


Real-World Outcomes of Systemic Therapy in Japanese Patients with Cancer (Tokushukai REAl-World Data Project: TREAD): Study Protocol for a Nationwide Cohort Study
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
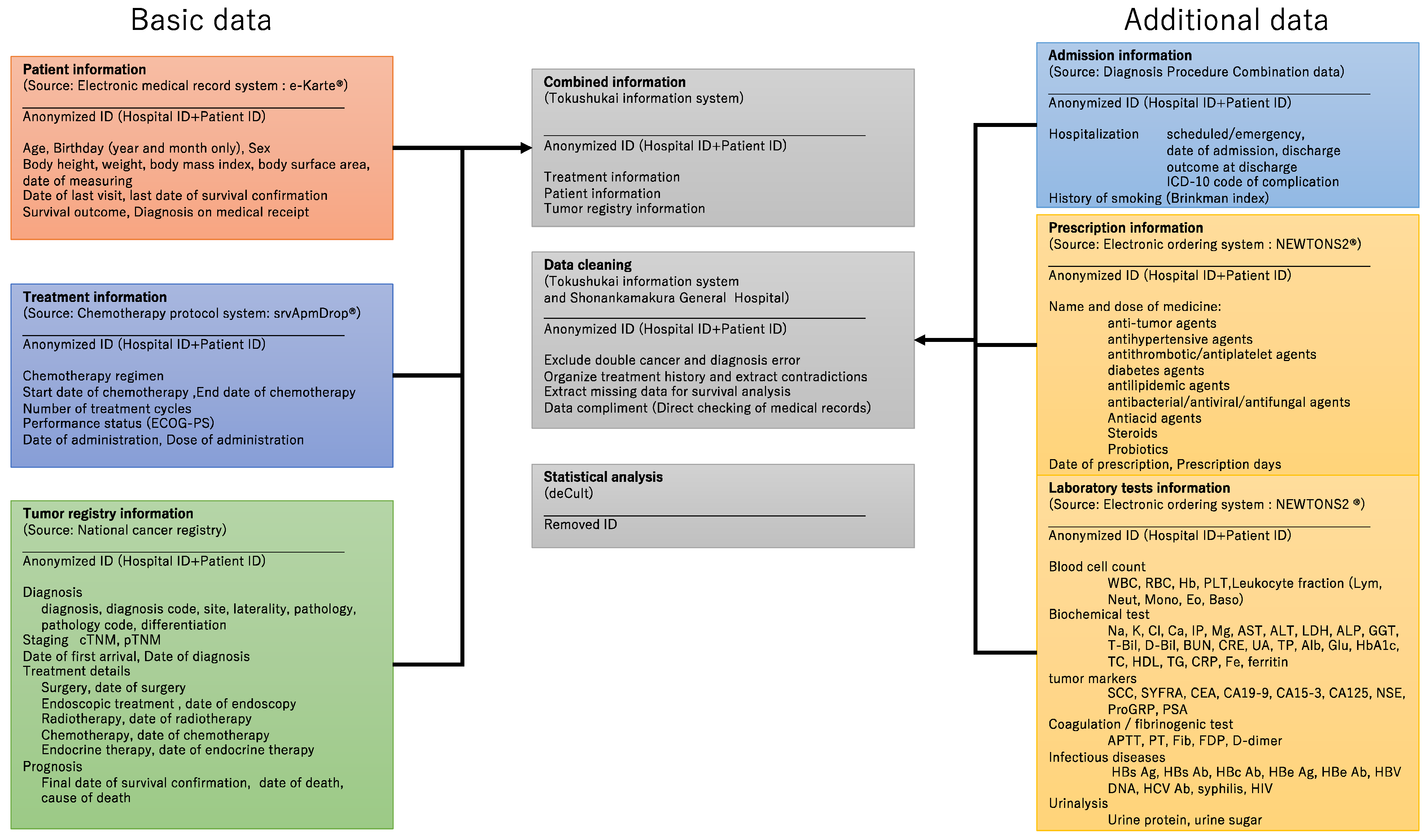
2.2. Information Source and Data Collection
2.3. Study Endpoints
2.4. Sample Size Calculation
2.5. Statistical Analysis
2.6. Patient and Public Involvement Statement
3. Discussion
Strengths and Weaknesses
4. Ethics and Dissemination
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Streptomycin in Tuberculosis Trials Committee. Streptomycin treatment of pulmonary tuberculosis. Br. Med. J. 1948, 2, 769–782. [Google Scholar] [CrossRef] [Green Version]
- Bothwell, L.E.; Podolsky, S.H. The emergence of the randomized, controlled trial. N. Engl. J. Med. 2016, 375, 501–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milsted, R. Cancer drug approval in the United States, Europe, and Japan. Adv. Cancer Res. 2006, 96, 371–391. [Google Scholar] [CrossRef]
- Townsley, C.A.; Selby, R.; Siu, L.L. Systematic review of barriers to the recruitment of older patients with cancer onto clinical trials. J. Clin. Oncol. 2005, 23, 3112–3124. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Rizzo, S.; Whipple, S.; Pal, N.; Pineda, A.L.; Lu, M.; Arnieri, B.; Lu, Y.; Capra, W.; Copping, R.; et al. Evaluating eligibility criteria of oncology trials using real-world data and AI. Nature 2021, 592, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Averitt, A.J.; Weng, C.; Ryan, P.; Perotte, A. Translating evidence into practice: Eligibility criteria fail to eliminate clinically significant differences between real-world and study populations. NPJ Digit. Med. 2020, 3, 67. [Google Scholar] [CrossRef] [PubMed]
- Okuyama, A.; Higashi, T. Patterns of cancer treatment in different age groups in Japan: An analysis of hospital-based cancer registry data, 2012–2015. Jpn. J. Clin. Oncol. 2018, 48, 417–425. [Google Scholar] [CrossRef]
- Hilgers, R.; König, F.; Molenberghs, G. Design and analysis of clinical trials for small rare disease populations. J. Rare Dis. Res. Treat. 2016, 1, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Latimer, N.R. Survival analysis for economic evaluations alongside clinical trials—Extrapolation with patient-level data: Inconsistencies, limitations, and a practical guide. Med. Decis. Mak. 2013, 33, 743–754. [Google Scholar] [CrossRef] [Green Version]
- Corrigan-Curay, J.; Sacks, L.; Woodcock, J. Real-world evidence and real-world data for evaluating drug safety and effectiveness. J. Am. Med. Assoc. 2018, 320, 867–868. [Google Scholar] [CrossRef]
- Katkade, V.B.; Sanders, K.N.; Zou, K.H. Real world data: An opportunity to supplement existing evidence for the use of long-established medicines in health care decision making. J. Multidiscip. Healthc. 2018, 11, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; McMurray, J.; Holman, R.R. Real-world studies no substitute for RCTs in establishing efficacy. Lancet 2019, 393, 210–211. [Google Scholar] [CrossRef]
- Wang, S.V.; Schneeweiss, S.; Gagne, J.J.; Evers, T.; Gerlinger, C.; Desai, R.; Najafzadeh, M. Using real-world data to extrapolate evidence from randomized controlled trials. Clin. Pharmacol. Ther. 2019, 105, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- Makady, A.; de Boer, A.; Hillege, H.; Klungel, O.; Goettsch, W. What is real-world data? A review of definitions based on literature and stakeholder interviews. Value Health 2017, 20, 858–865. [Google Scholar] [CrossRef] [Green Version]
- Jansana, A.; Del Cura, I.; Prados-Torres, A.; Cuesta, T.S.; Poblador-Plou, B.; Miguel, A.G.; Lanzuela, M.; Ibañez, B.; Tamayo, I.; Moreno-Iribas, C.; et al. Use of real-world data to study health services utilisation and comorbidities in long-term breast cancer survivors (the SURBCAN study): Study protocol for a longitudinal population-based cohort study. BMJ Open 2020, 10, e040253. [Google Scholar] [CrossRef]
- Kang, J.; Cairns, J. Protocol for data extraction: How real-world data have been used in the National Institute for Health and Care Excellence appraisals of cancer therapy. BMJ Open 2022, 12, e055985. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Medical Facility Survey of Japan 2020, Ministry of Health, Labour and Welfare Web Site. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/iryosd/m20/dl/is2003_01.pdf (accessed on 30 April 2022). (In Japanese).
- Hayashida, K.; Murakami, G.; Matsuda, S.; Fushimi, K. History and profile of diagnosis procedure combination (DPC): Development of a real data collection system for acute inpatient care in Japan. J. Epidemiol. 2021, 31, JE20200288. [Google Scholar] [CrossRef]
- National Cancer Center, Japan. The Standardised Roles for Hospital Based Cancer Registries. Available online: https://ganjoho.jp/med_pro/cancer_control/can_reg/hospital/regulation.html17 (accessed on 30 April 2022). (In Japanese).
- Okuyama, A.; Watabe, M.; Makoshi, R.; Takahashi, H.; Tsukada, Y.; Higashi, T. Impact of the COVID-19 pandemic on the diagnosis of cancer in Japan: Analysis of hospital-based cancer registries. Jpn. J. Clin. Oncol. 2022, 52, 1215–1224. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours Stage, 8th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2016. [Google Scholar]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Japan Clinical Oncology Group. Common Terminology Criteria for Adverse Events v. 5.0 Japanese Translation JCOG Version (CTCAE v. 5.0-JCOG). 2017. Available online: http://www.jcog.jp/doctor/tool/CTCAEv5.0J_20180915_miekeshi_v21_1.pdf (accessed on 30 April 2022).
- Kuk, A.Y.C.; Chen, C.-H. A mixture model combining logistic regression with proportional hazards regression. Biometrika 1992, 79, 531–541. [Google Scholar] [CrossRef]
- Miltenberger, R.; Götte, H.; Schüler, A.; Jahn-Eimermacher, A. Progression-free survival in oncological clinical studies: Assessment time bias and methods for its correction. Pharm. Stat. 2021, 20, 864–878. [Google Scholar] [CrossRef] [PubMed]
- Aleksakhina, S.N.; Imyanitov, E.N. Cancer therapy guided by mutation tests: Current status and perspectives. Int. J. Mol. Sci. 2021, 22, 10931. [Google Scholar] [CrossRef] [PubMed]
- Lewandowska, A.; Rudzki, G.; Lewandowski, T.; Prochnicki, M.; Rudzki, S.; Laskowska, B.; Brudniak, J. Quality of life of cancer patients treated with chemotherapy. Int. J. Environ. Res. Public Health 2020, 17, 6938. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria |
|---|
|
| Exclusion criteria |
|
| Blood cell counts | White blood cell (WBC), red blood cell (RBC), hemoglobin (Hb), platelet (PLT), leukocyte fraction, lymphocyte (Lym), neutrophil (Neu), monocyte (Mono), eosinophil (Eo), and basophil (Baso) |
| Biochemical tests | Sodium (Na), potassium (K), chloride (Cl), calcium (Ca), inorganic phosphorus (IP), magnesium (Mg), aspartate aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), alkaline phosphatase (ALP), γ-glutamyl transpeptidase (GGT), total bilirubin (T-Bil), direct bilirubin (D-Bil), blood urea nitrogen (BUN), creatinine (CRE), uric acid (UA), total protein (TP), albumin (Alb), blood glucose (Glu), hemoglobin A1c (HbA1c), total cholesterol (TC), HDL cholesterol, triglyceride (TG), C-reactive protein (CRP), iron (Fe), and ferritin |
| Tumor markers | Squamous cell carcinoma-related antigen (SCC), cytokeratin 19 fragment (SYFRA), carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), carbohydrate antigen 15-3 (CA15-3), carbohydrate antigen 125 (CA125), neuron-specific enolase (NSE), pro-gastrin-releasing peptide (ProGRP), and prostate specific antigen (PSA) |
| Coagulation/fibrinogenic tests | Activated partial thromboplastin time (APTT), prothrombin time (PT), fibrinogen (Fib), fibrin/fibrinogen degradation product (FDP), and D-dimer |
| Infectious disease markers | Hepatitis B surface (HBs) antigen, HBs antibody, HB core antibody, HBe antigen, HBe antibody, HB virus DNA quantification, HC virus antibody, syphilis, and HIV |
| Urinalysis parameters | Urine protein qualitative, urine sugar qualitative |
| Biliary tract cancer | 800 |
| Breast cancer | 10,000 |
| Colorectal cancer | 10,000 |
| Esophageal cancer | 1000 |
| Gastric cancer | 5000 |
| Gastrointestinal stromal tumor | 500 |
| Kidney cancer | 350 |
| Liver cancer | 500 |
| Lung cancer | 10,000 |
| Ovarian cancer | 1500 |
| Prostate cancer | 5000 |
| Pancreatic cancer | 2500 |
| Uterine body cancer | 350 |
| Uterine cervix cancer | 350 |
| Urothelial cancer | 1000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimoyama, R.; Imamura, Y.; Uryu, K.; Mase, T.; Fujimura, Y.; Hayashi, M.; Ohtaki, M.; Ohtani, K.; Shinozaki, N.; Minami, H. Real-World Outcomes of Systemic Therapy in Japanese Patients with Cancer (Tokushukai REAl-World Data Project: TREAD): Study Protocol for a Nationwide Cohort Study. Healthcare 2022, 10, 2146. https://doi.org/10.3390/healthcare10112146
Shimoyama R, Imamura Y, Uryu K, Mase T, Fujimura Y, Hayashi M, Ohtaki M, Ohtani K, Shinozaki N, Minami H. Real-World Outcomes of Systemic Therapy in Japanese Patients with Cancer (Tokushukai REAl-World Data Project: TREAD): Study Protocol for a Nationwide Cohort Study. Healthcare. 2022; 10(11):2146. https://doi.org/10.3390/healthcare10112146
Chicago/Turabian StyleShimoyama, Rai, Yoshinori Imamura, Kiyoaki Uryu, Takahiro Mase, Yoshiaki Fujimura, Maki Hayashi, Megu Ohtaki, Keiko Ohtani, Nobuaki Shinozaki, and Hironobu Minami. 2022. "Real-World Outcomes of Systemic Therapy in Japanese Patients with Cancer (Tokushukai REAl-World Data Project: TREAD): Study Protocol for a Nationwide Cohort Study" Healthcare 10, no. 11: 2146. https://doi.org/10.3390/healthcare10112146
APA StyleShimoyama, R., Imamura, Y., Uryu, K., Mase, T., Fujimura, Y., Hayashi, M., Ohtaki, M., Ohtani, K., Shinozaki, N., & Minami, H. (2022). Real-World Outcomes of Systemic Therapy in Japanese Patients with Cancer (Tokushukai REAl-World Data Project: TREAD): Study Protocol for a Nationwide Cohort Study. Healthcare, 10(11), 2146. https://doi.org/10.3390/healthcare10112146