


A Low-Cost System Using a Big-Data Deep-Learning Framework for Assessing Physical Telerehabilitation: A Proof-of-Concept

 ,
,  , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
- To present the development of a low-cost system for physical telerehabilitation.
- The use of big data and artificial intelligence technologies to identify the patients’ skeleton while performing telerehabilitation in real time.
- The evaluation of the system in a randomized controlled trial for PD patients’ fall prevention.
- RQ1: Is it possible to enable telerehabilitation for PD patients using low-cost systems?
- RQ2: Is it possible, with these low-cost systems, to process telerehabilitation exercises in real time?
- RQ3: Is the system easy to install and use?
2. Related Works
- It is believed that 3D specialized systems yield the best results [34]. These systems consist of numerous high-resolution cameras that are operated in controlled environments. The main disadvantages of these systems are their costs (several thousands of dollars) and the need for a controlled environment operated by specialized personnel. Some examples are Vicon (Vicon Motion Systems, Oxford, UK) [35], Optotrak (Northern Digital, Inc., Waterloo, ON, Canada), and Prime (NaturalPoint, Inc., Corvallis, OR, USA).
- Mobile capture systems (Microsoft Kinect is one of the best-known) can be installed in uncontrolled and mainly indoor environments. These systems are capable of full-body motion capture in 3D. Kinect has been used as a platform for rehabilitation exercises [36]. Less expensive standard 2D monocular cameras may also be included within this category; they are now also capable of tracking on-screen postures thanks to the appearance of modern deep-learning algorithms (e.g., [37]). Systems based on single 2D cameras in combination with deep learning algorithms have recently been used in the field of rehabilitation. In [38], they were used for the analysis of shoulder rehabilitation exercises and in [39] a client-server system, and the Deep Learning OpenPose framework was used to identify movements of any part of the body. This last work used a smartphone as the only device in the patient’s home, being the system able to estimate the position of the body in exercises previously recorded with this smartphone. Nonetheless, it was not capable of making the estimation in real time.
- Wearable sensor technology is portable and can capture data in uncontrolled environments, even outdoors. These systems are also much less expensive than the specialized 3D capture systems. Wearable sensors have previously been used to monitor patients with PD [40]. However, these same systems are very sensitive to correct placement and calibration, which makes their use very difficult, especially among older patients who have no assistance at that time.
- Video-game handheld controllers. The popular Nintendo Wii console has been used for the treatment of PD patients [41] and stroke rehabilitation [42]; Oculus Quest 2 has also previously been used in shoulder rehabilitation [43]. These systems can perform arm positioning quite precisely, using a combination of accelerometers and optical sensor technology. They are easy to use, but their main limitation is that they only are able to evaluate arm exercises.
2.1. Monocular Human Pose Estimation
2.2. Automatic Evaluation of Motions
- Rule-based methods. These systems require a set of rules to be defined by experts. These rules must capture the key features of each movement that should be executed and evaluated. There are multiple examples in both, sports evaluation [51] and telerehabilitation [52]. This approach requires little computational power and can provide feedback with specific information for experts, such as certain joints not being flexed at a certain angle. As disadvantages, this approach is more prone to generating false positives (incorrect execution of movements) due to errors in the capture sensors; and the set of rules for each move is required to be carefully defined by experts, which can be very difficult in complex moves (can only be applied to specific gestures with quantifiable characteristics). This is an approach with little flexibility or adaptability since modifying an exercise requires a complete review of the set of rules associated with it. An attempt has been made to solve this negative aspect by expressing the rules using a reusable and customized encoding based on eXtensible Markup Language (XML) [53].
- Template-based methods. In this approach, a sequence of movements is recorded a priori, and later, it is used to analyze other sequences of the same movement, carried out by other people. There are two subcategories:
- -
- Distance-based methods. The sequence of movements previously recorded is compared with the observed movements. The system obtains a distance between the movement made by the expert and the movement made by the trainee (e.g., the patient undergoing rehabilitation). A movement can be characterized as the position of the skeletal articulation at each point in time. Usually, the movements are aligned using techniques such as dynamic time warping (DTW) [54] to deal with different execution speeds. Normalization techniques are also used to decrease the influence of the morphology of each individual [55]. This approach is used, for example, in [56], where DTW is used to compare how patients performed a movement before, during, and after treatment.
- -
- Model-based methods. In this case, the recorded sequence of movements is used to train a model that can later be used to classify the observed movement. For example, in [57], a model training-based approach is used to classify movements between “good” and “poor” mobility in patients suffering from age-related impairments. From each frame of a video, a 3D skeleton is extracted using the Kinect camera. This skeleton is processed to obtain a fixed-size instance with numerical attributes, such as the center of mass (CoM), Euclidean distance between the shoulders and wrist, Euler angle between the torso and legs, etc. A motion, therefore, is a length-dependent size list of frame instances. Cluster analysis is used to determine the centroids of each movement, which are subsequently concatenated to create an instance that represents the entire movement. Finally, a classification algorithm, such as random forest or SVM, is trained with a dataset made up of movement instances collected from all patients.
3. Materials and Methods
3.1. Target Population
3.2. Rehabilitation
- First: rotations of the body trunk in a sitting position. In this exercise, the patient is asked to hold a ball with both hands and rotate the trunk to both sides of the body, following the instructions of the therapist. Then, the patient is asked to move the ball toward a series of images placed on the wall behind the patient.
- Second: mobilizations of the lower extremities. In this exercise, the patient is in a sitting position and they must move both feet following the therapist’s instructions, placing them on a series of colored cards arranged on the floor.
- Third: weight exercises with the lower extremities. In these exercises, the patient is in a sitting position and places both feet on a weighing scale, while trying to move the needle on the scales to the level that the therapist might indicate.
- Fourth: straightening reactions. Going from sitting to standing, and vice versa, the patient is asked to place the body in various postures, on a continuum from sitting to standing up.
- Fifth: mobility, balance, and coordination exercises. In a standing position, the patient is asked to follow the therapist’s instructions, moving and placing both feet in each of the four quadrants on the floor.
3.3. Technology
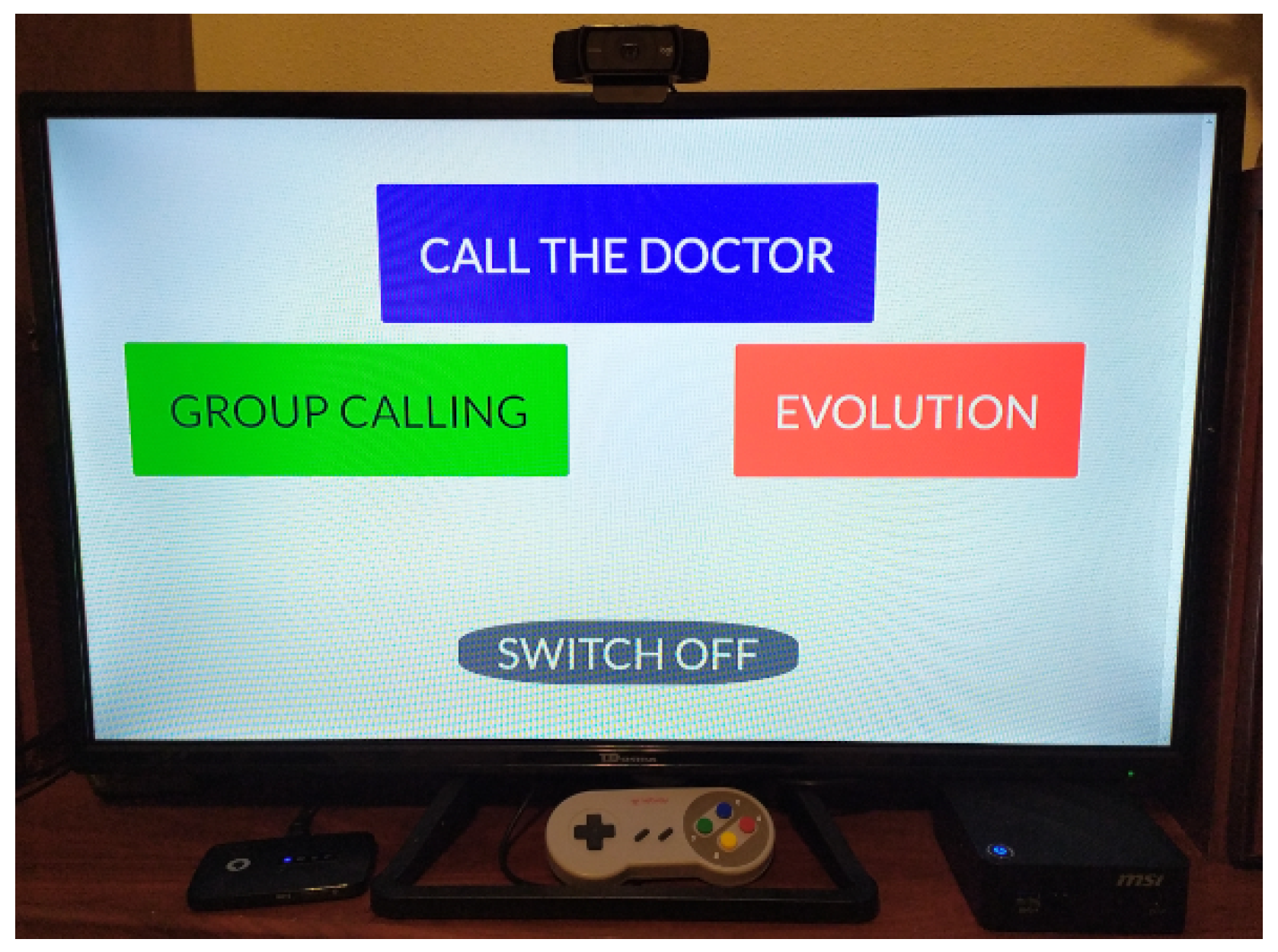
3.3.1. Device and Servers
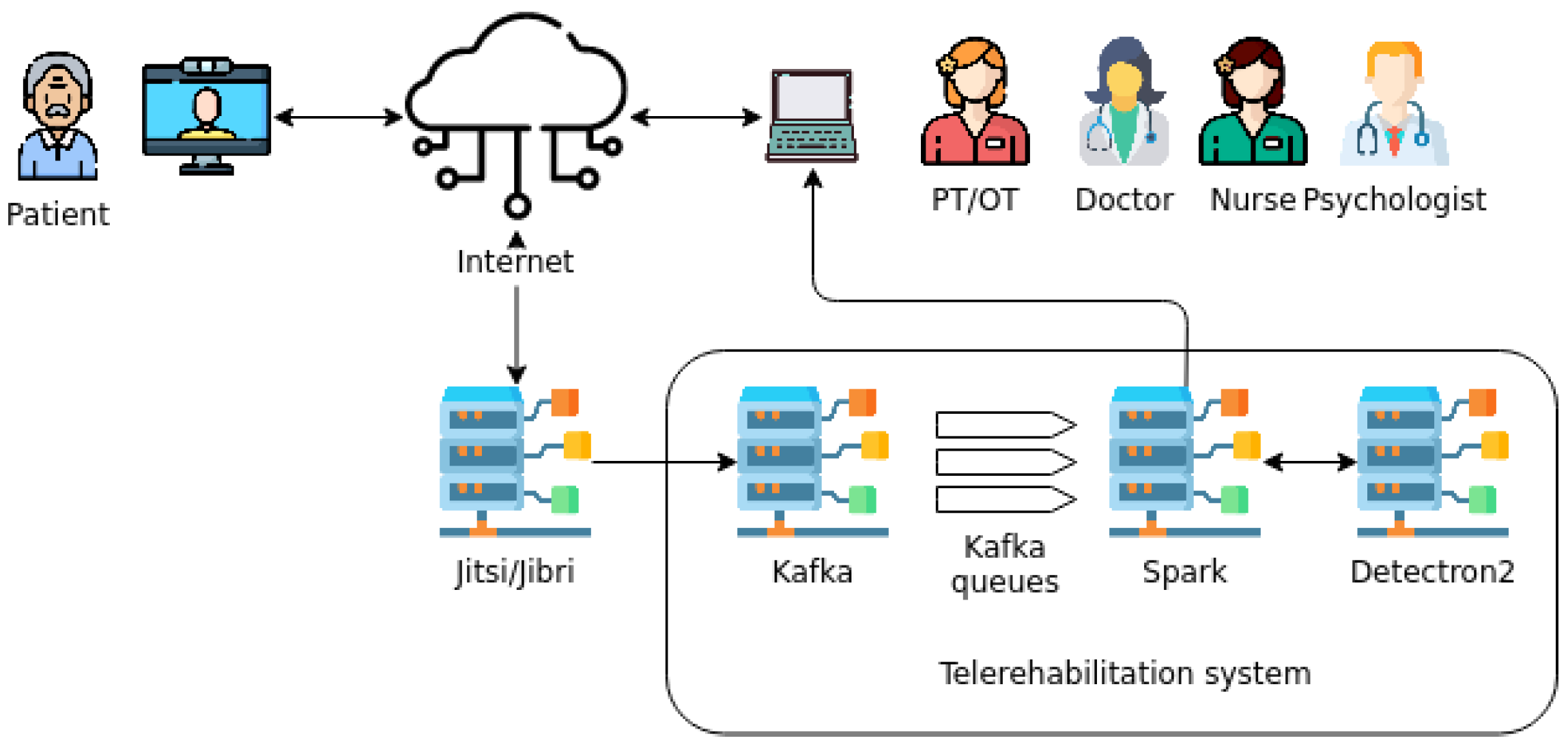
3.3.2. Big Data Architecture
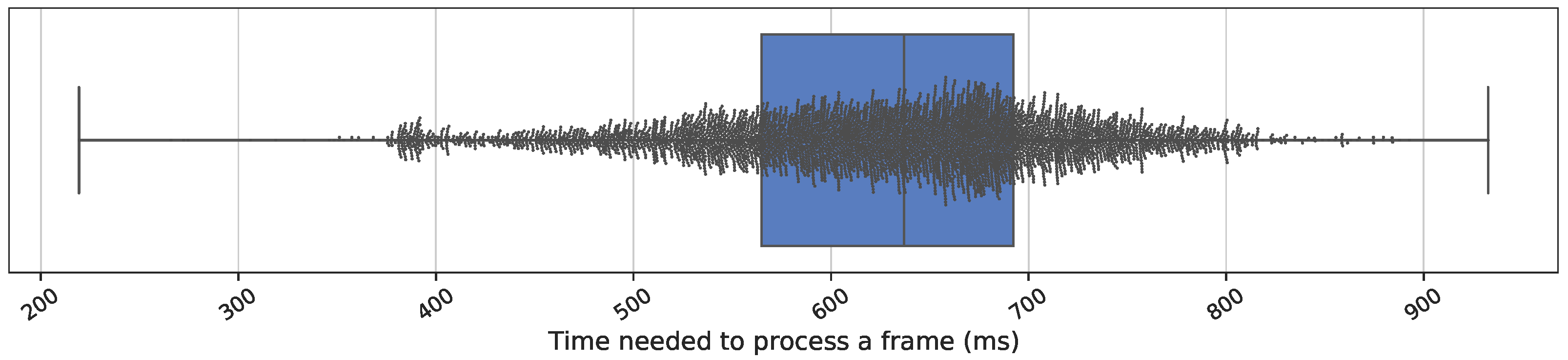
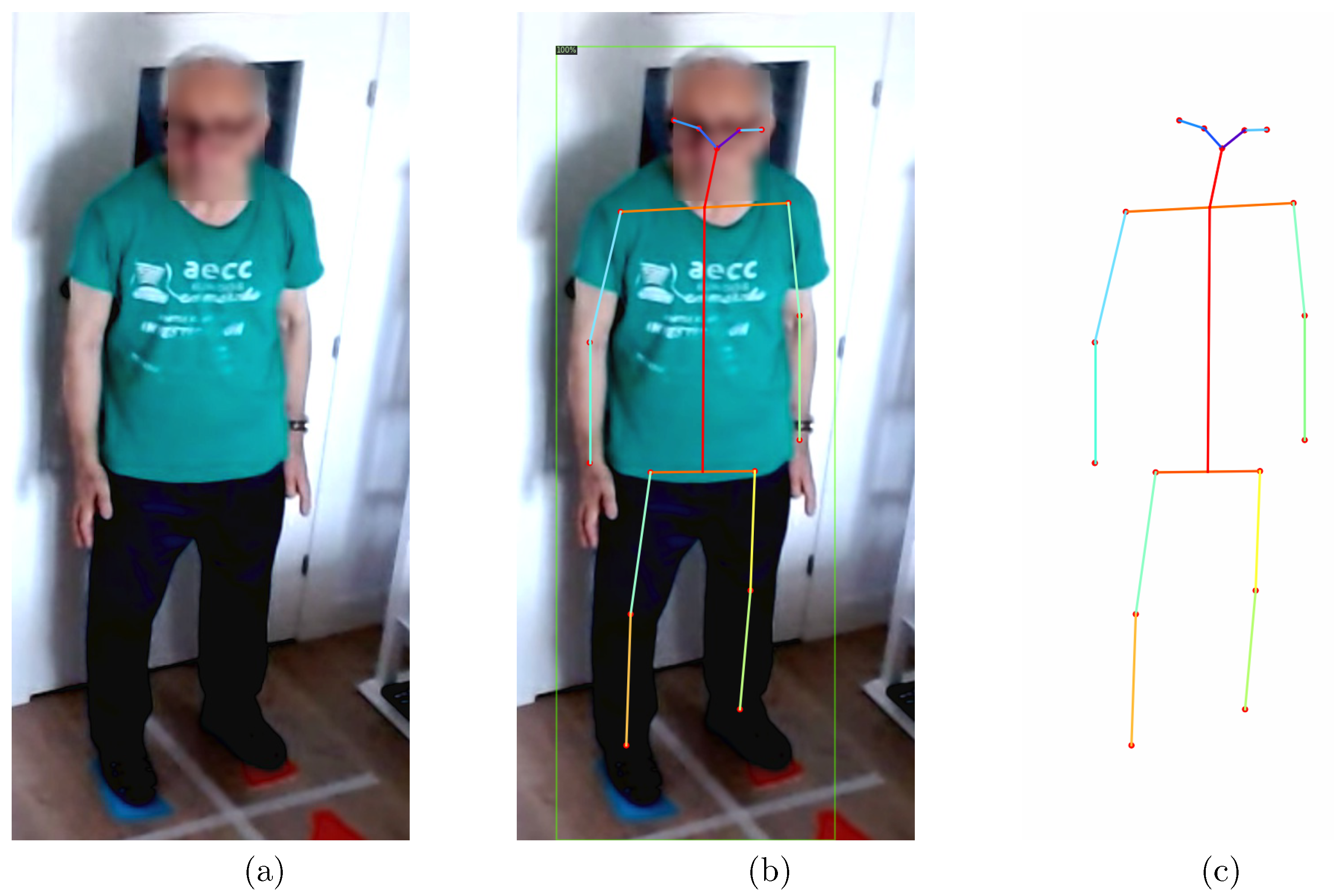
3.3.3. Video Processing
4. Discussion
5. Future Research Lines
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stokes, M. Physical Management in Neurological Rehabilitation; Elsevier Health Sciences: Amsterdam, The Netherlands, 2004. [Google Scholar]
- Dorsey, E.R.; Elbaz, A.; Nichols, E.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.C.; Ansha, M.G.; Brayne, C.; Choi, J.Y.J.; Collado-Mateo, D.; et al. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef]
- Noyes, K.; Liu, H.; Li, Y.; Holloway, R.; Dick, A.W. Economic burden associated with Parkinson’s disease on elderly Medicare beneficiaries. Mov. Disord. 2006, 21, 362–372. [Google Scholar] [CrossRef] [PubMed]
- Canadian Institute for Health Information; Canadian Neurological Sciences Federation; Canadian Brain and Nerve Health Coalition. The Burden of Neurological Diseases, Disorders and Injuries in Canada; Canadian Neurological Sciences Federation: Calgary, AB, Canada, 2007. [Google Scholar]
- Bloem, B.R.; Valkenburg, V.V.; Slabbekoorn, M.; van Dijk, J.G. The multiple tasks test. Strategies in Parkinson’s disease. Exp. Brain Res. 2001, 137, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Kordower, J.H.; Olanow, C.W.; Dodiya, H.B.; Chu, Y.; Beach, T.G.; Adler, C.H.; Halliday, G.M.; Bartus, R.T. Disease duration and the integrity of the nigrostriatal system in Parkinson’s disease. Brain 2013, 136, 2419–2431. [Google Scholar] [CrossRef] [PubMed]
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.E.; Lang, A.E. Parkinson disease. Nat. Rev. Dis. Prim. 2017, 3, 17013. [Google Scholar] [CrossRef]
- Schrag, A.; Hovris, A.; Morley, D.; Quinn, N.; Jahanshahi, M. Caregiver-burden in parkinson’s disease is closely associated with psychiatric symptoms, falls, and disability. Park. Relat. Disord. 2006, 12, 35–41. [Google Scholar] [CrossRef]
- Lezak, M.D.; Howieson, D.B.; Loring, D.W.; Fischer, J.S. Neuropsychological Assessment; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Weil, R.S.; Schrag, A.E.; Warren, J.D.; Crutch, S.J.; Lees, A.J.; Morris, H.R. Visual dysfunction in Parkinson’s disease. Brain 2016, 139, 2827–2843. [Google Scholar] [CrossRef]
- Christiansen, C.; Moore, C.; Schenkman, M.; Kluger, B.; Kohrt, W.; Delitto, A.; Berman, B.; Hall, D.; Josbeno, D.; Poon, C.; et al. Factors associated with ambulatory activity in de novo Parkinson disease. J. Neurol. Phys. Ther. JNPT 2017, 41, 93. [Google Scholar] [CrossRef]
- Balash, Y.; Peretz, C.; Leibovich, G.; Herman, T.; Hausdorff, J.; Giladi, N. Falls in outpatients with Parkinson’s disease. J. Neurol. 2005, 252, 1310–1315. [Google Scholar] [CrossRef]
- Canning, C.G.; Paul, S.S.; Nieuwboer, A. Prevention of falls in Parkinson’s disease: A review of fall risk factors and the role of physical interventions. Neurodegener. Dis. Manag. 2014, 4, 203–221. [Google Scholar] [CrossRef] [Green Version]
- Mak, M.K.; Pang, M.Y. Balance confidence and functional mobility are independently associated with falls in people with Parkinson’s disease. J. Neurol. 2009, 256, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Giladi, N.; Hausdorff, J.M. The role of mental function in the pathogenesis of freezing of gait in Parkinson’s disease. J. Neurol. Sci. 2006, 248, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Radder, D.L.M.; de Vries, N.M.; Riksen, N.P.; Diamond, S.J.; Gross, D.; Gold, D.R.; Heesakkers, J.; Henderson, E.; Hommel, A.L.A.J.; Lennaerts, H.H.; et al. Multidisciplinary care for people with Parkinson’s disease: The new kids on the block! Expert Rev. Neurother. 2019, 19, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Creaby, M.W.; Cole, M.H. Gait characteristics and falls in Parkinson’s disease: A systematic review and meta-analysis. Park. Relat. Disord. 2018, 57, 1–8. [Google Scholar] [CrossRef]
- Almeida, L.R.; Valença, G.T.; Negreiros, N.N.; Pinto, E.B.; Oliveira-Filho, J. Predictors of recurrent falls in people with Parkinson’s disease and proposal for a predictive tool. J. Park. Dis. 2017, 7, 313–324. [Google Scholar] [CrossRef]
- Ellis, T.D.; Cavanaugh, J.T.; DeAngelis, T.; Hendron, K.; Thomas, C.A.; Saint-Hilaire, M.; Pencina, K.; Latham, N.K. Comparative Effectiveness of mHealth-Supported Exercise Compared with Exercise Alone for People with Parkinson Disease: Randomized Controlled Pilot Study. Phys. Ther. 2019, 99, 203–216. [Google Scholar] [CrossRef]
- Shulman, L.M.; Katzel, L.I.; Ivey, F.M.; Sorkin, J.D.; Favors, K.; Anderson, K.E.; Smith, B.A.; Reich, S.G.; Weiner, W.J.; Macko, R.F. Randomized Clinical Trial of 3 Types of Physical Exercise for Patients with Parkinson Disease. JAMA Neurol. 2013, 70, 183–190. [Google Scholar] [CrossRef]
- Pretzer-Aboff, I.; Prettyman, A. Implementation of an Integrative Holistic Healthcare Model for People Living with Parkinson’s Disease. Gerontologist 2015, 55, S146–S153. [Google Scholar] [CrossRef]
- Giordano, A.; Bonometti, G.P.; Vanoglio, F.; Paneroni, M.; Bernocchi, P.; Comini, L.; Giordano, A. Feasibility and cost-effectiveness of a multidisciplinary home-telehealth intervention programme to reduce falls among elderly discharged from hospital: Study protocol for a randomized controlled trial. BMC Geriatr. 2016, 16, 209. [Google Scholar] [CrossRef]
- Cubo, E.; Hassan, A.; Bloem, B.; Mari, Z. Implementation of Telemedicine for Urgent and Ongoing Healthcare for Patients with Parkinson’s Disease during the COVID-19 Pandemic: New Expectations for the Future. J. Park. Dis. 2020, 10, 911–913. [Google Scholar] [CrossRef]
- Ben-Pazi, H.; Browne, P.; Chan, P.; Cubo, E.; Guttman, M.; Hassan, A.; Hatcher-Martin, J.; Mari, Z.; Moukheiber, E.; Okubadejo, N.; et al. The promise of telemedicine for movement disorders: An interdisciplinary approach. Curr. Neurol. Neurosci. Rep. 2018, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Carlos-Vivas, J.; Pérez-Gómez, J.; Delgado-Gil, S.; Campos-López, J.C.; Granado-Sánchez, M.; Rojo-Ramos, J.; Mu noz-Bermejo, L.; Barrios-Fernandez, S.; Mendoza-Mu noz, M.; Prado-Solano, A.; et al. Cost-Effectiveness of “Tele-Square Step Exercise” for Falls Prevention in Fibromyalgia Patients: A Study Protocol. Int. J. Environ. Res. Public Health 2020, 17, 695. [Google Scholar] [CrossRef] [PubMed]
- Jhaveri, M.M.; Benjamin-Garner, R.; Rianon, N.; Sherer, M.; Francisco, G.; Vahidy, F.; Kobayashi, K.; Gaber, M.; Shoemake, P.; Vu, K.; et al. Telemedicine-guided education on secondary stroke and fall prevention following inpatient rehabilitation for Texas patients with stroke and their caregivers: A feasibility pilot study. BMJ Open 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Bettger, J.P.; Green, C.L.; Holmes, D.N.; Chokshi, A.; Mather III, R.C.; Hoch, B.T.; de Leon, A.J.; Aluisio, F.; Seyler, T.M.; Del Gaizo, D.J.; et al. Effects of virtual exercise rehabilitation in-home therapy compared with traditional care after total knee arthroplasty: VERITAS, a randomized controlled trial. JBJS 2020, 102, 101–109. [Google Scholar] [CrossRef]
- Hosseiniravandi, M.; Kahlaee, A.H.; Karim, H.; Ghamkhar, L.; Safdari, R. Home-based telerehabilitation software systems for remote supervising: A systematic review. Int. J. Technol. Assess. Health Care 2020, 36, 113–125. [Google Scholar] [CrossRef]
- Achey, M.; Aldred, J.L.; Aljehani, N.; Bloem, B.R.; Biglan, K.M.; Chan, P.; Cubo, E.; Ray Dorsey, E.; Goetz, C.G.; Guttman, M.; et al. The past, present, and future of telemedicine for Parkinson’s disease. Mov. Disord. 2014, 29, 871–883. [Google Scholar] [CrossRef]
- Samii, A.; Ryan-Dykes, P.; Tsukuda, R.A.; Zink, C.; Franks, R.; Nichol, W.P. Telemedicine for delivery of health care in Parkinson’s disease. J. Telemed. Telecare 2006, 12, 16–18. [Google Scholar] [CrossRef]
- Stamford, J.A.; Schmidt, P.N.; Friedl, K.E. What Engineering Technology Could Do for Quality of Life in Parkinson’s Disease: A Review of Current Needs and Opportunities. IEEE J. Biomed. Health Inform. 2015, 19, 1862–1872. [Google Scholar] [CrossRef]
- Rybarczyk, Y.; Leconte, L.; Medina, J.L.P.; Vargas, K.J.; Acosta-Vargas, P.; Esparza, D. Design of a kinematic and emotional assessment module for the tele-rehabilitation platform. Int. J. Model. Optim. 2019, 9, 92–96. [Google Scholar] [CrossRef]
- Mani, S.; Sharma, S.; Omar, B.; Paungmali, A.; Joseph, L. Validity and reliability of Internet-based physiotherapy assessment for musculoskeletal disorders: A systematic review. J. Telemed. Telecare 2017, 23, 379–391. [Google Scholar] [CrossRef]
- Fong, D.T.P.; Chan, Y.Y. The Use of Wearable Inertial Motion Sensors in Human Lower Limb Biomechanics Studies: A Systematic Review. Sensors 2010, 10, 11556–11565. [Google Scholar] [CrossRef] [PubMed]
- Merriaux, P.; Dupuis, Y.; Boutteau, R.; Vasseur, P.; Savatier, X. A study of vicon system positioning performance. Sensors 2017, 17, 1591. [Google Scholar] [CrossRef]
- Desai, K.; Bahirat, K.; Ramalingam, S.; Prabhakaran, B.; Annaswamy, T.; Makris, U.E. Augmented reality-based exergames for rehabilitation. In Proceedings of the 7th International Conference on Multimedia Systems, Klagenfurt, Austria, 10–13 May 2016; pp. 1–10. [Google Scholar] [CrossRef]
- Liao, Y.; Vakanski, A.; Xian, M. A Deep Learning Framework for Assessing Physical Rehabilitation Exercises. IEEE Trans. Neural Syst. Rehabil. 2020, 28, 468–477. [Google Scholar] [CrossRef]
- Yahya, M.; Shah, J.; Kadir, K.; Warsi, A.; Khan, S.; Nasir, H. Accurate shoulder joint angle estimation using single RGB camera for rehabilitation. In Proceedings of the 2019 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Auckland, New Zealand, 20–23 May 2019; pp. 1–6. [Google Scholar] [CrossRef]
- Prima, O.D.A.; Imabuchi, T.; Ono, Y.; Murata, Y.; Ito, H.; Nishimura, Y. Single camera 3D human pose estimation for tele-rehabilitation. In Proceedings of the eTELEMED 2019: The Eleventh International Conference on eHealth, Telemedicine, and Social Medicine, Athens, Greece, 24–28 February 2019; pp. 13–18. [Google Scholar]
- Chen, B.; Patel, S.; Buckley, T.; Rednic, R.; McClure, D.J.; Shih, L.; Tarsy, D.; Welsh, M.; Bonato, P. A Web-Based System for Home Monitoring of Patients With Parkinson’s Disease Using Wearable Sensors. IEEE Trans. Biomed. Eng. 2011, 58, 831–836. [Google Scholar] [CrossRef]
- Dos Santos Mendes, F.A.; Pompeu, J.E.; Lobo, A.M.; da Silva, K.G.; de Paula Oliveira, T.; Zomignani, A.P.; Piemonte, M.E.P. Motor learning, retention and transfer after virtual-reality-based training in Parkinson’s disease–effect of motor and cognitive demands of games: A longitudinal, controlled clinical study. Physiotherapy 2012, 98, 217–223. [Google Scholar] [PubMed]
- Barcala, L.; Grecco, L.A.C.; Colella, F.; Lucareli, P.R.G.; Salgado, A.S.I.; Oliveira, C.S. Visual biofeedback balance training using wii fit after stroke: A randomized controlled trial. J. Phys. Ther. Sci. 2013, 25, 1027–1032. [Google Scholar]
- Carnevale, A.; Mannocchi, I.; Sassi, M.S.H.; Carli, M.; De Luca, G.; Longo, U.G.; Denaro, V.; Schena, E. Virtual reality for shoulder rehabilitation: Accuracy evaluation of oculus quest 2. Sensors 2022, 22, 5511. [Google Scholar] [CrossRef]
- Chen, Y.; Tian, Y.; He, M. Monocular human pose estimation: A survey of deep learning-based methods. Comput. Vis. Image Underst. 2020, 192, 102897. [Google Scholar] [CrossRef]
- He, K.; Gkioxari, G.; Dollár, P.; Girshick, R. Mask R-CNN. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 2961–2969. [Google Scholar] [CrossRef]
- Girshick, R. Fast R-CNN. In Proceedings of the IEEE International Conference on Computer Vision, Santiago, Chile, 7–13 December 2015; pp. 1440–1448. [Google Scholar]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster R-CNN: Towards real-time object detection with region proposal networks. In Proceedings of the Advances in Neural Information Processing Systems, Montreal, QC, Canada, 7–12 December 2015; Volume 28, pp. 91–99. [Google Scholar]
- Shelhamer, E.; Long, J.; Darrell, T. Fully Convolutional Networks for Semantic Segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 640–651. [Google Scholar] [CrossRef]
- Idris, W.M.R.W.; Rafi, A.; Bidin, A.; Jamal, A.A.; Fadzli, S.A. A systematic survey of martial art using motion capture technologies: The importance of extrinsic feedback. Multimed. Tools Appl. 2019, 78, 10113–10140. [Google Scholar] [CrossRef]
- Hofstad, E.F.; Våpenstad, C.; Chmarra, M.K.; Langø, T.; Kuhry, E.; Mårvik, R. A study of psychomotor skills in minimally invasive surgery: What differentiates expert and nonexpert performance. Surg. Endosc. 2013, 27, 854–863. [Google Scholar] [CrossRef]
- Burns, A.M. On the Relevance of Using Virtual Humans for Motor Skills Teaching: A Case Study on Karate Gestures. Ph.D. Thesis, Université Rennes, Rennes, France, 2013. [Google Scholar]
- Komatireddy, R.; Chokshi, A.; Basnett, J.; Casale, M.; Goble, D.; Shubert, T. Quality and quantity of rehabilitation exercises delivered by a 3-D motion controlled camera: A pilot study. Int. J. Phys. Med. Rehabil. 2014, 2. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Lun, R.; Espy, D.D.; Reinthal, M.A. Rule based realtime motion assessment for rehabilitation exercises. In Proceedings of the 2014 IEEE Symposium on Computational Intelligence in Healthcare and e-Health (CICARE), Orlando, FL, USA, 9–12 December 2014; pp. 133–140. [Google Scholar] [CrossRef]
- Berndt, D.J.; Clifford, J. Using Dynamic Time Warping to Find Patterns in Time Series. In Proceedings of the 3rd International Conference on Knowledge Discovery and Data Mining, Seattle, WA, USA, 31 July–1 August 1994; AAAI Press: Washington, DC, USA, 1994; AAAIWS’94, pp. 359–370. [Google Scholar]
- Morel, M.; Achard, C.; Kulpa, R.; Dubuisson, S. Automatic evaluation of sports motion: A generic computation of spatial and temporal errors. Image Vis. Comput. 2017, 64, 67–78. [Google Scholar] [CrossRef]
- Aghanavesi, S.; Fleyeh, H.; Dougherty, M. Feasibility of using dynamic time warping to measure motor states in Parkinson’s disease. J. Sens. 2020, 2020, 3265795. [Google Scholar] [CrossRef]
- Maudsley-Barton, S.; McPhee, J.; Bukowski, A.; Leightley, D.; Yap, M.H. A comparative study of the clinical use of motion analysis from Kinect skeleton data. In Proceedings of the 2017 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Banff, AB, Canada, 5–8 October 2017; pp. 2808–2813. [Google Scholar] [CrossRef]
- Capecci, M.; Ceravolo, M.G.; Ferracuti, F.; Iarlori, S.; Kyrki, V.; Monteriù, A.; Romeo, L.; Verdini, F. A Hidden Semi-Markov Model based approach for rehabilitation exercise assessment. J. Biomed. Inform. 2018, 78, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Venkataraman, V.; Grana, M.J.; Bull, M.T.; George, B.P.; Boyd, C.M.; Beck, C.A.; Rajan, B.; Seidmann, A.; Biglan, K.M. Randomized Controlled Clinical Trial of “Virtual House Calls” for Parkinson Disease. JAMA Neurol. 2013, 70, 565–570. [Google Scholar] [CrossRef] [Green Version]
- Deters, J.K.; Rybarczyk, Y. Hidden Markov Model approach for the assessment of tele-rehabilitation exercises. Int. J. Artif. Intell. 2018, 16, 1–19. [Google Scholar]
- Hua, A.; Chaudhari, P.; Johnson, N.; Quinton, J.; Schatz, B.; Buchner, D.; Hernandez, M.E. Evaluation of Machine Learning Models for Classifying Upper Extremity Exercises Using Inertial Measurement Unit-Based Kinematic Data. IEEE J. Biomed. Health Inform. 2020, 24, 2452–2460. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Postuma, R.B.; Poewe, W.; Litvan, I.; Lewis, S.; Lang, A.E.; Halliday, G.; Goetz, C.G.; Chan, P.; Slow, E.; Seppi, K.; et al. Validation of the MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2018, 33, 1601–1608. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism. Neurology 1967, 17, 427. [Google Scholar] [CrossRef] [PubMed]
- Hoops, S.; Nazem, S.; Siderowf, A.D.; Duda, J.E.; Xie, S.X.; Stern, M.B.; Weintraub, D. Validity of the MoCA and MMSE in the detection of MCI and dementia in Parkinson disease. Neurology 2009, 73, 1738–1745. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.S.; Canning, C.G.; Sherrington, C.; Lord, S.R.; Close, J.C.T.; Fung, V.S.C. Three simple clinical tests to accurately predict falls in people with Parkinson’s disease. Mov. Disord. 2013, 28, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Vassiliadis, P.; Simitsis, A. Extraction, transformation, and loading. Encycl. Database Syst. 2009. [Google Scholar]
- Jia, Y.; Shelhamer, E.; Donahue, J.; Karayev, S.; Long, J.; Girshick, R.; Guadarrama, S.; Darrell, T. Caffe: Convolutional Architecture for Fast Feature Embedding. arXiv 2014, arXiv:1408.5093. [Google Scholar]
- Wu, Y.; Kirillov, A.; Massa, F.; Lo, W.; Girshick, R. Detectron2. 2019. Available online: https://github.com/facebookresearch/detectron2 (accessed on 5 March 2020).
- Paszke, A.; Gross, S.; Chintala, S.; Chanan, G.; Yang, E.; DeVito, Z.; Lin, Z.; Desmaison, A.; Antiga, L.; Lerer, A. Automatic differentiation in PyTorch. In Proceedings of the NIPS-W, Long Beach, CA, USA, 4–9 December 2017. [Google Scholar]
- Lin, T.Y.; Maire, M.; Belongie, S.; Hays, J.; Perona, P.; Ramanan, D.; Dollár, P.; Zitnick, C.L. Microsoft COCO: Common Objects in Context. In Proceedings of the Computer Vision—ECCV 2014, Zurich, Switzerland, 6–12 September 2014; Fleet, D., Pajdla, T., Schiele, B., Tuytelaars, T., Eds.; Springer International Publishing: Cham, Switzerland, 2014; pp. 740–755. [Google Scholar]
- Lin, T.; Dollar, P.; Girshick, R.; He, K.; Hariharan, B.; Belongie, S. Feature Pyramid Networks for Object Detection. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2117–2125. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Girshick, R.; Donahue, J.; Darrell, T.; Malik, J. Region-Based Convolutional Networks for Accurate Object Detection and Segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2015, 38, 142–158. [Google Scholar] [CrossRef]
- Tinetti, M.E. Multifactorial fall-prevention strategies: Time to retreat or advance. J. Am. Geriatr. Soc. 2008, 56, 1563. [Google Scholar] [CrossRef]
- Parmanto, B.; Lewis, A.N., Jr.; Graham, K.M.; Bertolet, M.H. Development of the telehealth usability questionnaire (TUQ). Int. J. Telerehabilit. 2016, 8, 3. [Google Scholar]
- Elliott, T.; Yopes, M.C. Direct-to-Consumer Telemedicine. J. Allergy Clin. Immunol. Pract. 2019, 7, 2546–2552. [Google Scholar] [CrossRef]
- Espay, A.J.; Bonato, P.; Nahab, F.B.; Maetzler, W.; Dean, J.M.; Klucken, J.; Eskofier, B.M.; Merola, A.; Horak, F.; Lang, A.E.; et al. Technology in Parkinson’s disease: Challenges and opportunities. Mov. Disord. 2016, 31, 1272–1282. [Google Scholar] [CrossRef] [Green Version]
- Fisher, J.M.; Hammerla, N.Y.; Rochester, L.; Andras, P.; Walker, R.W. Body-Worn Sensors in Parkinson’s Disease: Evaluating Their Acceptability to Patients. Telemed. E-Health 2016, 22, 63–69. [Google Scholar] [CrossRef]
- Ledger, D.; McCaffrey, D. Inside wearables: How the science of human behavior change offers the secret to long-term engagement. Endeav. Partners 2014, 200, 1. [Google Scholar]
- Capecci, M.; Ceravolo, M.G.; Ferracuti, F.; Grugnetti, M.; Iarlori, S.; Longhi, S.; Romeo, L.; Verdini, F. An instrumental approach for monitoring physical exercises in a visual markerless scenario: A proof of concept. J. Biomech. 2018, 69, 70–80. [Google Scholar] [CrossRef]
- Iskakov, K.; Burkov, E.; Lempitsky, V.; Malkov, Y. Learnable triangulation of human pose. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Seoul, Republic of Korea, 27–28 October 2019; pp. 7718–7727. [Google Scholar]
- Reddy, N.D.; Guigues, L.; Pishchulin, L.; Eledath, J.; Narasimhan, S.G. Tessetrack: End-to-end learnable multi-person articulated 3d pose tracking. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Nashville, TN, USA, 20–25 June 2021; pp. 15190–15200. [Google Scholar]
- Zhang, J.; Tu, Z.; Yang, J.; Chen, Y.; Yuan, J. MixSTE: Seq2seq Mixed Spatio-Temporal Encoder for 3D Human Pose Estimation in Video. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, New Orleans, LA, USA, 18–24 June 2022; pp. 13232–13242. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 3D Specialized Systems | Movable Capture Systems (3D Cameras) | Movable Capture Systems (2D Cameras) | Wearable Wireless Sensors | Handheld Game Controllers | |
|---|---|---|---|---|---|
| Sample hardware | Vicon, Optotrak, Prime | Microsoft Kinect | Logitech HD Pro C920 | LilyPad, Steval | Nintendo Wii |
| Environment | Indoor, controlled environment | Indoor | Mainly indoor | Indoor, outdoor | Indoor, outdoor |
| Installation | Complex | Easy | Easy | Medium | Easy |
| Use | Complex | Easy | Easy | Complex | Easy |
| Scope | Full body | Full body | Full body | Full body | Arms |
| Quality | High | Medium | Medium | Medium | Medium |
| Price | High | Medium | Low | Medium | Medium |
| Model | Loading (ms) | Processing (ms) |
|---|---|---|
| keypoint_rcnn_R_50_FPN_1x | 8083.19 | 216,519.97 |
| keypoint_rcnn_R_50_FPN_3x | 7539.65 | 216,625.36 |
| keypoint_rcnn_R_101_FPN_3x | 9806.49 | 259,716.33 |
| keypoint_rcnn_X_101_32x8d_FPN_3x | 14,853.03 | 407,086.70 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez-Sanz, J.M.; Garrido-Labrador, J.L.; Olivares-Gil, A.; García-Bustillo, Á.; Arnaiz-González, Á.; Díez-Pastor, J.-F.; Jahouh, M.; González-Santos, J.; González-Bernal, J.J.; Allende-Río, M.; et al. A Low-Cost System Using a Big-Data Deep-Learning Framework for Assessing Physical Telerehabilitation: A Proof-of-Concept. Healthcare 2023, 11, 507. https://doi.org/10.3390/healthcare11040507
Ramírez-Sanz JM, Garrido-Labrador JL, Olivares-Gil A, García-Bustillo Á, Arnaiz-González Á, Díez-Pastor J-F, Jahouh M, González-Santos J, González-Bernal JJ, Allende-Río M, et al. A Low-Cost System Using a Big-Data Deep-Learning Framework for Assessing Physical Telerehabilitation: A Proof-of-Concept. Healthcare. 2023; 11(4):507. https://doi.org/10.3390/healthcare11040507
Chicago/Turabian StyleRamírez-Sanz, José Miguel, José Luis Garrido-Labrador, Alicia Olivares-Gil, Álvaro García-Bustillo, Álvar Arnaiz-González, José-Francisco Díez-Pastor, Maha Jahouh, Josefa González-Santos, Jerónimo J. González-Bernal, Marta Allende-Río, and et al. 2023. "A Low-Cost System Using a Big-Data Deep-Learning Framework for Assessing Physical Telerehabilitation: A Proof-of-Concept" Healthcare 11, no. 4: 507. https://doi.org/10.3390/healthcare11040507
APA StyleRamírez-Sanz, J. M., Garrido-Labrador, J. L., Olivares-Gil, A., García-Bustillo, Á., Arnaiz-González, Á., Díez-Pastor, J. -F., Jahouh, M., González-Santos, J., González-Bernal, J. J., Allende-Río, M., Valiñas-Sieiro, F., Trejo-Gabriel-Galan, J. M., & Cubo, E. (2023). A Low-Cost System Using a Big-Data Deep-Learning Framework for Assessing Physical Telerehabilitation: A Proof-of-Concept. Healthcare, 11(4), 507. https://doi.org/10.3390/healthcare11040507