
Psychometric Properties of the Traditional Chinese Version of the Stanford Presenteeism Scale (SPS-6) among Taiwanese Employees in Technology Companies



Abstract
:1. Introduction
2. Materials and Methods
2.1. Psychometric Properties
2.2. The Process of Translation
2.3. Samples
2.4. Measures
2.5. Data Analysis
- The S-CVI was calculated by averaging I-CVI values [29].
- Through email, we asked the first expert panel whether the translated version was easy to comprehend and would it be clear for all Taiwanese populations with five responses from 1 (“strongly disagree”) to 5 (“strongly agree”).
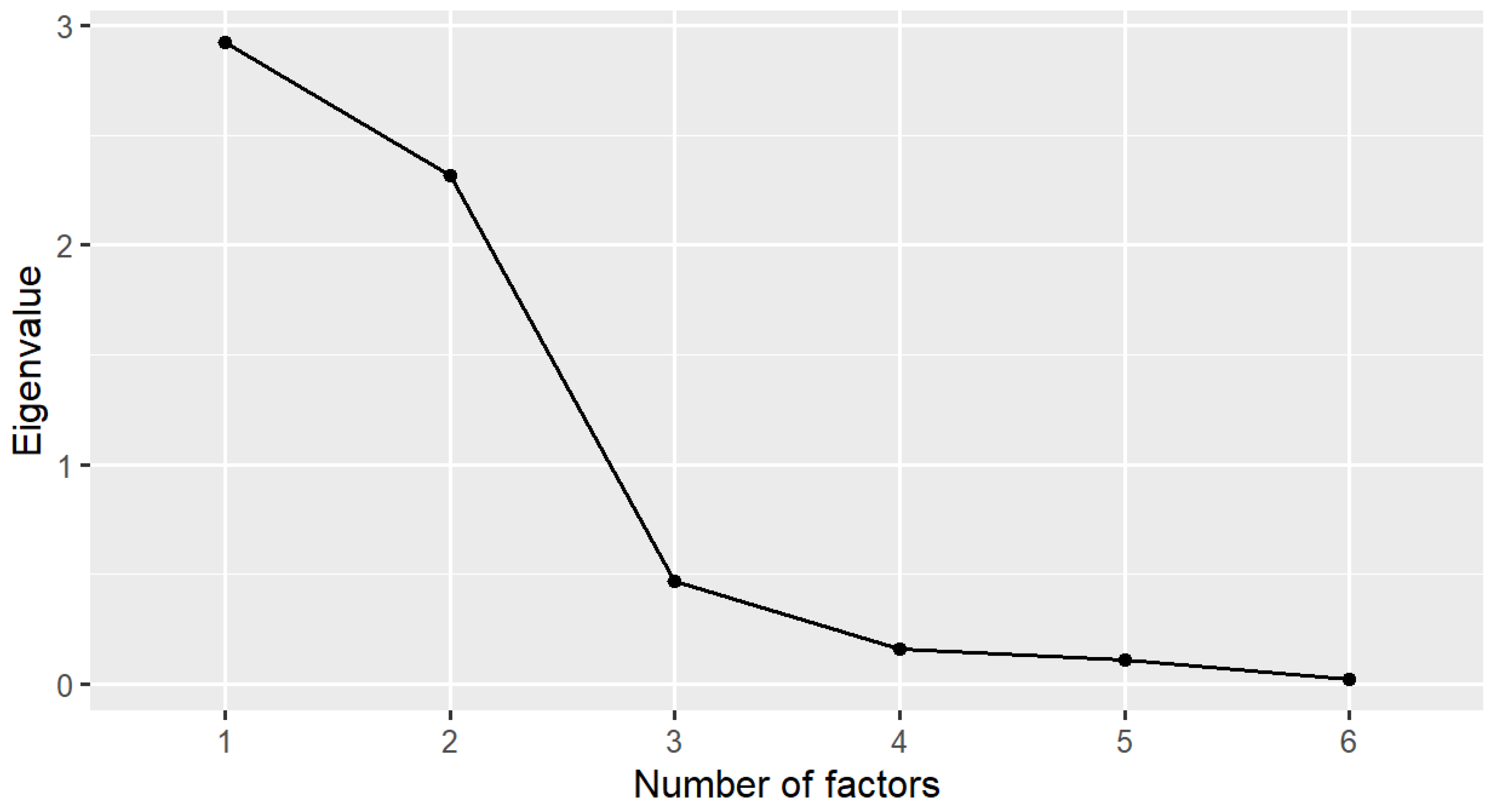
- Before conducting the EFA, we used the Kaiser–Mayer–Olkin (KMO) test to assess the sampling adequacy. A KMO index ≥0.50 is an acceptable value [34], and Bartlett’s test of sphericity with a significant statistical test (p < 0.05) [35] is desirable. The EFA with principal component analysis extraction and Varimax rotation methods was applied to test the dimensions of the CSPS-6. Items with a factor loading of >0.40 were set. Two methods we used to define the number of factors retained were the Kaiser criterion of eigenvalues (eigenvalue >1 rule) [36,37] and a scree plot. Factors to be retained were determined by the eigenvalues above and to the left of the straight line through the smallest eigenvalues on the scree plot [38,39].
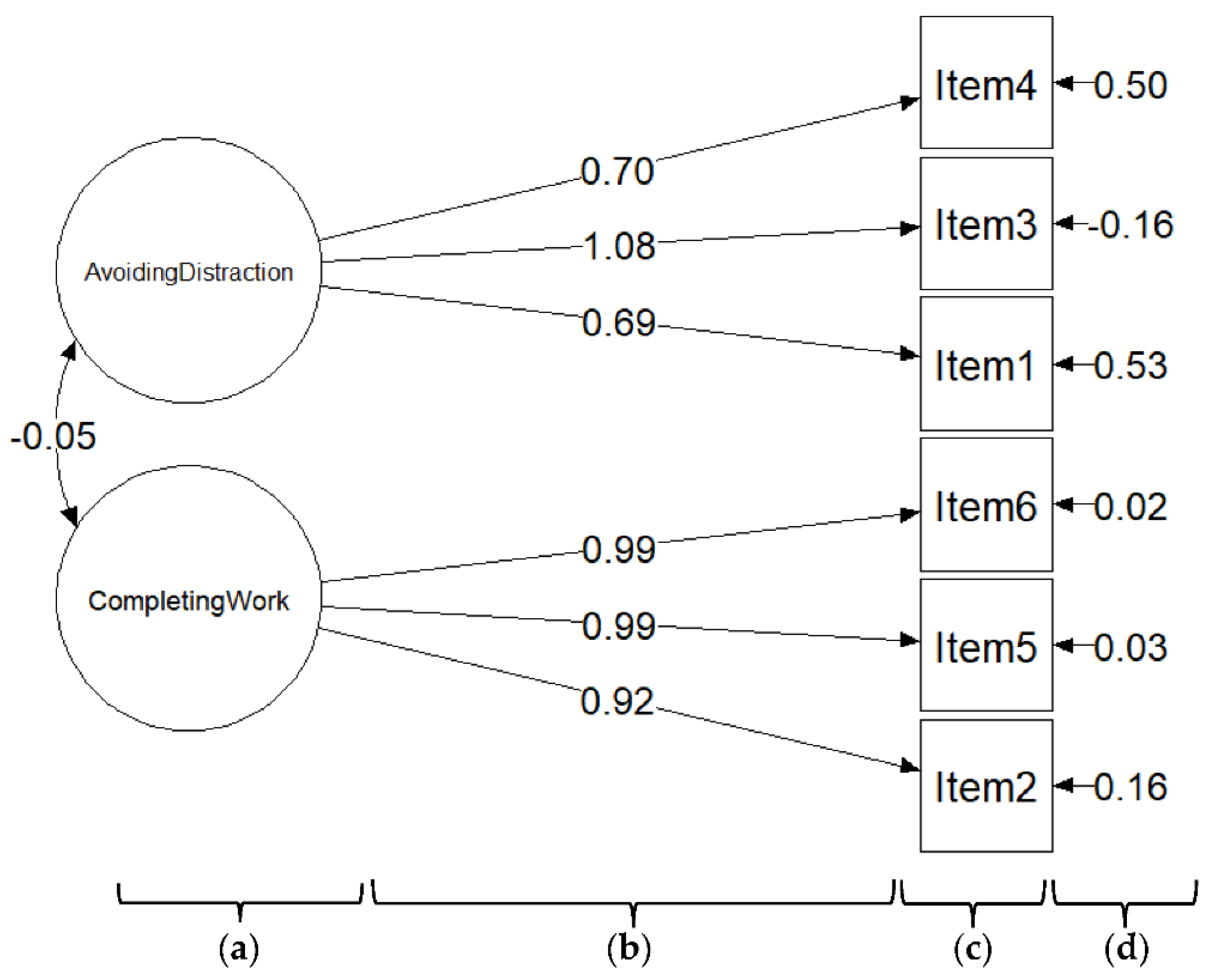
- A CFA was performed to confirm the structural validity of the CSPS-6. With a sample size N of ≤250, Hu and Bender (1999) recommended a two-index presentation strategy using the combination rule of fit indexes to conclude the model fit [40]. Therefore, we reported a combination of the comparative fit index (CFI) (or Tucker–Lewis Index (TLI)) with the standardized root-mean-squared residual (SRMR) for model evaluation. Cutoff values for these indices to determine a good model fit were a CFI of ≥0.95 (or a TLI of ≥0.95) and an SRMR of ≤0.08 [40]. The factor loading of an item was interpreted as excellent, very good, good, fair, and poor with loadings exceeding 0.71, 0.63, 0.55, 0.45, and 0.32, respectively [41,42].
3. Results
3.1. Internal Consistency
3.2. Content Validity
3.3. Structural Validity (Construct Validity)
3.4. Hypothesis Testing (Construct Validity)
3.5. Concurrent Validity (Criterion Validity)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kessler, R.C.; Barber, C.; Beck, A.; Berglund, P.; Cleary, P.D.; McKenas, D.; Pronk, N.; Simon, G.; Stang, P.; Ustun, T.B.; et al. The World Health Organization Health and Work Performance Questionnaire (HPQ). J. Occup. Environ. Med. 2003, 45, 156–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Ames, M.; Hymel, P.A.; Loeppke, R.; McKenas, D.K.; Richling, D.E.; Stang, P.E.; Ustun, T.B. Using the World Health Organization Health and Work Performance Questionnaire (HPQ) to Evaluate the Indirect Workplace Costs of Illness. J. Occup. Environ. Med. 2004, 46, S23–S37. [Google Scholar] [CrossRef] [PubMed]
- Bergström, G.; Bodin, L.; Hagberg, J.; Lindh, T.; Aronsson, G.; Josephson, M. Does Sickness Presenteeism Have an Impact on Future General Health? Int. Arch. Occup. Environ. Health 2009, 82, 1179–1190. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.F.; Ricci, J.A.; Chee, E.; Morganstein, D.; Lipton, R. Lost Productive Time and Cost Due to Common Pain Conditions in the US Workforce. JAMA 2003, 290, 2443–2454. [Google Scholar] [CrossRef] [Green Version]
- Goetzel, R.Z.; Long, S.R.; Ozminkowski, R.J.; Hawkins, K.; Wang, S.; Lynch, W. Health, Absence, Disability, and Presenteeism Cost Estimates of Certain Physical and Mental Health Conditions Affecting U.S. Employers. J. Occup. Environ. Med. 2004, 46, 398–412. [Google Scholar] [CrossRef] [Green Version]
- Koopman, C.; Pelletier, K.R.; Murray, J.F.; Sharda, C.E.; Berger, M.L.; Turpin, R.S.; Hackleman, P.; Gibson, P.; Holmes, D.M.; Bendel, T. Stanford Presenteeism Scale: Health Status and Employee Productivity. J. Occup. Environ. Med. 2002, 44, 14–20. [Google Scholar] [CrossRef]
- Johns, G. Presenteeism in the Workplace: A Review and Research Agenda: Presenteeism in the workplace. J. Organ. Behav. 2010, 31, 519–542. [Google Scholar] [CrossRef]
- Ospina, M.B.; Dennett, L.; Waye, A.; Jacobs, P.; Thompson, A.H. A Systematic Review of Measurement Properties of Instruments Assessing Presenteeism. Am. J. Manag. CARE 2015, 21, 15. [Google Scholar]
- Hubens, K.; Krol, M.; Coast, J.; Drummond, M.F.; Brouwer, W.B.F.; Uyl-de Groot, C.A.; Hakkaart-van Roijen, L. Measurement Instruments of Productivity Loss of Paid and Unpaid Work: A Systematic Review and Assessment of Suitability for Health Economic Evaluations From a Societal Perspective. Value Health 2021, 24, 1686–1699. [Google Scholar] [CrossRef]
- Frauendorf, R.; de Medeiros Pinheiro, M.; Ciconelli, R.M. Translation into Brazilian Portuguese, Cross-Cultural Adaptation and Validation of the Stanford Presenteeism Scale-6 and Work Instability Scale for Ankylosing Spondylitis. Clin. Rheumatol. 2014, 33, 1751–1757. [Google Scholar] [CrossRef]
- Laranjeira, C.A. Validation of the Portuguese Version of the Stanford Presenteeism Scale in Nurses: Portuguese Stanford Presenteeism Scale. Int. J. Nurs. Pract. 2013, 19, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Hutting, N.; Engels, J.A.; Heerkens, Y.F.; Staal, J.B.; Nijhuis-van der Sanden, M.W.G. Development and Measurement Properties of the Dutch Version of the Stanford Presenteeism Scale (SPS-6). J. Occup. Rehabil. 2014, 24, 268–277. [Google Scholar] [CrossRef]
- Cicolini, G.; Della Pelle, C.; Cerratti, F.; Franza, M.; Flacco, M.E. Validation of the Italian Version of the Stanford Presenteeism Scale in Nurses. J. Nurs. Manag. 2016, 24, 598–604. [Google Scholar] [CrossRef]
- Abdi, F.; Jahangiri, M.; Kamalinia, M.; Cousins, R.; Mokarami, H. Presenteeism and Work Ability: Development of the Persian Version of the Stanford Presenteeism Scale (P-SPS-6) and Measurement of Its Psychometric Properties. BMC Psychol. 2021, 9, 120. [Google Scholar] [CrossRef] [PubMed]
- Baldonedo-Mosteiro, M.; Sánchez-Zaballos, M.; Rodríguez-Díaz, F.J.; Herrero, J.; Mosteiro-Díaz, M.P. Adaptation and Validation of the Stanford Presenteeism Scale-6 in Healthcare Professionals. Int. Nurs. Rev. 2020, 67, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Intensive Care Unit Nurse, Sisli Hamidiye Etfal Training and Research Hospital, University of Health Sciences Turkey, Istanbul, Turkey; Teoman, E.; Seren, A.K.H.; Department of Nursing, Fenerbahce University, Faculty of Health Sciences, Istanbul, Turkey. Psychometrics of Stanford Presenteeism Scale-Short Form in Turkish. Florence Nightingale J. Nurs. 2022, 30, 190–195. [Google Scholar] [CrossRef]
- Paschoalin, H.C.; Griep, R.H.; Lisboa, M.T.L.; de Mello, D.C.B. Transcultural Adaptation and Validation of the Stanford Presenteeism Scale for the Evaluation of Presenteeism for Brazilian Portuguese. Rev. Lat. Am. Enfermagem 2013, 21, 388–395. [Google Scholar] [CrossRef] [Green Version]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C.W. The COSMIN Study Reached International Consensus on Taxonomy, Terminology, and Definitions of Measurement Properties for Health-Related Patient-Reported Outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef] [Green Version]
- Braakman-Jansen, L.M.A.; Taal, E.; Kuper, I.H.; van de Laar, M.A.F.J. Productivity Loss Due to Absenteeism and Presenteeism by Different Instruments in Patients with RA and Subjects without RA. Rheumatology 2012, 51, 354–361. [Google Scholar] [CrossRef] [Green Version]
- Sousa, V.D.; Rojjanasrirat, W. Translation, Adaptation and Validation of Instruments or Scales for Use in Cross-Cultural Health Care Research: A Clear and User-Friendly Guideline: Validation of Instruments or Scales. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef]
- Jackson, D.L. Revisiting Sample Size and Number of Parameter Estimates: Some Support for the N:Q Hypothesis. Struct. Equ. Model. Multidiscip. J. 2003, 10, 128–141. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Hays, R.D.; Sherbourne, C.D.; Mazel, R.M. The Rand 36-Item Health Survey 1.0. Health Econ. 1993, 2, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Reilly, M.C.; Zbrozek, A.S.; Dukes, E.M. The Validity and Reproducibility of a Work Productivity and Activity Impairment Instrument. PharmacoEconomics 1993, 4, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Ta-Thi, K.-N.; Chuang, K.-J. A Comparison of the Validities of Traditional Chinese Versions of the Work Productivity and Activity Impairment Questionnaire: General Health and the World Health Organization’s Health and Work Performance Questionnaire. Int. J. Environ. Res. Public Health 2022, 19, 4417. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Taber, K.S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef] [Green Version]
- McHorney, C.A.; Tarlov, A.R. Individual-Patient Monitoring in Clinical Practice: Are Available Health Status Surveys Adequate? Qual. Life Res. 1995, 4, 293–307. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. The Content Validity Index: Are You Sure You Know What’s Being Reported? Critique and Recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef] [Green Version]
- Rubio, D.M.; Berg-Weger, M.; Tebb, S.S.; Lee, E.S.; Rauch, S. Objectifying Content Validity: Conducting a Content Validity Study in Social Work Research. Soc. Work Res. 2003, 27, 94–104. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an Acceptable Indicator of Content Validity? Appraisal and Recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Halek, M.; Holle, D.; Bartholomeyczik, S. Development and Evaluation of the Content Validity, Practicability and Feasibility of the Innovative Dementia-Oriented Assessment System for Challenging Behaviour in Residents with Dementia. BMC Health Serv. Res. 2017, 17, 554. [Google Scholar] [CrossRef] [Green Version]
- Fleiss, J.L.; Levin, B.; Paik, M.C. Statistical Methods for Rates and Proportions, 3rd ed.; John Wiley: Hoboken, NJ, USA, 2003; ISBN 978-0-471-52629-2. [Google Scholar]
- Kaiser, H.F. An Index of Factorial Simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Williams, B.; Onsman, A.; Brown, T. Exploratory Factor Analysis: A Five-Step Guide for Novices. Australas. J. Paramed. 2010, 8, 3. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, H.F. The Application of Electronic Computers to Factor Analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Norris, M.; Lecavalier, L. Evaluating the Use of Exploratory Factor Analysis in Developmental Disability Psychological Research. J. Autism Dev. Disord. 2010, 40, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Pett, M.A.; Lackey, N.R.; Sullivan, J.J. Making Sense of Factor Analysis: The Use of Factor Analysis for Instrument Development in Health Care Research; SAGE Publications: Thousand Oaks, CA, USA, 2003; ISBN 978-0-7619-1949-0. [Google Scholar]
- Cattell, R.B. The Scree Test For The Number Of Factors. Multivar. Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Pearson Education Inc.: New York City, NY, USA, 2013. [Google Scholar]
- Comrey, A.L.; Lee, H.B. A First Course in Factor Analysis, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1992; ISBN 978-0-8058-1062-2. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Kawai, K.; Kawai, A.T.; Wollan, P.; Yawn, B.P. Adverse Impacts of Chronic Pain on Health-Related Quality of Life, Work Productivity, Depression and Anxiety in a Community-Based Study. Fam. Pract. 2017, 34, 656–661. [Google Scholar] [CrossRef]
- Keramat, S.A.; Alam, K.; Gow, J.; Biddle, S.J.H. A Longitudinal Exploration of the Relationship between Obesity, and Long Term Health Condition with Presenteeism in Australian Workplaces, 2006–2018. PLoS ONE 2020, 15, e0238260. [Google Scholar] [CrossRef]
- Yang, T.; Guo, Y.; Ma, M.; Li, Y.; Tian, H.; Deng, J. Job Stress and Presenteeism among Chinese Healthcare Workers: The Mediating Effects of Affective Commitment. Int. J. Environ. Res. Public. Health 2017, 14, 978. [Google Scholar] [CrossRef] [Green Version]
- Niven, K.; Ciborowska, N. The Hidden Dangers of Attending Work While Unwell: A Survey Study of Presenteeism Among Pharmacists. Int. J. Stress Manag. 2015, 22, 207–221. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | n (%) |
|---|---|
| Age + | 34.08 (7.55) |
| Gender Male | 158 (79.6) |
| Educational attainment | |
| High school | 75 (38.3) |
| Undergraduate | 91 (46.4) |
| Postgraduate | 30 (15.3) |
| Marital status | |
| Married/cohabiting | 86 (43.9) |
| Separated/divorced/widowed | 5 (2.5) |
| Never married | 105 (53.6) |
| Type of job | |
| Manager, professional | 26 (13.2) |
| Technologist | 109 (55.6) |
| Office job, service | 61 (31.2) |
| Disability status | |
| Work-related disability | 135 (68.9) |
| Non-work-related disability | 6 (3.1) |
| No disability | 55 (28.0) |
| Item | Factor 1 (Completing Work) | Factor 2 (Avoiding Distraction) |
|---|---|---|
| Item 1 | 0.845 | |
| Item 2 | 0.959 | |
| Item 3 | 0.951 | |
| Item 4 | 0.843 | |
| Item 5 | 0.981 | |
| Item 6 | 0.983 | |
| Total variance explained | 48.5% | 38.9% |
| Eigenvalue | 2.91 | 2.33 |
| Health Status Outcome | Mean (Standard Deviation) | rs |
|---|---|---|
| Role—Physical | 86.10 (23.91) | rs = 0.31 |
| Physical functioning | 94.61 (9.89) | rs = 0.32 |
| Role—Emotional | 91.80 (19.56) | rs = 0.28 |
| Pain | 84.44 (23.83) | rs = 0.29 |
| Social functioning | 84.76 (21.66) | rs = 0.48 |
| Vitality | 69.13 (18.16) | rs = 0.52 |
| General health | 57.50 (16.66) | rs = 0.47 |
| Mental health | 75.51 (16.38) | rs = 0.42 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ta-Thi, K.-N.; Chuang, K.-J. Psychometric Properties of the Traditional Chinese Version of the Stanford Presenteeism Scale (SPS-6) among Taiwanese Employees in Technology Companies. Healthcare 2022, 10, 2202. https://doi.org/10.3390/healthcare10112202
Ta-Thi K-N, Chuang K-J. Psychometric Properties of the Traditional Chinese Version of the Stanford Presenteeism Scale (SPS-6) among Taiwanese Employees in Technology Companies. Healthcare. 2022; 10(11):2202. https://doi.org/10.3390/healthcare10112202
Chicago/Turabian StyleTa-Thi, Kim-Ngan, and Kai-Jen Chuang. 2022. "Psychometric Properties of the Traditional Chinese Version of the Stanford Presenteeism Scale (SPS-6) among Taiwanese Employees in Technology Companies" Healthcare 10, no. 11: 2202. https://doi.org/10.3390/healthcare10112202
APA StyleTa-Thi, K. -N., & Chuang, K. -J. (2022). Psychometric Properties of the Traditional Chinese Version of the Stanford Presenteeism Scale (SPS-6) among Taiwanese Employees in Technology Companies. Healthcare, 10(11), 2202. https://doi.org/10.3390/healthcare10112202