
Understanding the Influence of Socioeconomic Variables on Medicinal Plant Knowledge in the Peruvian Andes



Abstract
:1. Introduction
2. Results
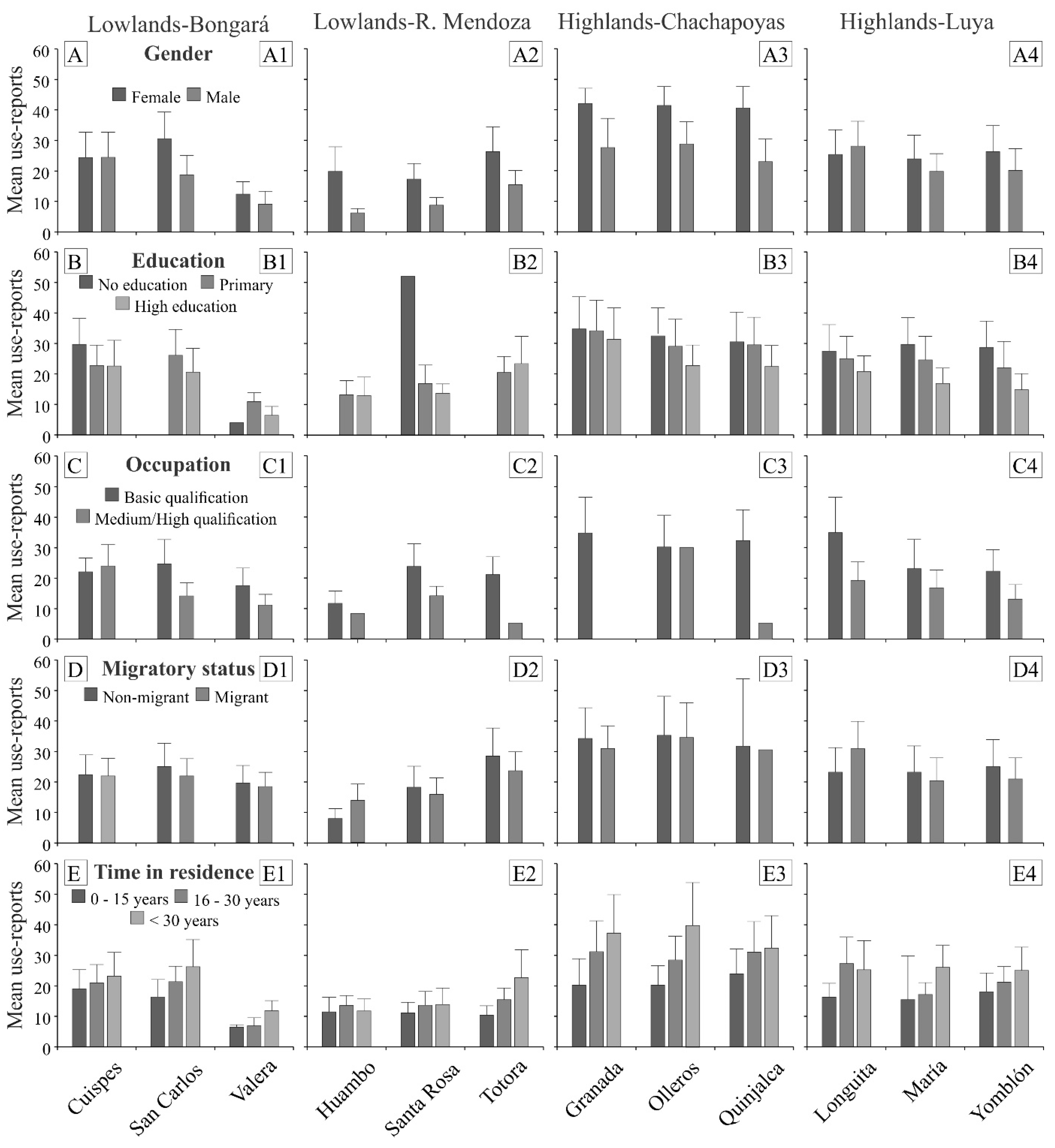
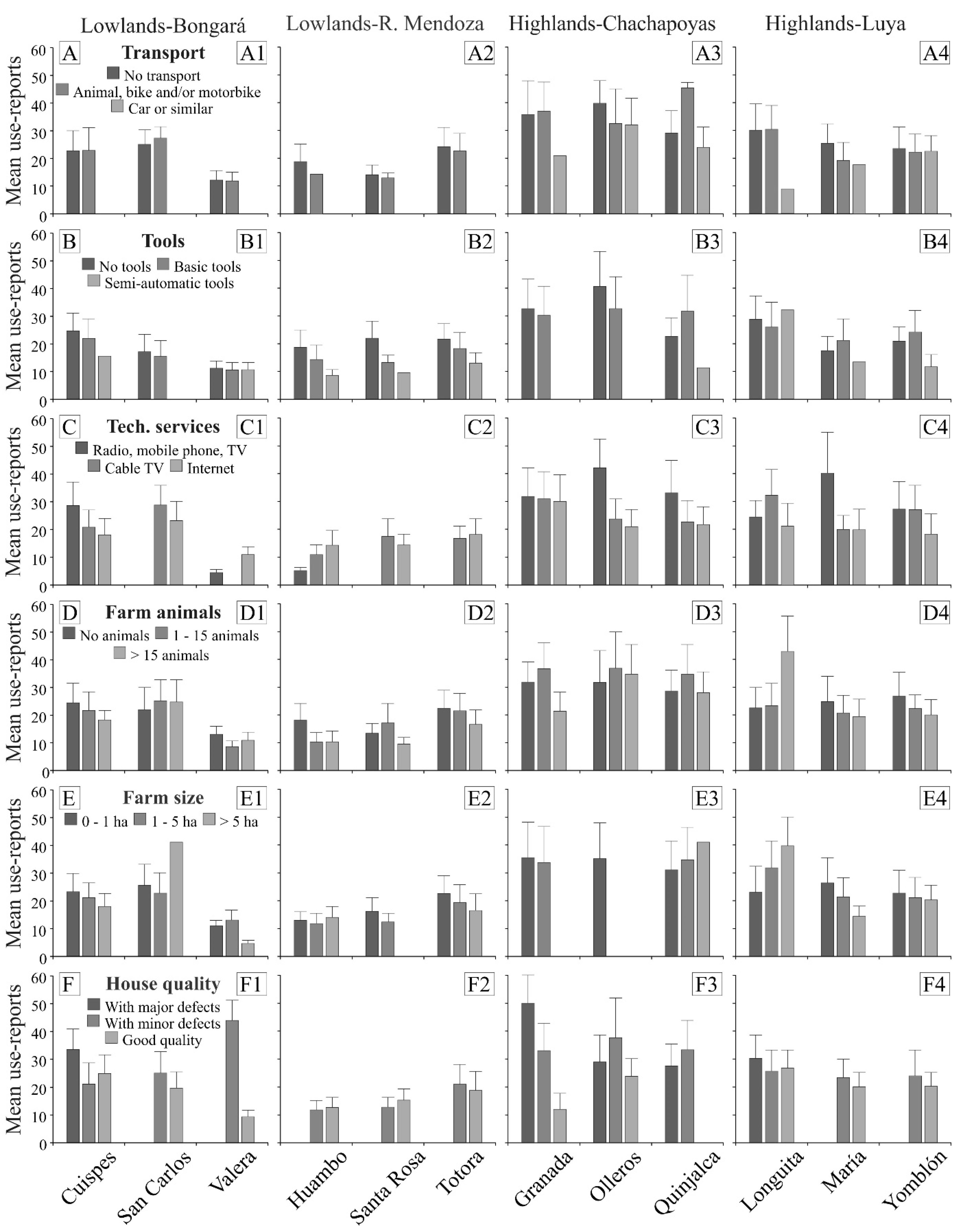
2.1. The Influence of Socioeconomic Factors on MPK
2.2. Mixed-Model Effects of Socioeconomic Factors on MPK
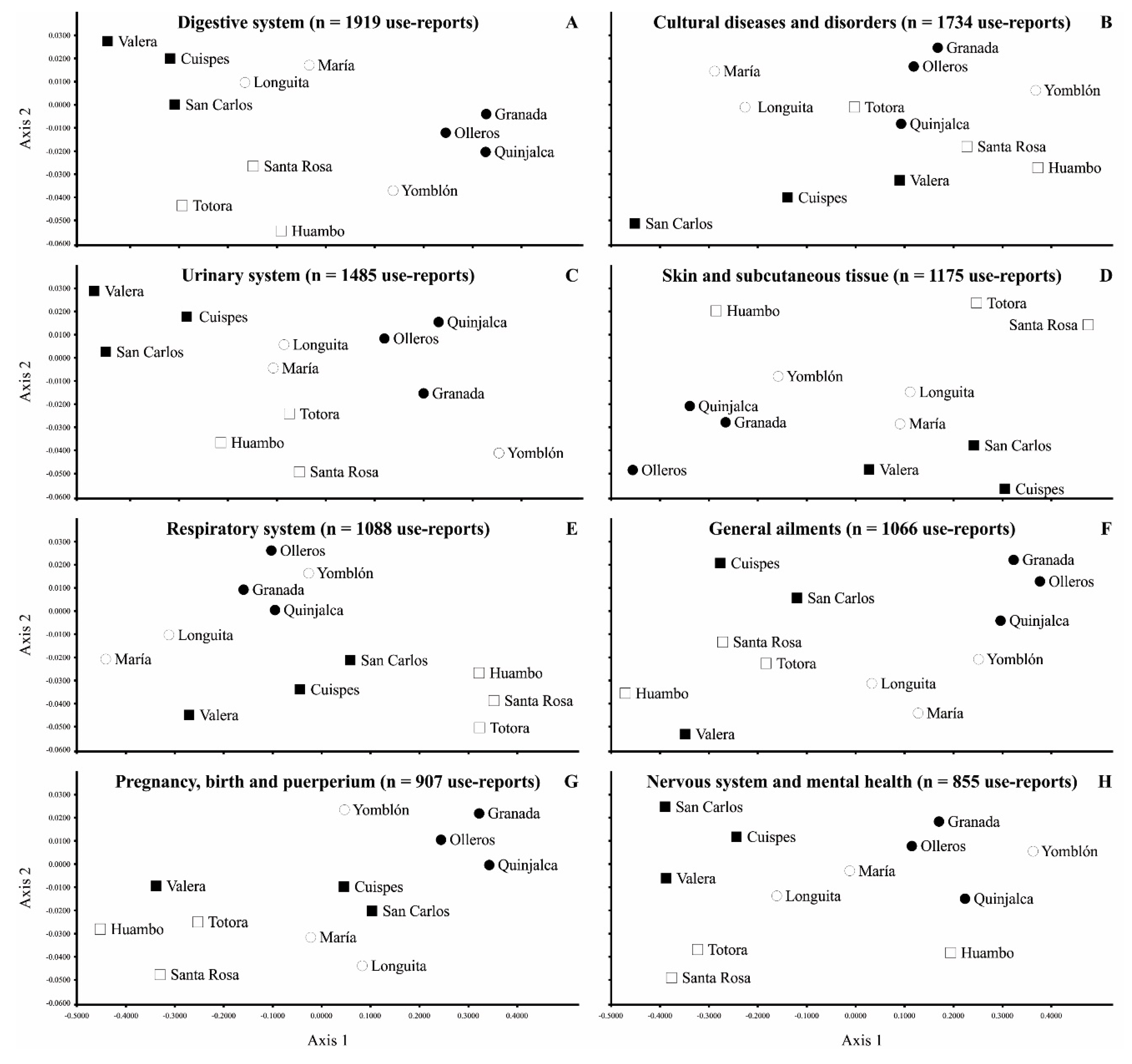
2.3. Relationship between Socioeconomic Factors and Medicinal Categories
3. Discussion
3.1. Influence of Socioeconomic Factors on MPK at the Individual Level
3.2. Influence of Socioeconomic Factors on MPK at the Family Level
3.3. Influence of Socioeconomic Factors on MPK at the Locality Level
3.4. Similarities of Socioeconomic Factors across Localities and Medicinal Categories
4. Materials and Methods
4.1. Study Area
4.2. Data Collection
4.3. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Almeida, C.F.C.B.R.; Ramos, M.A.; Amorim, E.L.C.; Albuquerque, U.P. A comparison of knowledge about medicinal plants for three rural communities in the semi-arid region of northeast of Brazil. J. Ethnopharmacol. 2010, 127, 674–684. [Google Scholar] [CrossRef]
- Mafimisebi, T.E.; Oguntade, A.E.; Fajemisin, A.N.; Aiyelari, O.P. Local knowledge and socio-economic determinants of traditional medicines’ utilization in livestock health management in Southwest Nigeria. J. Ethnobiol. Ethnomed. 2012, 8, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albuquerque, U.P.; Nascimento, A.L.B.; Soldati, G.T.; Feitosa, I.S.; Campos, J.L.A.; Hurrell, J.A.; Hanazaki, N.; Medeiros, P.M.D.; Silva, R.R.V.D.; Ludwinsky, R.H.; et al. Ten important questions/issues for ethnobotanical research. Acta Bot. Brasilica 2019, 33, 376–385. [Google Scholar] [CrossRef]
- Botha, J.; Witkowski, E.T.F.; Shackleton, C.M. Market profiles and trade in medicinal plants in the Lowveld, South Africa. Env. Conserv. 2004, 31, 38–46. [Google Scholar] [CrossRef] [Green Version]
- Mathez-Stiefel, S.L.; Brandt, R.; Lachmuth, S.; Rist, S. Are the young less knowledgeable? Local knowledge of natural remedies and its transformations in the Andean Highlands. Hum. Ecol. 2012, 40, 909–930. [Google Scholar] [CrossRef] [Green Version]
- Phillips, O.; Gentry, A.H.; Reynel, C.; Wilkin, P.; Gálvez-Durand, B.C. Quantitative ethnobotany and Amazonian conservation. Conserv. Biol. 1994, 8, 225–248. [Google Scholar] [CrossRef]
- Reyes-Garcia, V.; McDade, T.; Vadez, V.; Huanca, T.; Leonard, W.R.; Tanner, S.; Godoy, R. Non-market returns to traditional human capital: Nutritional status and traditional knowledge in a native Amazonian society. J. Dev. Stud. 2008, 44, 217–232. [Google Scholar] [CrossRef]
- Bussmann, R.W.; Sharon, D.; Lopez, A. Blending traditional and Western medicine: Medicinal plant use among patients at Clinica Anticona in El Porvenir, Peru. Ethnobot. Res. Appl. 2007, 5, 185–199. [Google Scholar] [CrossRef] [Green Version]
- Macía, M.J.; García, E.; Vidaurre, P.J. An ethnobotanical survey of medicinal plants commercialized in the markets of La Paz and El Alto, Bolivia. J. Ethnopharmacol. 2005, 97, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Pardo-de-Santayana, M.; Macía, M.J. Biodiversity: The benefits of traditional knowledge. Nature 2015, 518, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Salpeteur, M.; Patel, H.H.; Molina, J.L.; Balbo, A.L.; Rubio-Campillo, X.; Reyes-García, V.; Madella, M. Comigrants and friends: Informal networks and the transmission of traditional ecological knowledge among seminomadic pastoralists of Gujarat, India. Ecol. Soc. 2016, 21, 20. [Google Scholar] [CrossRef] [Green Version]
- Voeks, R.A. Are women reservoirs of traditional plant knowledge? Gender, ethnobotany and globalization in northeast Brazil. Singap. J. Trop. Geogr. 2007, 28, 7–20. [Google Scholar] [CrossRef]
- Mathez-Stiefel, S.L.; Vandebroek, I. Distribution and transmission of medicinal plant knowledge in the Andean highlands: A case study from Peru and Bolivia. Evid. Based Complement. Altern. Med. 2012, 2012, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes-García, V.; Guèze, M.; Luz, A.C.; Paneque-Gálvez, J.; Macía, M.J.; Orta-Martínez, M.; Pino, J.; Rubio-Campillo, X. Evidence of traditional knowledge loss among a contemporary indigenous society. Evol. Hum. Behav. 2013, 34, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muthu, C.; Ayyanar, M.; Raja, N.; Ignacimuthu, S. Medicinal plants used by traditional healers in Kancheepuram District of Tamil Nadu, India. J. Ethnobiol. Ethnomed. 2006, 2, 43. [Google Scholar] [CrossRef] [Green Version]
- Corroto, F.; Rascón, J.; Barboza, E.; Macía, M.J. Medicinal plants for rich people vs. Medicinal plants for poor people: A case study from the Peruvian andes. Plants 2021, 10, 1634. [Google Scholar] [CrossRef] [PubMed]
- Pirker, H.; Haselmair, R.; Kuhn, E.; Schunko, C.; Vogl, C.R. Transformation of traditional knowledge of medicinal plants: The case of Tyroleans (Austria) who migrated to Australia, Brazil and Peru. J. Ethnobiol. Ethnomed. 2012, 8, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abreu, D.B.O.; Santoro, F.R.; Albuquerque, U.P.; Ladio, A.H.; Medeiros, P.M. Medicinal plant knowledge in a context of cultural pluralism: A case study in Northeastern Brazil. J. Ethnopharmacol. 2015, 175, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Kunwar, R.M.; Bussmann, R.W. Ethnobotany in the Nepal Himalaya. J. Ethnobiol. Ethnomed. 2008, 4, 24. [Google Scholar] [CrossRef] [Green Version]
- Benz, B.F.; Cevallos, J.; Santana, F.; Rosales, J.; Graf, S. Losing knowledge about plant use in the Sierra de Manantlan biosphere reserve Mexico Econ. Botany 2000, 54, 183–191. [Google Scholar] [CrossRef]
- Rai, P.K.; Lalramnghinglova, H. Ethnomedicinal plant resources of Mizoram, India: Implication of traditional knowledge in health care system. Ethnobot. Leafl. 2010, 14, 274–305. [Google Scholar]
- Vandebroek, I. The dual intracultural and intercultural relationship between medicinal plant knowledge and consensus. Econ. Bot. 2010, 64, 303–317. [Google Scholar] [CrossRef]
- World Health Organization. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines; World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF): Geneva, Switzerland, 2017. [Google Scholar]
- Wearing, S.; McDonald, M. The development of community-based tourism: Re-thinking the relationship between tour operators and development agents as intermediaries in rural and isolated area communities. J. Sustain. Tour. 2002, 10, 191–206. [Google Scholar] [CrossRef]
- De la Cruz, H.; Vilcapoma, G.; Zevallos, P.A. Ethnobotanical study of medicinal plants used by the Andean people of Canta, Lima, Peru. J. Ethnopharmacol. 2007, 111, 284–294. [Google Scholar] [CrossRef]
- Monigatti, M.; Bussmann, R.W.; Weckerle, C.S. Medicinal plant use in two Andean communities located at different altitudes in the Bolívar Province, Peru. J. Ethnopharmacol. 2013, 145, 450–464. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, M.; Malpartida, S.B.; Santiago, H.B.; Jullian, V.; Bourdy, G. Hot and cold: Medicinal plant uses in Quechua speaking communities in the high Andes (Callejón de Huaylas, Ancash, Perú). J. Ethnopharmacol. 2014, 155, 1093–1117. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Biset, J.; Campos de la Cruz, J.; Epiquién Rivera, M.A.; Canigueral, S. A first survey on the medicinal plants of the Chazuta valley (Peruvian Amazon). J. Ethnopharmacol. 2009, 122, 333–362. [Google Scholar] [CrossRef]
- Sylvester, O.; Segura, A.G.; Davidson-Hunt, I.J. Wild food harvesting and access by household and generation in the Talamanca Bribri Indigenous Territory, Costa Rica. Hum. Ecol. 2016, 44, 449–461. [Google Scholar] [CrossRef]
- Arruda, H.L.S.; Santos, J.F.O.; Albuquerque, U.P.; Ramos, M.A. Influence of Socioeconomic Factors on the Knowledge and Consumption of Firewood in the Atlantic Forest of Northeast Brazil. Econ. Bot. 2019, 73, 1–12. [Google Scholar] [CrossRef]
- Case, R.J.; Pauli, G.F.; Soejarto, D.D. Factors in maintaining indigenous knowledge among ethnic communities of Manus Island. Econ. Bot. 2005, 59, 356–365. [Google Scholar] [CrossRef]
- McMillen, H. Ethnobotanical knowledge transmission and evolution: The case of medicinal markets in Tanga, Tanzania. Econ. Bot. 2012, 66, 121–131. [Google Scholar] [CrossRef]
- Vandebroek, I.; Balick, M.J. Globalization and loss of plant knowledge: Challenging the paradigm. PLoS ONE 2012, 7, e37643. [Google Scholar] [CrossRef] [PubMed]
- Miguéis, G.S.; Da Silva, R.H.; Júnior, G.A.D.; Guarim-Neto, G. Plants used by the rural community of Bananal, Mato Grosso, Brazil: Aspects of popular knowledge. PLoS ONE 2019, 14, e0210488. [Google Scholar] [CrossRef] [PubMed]
- Byg, A.; Balslev, H. Diversity and use of palms in Zahamena, eastern Madagascar. Biodivers. Conserv. 2001, 10, 951–970. [Google Scholar] [CrossRef]
- Singhal, R. Medicinal plants and primary health care: The role of gender. J. Health Manag. 2005, 7, 277–293. [Google Scholar] [CrossRef]
- Signorini, M.A.; Piredda, M.; Bruschi, P. Plants and traditional knowledge: An ethnobotanical investigation on Monte Ortobene (Nuoro, Sardinia). J. Ethnobiol. Ethnomed. 2009, 5, 6. [Google Scholar] [CrossRef] [Green Version]
- Nolan, J.M.; Robbins, M.C. Cultural conservation of medicinal plant use in the Ozarks. Hum. Organ. 1999, 58, 67–72. [Google Scholar] [CrossRef]
- Menendez-Baceta, G.; Pardo-de-Santayana, M.; Aceituno-Mata, L.; Tardío, J.; Reyes-García, V. Trends in wild food plants uses in Gorbeialdea (Basque Country). Appetite 2017, 112, 9–16. [Google Scholar] [CrossRef]
- Paniagua-Zambrana, N.; Cámara-Leret, R.; Bussmann, R.; Macía, M.J. The influence of socioeconomic factors on traditional knowledge: A cross scale comparison of palm use in northwestern South America. Ecol. Soc. 2014, 19, 9. [Google Scholar] [CrossRef] [Green Version]
- Andriamparany, J.N.; Brinkmann, K.; Jeannoda, V.; Buerkert, A. Effects of socio-economic household characteristics on traditional knowledge and usage of wild yams and medicinal plants in the Mahafaly region of south-western Madagascar. J. Ethnobiol. Ethnomed. 2014, 10, 82. [Google Scholar] [CrossRef] [Green Version]
- Mauro, F.; Hardison, P.D. Traditional knowledge of indigenous and local communities: International debate and policy initiatives. Ecol. Appl. 2000, 10, 1263–1269. [Google Scholar] [CrossRef]
- Toda, M.; Salgado, E.L.R.; Masuda, M. Assessing medicinal plants as the linkage between healthcare, livelihood and biodiversity: A case study from native villages surrounding a second-tier city in the central Peruvian Amazon. Tropics 2016, 25, 53–65. [Google Scholar] [CrossRef]
- Bellia, G.; Pieroni, A. Isolated, but transnational: The glocal nature of Waldensian ethnobotany, Western Alps, NW Italy. J. Ethnobiol. Ethnomed. 2015, 11, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leatherman, T.L.; Carey, J.W.; Thomas, R.B. Socioeconomic change and patterns of growth in the Andes. Amer. J. Phys. Anthr. 1995, 97, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Vandebroek, I.; Calewaert, J.B.; Sanca, S.; Semo, L.; Van Damme, P.; Van Puyvelde, L.; De Kimpe, N. Use of medicinal plants and pharmaceuticals by indigenous communities in the Bolivian Andes and Amazon. Bull. World Health Organ. 2004, 82, 243–250. [Google Scholar]
- Sandlos, J.; Keeling, A. Aboriginal communities, traditional knowledge, and the environmental legacies of extractive development in Canada. Extr. Ind. Soc. 2015, 3, 278–287. [Google Scholar] [CrossRef]
- Johnston, A. Indigenous peoples and ecotourism: Bringing indigenous knowledge and rights into the sustainability equation. Tour. Recreat. Res. 2000, 25, 89–96. [Google Scholar] [CrossRef]
- Cotruvo, J.A. WHO Guidelines for Drinking Water Quality: First Addendum to the Fourth Edition. J. Am. Water Work. Assoc. 2017, 109, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Pieroni, A.; Quave, C. Traditional pharmacopoeias and medicines among Albanians and Italians in southern Italy: A comparison. J. Ethnopharmacol. 2005, 101, 258–270. [Google Scholar] [CrossRef]
- Eyssartier, C.; Ladio, A.H.; Lozada, M. Cultural transmission of traditional knowledge in two populations of north-western Patagonia. J. Ethnobiol. Ethnomed. 2008, 4, 25. [Google Scholar] [CrossRef] [Green Version]
- León, B.; Pitman, N.; Roque, J. Introducción a las plantas endémicas del Perú. Rev. Per. Bio. 2006, 13, 9–22. [Google Scholar] [CrossRef] [Green Version]
- SENAMHI (Servicio Nacional de Meteorología e Hidrología). Reporte mensual de Meteorología y Climatología. 2019. Lima, Peru. Available online: https://www.senamhi.gob.pe/?p=descarga-datos-hidrometeorologicos/>/ (accessed on 6 March 2019).
- INEI (Instituto Nacional de Estadística e Informática). Síntesis Estadística 2015. Boletín Especial, N° 18, Septiembre, 2015. Lima: INEI. Available online: https://www.inei.gob.pe/estadisticas/indice-tematico/poblacion-y-vivienda/ (accessed on 10 March 2019).
- Corroto, F.; Torres, O.A.G.; Macía, M.J. Different patterns in medicinal plant use along an elevational gradient in northern Peruvian Andes. J. Ethnopharmacol. 2019, 239, 111924. [Google Scholar] [CrossRef]
- The Plant List: A Working List of All Known Plant Species. 2018. Available online: http://www.theplantlist.org (accessed on 4 December 2018).
- Chase, M.W.; Christenhusz, M.J.M.; Fay, M.F.; Judd, W.S. An update of the Angiosperm Phylogeny Group classification for the orders and families of flowering plants: APG IV. Bot. J. Linn. Soc. 2016, 181, 1–20. [Google Scholar] [CrossRef] [Green Version]
- WONCA. ICPC-2-R: International Classification of Primary Care, 2nd ed.; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Macía, M.J.; Armesilla, P.J.; Cámara-Leret, R.; Paniagua-Zambrana, N.; Villalba, S.; Balslev, H.; Pardo-de-Santayana, M. Palm uses in northwestern South America: A quantitative review. Bot. Rev. 2011, 77, 462–570. [Google Scholar] [CrossRef]
- Gruca, M.; Cámara-Leret, R.; Macía, M.J.; Balslev, H. New categories for traditional medicine in the Economic Botany Data Collection Standard. J. Ethnopharmacol. 2014, 155, 1388–1392. [Google Scholar] [CrossRef]
- Di Rienzo, J.A.; Casanoves, F.; Balzarini, M.G.; Gonzalez, L.; Tablada, M.; Robledo, C.W. InfoStat version 2011. Grupo InfoStat, FCA. 2011. Universidad Nacional de Córdoba, Argentina. Available online: http://www.infostat.com.ar (accessed on 5 November 2018).
- SCBD (Secretariat of the Convention on Biological Diversity). Nagoya Protocol on Access to Genetic Resources and the Fair and Equitable Sharing of Benefits Arising from Their Utilization to the Convention on Biological Diversity; Secretariat of the Convention on Biological Diversity: Montreal, QC, Canada, 2011; pp. 1–15. Available online: https://www.cbd.int/abs/doc/protocol/nagoya-protocol-en.pdf (accessed on 23 March 2020).
- SCBD (Secretariat of the Convention on Biological Diversity). Bonn Guidelines on Access to Genetic Resources and Fair and Equitable Sharing of the Benefits Arising Out of Their Utilization; Secretariat of the Convention on Biological Diversity: Montreal, QC, Canada, 2002; pp. 1–26. Available online: https://www.cbd.int/doc/publications/cbd-bonn-gdls-en.pdf (accessed on 22 March 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ecoregion—Province | Locality | # Medicinal Species | # Medicinal Plant Usage | Age | Family Size |
|---|---|---|---|---|---|
| Lowlands—Bongará | Cuispes | 19.4 ± 6.4 | 22.2 ± 7.1 | 0.08 | 0.14 |
| San Carlos | 22.0 ± 5.8 | 24.6 ± 7.9 | 0.17 | 0.03 | |
| Valera | 9.6 ± 3.6 | 10.8 ± 4.5 | 0.14 | 0.28 | |
| Lowlands—R. Mendoza | Huambo | 10.6 ± 3.9 | 12.3 ± 4.1 | 0.24 | 0.04 |
| Santa Rosa | 13.1 ± 4.0 | 13.8 ± 4.2 | 0.15 | 0.19 | |
| Totora | 18.5 ± 4.4 | 20.8 ± 5.2 | 0.09 | 0.14 | |
| Highlands—Chachapoyas | Granada | 26.9 ± 7.8 | 34.8 ± 8.9 | 0.23 | 0.28 |
| Olleros | 27.2 ± 7.3 | 35.1 ± 7.8 | 0.29 | 0.09 | |
| Quinjalca | 26.8 ± 7.5 | 31.8 ± 7.6 | 0.06 | 0.11 | |
| Highlands—Luya | Longuita | 22.4 ± 6.6 | 26.2 ± 7.1 | 0.12 | 0.13 |
| María | 19.0 ± 5.9 | 22.3 ± 6.6 | 0.12 | 0.25 | |
| Yomblón | 20.1 ± 6.0 | 23.1 ± 6.8 | 0.19 | 0.18 |
| Attributes | High | Medium | Low |
|---|---|---|---|
| Proximity of tourist attractions | 19.7 ± 6.4 | 23.4 ± 7.2 | 30.1 ± 8.4 |
| Proximity to paved roads | 19.1 ± 6.7 | 19.2 ± 6.4 | 31.2 ± 8.2 |
| Proximity to hospitals | 15.6 ± 5.4 | 21.2 ± 6.8 | 31.2 ± 8.2 |
| Proximity to big markets | 17.4 ± 5.6 | 24.2 ± 7.5 | 31.2 ± 8.2 |
| Chlorination of drinking water | 18.9 ± 6.1 | – | 29.1 ± 8.0 |
| Attributes | Lowlands—Bongará | Lowlands—Mendoza | Highlands—Chachapoyas | Highlands—Luya | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cuispes | San Carlos | Valera | Huambo | Santa Rosa | Totora | Granada | Olleros | Quinjalca | Longuita | María | Yomblón | |
| Intercept | 45.462 | 24.553 | 35.234 ** | 11.791 | 23.797 | 34.316 * | 37.979 | 24.263 | 11.641 | 19.558 | 42.486 | 23.159 |
| Women | 1.245 | 3.244 ** | 2.506 * | 0.821 | 1.109 | 2.068 * | 1.110 | 1.080 | 2.471 * | 0.809 | 0.908 | 0.859 |
| Education | 1.077 | −3.618 * | 0.714 | −1.752 | −4.291 ** | −2.662 * | −0.580 | 0.490 | 0.520 | −1.532 | −0.400 | −3.246 * |
| Occupation | 1.012 | −4.783 ** | −1.527 | 0.206 | −4.935 ** | −1.672 | nd | 0.919 | −0.353 | −1.992 | −0.506 | 0.065 |
| Migratory status | −0.373 | −0.348 | −0.161 | 0.508 | 0.422 | 0.534 | −0.161 | −1.029 | −0.015 | −3.347 * | −1.656 | −0.107 |
| Time-in-residence | 0.927 | 0.791 | 0.734 | 0.839 | 0.248 | 1.449 | 0.811 | 1.599 | −0.143 | 2.471 * | 1.711 | 2.124 * |
| Family size | 0.697 | 0.409 | 0.218 | 0.703 | 1.405 | 0.616 | 2.072 * | 2.782 * | 0.979 | 1.405 | 0.779 | 3.271 * |
| Transport | 0.863 | 0.919 | −0.969 | −0.389 | −0.835 | −2.138 * | 0.753 | −0.536 | 0.767 | −1.596 | −0.901 | −1.528 |
| Tools | −3.927 * | −1.207 | −4.768 * | −0.361 | −0.738 | −0.424 | −4.284 * | −8.122 ** | 0.326 | 0.951 | 1.298 | −0.966 |
| Technologic access | −0.406 | −0.073 | −1.589 | −1.771 * | −2.741 ** | 0.053 | −2.195 * | −0.252 | −1.055 | 0.857 | −0.238 | −0.548 |
| Locality | 8.682 | 5.466 | 6.022 | 4.440 | 8.212 | 6.799 | 6.245 | 3.599 | 2.421 | 3.328 | 7.056 | 5.592 |
| Interviewed residuals | 6.324 | 3.026 | 4.073 | 1.893 | 5.889 | 3.802 | 3.935 | 1.447 | 0.971 | 1.722 | 4.800 | 3.232 |
| Attributes | Bongará (Lowlands) | R. Mendoza (Lowlands) | Chachapoyas (Highlands) | Luya (Highlands) |
|---|---|---|---|---|
| Agriculture | Subsistence agriculture (corn, fruit trees, and pasture) | Predominance of productive coffee | Predominance of productive Andean tubers, corn, and pasture | Predominance of productive Andean tubers, corn, and pasture |
| Livestock | Extensive subsistence cattle | Intensive bovine cattle and swine | Extensive subsistence cattle | Extensive subsistence cattle |
| Fisheries | Small-scale trout farms | Fishing in rivers | Small-scale trout farms | Small-scale trout farms |
| Tourist attractions | Yes | No | No | Yes |
| Paved roads | No | Yes | No | Yes |
| Hospitals | No | Yes | No | No |
| Big markets | Yes | Yes | No | Yes |
| Water chlorination | Yes | Yes | No | Yes |
| Population | 2588 | 3277 | 1034 | 1991 |
| Independent Variable Name | Variable Scale | Variable Type | Variable Classification |
|---|---|---|---|
| Gender | Individual | Nominal | (0) Men; (1) Women |
| Age (years) | Individual | Continuous | Between 18 and 91 |
| Education | Individual | Ordinal | (0) No education; (1) Primary education; (2) High education |
| Occupation | Individual | Ordinal | (0) Basic qualification; (1) Medium/High qualifiation |
| Migratory status | Individual | Ordinal | (0) Non-migrant; (1) Migrant |
| Time-in-residence | Individual | Ordinal | (0) Between 0–15 years; (1) Between 16–30 years; (2) More than 30 years |
| Family size | Familiar | Continuous | Between 0–11 children |
| Means of transport | Familiar | Ordinal | (0) No transport; (1) Animal and bicycle; (2) Motorbike, car, or similar |
| Tools | Familiar | Ordinal | (0) No tools; (1) Basic tools; (2) Semi-automatic tools |
| Technological services | Familiar | Ordinal | (0) Radio, mobile phone, TV; (1) Cable TV; (2) Internet |
| Farm animals | Familiar | Ordinal | (0) No animals; (1) 1–15 animals; (2) >15 animals |
| Farm size | Familiar | Ordinal | (0) 0–1 ha; (1) 1–5 ha; (2) >5 ha |
| House quality | Familiar | Ordinal | (0) Some defects; (1) Good quality, no defects |
| Proximity to tourist attractions | Locality | Ordinal | (0) Less than 1 h; (1) 1–2 h; (2) More than 2 h |
| Proximity to paved roads | Locality | Ordinal | (0) Less than 1 h; (1) 1–2 h; (2) More than 2 h |
| Proximity to hospitals | Locality | Ordinal | (0) Less than 1 h; (1) 1–2 h; (2) More than 2 h |
| Proximity to big markets | Locality | Ordinal | (0) Less than 1 h; (1) 1–2 h; (2) More than 2 h |
| Water quality | Locality | Ordinal | (0) Drinking water with a chlorination system; (1) Unguarded, without a chlorination system |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corroto, F.; Gamarra Torres, O.A.; Macía, M.J. Understanding the Influence of Socioeconomic Variables on Medicinal Plant Knowledge in the Peruvian Andes. Plants 2022, 11, 2681. https://doi.org/10.3390/plants11202681
Corroto F, Gamarra Torres OA, Macía MJ. Understanding the Influence of Socioeconomic Variables on Medicinal Plant Knowledge in the Peruvian Andes. Plants. 2022; 11(20):2681. https://doi.org/10.3390/plants11202681
Chicago/Turabian StyleCorroto, Fernando, Oscar Andrés Gamarra Torres, and Manuel J. Macía. 2022. "Understanding the Influence of Socioeconomic Variables on Medicinal Plant Knowledge in the Peruvian Andes" Plants 11, no. 20: 2681. https://doi.org/10.3390/plants11202681
APA StyleCorroto, F., Gamarra Torres, O. A., & Macía, M. J. (2022). Understanding the Influence of Socioeconomic Variables on Medicinal Plant Knowledge in the Peruvian Andes. Plants, 11(20), 2681. https://doi.org/10.3390/plants11202681