Benzodiazepines Withdrawal: Initial Outcomes and Long-Term Impact on Falls in a French Nursing Home


Abstract
:1. Introduction
2. Materials and Methods
2.1. General Description of the Study and Informed Consent
2.2. BZD Withdrawal
2.3. Evaluation of the Number of Falls
3. Results
3.1. BZD Deprescription
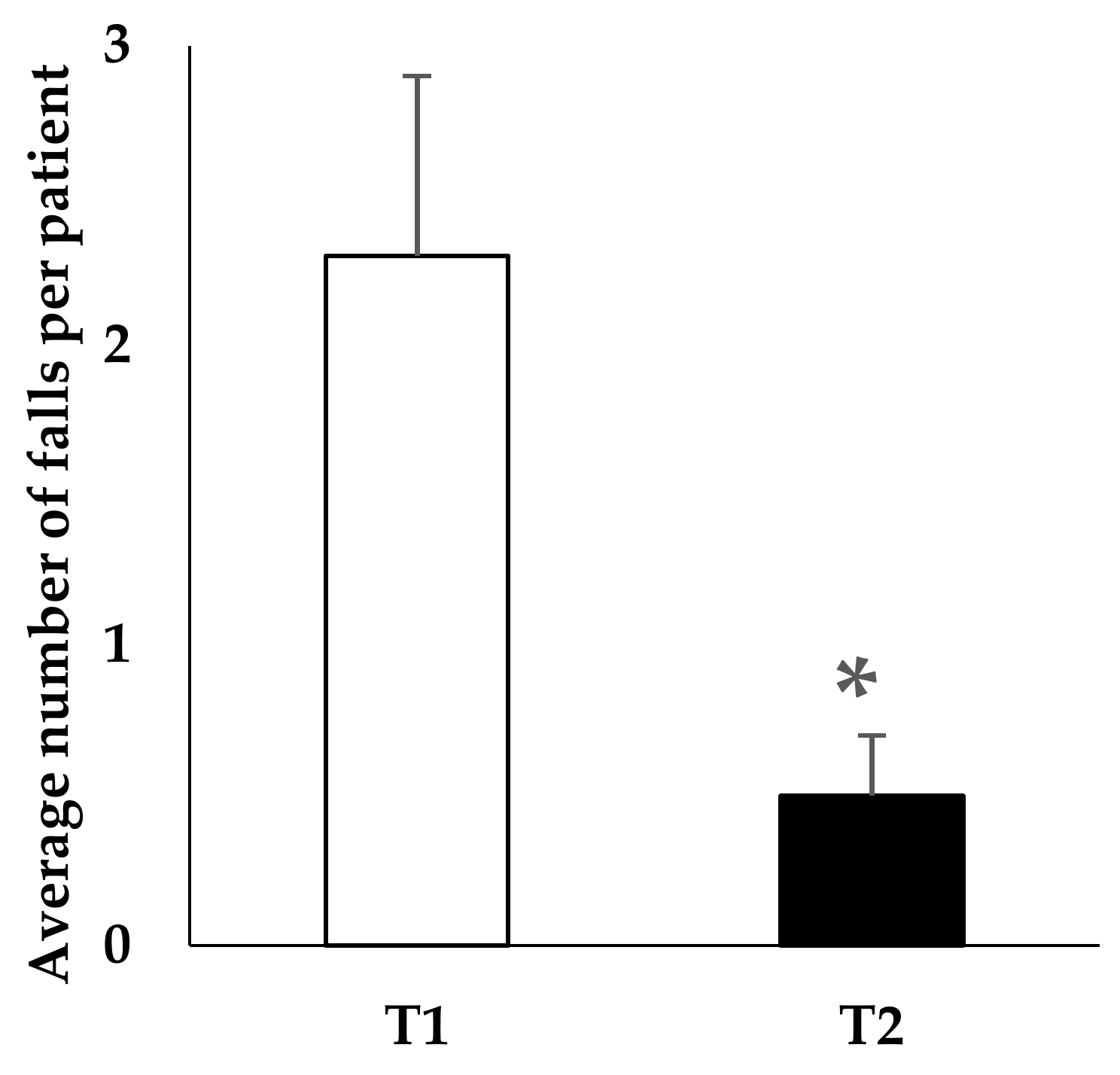
3.2. Evaluation of Number of Falls
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Pelissolo, A.; Bisserbe, J.C. [Dependence on benzodiazepines. Clinical and biological aspects]. L’Encephale 1994, 20, 147–157. [Google Scholar] [PubMed]
- Bateson, A.N. Basic Pharmacologic Mechanisms Involved in Benzodiazepine Tolerance and Withdrawal. Curr. Pharm. Des. 2002, 8, 5–21. [Google Scholar] [CrossRef] [PubMed]
- Haute Autorité de Santé-Modalités d’arrêt des Benzodiazépines et Médicaments Apparentés chez le Patient Agé. Available online: https://www.has-sante.fr/portail/jcms/c_601509/fr/modalites-d-arret-des-benzodiazepines-et-medicaments-apparentes-chez-le-patient-age (accessed on 19 February 2018).
- Koski, K.; Luukinen, H.; Laippala, P.; Kivelä, S.L. Risk factors for major injurious falls among the home-dwelling elderly by functional abilities. A prospective population-based study. Gerontology 1998, 44, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Onder, G.; Cesari, M.; Barillaro, C.; Russo, A.; Bernabei, R. Silver Network Home Care Study Group Psychotropic medications and risk for falls among community-dwelling frail older people: An observational study. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Pariente, A.; Dartigues, J.-F.; Benichou, J.; Letenneur, L.; Moore, N.; Fourrier-Réglat, A. Benzodiazepines and injurious falls in community dwelling elders. Drugs Aging 2008, 25, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Berdot, S.; Bertrand, M.; Dartigues, J.-F.; Fourrier, A.; Tavernier, B.; Ritchie, K.; Alpérovitch, A. Inappropriate medication use and risk of falls—A prospective study in a large community-dwelling elderly cohort. BMC Geriatr. 2009, 9, 30. [Google Scholar] [CrossRef] [PubMed]
- Barker, M.J.; Greenwood, K.M.; Jackson, M.; Crowe, S.F. Persistence of cognitive effects after withdrawal from long-term benzodiazepine use: A meta-analysis. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 2004, 19, 437–454. [Google Scholar] [CrossRef]
- Billioti de Gage, S.; Bégaud, B.; Bazin, F.; Verdoux, H.; Dartigues, J.-F.; Pérès, K.; Kurth, T.; Pariente, A. Benzodiazepine use and risk of dementia: Prospective population based study. BMJ 2012, 345, e6231. [Google Scholar] [CrossRef] [PubMed]
- Bénard-Laribière, A.; Noize, P.; Pambrun, E.; Bazin, F.; Verdoux, H.; Tournier, M.; Bégaud, B.; Pariente, A. Comorbidities and concurrent medications increasing the risk of adverse drug reactions: Prevalence in French benzodiazepine users. Eur. J. Clin. Pharmacol. 2016, 72, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Yu, N.W.; Chen, P.J.; Tsai, H.J.; Huang, C.W.; Chiu, Y.W.; Tsay, W.I.; Hsu, J.; Chang, C.M. Association of benzodiazepine and Z-drug use with the risk of hospitalisation for fall-related injuries among older people: A nationwide nested case-control study in Taiwan. BMC Geriatr. 2017, 17, 140. [Google Scholar] [CrossRef] [PubMed]
- Briot, M. Assemblée Nationale, Office Parlementaire d’Evaluation des Politiques de Santé (OPEPS). Rapport sur le Bon Usage des Médicaments Psychotropes. Assemblée Nationale: Paris, France, 2006. Available online: http://www.assemblee-nationale.fr/12/rap-off/i3187.asp (accessed on 19 February 2018).
- Mebarki, S.; Trivalle, C. Échelles d’évaluation de l’effet anticholinergique des médicaments. NPG Neurol. Psychiatr. Gériatr. 2012, 12, 131–138. [Google Scholar] [CrossRef]
- Rickels, K.; DeMartinis, N.; García-España, F.; Greenblatt, D.J.; Mandos, L.A.; Rynn, M. Imipramine and buspirone in treatment of patients with generalized anxiety disorder who are discontinuing long-term benzodiazepine therapy. Am. J. Psychiatry 2000, 157, 1973–1979. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. 2012. Available online: http://www.who.int/mediacentre/factsheets/fs344/en/ (accessed on 3 April 2018).
- AFSSAPS. Report de mise en Application de la Restriction de Prescription Initiale Annuelle aux Neurologues et aux Pédiatres des formes orales de Rivotril® (clonazépam). Lettre aux Professionnels de Santé (Report du 2 Janvier 2012 au 15 Mars 2012). Décembre 2011. Available online: http://ansm.sante.fr/Activites/Surveillance-des-stupefiants-et-des-psychotropes/Medicaments-a-risque-d-usage-detourne-ou-de-dependance/Medicaments-a-risque-d-usage-detourne-ou-de-dependance/RIVOTRIL (accessed on 19 February 2018).
- De Gage, S.B.; Moride, Y.; Ducruet, T.; Kurth, T.; Verdoux, H.; Tournier, M.; Pariente, A.; Bégaud, B. Benzodiazepine use and risk of Alzheimer’s disease: Case-control study. BMJ 2014, 349, g5205. [Google Scholar] [CrossRef] [PubMed]
- Vicens, C.; Socias, I.; Mateu, C.; Leiva, A.; Bejarano, F.; Sempere, E.; Basora, J.; Palop, V.; Mengual, M.; Beltran, J.L.; et al. Comparative efficacy of two primary care interventions to assist withdrawal from long term benzodiazepine use: A protocol for a clustered, randomized clinical trial. BMC Fam. Pract. 2011, 12, 23. [Google Scholar] [CrossRef] [PubMed]
- Voshaar, R.C.O.; Couvée, J.E.; van Balkom, A.J.L.M.; Mulder, P.G.H.; Zitman, F.G. Strategies for discontinuing long-term benzodiazepine use: Meta-analysis. Br. J. Psychiatry J. Ment. Sci. 2006, 189, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Parr, J.M.; Kavanagh, D.J.; Cahill, L.; Mitchell, G.; McD Young, R. Effectiveness of current treatment approaches for benzodiazepine discontinuation: A meta-analysis. Addict. Abingdon Engl. 2009, 104, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Pierfitte, C.; Macouillard, G.; Thicoïpe, M.; Chaslerie, A.; Pehourcq, F.; Aïssou, M.; Martinez, B.; Lagnaoui, R.; Fourrier, A.; Bégaud, B.; et al. Benzodiazepines and hip fractures in elderly people: Case-control study. BMJ 2001, 322, 704–708. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, E.S.F.; Fletcher, A.; Bloch, K.V.; Rodrigues, L.C. Risk factors for falls with severe fracture in elderly people living in a middle-income country: A case control study. BMC Geriatr. 2008, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Finkle, W.D.; Der, J.S.; Greenland, S.; Adams, J.L.; Ridgeway, G.; Blaschke, T.; Wang, Z.; Dell, R.M.; VanRiper, K.B. Risk of fractures requiring hospitalization after an initial prescription for zolpidem, alprazolam, lorazepam, or diazepam in older adults. J. Am. Geriatr. Soc. 2011, 59, 1883–1890. [Google Scholar] [CrossRef] [PubMed]
- Xing, D.; Ma, X.L.; Ma, J.X.; Wang, J.; Yang, Y.; Chen, Y. Association between use of benzodiazepines and risk of fractures: A meta-analysis. Osteoporos. Int. 2014, 25, 105–120. [Google Scholar] [CrossRef] [PubMed]
- Verger, P. La Politique du Médicament en EHPAD; Ministère des Solidarités et de la Santé: Paris, France, 2013. [Google Scholar]
- Shash, D.; Kurth, T.; Bertrand, M.; Dufouil, C.; Barberger-Gateau, P.; Berr, C.; Ritchie, K.; Dartigues, J.F.; Bégaud, B.; Alpérovitch, A.; et al. Benzodiazepine, psychotropic medication, and dementia: A population-based cohort study. Alzheimers Dement. 2016, 12, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Billioti de Gage, S.; Pariente, A.; Bégaud, B. Is there really a link between benzodiazepine use and the risk of dementia? Expert Opin. Drug Saf. 2015, 14, 733–747. [Google Scholar] [CrossRef] [PubMed]
- Gray, S.L.; Dublin, S.; Yu, O.; Walker, R.; Anderson, M.; Hubbard, R.A.; Crane, P.K.; Larson, E.B. Benzodiazepine use and risk of incident dementia or cognitive decline: Prospective population based study. BMJ. 2016, 352, i90. [Google Scholar] [CrossRef] [PubMed]
- Zhong, G.; Wang, Y.; Zhang, Y.; Zhao, Y. Association between Benzodiazepine Use and Dementia: A Meta-Analysis. PLoS ONE 2015, 10, e0127836. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Starting the Withdrawal Program | Patient’s Follow-Up under BZD at Four Months | Patient’s Follow-Up under BZD at One Year |
|---|---|---|
| Number of patients under BZD n = 31 patients (28.7% of the patients in nursing home) | Total number of patients n = 31 | Total number of patients n = 29 |
| 15 patients: maintenance | 8 patients: maintenance 1: diminution 2: stop 4: deceased | |
| 7 patients: diminution | 1 patient: diminution 6: stop | |
| 7 patients: stop | 3 patients: stop (maintenance) 4: deceased | |
| 1 sight loss (transferred) | ||
| 1 deceased |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Javelot, H.; Marquis, A.; Antoine-Bernard, E.; Grandidier, J.; Weiner, L.; Javelot, T.; Michel, B. Benzodiazepines Withdrawal: Initial Outcomes and Long-Term Impact on Falls in a French Nursing Home. Pharmacy 2018, 6, 30. https://doi.org/10.3390/pharmacy6020030
Javelot H, Marquis A, Antoine-Bernard E, Grandidier J, Weiner L, Javelot T, Michel B. Benzodiazepines Withdrawal: Initial Outcomes and Long-Term Impact on Falls in a French Nursing Home. Pharmacy. 2018; 6(2):30. https://doi.org/10.3390/pharmacy6020030
Chicago/Turabian StyleJavelot, Hervé, Anne Marquis, Emilie Antoine-Bernard, Jean Grandidier, Luisa Weiner, Thierry Javelot, and Bruno Michel. 2018. "Benzodiazepines Withdrawal: Initial Outcomes and Long-Term Impact on Falls in a French Nursing Home" Pharmacy 6, no. 2: 30. https://doi.org/10.3390/pharmacy6020030
APA StyleJavelot, H., Marquis, A., Antoine-Bernard, E., Grandidier, J., Weiner, L., Javelot, T., & Michel, B. (2018). Benzodiazepines Withdrawal: Initial Outcomes and Long-Term Impact on Falls in a French Nursing Home. Pharmacy, 6(2), 30. https://doi.org/10.3390/pharmacy6020030