Design, Fabrication, and Testing of an Internet Connected Intravenous Drip Monitoring Device

Abstract
:1. Introduction
2. Materials and Methods
2.1. Working Principle
2.2. Design and Fabrication
2.3. Algorithm Description and Cloud
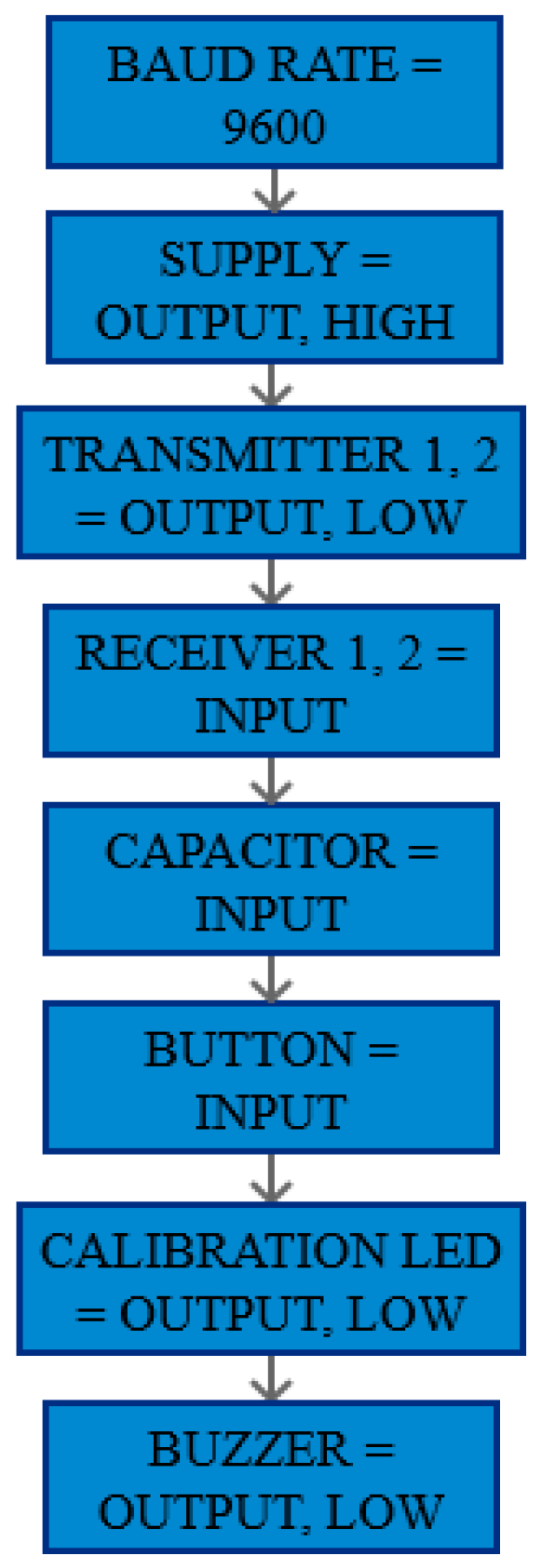
2.3.1. Setup Loop
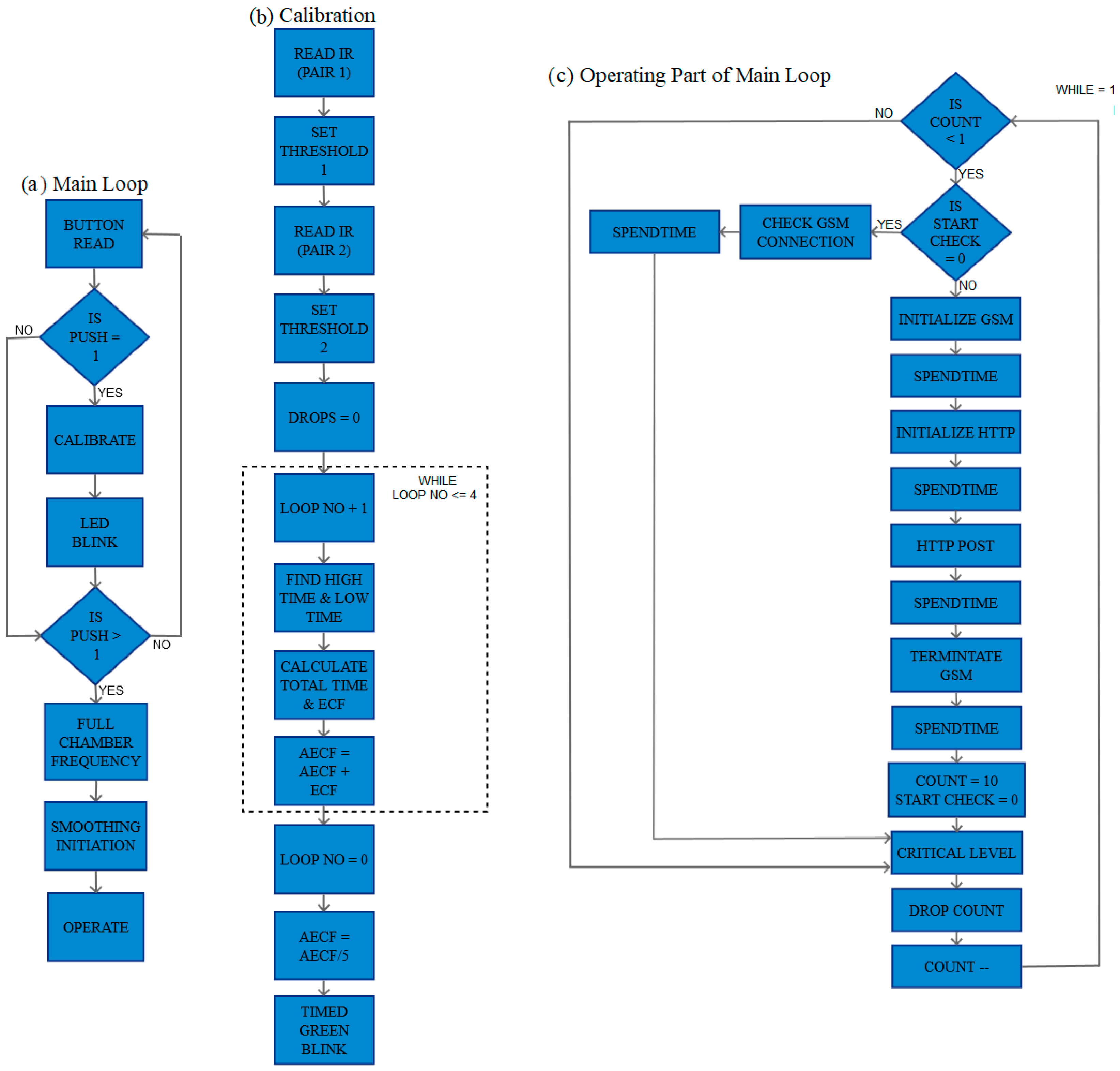
2.3.2. Main Loop
2.3.3. GSM Initialization & GSM Termination
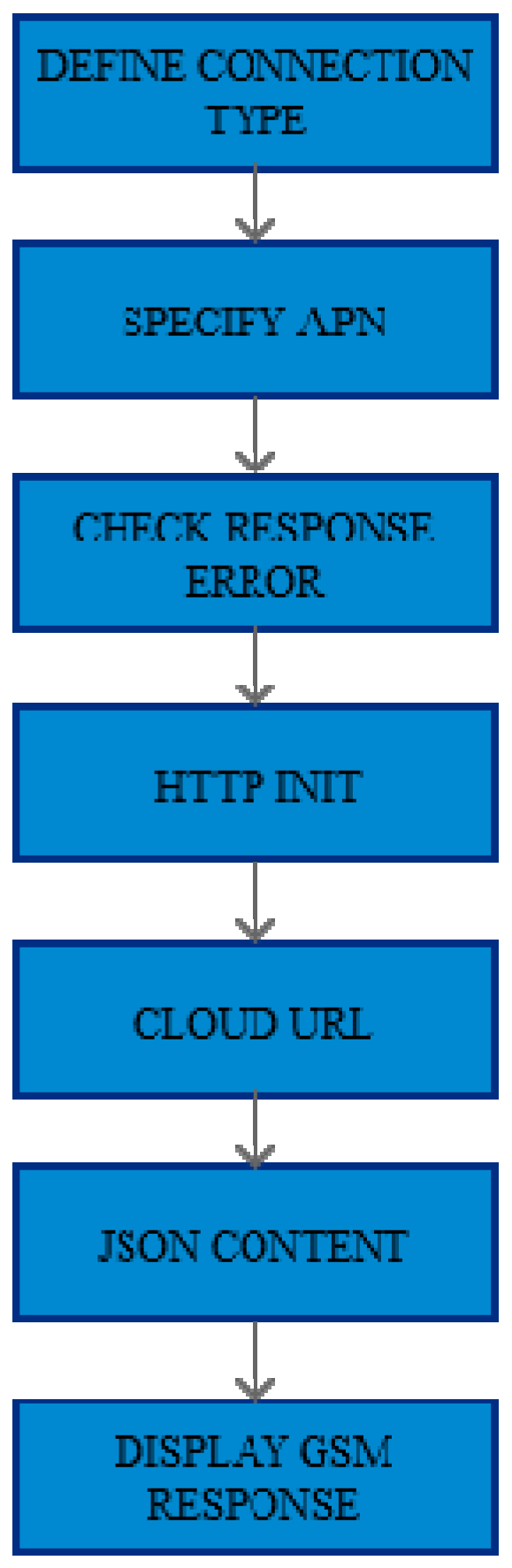
2.3.4. HTTP Initialization
2.3.5. Post Data
2.3.6. Drop Count
2.3.7. Critical Level using IIR Filtering
2.3.8. Spend Time
2.3.9. Green Blink and Timed Green Blink
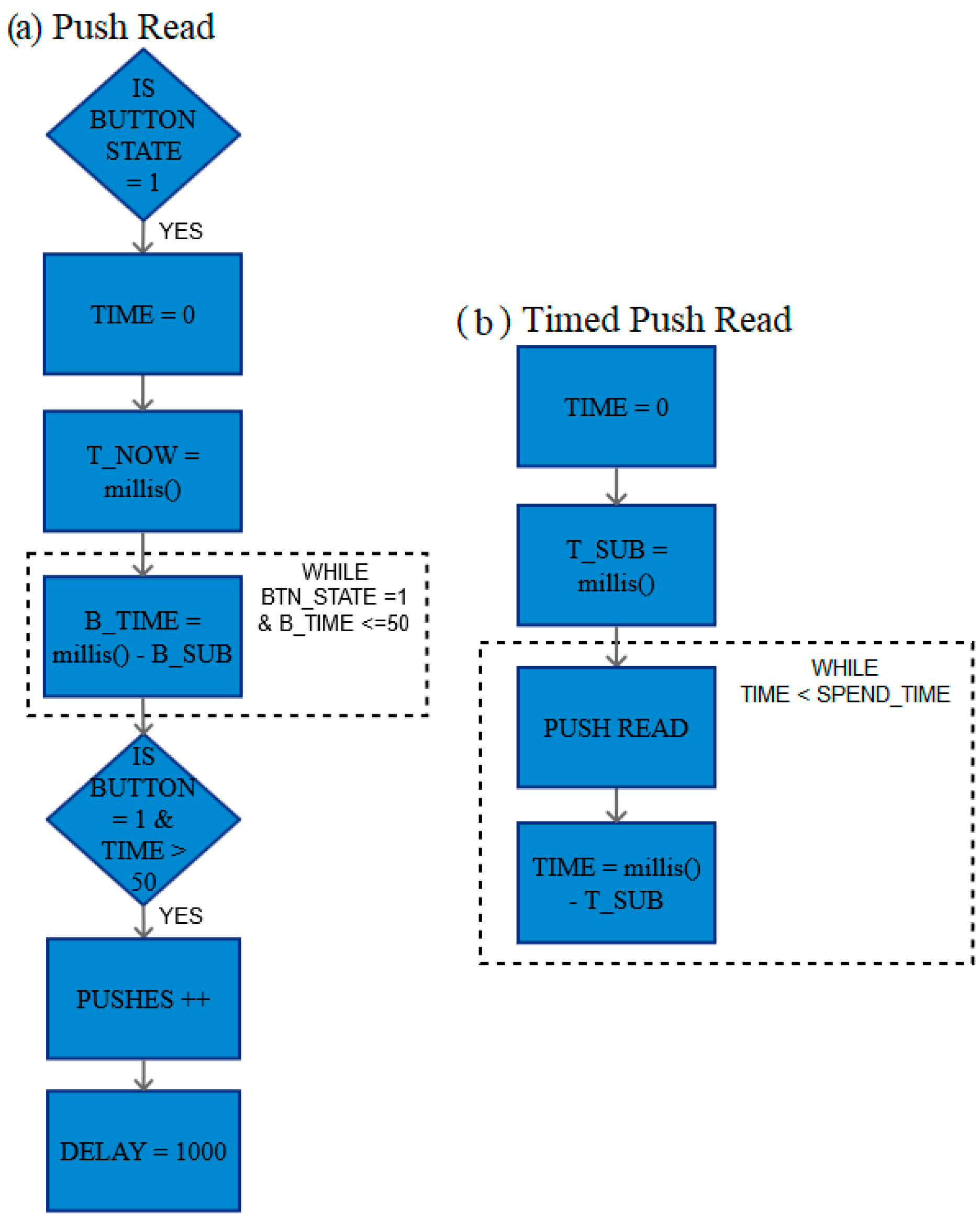
2.3.10. Push Read and Timed Push Read
2.3.11. GSM Response and GSM Connection Check
3. Results
3.1. Accuracy of Drop Count
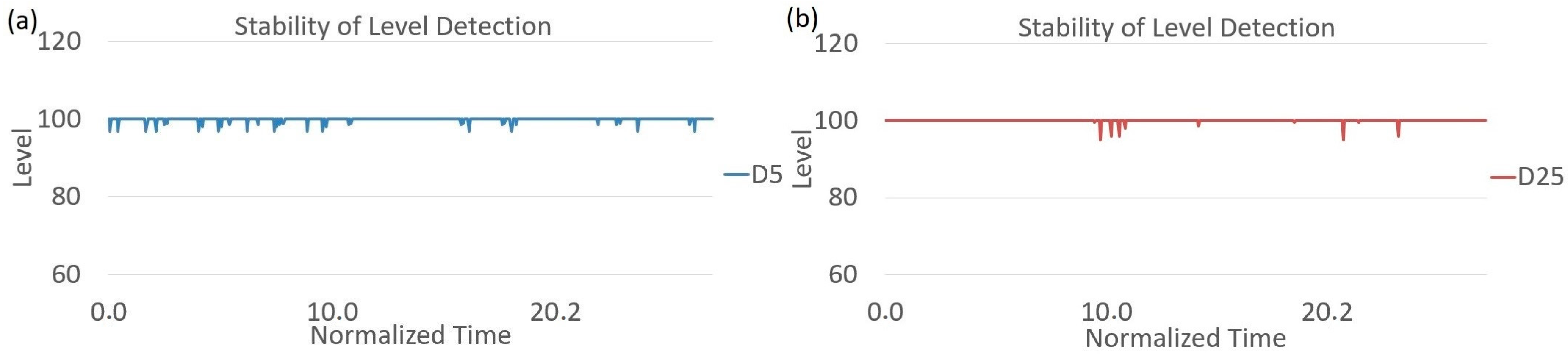
3.2. Stability of Level Detection
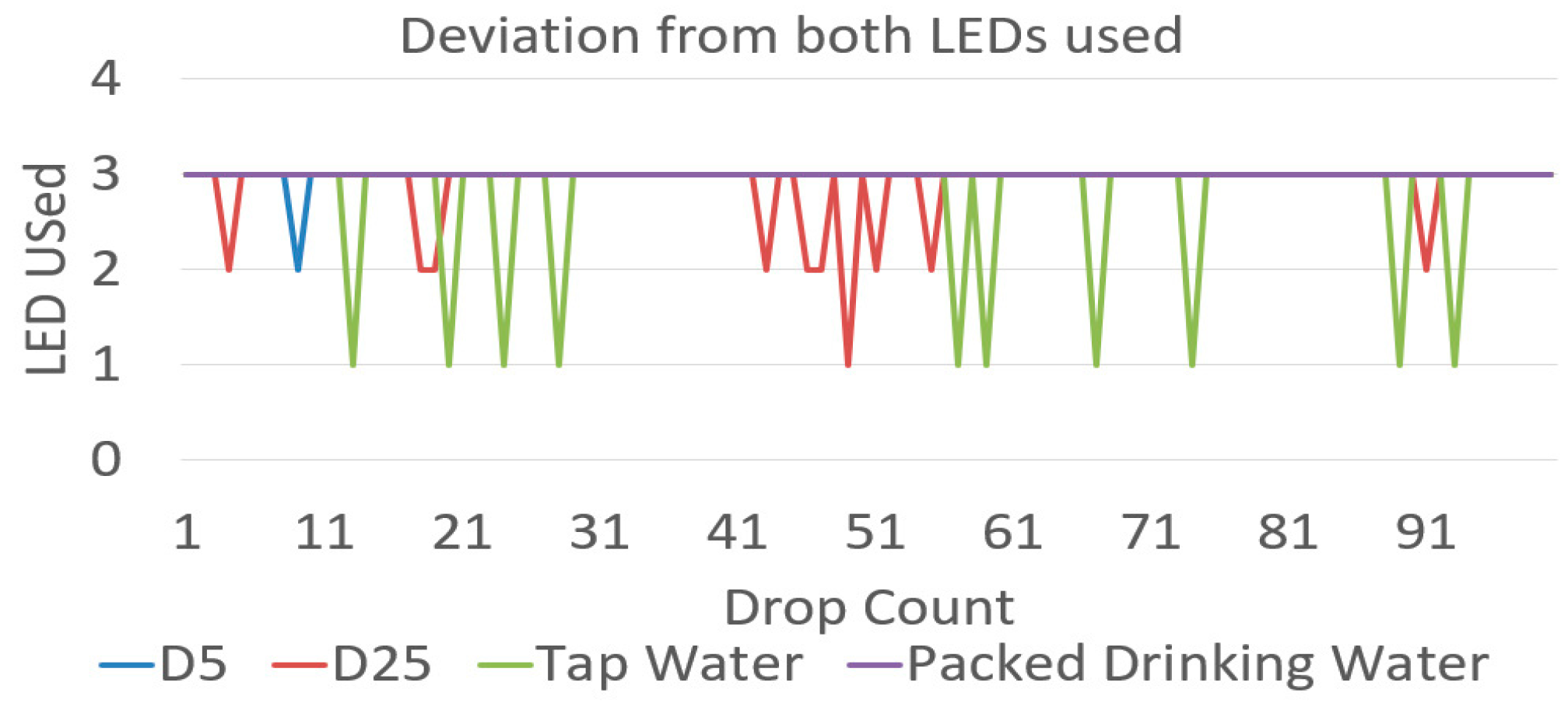
3.3. Change in Fluid Used
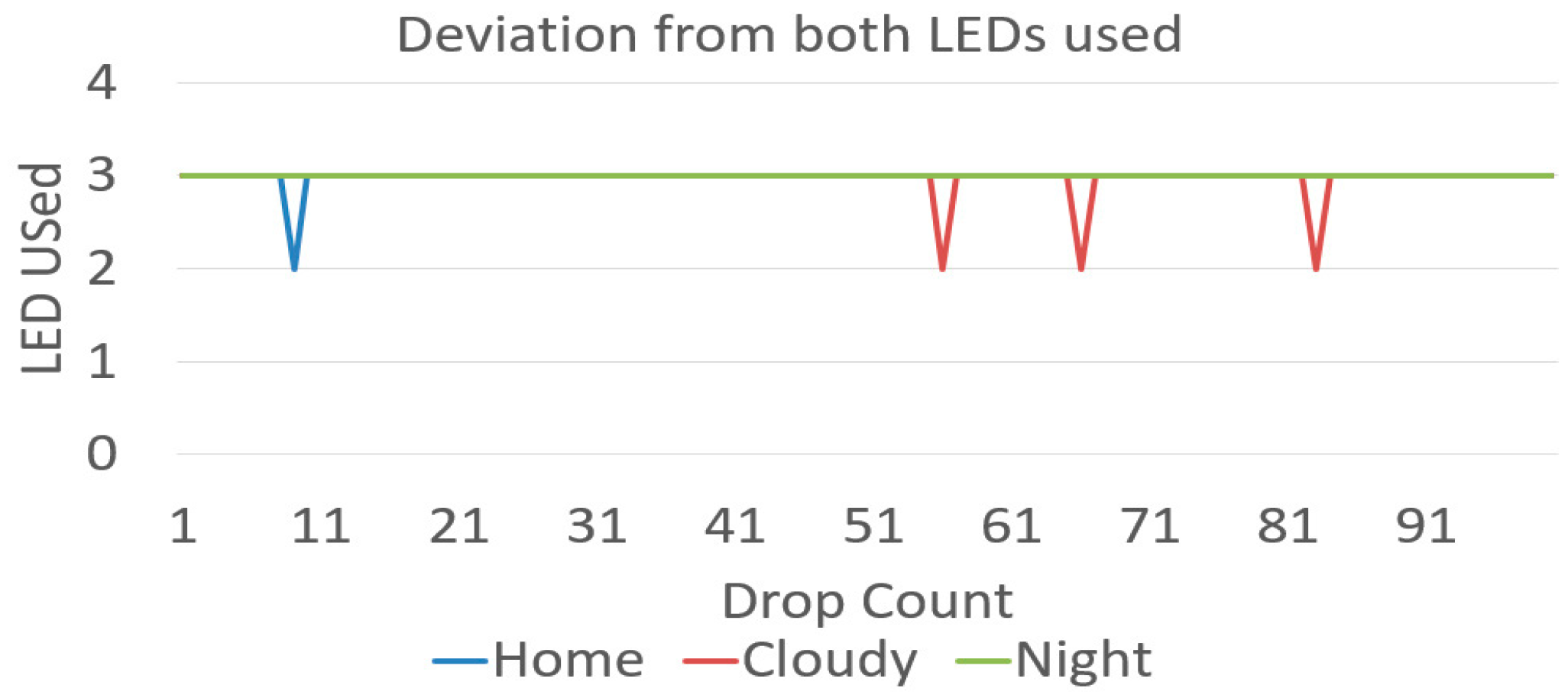
3.4. Change in Ambient Conditions
3.5. End Chamber Conditions
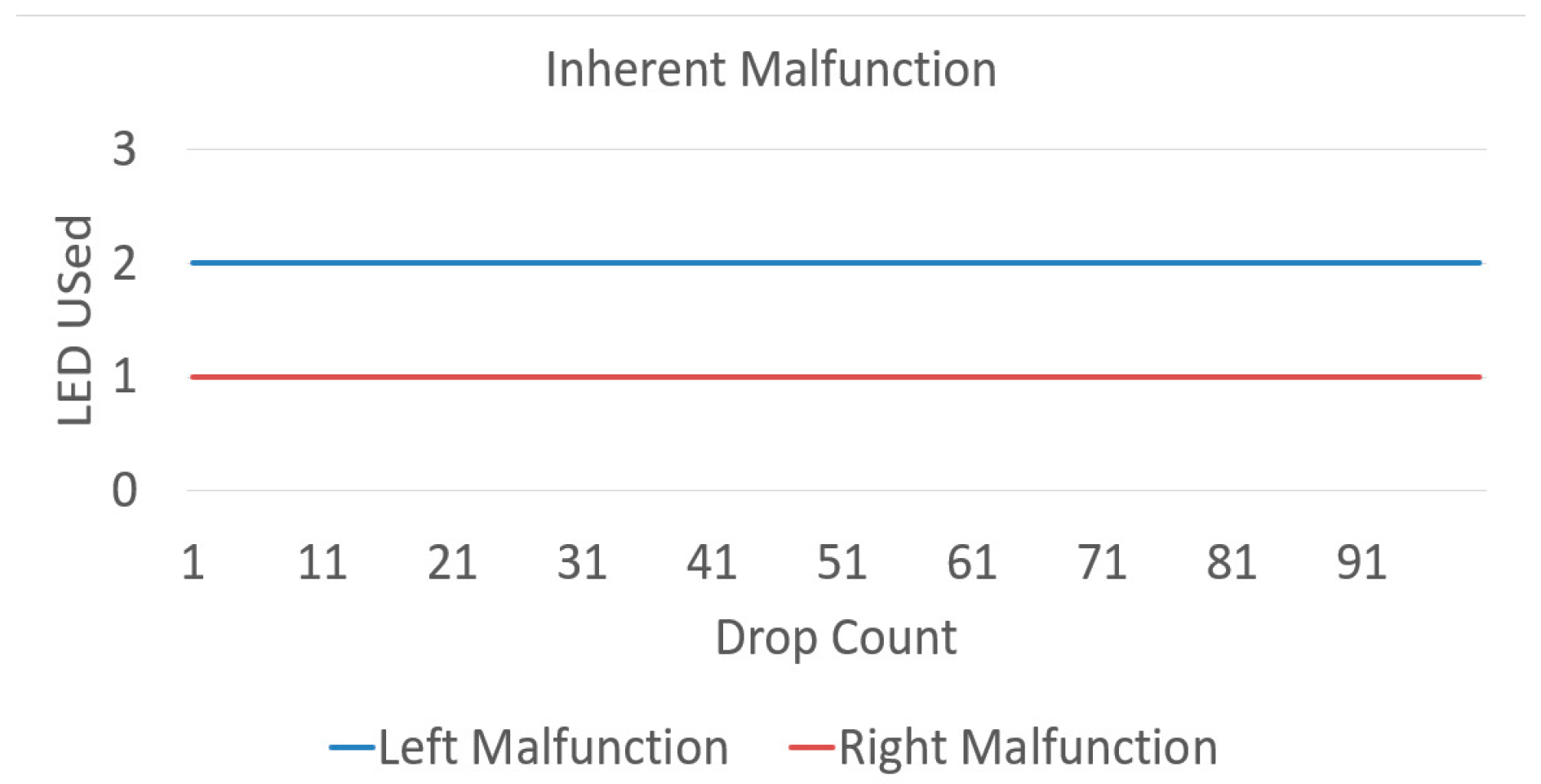
3.6. LED Malfunction
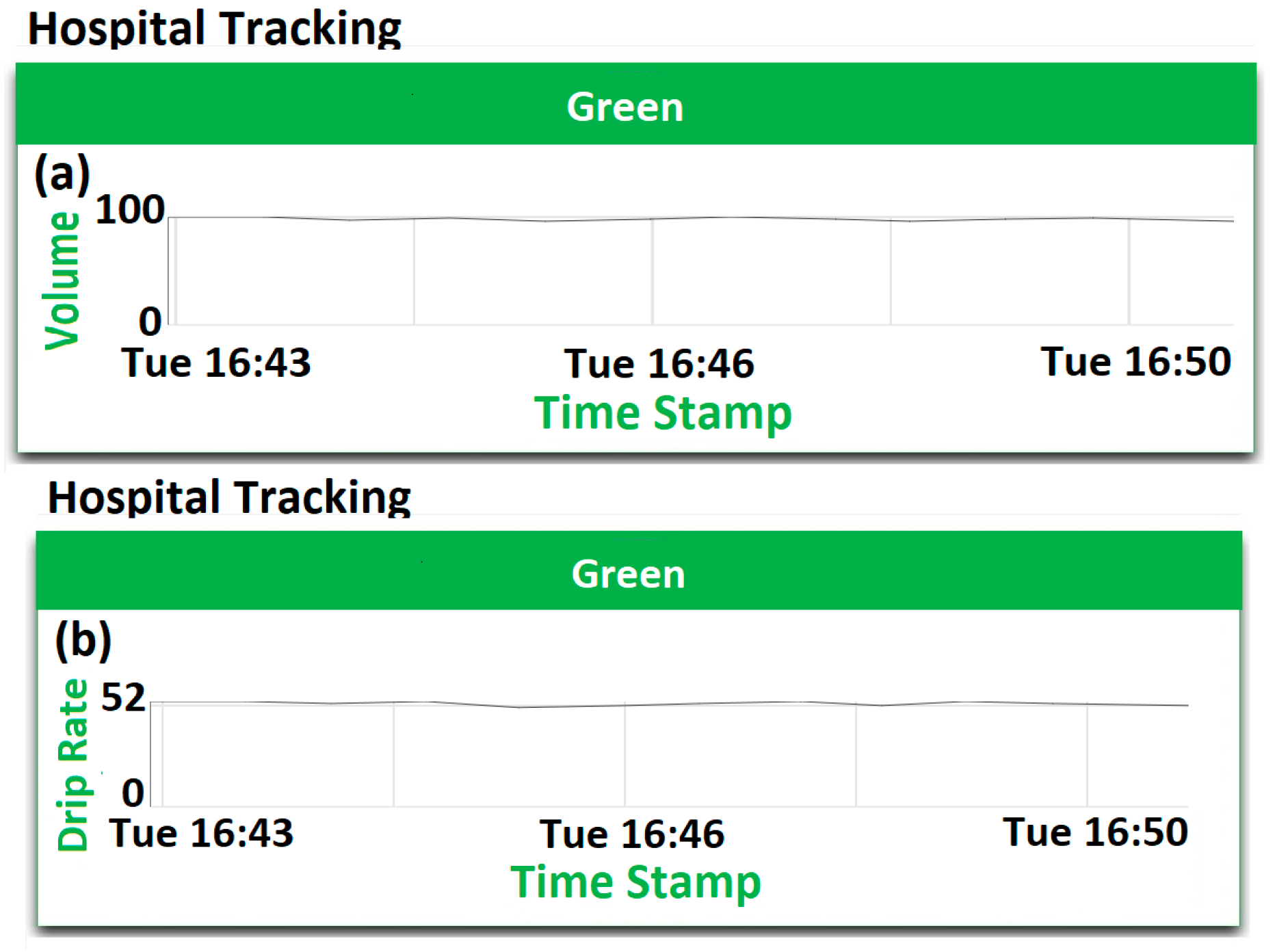
3.7. Cloud Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Agarwal, S.S.; Kumar, L.; Chavali, K.H.; Mestri, S.C. Fatal Venous Air Embolism Following Intravenous Infusion. J Forensic Sci. 2009, 53, 682–684. [Google Scholar] [CrossRef] [PubMed]
- Laskey, A.L.; Dyer, C.; Tobias, J.D. Venous Air Embolism During Home Infusion Therapy. Pediatrics 2002, 109, e15. [Google Scholar] [CrossRef] [PubMed]
- Senior, K. Wanted: 2.4 million nurses, and that’s just in India, Special theme—Health workforce retention in remote and rural areas. Bull. World Health Organ. 2010, 88, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; You, L.M.; Zheng, J.; Liu, K.; Fang, J.B.; Hou, S.X.; Lu, M.M.; Lv, A.L.; Ma, W.G.; Wang, H.H.; et al. Nurse Staffing Levels Make a Difference on Patient Outcomes: A Multisite Study in Chinese Hospitals. J. Nurs. Scholarsh. 2012, 44, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Anliker, U.; Ward, J.A.; Lukowicz, P.; Dolveck, F.; Baer, M.; Keita, F.; Schenker, E.B.; Catarsi, F.; Coluccini, L.; Belardinelli, A.; et al. AMON: A Wearable Multiparameter Medical Monitoring and Alert System. IEEE Trans. Inf. Technol. Biomed. 2004, 8, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.G.; Chen, K.C.; Hsiao, C.C.; Tseng, C.L. A Mobile Care System with Alert Mechanism. IEEE Trans. Inf. Technol. Biomed. 2007, 11, 507–517. [Google Scholar] [CrossRef] [PubMed]
- Paschou, M.; Sakkopoulos, E.; Sourla, E.; Tsakalidis, A. Health Internet of Things: Metrics and methods for efficient data transfer. Simul. Model. Pract. Theory 2013, 34, 186–199. [Google Scholar] [CrossRef]
- Xu, B.; Xu, L.D.; Cai, H.; Xie, C.; Hu, J.; Bu, F. Ubiquitous Data Accessing Method in IoT-Based Information System for Emergency Medical Services. IEEE Trans. Ind. Inf. 2014, 10, 1578–1586. [Google Scholar] [CrossRef]
- Maia, P.; Batista, T.; Cavalcante, E.; Baffa, A.; Delicatod, F.C.; Pires, P.F.; Zomaya, A. A Web platform for interconnecting body sensors and improving health care. Procedia Comput. Sci. 2014, 40, 135–142. [Google Scholar] [CrossRef]
- Kamble, V.V.; Pandey, P.C.; Gadgil, C.P.; Choudhary, D.S. Monitoring of Intravenous Drip Rate. In Proceedings of the ICBME, Bangalore, India, 21–24 December 2001; pp. 51–55. [Google Scholar]
- Thariyan, K.K.; Verma, S.; Taneja, S.R.; Gupta, R.C.; Ahluwalia, S.S. Design and Development of a Unique Drop Sensing Unit for Infusion Pump. J. Sci. Ind. Res. 2002, 61, 798–801. [Google Scholar]
- Bilbao, U.; Bustamante, P.; Guarretxena, N.; Domingo, J.S. A new Wireless Sensor for Intravenous Dripping Detection. In Proceedings of the International Conference on Sensor Technologies and Applications, Valencia, Spain, 14–20 October 2007; IEEE: Piscataway, NJ, USA, 2007; pp. 30–35. [Google Scholar]
- Yang, W.; Sun, L. A novel medical infusion monitoring system based on ZigBee wireless sensor network. In Proceedings of the 2009 International Symposium on Web Information Systems and Applications (WISA’09), Nanchang, China, 22–24 May 2009; Springer: New York, NY, USA; pp. 291–293. [Google Scholar]
- Bustamante, P.; Solas, G.; Grandez, K.; Bilbao, U. A new Wireless Sensor for Intravenous Dripping Detection. Int. J. Adv. Netw. Serv. 2010, 3, 50–58. [Google Scholar]
- Vasuki, R.; Dennis, C.; Chander, H.P. Designing a portable monitoring device to measure the drips rate. Middle East J. Sci. Res. 2011, 1, 29–35. [Google Scholar]
- Wei, Q.; Lee, J.H.; Seong, K.W.; Kim, M.N.; Cho, J.H. The Design of a Wireless Flexible Capacitive Sensor Detection System to Detect Liquid Level in Plastic Bag Intravenous Drip Sets. Biomed Eng. Lett. 2011, 1, 247–253. [Google Scholar] [CrossRef]
- Cataldo, A.; Cannazza, G.; Giaquinto, N.; Trotta, A.; Andria, G. Microwave TDR for real-time control of intravenous drip infusions. IEEE Trans. Inst. Meas. 2012, 61, 1866–1873. [Google Scholar] [CrossRef]
- Du, Q.; Liu, J.; Tian, L. Simulation and Design of Intravenous Infusion Dripping Rate Detection based on Infrared Ray. In Proceedings of the 3rd International Conference on Multimedia Technology (ICMT 2013), Guangzhou, China, 29 November–1 December 2013; Atlantis Press: Paris, France, 2013. [Google Scholar] [CrossRef]
- Chen, C.L.; Hsieh, N.C.; Hung, L.P. Developing a wireless based dynamic management mechanism for intravenous drip scheduling. Int. J. Ad Hoc Ubiquitous Comput. 2015, 19, 208–220. [Google Scholar] [CrossRef]
- Priyadharshini, R.; Mithuna, S.; Vasanth, K.U.; Kalpana, D.S.; Suthanthira, V.N. Automatic Intravenous Fluid Level Indication System for Hospitals. Int. J. Res. Appl. Sci. Eng. Technol. 2015, 3, 427–432. [Google Scholar]
- Alas, G.R.D., Jr.; Padilla, J.N.; Tanguilig, B.T., III. Intravenous piggyback infusion control and monitoring system using wireless technology. Int. J. Adv. Technol. Eng. Explor. 2016, 3, 50–57. [Google Scholar] [CrossRef]
- Raghavendra, B.; Vijyalakshmi, K.; Arora, M. Intravenous Drip meter & controller, need analysis and conceptual design. In Proceedings of the 8th International Conference on Communication Systems & Networks (COMSNETS), Banglore, India, 5–9 January 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 1–5. [Google Scholar]
- Pandi, S.A.; Bharathi, S.; Bharathiraja, R.; Kiruthika, L.; Boopathy, S. Novel approach to maintain the real time instantaneous data from patient using ultra low power micro controller. Int. J. Adv. Res. Compt. Sci. 2017, 8, 452–455. [Google Scholar] [CrossRef]
- Gayathri, S.; Ganesh, C.S.S. Automatic indication system of glucose level in glucose trip bottle. Int. J. Multidiscip. Res. Mod. Educ. 2017, 3, 148–151. [Google Scholar] [CrossRef]
- Krishnasamy, R.R.; Shabana, N.; Tanmayee, P.; Loganathan, S.; Velmathi, G. Smart drip infusion monitoring system for instant alert—Through nRF24L01. In Proceedings of the International Conference on Nextgen Electronics Technologies, Chennai, India, 23–25March 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 452–455. [Google Scholar]
- Zhang, H.; Li, J.; Wen, B.; Xun, Y.; Liu, J. Connecting intelligent things in smart hospitals using NB-IoT. IEEE Internet Things J. 2018, 5, 1550–1560. [Google Scholar] [CrossRef]
- Kumar, C.R.; Vijayalakshmi, B.; Karthik, S.; Hanitha, R.; Hemapreetha, T. Drip rate monitor for infusion fluids. Taga J. 2018, 14, 2312–2316. [Google Scholar]
- Alagundagi, S.S.; Pasala, K.; Arora, M. Opto-electronic system for intravenous infusion monitoring. In Proceedings of the 10th International Conference on Communication Systems & Networks (COMSNETS), Banglore, India, 3–7 January 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 688–692. [Google Scholar]
- Wang, S.; Jiang, B. Design of wireless infusion monitor based on bluetooth 4.0. In Proceedings of the 13th IEEE Conference on Industrial Electronics and Applications (ICIEA), Wuhan, China, 31 May–2 June 2018. [Google Scholar]
- Arduino Documentation. Available online: https://www.arduino.cc/reference/en/language/functions/analog-io/analogread/ (accessed on 21 November 2018).
- Várady, P.; Benyó, Z.; Benyó, B. An Open Architecture Patient Monitoring System Using Standard Technologies. IEEE Trans. Inf. Technol. Biomed. 2002, 6, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Pan, D.; Dhall, R.; Lieberman, A.; Petitti, D.B. A Mobile Cloud-Based Parkinson’s Disease Assessment System for Home-Based Monitoring. JMIR Mhealth Uhealth 2015, 3, e29. [Google Scholar] [CrossRef] [PubMed]
- Axelta Internet Osmosis. Available online: http://aws2.axelta.com/ (accessed on 21 November 2018).






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Sensing Method (Location) | Advantages | Disadvantages |
|---|---|---|---|
| 2001 | Infrared detection (Drip chamber) [10] | Minimalistic approach to design the circuit Circuit consumes low power | Display consumes high power No results provided |
| 2002 | Infrared detection (Drip chamber) [11] | Three IR pairs at different planes Prismatic effect compensation | Unconnected system No alarms generated |
| 2007 | Infrared detection (Drip chamber) [12] | Efficient battery life Uses wireless sensor networks | Non-consistent monitoring Lack of testing |
| 2009 | Infrared detection (Drip chamber) [13] | Multi-parameter measurement | No device or design shown No results provided |
| 2010 | Infrared detection (Drip chamber) [14] | Low energy consumption Multi-layer software structure | Listening periods reduces the accuracy of the device |
| 2011 | Infrared detection (Drip chamber) [15] | Infrared region of operation | Display consumes high power Lack of testing |
| 2011 | Flexible capacitive sensor (Bottom of the bottle) [16] | Over the bottle setup Low cost, Simple structure & Compact | Binary value for the liquid level Use of consumable, i.e., glue spray |
| 2012 | Microwave time-domain reflectometry (Bottle) [17] | Non-invasive sensing Easy, low-cost fabrication, and dimension control | Careful alignment between bottle and holder is must Dependent on the shape of bottle Difficult to reproduce results |
| 2013 | Ray path simulations (Drip chamber) [18] | Optical detection | Simulations |
| 2015 | Infrared detection (Drip chamber) [19] | Lack of testing results provided Comparison with other devices/schemes difficult | |
| 2015 | Infrared detection (Drip chamber) [20] | Centralized receiver module Audio and visual alerts | Incomplete, ineffective and costly device Lack of testing |
| 2016 | Infrared detection (Drip chamber) [21] | PC and Android based monitoring Multi-bag setup | Specific liquid amount can be used Unknown sensor mounting |
| 2016 | Infrared detection (Drip chamber) [22] | Stakeholders interviewed | No device or design shown Unconnected system No results provided |
| 2017 | Capacitive Level detection [23] | Multi-parameter measurement | Lack of testing No device or design shown Unknown sensor mounting |
| 2017 | Load cell (Glucose hanger) [24] | Weight-based measurement | Restricted to one fluid type No device or design shown |
| 2017 | Pressure sensing (Bottle) [25] | Circuit consumes low power | No alarms generated Lack of testing No device or design shown |
| 2018 | Infrared sensor (Drip chamber) [26] | Cloud-connected device Testing done for ambient environment | Assumption about droplet volume |
| 2018 | Infrared sensor (Drip chamber) [27] | Power supply backup | No results No device or design shown Lack of electrical isolation and safety details and reliability |
| 2018 | Infrared sensor (Drip chamber) [28] | Multi-alert system | Display consumes high power Unknown sensor mounting Lack of testing |
| 2018 | Infrared Detection (Drip chamber) [29] | Device tested extensively in different ambient conditions | No actual device shown Restricted to diameter of infusion tube |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sardana, P.; Kalra, M.; Sardana, A. Design, Fabrication, and Testing of an Internet Connected Intravenous Drip Monitoring Device. J. Sens. Actuator Netw. 2019, 8, 2. https://doi.org/10.3390/jsan8010002
Sardana P, Kalra M, Sardana A. Design, Fabrication, and Testing of an Internet Connected Intravenous Drip Monitoring Device. Journal of Sensor and Actuator Networks. 2019; 8(1):2. https://doi.org/10.3390/jsan8010002
Chicago/Turabian StyleSardana, Pranshul, Mohit Kalra, and Amit Sardana. 2019. "Design, Fabrication, and Testing of an Internet Connected Intravenous Drip Monitoring Device" Journal of Sensor and Actuator Networks 8, no. 1: 2. https://doi.org/10.3390/jsan8010002
APA StyleSardana, P., Kalra, M., & Sardana, A. (2019). Design, Fabrication, and Testing of an Internet Connected Intravenous Drip Monitoring Device. Journal of Sensor and Actuator Networks, 8(1), 2. https://doi.org/10.3390/jsan8010002