Development of a Novel Framework to Propose New Strategies for Automated External Defibrillators Deployment Targeting Residential Out-Of-Hospital Cardiac Arrests: Application to the City of Milan

 ,
,  ,
, 
Abstract
:1. Introduction
- Efficiency analysis of the current distribution of AEDs, based on the area where AEDs can be used within the scientifically assessed time limit for an effective and beneficial use, hence there is no standard in how to convert this time limit into a spatial measure.
- Mapping of OHCA occurrence risk by development of a geographic risk function using different approaches: purely statistical (simulation of events based on retrospective data or application of distribution models, such as Poisson regression or Kernel density analysis) or more sophisticated ones (modelling of explicative factors, relevant to demography, socio-economic conditions, and land-use). Given the intrinsic randomness of the phenomenon, both predictive performance and generalization of the proposed methods are uncertain.
- Identification of new AED spatial distributions, based on the optimization of a target function, and assessment of the related performance by a validation procedure. Whereas the proposed mathematical optimizations of target functions are detailed and successful, their conversion into PAD performance improvement is hard to validate.
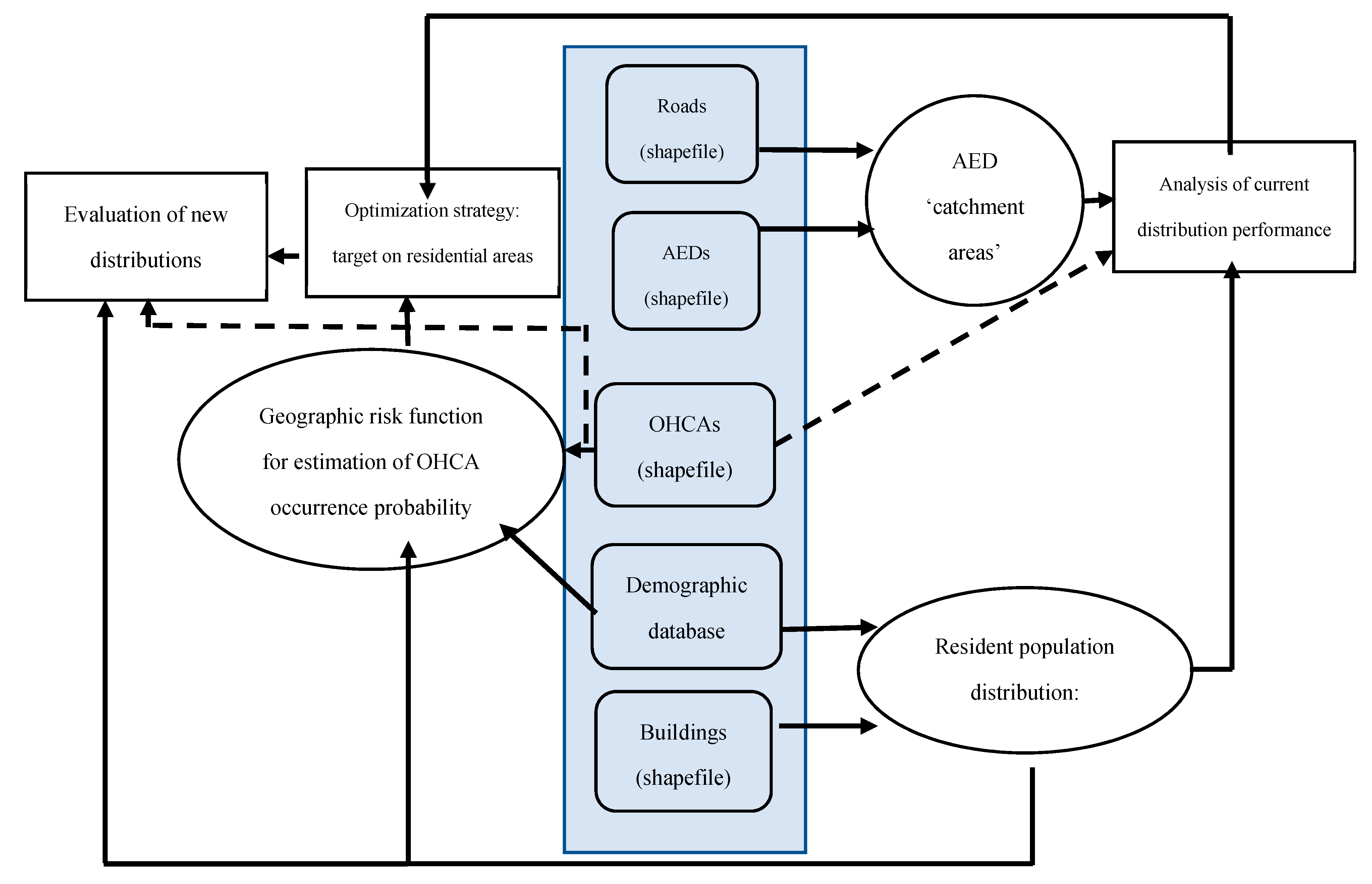
2. Materials and Methods
2.1. Data Sources and Pre-Processing
- Georeferenced database of OHCAs (collected and made available for this research by AREU, Azienda Regionale Emergenza/Urgenza, responsible for the 112 emergency number service and Emergency Medical Services (EMS) provider for Lombardy region): it includes records of all OHCAs that occurred in Lombardy from 2015 to 2018 for a total of 45,043 records. In this timeframe, 8152 OHCAs occurred in the city of Milan, of which 7179 (88.06%) in residential locations. The anonymized database contains, as fields, the geolocation of each event, its date and time, time-to-intervention, information related to CPR and AED use, and more.
- Georeferenced database of AED (from AREU): it includes geo-reference (geographic coordinates), location (description of the AED’s installation place), and accessibility of known publicly accessible AEDs in Lombardy as of 31 December 2018 (10,023 devices, 1001 in the city of Milan).
- Milan City Topographic Database (open data at https://geoportale.comune.milano.it/sit/): Geographic information about residential buildings, roads, subdivision of the city into 88 districts (Local Identity Nuclei, LINs: an administrative subdivision of the city based on traditional areas of the city and history of urban development).
- Demography (open data at http://dati.comune.milano.it/): demographic and socioeconomic information about the resident population specifically for each LIN (gender, age, and nationality).
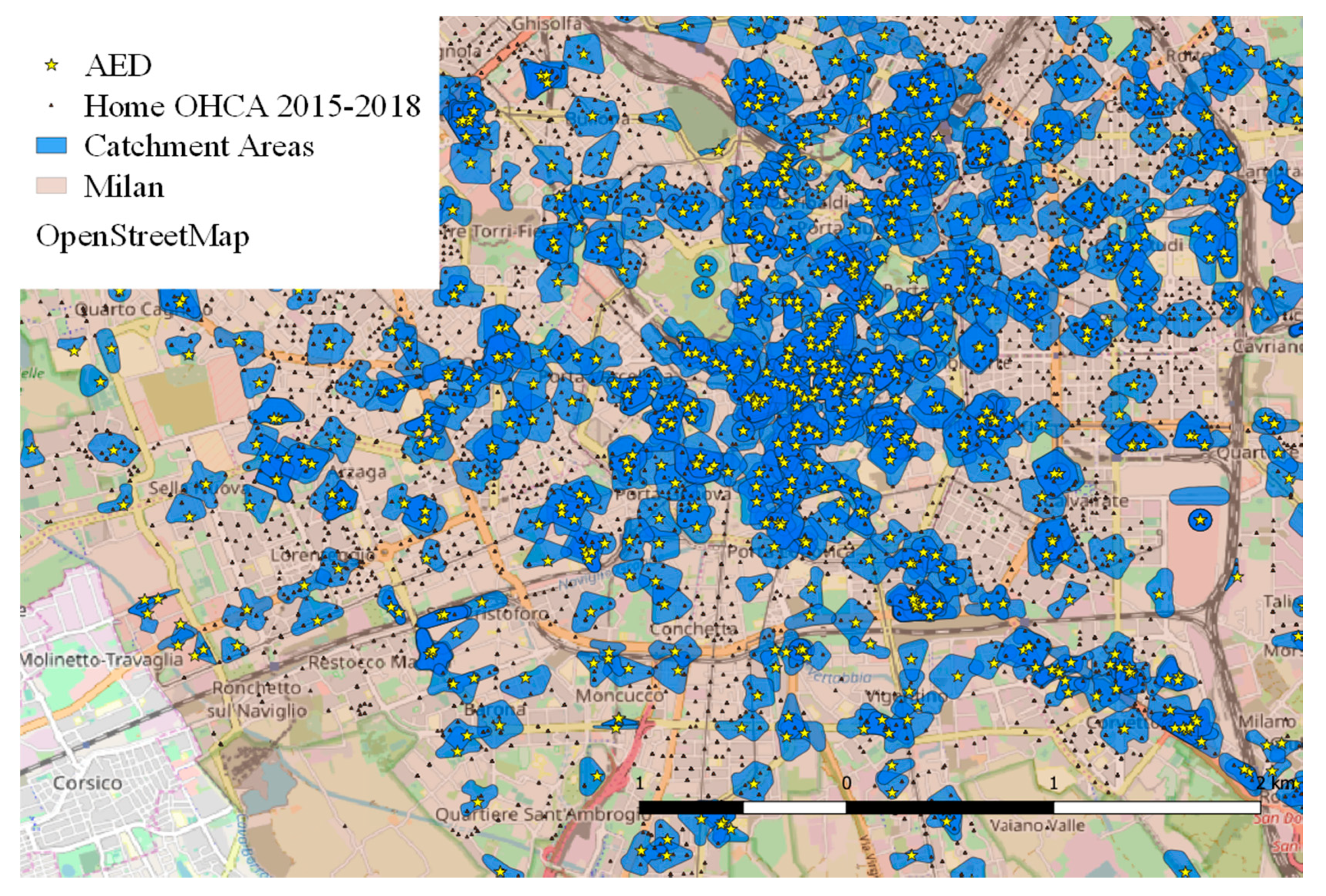
2.2. AED “Catchment Areas”
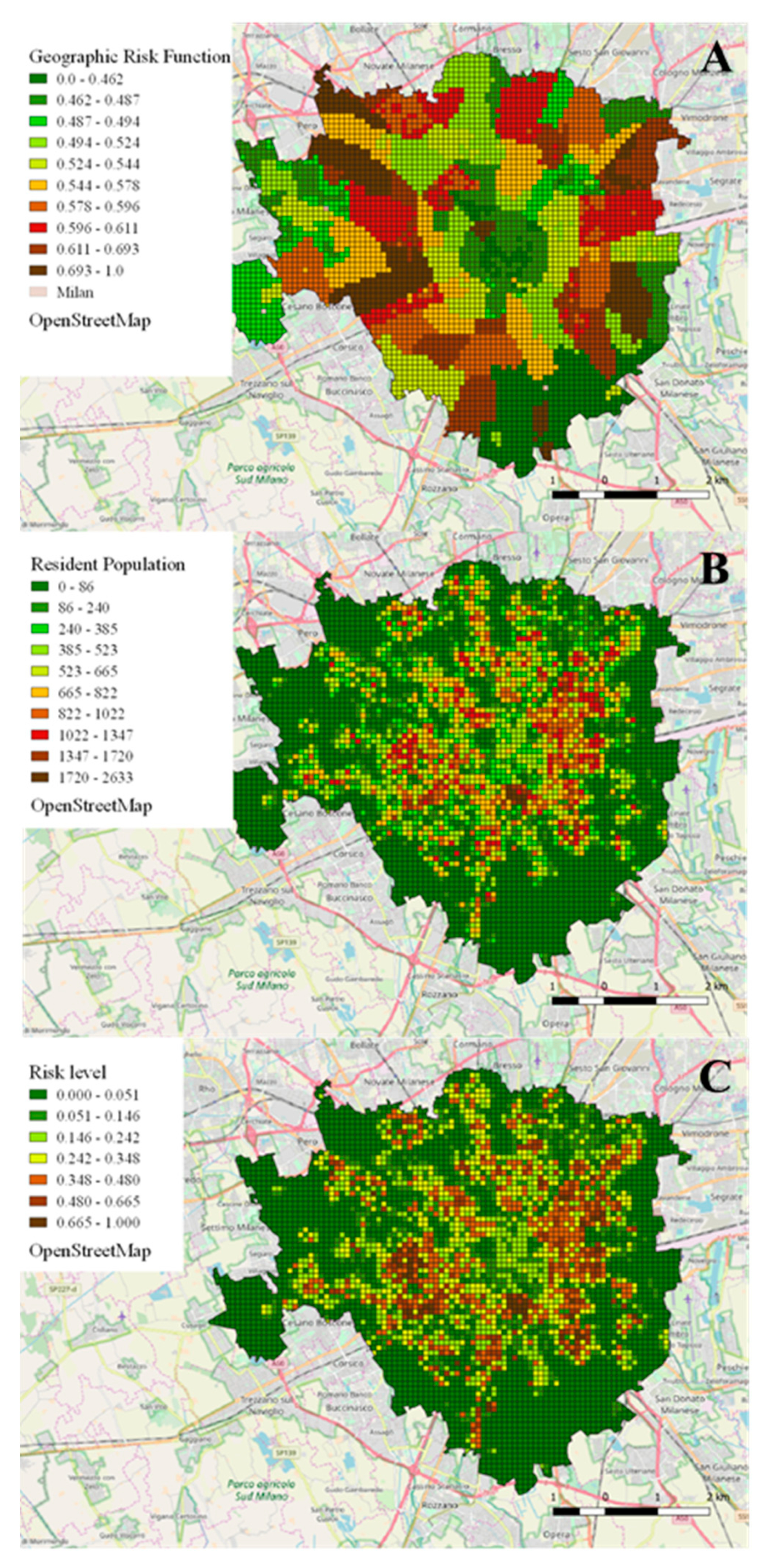
2.3. Geographic Risk Function
- : Target variable predictor (i-th item), estimate for the purely geographic risk function;
- : Attributes number;
- : Coefficients for polynomial third degree interpolation (j-th attribute);
- : Value of the j-th attribute for the i-th item;
- : , where is the absolute value of the mean of residuals for the estimator from interpolation of j-th attribute.
- : Final risk level (i-th cell);
- : Predictor of OHCA percentage incidence (i-th cell, rescaled [0,1]), representing the estimate of the purely geographic risk function;
- : Estimated resident population (i-th cell);
2.4. Optimization Strategy
- AEDs database, each weighted by an efficiency score (coverage of final risk level through its catchment area), and by a time-accessibility score (ts) ranged 0 to 1, with 1 assigned to AEDs accessible 24/7.
- dataset of 200 × 200 m cells not covered by an AED, where each cell has a priority score expressed by the final risk level.
- Identification of all the cells where an AED should be positioned according to the selected goal, with priority ranking, as a new installation or a re-displacement;
- Identification of the currently located AEDs that should be repositioned.
- -
- ΔTp represents the increase in percentage of covered OHCAs from the baseline: when evaluating the current AED distribution, the baseline value is assumed as 0%, whereas when evaluating new distributions, the baseline represents the percentage of OHCAs covered through the pre-existing deployment. As an example, a new simulated deployment covering 60% of retrospective events could results in ΔTp = 60 if representing a new distribution starting from blank (i.e., no AED on the territory); otherwise in case of a coverage of 41.77% provided by the current distribution, it results in ΔTp = 60 − 41.77 = 18.23, thus representing further processing of the currently implemented deployment.
- -
- Tc is the cost for the implementation of such distribution, expressed in M€.
3. Results
3.1. Performance of Current AEDs Distribution
3.2. Validation of the Geographic Risk Function
3.3. Performance of the Optimized Distribution of AEDs
4. Discussion
- Dimensioning of the catchment areas: the proposed computation considers realistic areas, based on the reachable distance within 3 min (allowing back and forth within 6 min) at 1.5 m/s velocity (270 m), reduced by a variable quantity (max 70 m) depending on the mean height of the surrounding buildings. This solution constitutes a possible improvement in matching a real-world scenario, compared to previous literature (100 m circular area [17,20,22,34,38,39]).
- Development of the risk function: the main innovation was to focus on OHCAs occurring inside residential locations constituting the majority of the events (almost 90% in the considered dataset), characterized by higher mortality. Differently from previous studies [9,20,39], a supervised learning approach inspecting the relation between geographic risk (target) and attributes related to demography, socio-economic conditions and land-use was applied.
- Applicability as a decision-making support tool: in literature, only one example [9] of an interactive interface for the optimization framework with the possibility for the user to modify the initial parameters as a decision-making support was present. The novelty (and main potentiality) of the proposed framework is related to its generalization and application to any new territory where the input data (AEDs and past OHCAs geolocation, streets network, demography) are available, although with variable accuracy to be determined according to the provided information (both regarding quantity and quality). Moreover, the proposed framework also considers the possibility to re-displace current devices (as suggested by Tierney et al. [38]) and allows the user to set the target constraints for optimization, choosing among a wider number of different criteria including area, population or risk coverage, not just limited to budget or number of devices.
- Data quality: topographic and demographic open data, not specifically collected for scientific purposes, were used for the development of the risk function. Moreover, the topographic mapping information was not complete and prevented the computation of realistic catchment areas for 72 (7.2%) of the considered devices, for which the use of the traditional (yet inefficient in terms of OHCA coverage [40]) 100 m circular buffer was implemented. However, due to the limited number of affected AED and their location (parks, squares and large facilities), which is not relevant in addressing residential events (i.e., the main focus of this study), we considered the resulting approximation as acceptable.
- AED placement spot: the algorithm identifies squared cells where an installation is considered necessary (according to specifications), but no output is provided about the exact spot within the cell where the AED should be placed, which means that the resulting coverage area might not be the most efficient. A future development could address the identification of these spots, with a following phase of fine-tuning positioning for each cell.
- Follow-up survival data not available: due to Italian legislation and separate database system between the EMS provider and the hospitals, the assessment of the rescue outcome, neither in short-term (as EMS crew often does not include a physician, so death could not be declared until body arrival to the hospital) nor in long-term survival, was not available. This prevented a possible comparison of the rate of AED use and successful resuscitation between cases of home-OHCA, which occurred within the actual public AED catchment areas, versus those that occurred outside. Although timely interventions on OHCA with a public AED do increase survival probability [4,5], and the likelihood of such interventions is higher when the distance between the OHCA location and the AED is shorter [28], the proposed increase in spatial coverage provided by public AEDs, which is the target of this study, could be evaluated from an efficiency point of view (e.g., by computing the results in terms of Quality-Adjusted Life Years, QALYs). This is only if correlating more frequent uses of AED in events occurring within their catchment areas with higher survival rates and better medical outcomes, of which were not available in this study. However, Sondergaard et al. [28] reported a higher likelihood of use of public AEDs when placed closer to OHCA locations, while Sun et al. [39] demonstrated, exploiting the Utstein-based outcome prediction, that the increase in spatial coverage provided by AEDs is correlated with higher survival chances and better neurological outcome. In addition, the report remarked that this kind of “in-silico” trial “can be used to identify promising interventions based on objective performance criteria and inform trial design in a data-driven manner, potentially saving significant time and money”.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Adams, R.J.; Berry, J.D.; Brown, T.M.; Carnethon, M.R.; Dai, S.; Simone, D.G.; Ford, E.S.; et al. Heart Disease and Stroke Statistics—2011 Update: A Report From the American Heart Association. Circulation 2011, 123, 18–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Priori, S.G.; Blomstrom-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac Death. The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Eur. Heart J. 2015, 36, 2793–2867. [Google Scholar] [PubMed] [Green Version]
- Wellens, H.J.; Lindemans, F.W.; Houben, R.P.; Gorgels, A.; Volders, P.G.; Bekke, R.M.; Crijns, H.J. Improving survival after out-of-hospital cardiac arrest requires new tools. Eur. Heart J. 2016, 37, 1499–1503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmberg, M.J.; Vognsen, M.; Andersen, M.S.; Donnino, M.W.; Andersen, L.W. Bystander automated external defibrillator use and clinical outcomes after out-of-hospital cardiac arrest: A systematic review and meta-analysis. Resuscitation 2017, 120, 77–87. [Google Scholar] [CrossRef]
- Kiyohara, K.; Nishiyama, C.; Kitamura, T.; Matsuyama, T.; Sado, J.; Shimamoto, T.; Kobayashi, D.; Kiguchi, T.; Okabayashi, S.; Kawamura, T.; et al. The association between public access defibrillation and outcome in witnessed out-of-hospital cardiac arrest with shockable rhythm. Resuscitation 2019, 140, 93–97. [Google Scholar] [CrossRef]
- Zulli, L. La Morte Cardiaca Improvvisa—L’arresto Cardiocircolatorio—La Rianimazione Cardiopolmonare. Available online: http://internetsfn.asl-rme.it/file_allegati/morte_improvvisa.pdf (accessed on 10 September 2019).
- Jost, D.; Degrange, H.; Verret, C.; Hersan, O.; Banville, I.L.; Chapman, F.W.; Lank, P.; Petit, J.L.; Fuilla, C.; Migliani, R.; et al. DEFI 2005: A randomized controlled trial of the effect of automated external defibrillator cardiopulmonary resuscitation protocol on outcome from out-of-hospital cardiac arrest. Circulation 2010, 121, 1614–1622. [Google Scholar] [CrossRef] [Green Version]
- Perkins, G.D.; Handley, A.J.; Koster, R.W.; Castren, M.; Smyth, M.; Olasveengen, T.; Monsieurs, K.G.; Raffay, V.; Gräsner, J.-T.; Wenzel, V.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 2. Adult basic life support and automated external defibrillation. Resuscitation 2015, 95, 81–99. [Google Scholar] [CrossRef] [Green Version]
- Bonnet, B.; Dessavre, D.G.; Kraus, K.; Ramirez-Marquez, J.E. Optimal placement of public-access AEDs in urban environments. Comput. Ind. Eng. 2015, 90, 269–280. [Google Scholar] [CrossRef]
- Weisfeldt, M.L.; Kreber, R.E.; McGoldrick, R.P.; Moss, A.J.; Nichol, G.; Ornato, J.P.; Palmer, D.G.; Reigel, B.; Smith, S.C. Public Access Defibrillation A Statement for Healthcare Professionals From the American Heart Association Task Force on Automatic External Defibrillation. Circulation 1995, 92, 2763. [Google Scholar] [CrossRef]
- Mauri, R.; Burkart, R.; Benvenuti, C.; Caputo, M.L.; Moccetti, T.; Bufalo, D.A.; Gallino, A.; Casso, C.; Anselmi, L.; Cassina, T.; et al. Better management of out-ofhospital cardiac arrest increases survival rate and improves neurological outcome in the Swiss Canton Ticino. Europace 2016, 18, 398–404. [Google Scholar] [CrossRef]
- Smith, C.M.; Wilson, M.H.; Hartley-Sharpe, C.; Gwinnutt, C.; Dicker, B.; Perkins, G.D. The use of trained volunteers in the response to out-of-hospital cardiac arrest—The GoodSAM experience. Resuscitation 2017, 121, 123–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisfeldt, M.L.; Sitlani, C.M.; Ornato, J.P.; Rea, T.; Aufderheide, T.P.; Davis, D.; Dreyer, J.; Hess, E.P.; Jui, J.; Maloney, J.; et al. Survival after application of automatic external defibrillators before arrival of the emergency medical system: Evaluation in the resuscitation outcomes consortium population of 21 million. J. Am. Coll. Cardiol. 2010, 55, 1713–1720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deakin, C.D.; Shewry, E.; Gray, H.H. Public access defibrillation remains out of reach for most victims of out-of-hospital sudden cardiac arrest. Heart 2014, 100, 619–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, R.D.; Ong, M.E.H. Public access defibrillation: Improving accessibility and outcomes. Br. Med. Bull. 2016, 118, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldi, E.; Savastano, S. AED use before EMS arrival: When survival becomes a matter of law and system in Italy, which can be improved. Eur. Heart J. 2018, 39, 1664. [Google Scholar] [CrossRef]
- Sun, C.L.F.; Demirtas, D.; Brooks, S.; Morrison, L.J.; Chan, T.C. Overcoming Spatial and Temporal Barriers to Public Access Defibrillators Via Optimization. J. Am. Coll. Cardiol. 2016, 68, 836–845. [Google Scholar] [CrossRef]
- Lin, B.-C.; Chen, C.-W.; Chen, C.-C.; Kuo, C.-L.; Fan, I.-C.; Ho, C.-K.; Liu, I.-C.; Chan, T.-C. Spatial decision on allocating automated external defibrillators (AED) in communities by multi-criterion two-step floating catchment area (MC2SFCA). Int. J. Health Geogr. 2016, 15, 17. [Google Scholar] [CrossRef] [Green Version]
- Chrisinger, B.; Grossestreuer, A.V.; Laguna, M.C.; Griffis, H.M.; Branas, C.C.; Wiebe, U.J.; Merchant, R.M. Characteristics of automated external defibrillator coverage in Philadelphia, PA, based on land use and estimated risk. Resuscitation 2016, 109, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Chan, T.C.; Demirtas, D.; Kwon, R.H. Optimizing the Deployment of Public Access Defibrillators. Manag. Sci. 2017, 62, 3617–3635. [Google Scholar] [CrossRef] [Green Version]
- Bardy, G.H.; Lee, K.L.; Mark, D.B.; Poole, J.E.; Toff, W.; Tonkin, A.M.; Smith, W.; Dorian, P.; Packer, U.L.; White, R.D.; et al. Home Use of Automated External Defibrillators for Sudden Cardiac Arrest. N. Engl. J. Med. 2008, 358, 1793–1804. [Google Scholar] [CrossRef] [Green Version]
- Folke, F.; Gislason, G.H.; Lippert, F.; Nielsen, S.L.; Weeke, P.; Hansen, M.L.; Fosbøl, E.L.; Andersen, S.S.; Rasmussen, S.; Schramm, T.K.; et al. Differences Between Out-of-Hospital Cardiac Arrest in Residential and Public Locations and Implications for Public-Access Defibrillation. Circulation 2010, 122, 623–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, S.M.; Hansen, C.M.; Folke, F.; Rajan, S.; Kragholm, K.; Ejlskov, L.; Gislason, G.; Køber, L.; Gerds, T.A.; Hjortshøj, S.; et al. Bystander Defibrillation for Out-of-Hospital Cardiac Arrest in Public vs Residential Locations. JAMA Cardiol. 2017, 2, 507–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deakin, C.D.; Anfield, S.A.; Hodgetts, G. Underutilisation of public access defibrillation is related to retrieval distance and time-dependent availability. Heart 2018, 104, 1339–1343. [Google Scholar] [CrossRef] [PubMed]
- Sondergaard, K.B.; Wissenberg, M.; Gerds, T.A.; Rajan, S.; Karlsson, L.; Kragholm, K.; Pape, M.; Lippert, F.; Gislason, G.; Folke, F.; et al. Bystander cardiopulmonary resuscitation and long-term outcomes in out-of-hospital cardiac arrest according to location of arrest. Eur. Heart J. 2019, 40, 309–318. [Google Scholar] [CrossRef]
- Iwami, T.; Hiraide, A.; Nakanishi, N.; Hayashi, Y.; Nishiuchi, T.; Uejima, T.; Morita, H.; Shigemoto, T.; Ikeuchi, H.; Matsusaka, M.; et al. Outcome and characteristics of out-of-hospital cardiac arrest according to location of arrest: A report from a large-scale, population-based study in Osaka, Japan. Resuscitation 2006, 69, 221–228. [Google Scholar] [CrossRef]
- Weisfeldt, M.L.; Everson-Stewart, S.; Sitlani, C.; Rea, T.; Aufderheide, T.P.; Atkins, D.L.; Bigham, B.; Brooks, S.; Foerster, C.; Gray, R.; et al. Ventricular Tachyarrhythmias after Cardiac Arrest in Public versus at Home. N. Engl. J. Med. 2011, 364, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Sondergaard, K.B.; Hansen, S.M.; Pallisgaard, J.L.; Gerds, T.A.; Wissenberg, M.; Karlsson, L.; Lippert, F.; Gislason, G.H.; Madelaire, C.; Folke, F. Out-of-hospital cardiac arrest: Probability of bystander defibrillation relative to distance to nearest automated external defibrillator. Resuscitation 2018, 124, 138–144. [Google Scholar] [CrossRef] [Green Version]
- Giacoppo, D. Impact of bystander-initiated cardiopulmonary resuscitation for out-of-hospital cardiac arrest: Where would you be happy to have a cardiac arrest? Eur. Heart J. 2019, 40, 319–321. [Google Scholar] [CrossRef]
- Rea, T. Paradigm shift: Changing public access to all-access defibrillation. Heart 2018, 104, 1311–1312. [Google Scholar] [CrossRef]
- Blackwood, J.; Eisenberg, M.; Jorgenson, D.; Nania, J.; Howard, B.; Collins, B.; Connell, P.; Day, T.; Rohrbach, C.; Rea, T.D. Strategy to Address Private Location Cardiac Arrest: A Public Safety Survey. Prehospital Emerg. Care 2018, 22, 784–787. [Google Scholar] [CrossRef]
- Open Geospatial Consortium. Glossary of Terms. Available online: https://www.opengeospatial.org/ogc/glossary/g (accessed on 10 August 2020).
- Folke, F.; Knudsen Lippert, F.; Nielsen, S.L.; Gislason, G.H.; Hansen, M.L.; Schramm, T.K.; Sorensen, R.; Loldrup Fosbol, E.; Andresen, S.S.; Rasmussen, S.; et al. Location of cardiac arrest in a city centre strategic placement of automated external defibrillators in public locations. Circulation 2009, 120, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.C.; Li, H.; Lebovic, G.; Tang, S.K.; Chan, J.Y.; Cheng, H.C.; Morrison, L.J.; Brooks, S. Identifying Locations for Public Access Defibrillators Using Mathematical Optimization. Circulation 2013, 127, 1801–1809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ringh, M.; Hollenberg, J.; Møller, T.P.; Svensson, L.; Rosenqvist, M.; Lippert, F.; Wissenberg, M.; Hansen, C.M.; Claessen, A.; Viereck, S.; et al. The challenges and possibilities of public access defibrillation. J. Intern. Med. 2018, 283, 238–256. [Google Scholar] [CrossRef] [PubMed]
- American Heart Association. Implementing an AED Program, DS13398 5/18. Available online: https://cpr.heart.org/idc/groups/ahaecc-public/@wcm/@ecc/documents/downloadable/ucm_501521.pdf (accessed on 10 August 2020).
- Smith, C.M.; Keung, S.N.L.C.; Khan, M.O.; Arvanitis, T.N.; Fothergill, R.; Hartley-Sharpe, C.; Wilson, M.; Perkins, G.D. Barriers and facilitators to public access defibrillation in out-of-hospital cardiac arrest: A systematic review. Eur. Heart J. Qual. Care Clin. Outcomes 2017, 3, 264–273. [Google Scholar] [CrossRef]
- Tierney, N.J.; Reinhold, H.; Mira, A.; Weiser, M.; Burkart, R.; Benvenuti, C.; Auricchio, A. Novel relocation methods for automatic external defibrillator improve out-of-hospital cardiac arrest coverage under limited resources. Resuscitation 2018, 125, 83–89. [Google Scholar] [CrossRef] [Green Version]
- Sun, C.L.; Karlsson, L.; Torp-Pedersen, C.; Morrison, L.J.; Brooks, S.; Folke, F.; Chan, T.C. In Silico Trial of Optimized Versus Actual Public Defibrillator Locations. J. Am. Coll. Cardiol. 2019, 74, 1557–1567. [Google Scholar] [CrossRef]
- Gianquintieri, L.; Caiani, E.G.; Brambilla, P.; Pagliosa, A.; Villa, G.F.; Brovelli, M.A. Open Data in Health-Geomatics: Mapping and Evaluating Publicly Accessible Defibrillators. Isprs Archives 2019, XLII-4/W14, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Dicker, B.; Garrett, N.; Wong, S.; McKenzie, H.; McCarthy, J.; Jenkin, G.; Smith, T.; Skinner, J.R.; Pegg, T.; Devlin, G.; et al. Relationship between socioeconomic factors, distribution of public access defibrillators and incidence of out-of-hospital cardiac arrest. Resuscitation 2019, 138, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Vercellis, C. Business Intelligence Modelli Matematici e Sistemi per le Decisioni, 1st ed.; McGraw-Hill: Milano, Italy, 2006; pp. 77–79, 83–88. [Google Scholar]
- Culley, L.L.; Rea, T.D.; Murray, J.A.; Welles, B.; Fahrenbruch, C.E.; Olsufka, M.; Eisenberg, M.S.; Copass, M.K. Public Access Defibrillation in Out-of-Hospital Cardiac Arrest. Circulation 2004, 109, 1859–1863. [Google Scholar] [CrossRef] [Green Version]
- Holmberg, M.; Holmberg, S.; Herlitz, J. Incidence, duration and survival of ventricular fibrillation in out-of-hospital cardiac arrest patients in sweden. Resuscitation 2000, 44, 7–17. [Google Scholar] [CrossRef]
- Norris, R.M.; UK Heart Attack Study (UKHAS) Collaborative Group. Circumstances of out of hospital cardiac arrest in patients with ischaemic heart disease. Heart 2005, 91, 1537–1540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nehme, Z.; Andrew, E.; Bernard, S.; Patsamanis, H.; Cameron, P.; Bray, J.; Meredith, I.T.; Smith, K. Impact of a public awareness campaign on out-of-hospital cardiac arrest incidence and mortality rates. Eur. Heart J. 2017, 38, 1666–1673. [Google Scholar] [CrossRef] [PubMed]
- Nordberg, P.; Hollenberg, J.; Rosenqvist, M.; Herlitz, J.; Jonsson, M.; Järnbert-Petterson, H.; Forsberg, S.; Dahlqvist, T.; Ringh, M.; Svensson, L. The implementation of a dual dispatch system in out-of-hospital cardiac arrest is associated with improved short and long term survival. Eur. Heart J. Acute Cardiovasc. Care 2014, 3, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Pijls, R.W.; Nelemans, P.J.; Rahel, B.M.; Gorgels, A.P. Factors modifying performance of a novel citizen text message alert system in improving survival of out-of-hospital cardiac arrest. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Caputo, M.L.; Muschietti, S.; Burkart, R.; Benvenuti, C.; Conte, G.; Regoli, F.; Mauri, R.; Klersy, C.; Moccetti, T.; Auricchio, A.; et al. Lay persons alerted by mobile application system initiate earlier cardio-pulmonary resuscitation: A comparison with SMS-based system notification. Resuscitation 2018, 114, 73–78. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Territory | Coverage on Milan City Area (%) | Overlapping (%) | Overlapped Coverage on Milan City Area (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 23.14% | 39.28% | 9.09% | |||||||
| Population | Covered Population (%) | Percentage of Covered Population in Overlap | Total Population in Overlap (%) | ||||||
| 40.02% | 40.3% | 16.13% | |||||||
| OHCAs | 2015–2016 | 2017–2018 | Overall (2015–2018) | ||||||
| Coverage | Home | Out | Tot | Home | Out | Tot | Home | Out | Tot |
| # | 1387 | 222 | 1609 | 1527 | 269 | 1796 | 2914 | 491 | 3405 |
| % on Total | 39.56% | 47.54% | 40.5% | 41.57% | 53.16% | 42.98% | 40.59% | 50.46% | 41.77% |
| # in overlapping | 484 | 113 | 597 | 559 | 149 | 708 | 1043 | 262 | 1305 |
| % in overl. on cov | 34.9% | 50.9% | 37.1% | 36.61% | 55.39% | 39.42% | 35.79% | 53.36% | 38.33% |
| % in overl. on tot | 13.8% | 24.2% | 15.03% | 15.22% | 29.45% | 16.94% | 14.53% | 26.93% | 16.01% |
| Coverages | OHCAs (Home, Outside) | Geographic Risk Function | Area | Resident Population | Cost-Efficiency Parameter CE |
|---|---|---|---|---|---|
| Current deployment | 41.77% (40.59%, 50.46%) | 39.51% | 23.14% | 40.02% | 16.69% |
| Model-based simulated deployment (% Δ) | 73.33% (+31.56%) (75.65%, 56.22%) (+35.06%, +5.76%) | 65.27% (+25.76%) | 29.07% (+5.93%) | 70.15% (+30.13%) | 29.3% (+12.61%) |
| Current Placement | Displacements Only | 100 New AEDs | Risk Coverage Doubling | Budget Doubling | |
|---|---|---|---|---|---|
| Final AEDs N° | 1001 | 1001 (=) | 1101 (+100) | 1396 (+295) | 1943 (+942) |
| N° of re-displaced AEDs (%) | / | 373 (37.26%) | 366 (36.56%) | 357 (35.66%) | 293 (29.27%) |
| Total Cost (€) (% of initial estimated investment) | 2,502,500 | 186,500 (7.45%) | 433,000 (17.3%) | 916,000 (36.6%) | 2,501,500 (99.96%) |
| Covered Risk | 39.51% | 64.52% (+25.01%) | 69.96% (+30.45%) | 79.03% (+39.52%) | 98.79% (+59.28%) |
| Covered Area | 23.14% | 17.94% (-5.2%) | 19.98% (-3.16%) | 23.91% (+0.77%) | 36.43% (+13.29%) |
| Covered Resident Population | 40.02% | 59.49% (+19.47%) | 64.08% (+24.06%) | 71.66% (+31.64%) | 88.75% (+48.73%) |
| Covered home OHCAs 2015–2016 | 39.56% | 65.43% (+25.87%) | 69.91% (+30.35%) | 76.41% (+36.85%) | 89.45% (+49.89%) |
| Covered home OHCAs 2017–2018 | 41.57% | 64.69% (+23.12%) | 68.69% (+27.12%) | 74.93% (+33.36%) | 89.14% (+47.57%) |
| Covered home OHCAs 2015–2018 | 40.59% | 65.05% (+24.46%) | 69.29% (+28.7%) | 75.65% (+35.06%) | 89.29% (+48.7%) |
| Covered outside OHCAs 2015–2018 | 50.46% | 63.21% (+12.75%) | 65.15% (+14.69%) | 69.37% (+18.91%) | 78.52% (+28.06%) |
| Total Covered OHCAs 2015–2018 | 41.77% | 64.83% (+23.06%) | 68.79% (+27.02%) | 74.9% (+33.13%) | 88% (+46.23%) |
| Cost-efficiency (% coverage improvement over baseline/M€) | 16.69% | 123.65% (+106.96%) | 62.4% (+45.71%) | 36.17% (+19.48%) | 18.47% (+16.78%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorenzo, G.; Maria Antonia, B.; Piero Maria, B.; Andrea, P.; Guido Francesco, V.; Enrico Gianluca, C. Development of a Novel Framework to Propose New Strategies for Automated External Defibrillators Deployment Targeting Residential Out-Of-Hospital Cardiac Arrests: Application to the City of Milan. ISPRS Int. J. Geo-Inf. 2020, 9, 491. https://doi.org/10.3390/ijgi9080491
Lorenzo G, Maria Antonia B, Piero Maria B, Andrea P, Guido Francesco V, Enrico Gianluca C. Development of a Novel Framework to Propose New Strategies for Automated External Defibrillators Deployment Targeting Residential Out-Of-Hospital Cardiac Arrests: Application to the City of Milan. ISPRS International Journal of Geo-Information. 2020; 9(8):491. https://doi.org/10.3390/ijgi9080491
Chicago/Turabian StyleLorenzo, Gianquintieri, Brovelli Maria Antonia, Brambilla Piero Maria, Pagliosa Andrea, Villa Guido Francesco, and Caiani Enrico Gianluca. 2020. "Development of a Novel Framework to Propose New Strategies for Automated External Defibrillators Deployment Targeting Residential Out-Of-Hospital Cardiac Arrests: Application to the City of Milan" ISPRS International Journal of Geo-Information 9, no. 8: 491. https://doi.org/10.3390/ijgi9080491
APA StyleLorenzo, G., Maria Antonia, B., Piero Maria, B., Andrea, P., Guido Francesco, V., & Enrico Gianluca, C. (2020). Development of a Novel Framework to Propose New Strategies for Automated External Defibrillators Deployment Targeting Residential Out-Of-Hospital Cardiac Arrests: Application to the City of Milan. ISPRS International Journal of Geo-Information, 9(8), 491. https://doi.org/10.3390/ijgi9080491