40 | 300.15 | 186.65 | ||||||||||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marek, L.; Campbell, M.; Epton, M.; Kingham, S.; Storer, M. Winter Is Coming: A Socio-Environmental Monitoring and Spatiotemporal Modelling Approach for Better Understanding a Respiratory Disease. ISPRS Int. J. Geo-Inf. 2018, 7, 432. https://doi.org/10.3390/ijgi7110432
Marek L, Campbell M, Epton M, Kingham S, Storer M. Winter Is Coming: A Socio-Environmental Monitoring and Spatiotemporal Modelling Approach for Better Understanding a Respiratory Disease. ISPRS International Journal of Geo-Information. 2018; 7(11):432. https://doi.org/10.3390/ijgi7110432
Chicago/Turabian StyleMarek, Lukas, Malcolm Campbell, Michael Epton, Simon Kingham, and Malina Storer. 2018. "Winter Is Coming: A Socio-Environmental Monitoring and Spatiotemporal Modelling Approach for Better Understanding a Respiratory Disease" ISPRS International Journal of Geo-Information 7, no. 11: 432. https://doi.org/10.3390/ijgi7110432
APA StyleMarek, L., Campbell, M., Epton, M., Kingham, S., & Storer, M. (2018). Winter Is Coming: A Socio-Environmental Monitoring and Spatiotemporal Modelling Approach for Better Understanding a Respiratory Disease. ISPRS International Journal of Geo-Information, 7(11), 432. https://doi.org/10.3390/ijgi7110432