
The Prevalence and Impact of Evidence-Based Medications on Cardiovascular and Cerebrovascular Outcomes in Patients with Acute Coronary Syndrome Post-Revascularization in Oman
 and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Settings
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Collection
2.5. Evidence-Based Medication (EBM)
Full Versus Partial EBM
2.6. Study Outcomes
2.7. Sample Size
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith, J.N.; Negrelli, J.M.; Manek, M.B.; Hawes, E.M.; Viera, A.J. Diagnosis and Management of Acute Coronary Syndrome: An Evidence-Based Update. J. Am. Board Fam. Med. 2015, 28, 283–293. [Google Scholar] [CrossRef]
- James, S. Epidemiology of acute coronary syndromes. In The ESC Textbook of Cardiovascular Medicine, 3rd ed.; Oxford University Press: Oxford, UK, 2018; pp. 1213–1218. [Google Scholar]
- Vos, T.; Lim, S.; Abbafati, C.; Abbas, K.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Panduranga, P.; Sulaiman, K.; Al-Zakwani, I. Acute coronary syndrome in oman: Results from the gulf registry of acute coronary events. Sultan Qaboos Univ. Med. J. 2011, 11, 338. [Google Scholar] [CrossRef] [PubMed]
- Alnasser, S.M.A.; Huang, W.; Gore, J.M.; Steg, P.H.G.; Eagle, K.A.; Anderson, F.A.; Fox, K.A.A.; Gurfinkel, E.; Brieger, D.; Klein, W.; et al. Late Consequences of Acute Coronary Syndromes: Global Registry of Acute Coronary Events (GRACE) Follow-up. Am. J. Med. 2015, 128, 766–775. [Google Scholar] [CrossRef] [PubMed]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E.; Ganiats, T.G.; Holmes, D.R.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Non–ST-Elevation Acute Coronary Syndromes. J. Am. Coll. Cardiol. 2014, 64, e139–e228. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.; Saxon, L.; Cunningham, W.; Adams, P. Secondary prevention for patients after a myocardial infarction: Summary of updated NICE guidance. BMJ 2013, 347, f6544. [Google Scholar] [CrossRef]
- Fitchett, D.H.; Leiter, L.A.; Lin, P.; Pickering, J.; Welsh, R.; Stone, J.; Gregoire, J.; McFarlane, P.; Langer, A.; Gupta, A.; et al. Update to Evidence-Based Secondary Prevention Strategies After Acute Coronary Syndrome. CJC Open 2020, 2, 402–415. [Google Scholar] [CrossRef]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization. J. Am. Coll. Cardiol. 2022, 79, e21–e129. [Google Scholar] [CrossRef]
- Yang, J.H.; Hahn, J.-Y.; Song, Y.B.; Choi, S.-H.; Choi, J.-H.; Lee, S.H.; Jeong, M.-H.; Choi, D.-J.; Park, J.S.; Park, H.S.; et al. Angiotensin receptor blocker in patients with ST segment elevation myocardial infarction with preserved left ventricular systolic function: Prospective cohort study. BMJ 2014, 349, g6650. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Park, G.-M.; Kim, Y.-H.; Yun, S.-C.; Chang, M.; Roh, J.-H.; Yoon, S.-H.; Ahn, J.-M.; Park, D.-W.; Kang, S.-J.; et al. Effect of Beta Blockers and Renin–Angiotensin System Inhibitors on Survival in Patients with Acute Myocardial Infarction Undergoing Percutaneous Coronary Intervention. Medicine 2016, 95, e2971. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Cui, Q.; Liu, Y.; Liu, Z.; Zhang, Y.; Liu, F.; Wang, J. Effects of a Secondary Prevention Combination Therapy with beta-Blocker and Statin on Major Adverse Cardiovascular Events in Acute Coronary Syndrome Patients. Med. Sci. Monit. 2020, 26, e925114-1. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Zhao, F.; Mehta, S.R.; Chrolavicius, S.; Tognoni, G.; Fox, K.K. Effects of Clopidogrel in Addition to Aspirin in Patients with Acute Coronary Syndromes without ST-Segment Elevation. N. Engl. J. Med. 2001, 345, 494–502. [Google Scholar] [CrossRef]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic Therapy after Acute Coronary Syndrome or PCI in Atrial Fibrillation. N. Engl. J. Med. 2019, 380, 1509–1524. [Google Scholar] [CrossRef]
- Al-Zakwani, I.; Zubaid, M.; Alsheikh-Ali, A.A.; Almahmeed, W.; Rashed, W. Effect of evidence-based cardiac drug therapy on mortality in patients with acute coronary syndrome: Findings from the Gulf COAST registry. Cardiovasc. Ther. 2018, 36, e12463. [Google Scholar] [CrossRef]
- Rubin, D.B. Using propensity scores to help design observational studies: Application to the tobacco litigation. Health Serv. Outcomes Res. Methodol. 2001, 2, 169–188. [Google Scholar] [CrossRef]
- Amann, U.; Kirchberger, I.; Heier, M.; Golüke, H.; von Scheidt, W.; Kuch, B.; Peters, A.; Meisinger, C. Long-term survival in patients with different combinations of evidence-based medications after incident acute myocardial infarction: Results from the MONICA/KORA Myocardial Infarction Registry. Clin. Res. Cardiol. 2014, 103, 655–664. [Google Scholar] [CrossRef]
- Gausia, K.; Katzenellenbogen, J.M.; Sanfilippo, F.M.; Knuiman, M.W.; Thompson, P.L.; Hobbs, M.S.T.; Thompson, S.C. Evidence-based prescribing of drugs for secondary prevention of acute coronary syndrome in Aboriginal and non-Aboriginal patients admitted to Western Australian hospitals. Intern. Med. J. 2014, 44, 353–361. [Google Scholar] [CrossRef]
- Gaedke, M.Â.; da Costa, J.S.D.; Manenti, E.R.F.; Henn, R.L.; Paniz, V.M.V.; Nunes, M.F.; da Motta, M.A.; Olinto, M.T.A. Use of medicines recommended for secondary prevention of acute coronary syndrome. Rev. Saude Publica 2015, 49, 88. [Google Scholar] [CrossRef]
- Bramlage, P.; Messer, C.; Bitterlich, N.; Pohlmann, C.; Cuneo, A.; Stammwitz, E.; Tebbenjohanns, J.; Gohlke, H.; Senges, J.; Tebbe, U. The effect of optimal medical therapy on 1-year mortality after acute myocardial infarction. Heart 2010, 96, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Machado-Alba, J.E. Analysis of secondary prevention measures implemented in patients with a history of acute coronary syndrome. Rev. Colomb. Cardiol. 2019, 26, 63–69. [Google Scholar] [CrossRef]
- Danchin, N.; Cambou, J.-P.; Hanania, G.; Kadri, Z.; Genès, N.; Lablanche, J.-M.; Blanchard, D.; Vaur, L.; Clerson, P.; Guéret, P. Impact of combined secondary prevention therapy after myocardial infarction: Data from a nationwide French registry. Am. Heart J. 2005, 150, 1147–1153. [Google Scholar] [CrossRef]
- Nassr, O.A.; Forsyth, P.; Johnson, C.F. Evaluation of discharge prescriptions for secondary prevention in patients with acute coronary syndromes in Iraq. Pharm. Pract. 2019, 17, 1372. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar] [CrossRef]
- Mehta, S.R.; Yusuf, S.; Peters, R.J.; Bertrand, M.E.; Lewis, B.S.; Natarajan, M.K.; Malmberg, K.; Rupprecht, H.-J.; Zhao, F.; Chrolavicius, S.; et al. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: The PCI-CURE study. Lancet 2001, 358, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.J.; Byeon, H.J.; Yang, Y.-M. Optimal medical therapy for secondary prevention after an acute coronary syndrome: 18-month follow-up results at a tertiary teaching hospital in South Korea. Ther. Clin. Risk. Manag. 2016, 12, 167–175. [Google Scholar] [CrossRef]
- Wilkins, B.; Hullikunte, S.; Simmonds, M.; Sasse, A.; Larsen, P.; Harding, S.A. Improving the Prescribing Gap for Guideline Recommended Medications Post Myocardial Infarction. Heart Lung Circ. 2019, 28, 257–262. [Google Scholar] [CrossRef]
- Ma, T.-T.; Wong, I.C.K.; Man, K.K.C.; Chen, Y.; Crake, T.; Ozkor, M.A.; Ding, L.-Q.; Wang, Z.-X.; Zhang, L.; Wei, L. Effect of evidence-based therapy for secondary prevention of cardiovascular disease: Systematic review and meta-analysis. PLoS ONE 2019, 14, e0210988. [Google Scholar] [CrossRef]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic, n (%) Unless Specified Otherwise | All (n = 268) | EBM | p-Value | |
|---|---|---|---|---|
| Partial (n = 80) | Full (n = 188) | |||
| Demographic | ||||
| Age, mean ± SD, years | 59 ± 12 | 62 ± 14 | 58 ± 12 | 0.03 |
| Female gender | 64 (24%) | 20 (25%) | 44 (23%) | 0.779 |
| Smoker | 73 (27%) | 19 (24%) | 54 (29%) | 0.403 |
| Medical history | ||||
| Atrial fibrillation | 16 (6%) | 7 (9%) | 9 (5%) | 0.21 |
| Heart failure | 33 (12%) | 16 (20%) | 17 (9%) | 0.01 |
| Stroke | 13 (5%) | 6 (8%) | 7 (4%) | 0.18 |
| Transient ischemic attack | 7 (3%) | 4 (5%) | 3 (2%) | 0.11 |
| Chronic kidney disease | 53 (20%) | 33 (41%) | 20 (11%) | <0.001 |
| Diabetes mellitus | 157 (59%) | 47 (59%) | 110 (59%) | 0.97 |
| Hypertension | 181 (68%) | 46 (58%) | 135 (72%) | 0.02 |
| Dyslipidemia | 148 (55%) | 42 (53%) | 106 (56%) | 0.55 |
| Clinical parameters at presentation | ||||
| Heart rate, mean ± SD, beats/min | 72 ± 12 | 69 ± 12 | 74 ± 12 | <0.001 |
| Systolic BP, mean ± SD, mmHg | 125 ± 19 | 125 ± 23 | 125 ± 18 | 0.81 |
| Diastolic BP, mean ± SD, mmHg | 69 ± 14 | 65 ± 13 | 71 ± 14 | <0.001 |
| LVEF, mean ± SD, % | 52 ± 11 | 53 ± 12 | 51 ± 11 | 0.23 |
| Laboratory parameters at the presentation | ||||
| HbA1c, mean ± SD, % | 7.0 ± 2.0 | 8.0 ± 2.0 | 7.0 ± 2.0 | 0.13 |
| Potassium, mean ± SD, mmol/L | 4.0 ± 0.4 | 4.0 ± 0.5 | 4.0 ± 0.4 | 0.91 |
| Creatinine, mean ± SD, μmol/L | 101 ± 7 | 144 ± 12 | 82 ± 25 | <0.001 |
| eGFR, mean ± SD, mL/min/1.73 m2 | 72 ± 22 | 60 ± 28 | 77 ± 15 | <0.001 |
| Discharge diagnosis | ||||
| NSTEMI | 129 (48%) | 44 (55%) | 85 (45%) | 0.14 |
| STEMI | 112 (42%) | 27 (34%) | 85 (45%) | 0.08 |
| Unstable angina | 27 (10%) | 8 (10%) | 19 (10%) | 0.88 |
| LOS during admission, median (IQR) days | 2 (2–4) | 3 (2–5) | 2 (2–3) | <0.001 |
| Characteristic, (%) | All (n = 268) | Full EBM | p-Value | |
|---|---|---|---|---|
| No (n = 80) | Yes (n = 188) | |||
| Discharged medications | ||||
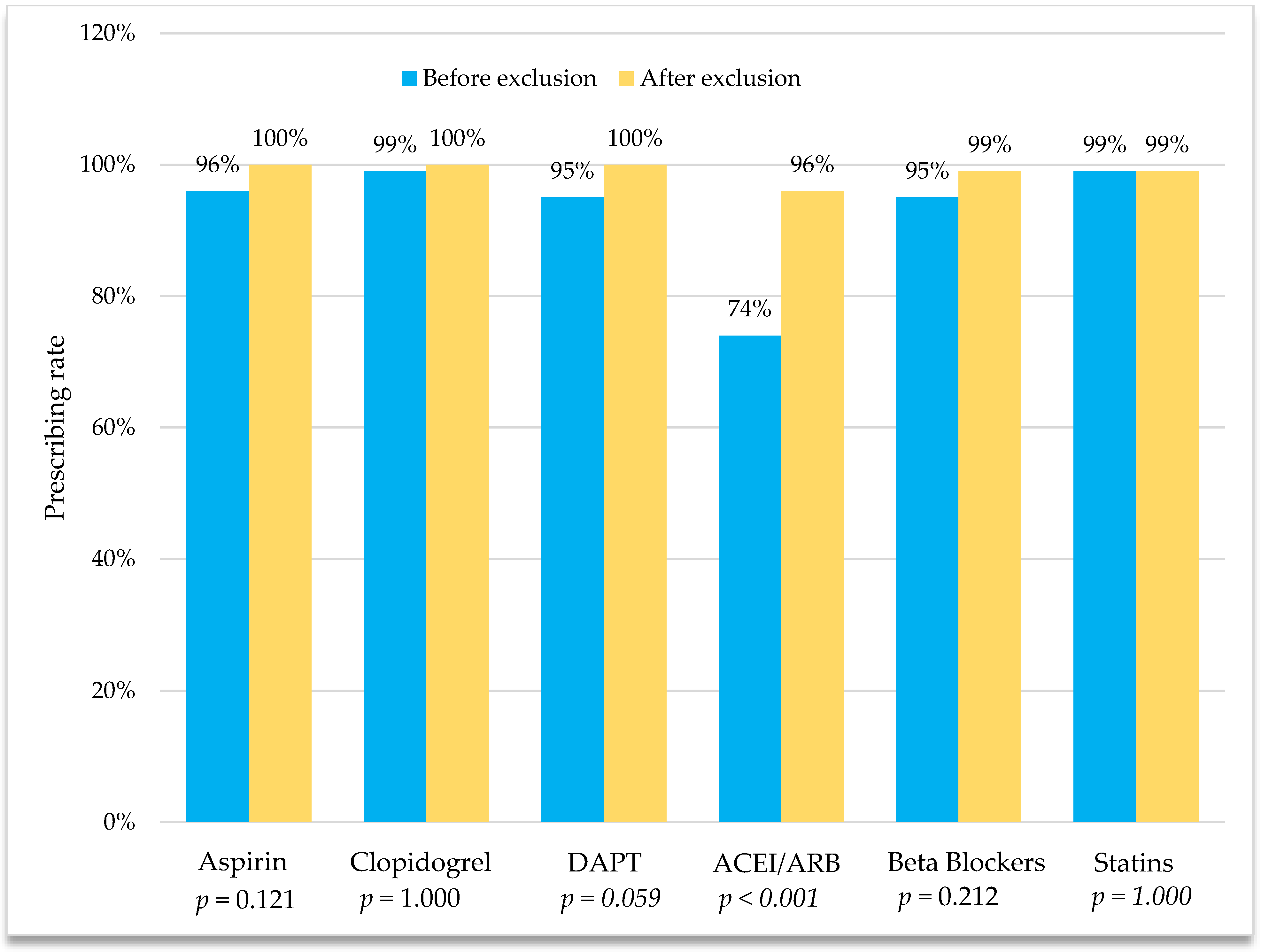
| DAPT | 254 (95%) | 79 (95%) | 178 (95%) | 1 |
| Aspirin | 256 (96%) | 77 (96%) | 179 (95%) | 1 |
| Clopidogrel | 266 (99%) | 79 (99%) | 187 (99%) | 0.509 |
| Oral anticoagulant | 19 (7%) | 5 (6%) | 14 (7%) | 1 |
| Warfarin | 11 (4%) | 4 (5%) | 7 (4%) | 0.738 |
| DOAC | 8 (3%) | 1 (1%) | 7 (4%) | 0.442 |
| ACEI/ARB | 199 (74%) | 11 (14%) | 188 (100%) | <0.001 |
| ACEI (Lisinopril) | 162 (60%) | 9 (11%) | 153 (81%) | <0.001 |
| ARB | 37 (14%) | 2 (3%) | 35 (19%) | <0.001 |
| Irbesartan | 25 (9%) | 1 (1%) | 24 (13%) | 0.002 |
| Valsartan | 12 (5%) | 1 (1%) | 11 (6%) | 0.116 |
| Beta-blocker a | 257 (95%) | 70 (88%) | 187 (99%) | <0.001 |
| Bisoprolol | 217 (81%) | 60 (75%) | 157 (84%) | 0.104 |
| Carvedilol | 39 (15%) | 10 (13%) | 29 (15%) | 0.534 |
| Statin | 266 (99%) | 78 (98%) | 188 (100%) | 0.088 |
| Atorvastatin | 242 (90%) | 73 (91%) | 169 (90%) | 0.731 |
| Rosuvastatin | 24 (9%) | 5 (6%) | 19 (10%) | 0.36 |
| Hydr + isdn | 48 (18%) | 31 (39%) | 17 (9%) | <0.001 |
| CCB (Amlodipine) | 61 (23%) | 18 (23%) | 43 (23%) | 0.947 |
| Spironolactone | 19 (7%) | 6 (8%) | 13 (7%) | 0.864 |
| Medication, n (%) | Not on Medication n = 82 | Reasons behind Non-Prescribing | n (%) |
|---|---|---|---|
| Clopidogrel | 1 (<1%) |
| 1 (100%) |
| Beta-blockers | 10 (4%) |
| 6 (60%) |
| 2 (20%) | ||
| 1 (10%) | ||
| 1 (10%) | ||
| RAS blockers | 69 (26%) |
| 29 (42%) |
| 26 (38%) | ||
| 6 (9%) | ||
| 7 (10%) | ||
| 1 (1%) | ||
| Statins | 2 (1%) |
| 1 (50%) |
| 1 (50%) |
| Characteristic | Original Cohort | PS Matched Cohort | ||||
|---|---|---|---|---|---|---|
| 5 Meds | ≤4 Meds | SMD | 5 Meds | ≤4 Meds | SMD | |
| (n = 188) | (n = 80) | (n = 80) | (n = 80) | |||
| Age, mean, years | 58.41 | 61.84 | −0.27 * | 59.96 | 61.84 | −0.15 |
| Heart failure, % | 9% | 20% | −0.31 * | 11% | 20% | −0.25 |
| Chronic kidney disease, % | 11% | 41% | −0.74 * | 20% | 41% | −0.51 * |
| Hypertension, % | 72% | 58% | 0.31 * | 49% | 58% | −0.18 |
| Heart rate, mean, bpm | 73.88 | 69.18 | 0.39 * | 71.97 | 69.18 | 0.23 |
| Diastolic BP, mean, mmHg | 70.74 | 64.91 | 0.43 * | 67.06 | 64.91 | 0.16 * |
| eGFR, mean, ml/min/1.73 m2 | 76.80 | 59.59 | 0.76 * | 72.61 | 59.59 | 0.57 * |
| Creatinine, mean, μmol/L | 82.07 | 143.66 | −0.68 * | 88.89 | 43.66 | −0.60 * |
| Length of stay, mean, days | 2.91 | 5.40 | −0.45 * | 3.18 | 5.40 | −0.40 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Hadithy, D.A.; Al-Maqbali, J.S.; Al-Riyami, A.; Al Za’abi, M.; Al-Zakwani, I. The Prevalence and Impact of Evidence-Based Medications on Cardiovascular and Cerebrovascular Outcomes in Patients with Acute Coronary Syndrome Post-Revascularization in Oman. Pharmacy 2023, 11, 79. https://doi.org/10.3390/pharmacy11030079
Al-Hadithy DA, Al-Maqbali JS, Al-Riyami A, Al Za’abi M, Al-Zakwani I. The Prevalence and Impact of Evidence-Based Medications on Cardiovascular and Cerebrovascular Outcomes in Patients with Acute Coronary Syndrome Post-Revascularization in Oman. Pharmacy. 2023; 11(3):79. https://doi.org/10.3390/pharmacy11030079
Chicago/Turabian StyleAl-Hadithy, Dalia Ahmed, Juhaina Salim Al-Maqbali, Adil Al-Riyami, Mohammed Al Za’abi, and Ibrahim Al-Zakwani. 2023. "The Prevalence and Impact of Evidence-Based Medications on Cardiovascular and Cerebrovascular Outcomes in Patients with Acute Coronary Syndrome Post-Revascularization in Oman" Pharmacy 11, no. 3: 79. https://doi.org/10.3390/pharmacy11030079
APA StyleAl-Hadithy, D. A., Al-Maqbali, J. S., Al-Riyami, A., Al Za’abi, M., & Al-Zakwani, I. (2023). The Prevalence and Impact of Evidence-Based Medications on Cardiovascular and Cerebrovascular Outcomes in Patients with Acute Coronary Syndrome Post-Revascularization in Oman. Pharmacy, 11(3), 79. https://doi.org/10.3390/pharmacy11030079