
Racial Differences in Breastfeeding on the Mississippi Gulf Coast: Making Sense of a Promotion-Prevalence Paradox with Cross-Sectional Data

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Setting and Relevant Context
2.3. Data Collection and Sample
2.4. Measurement
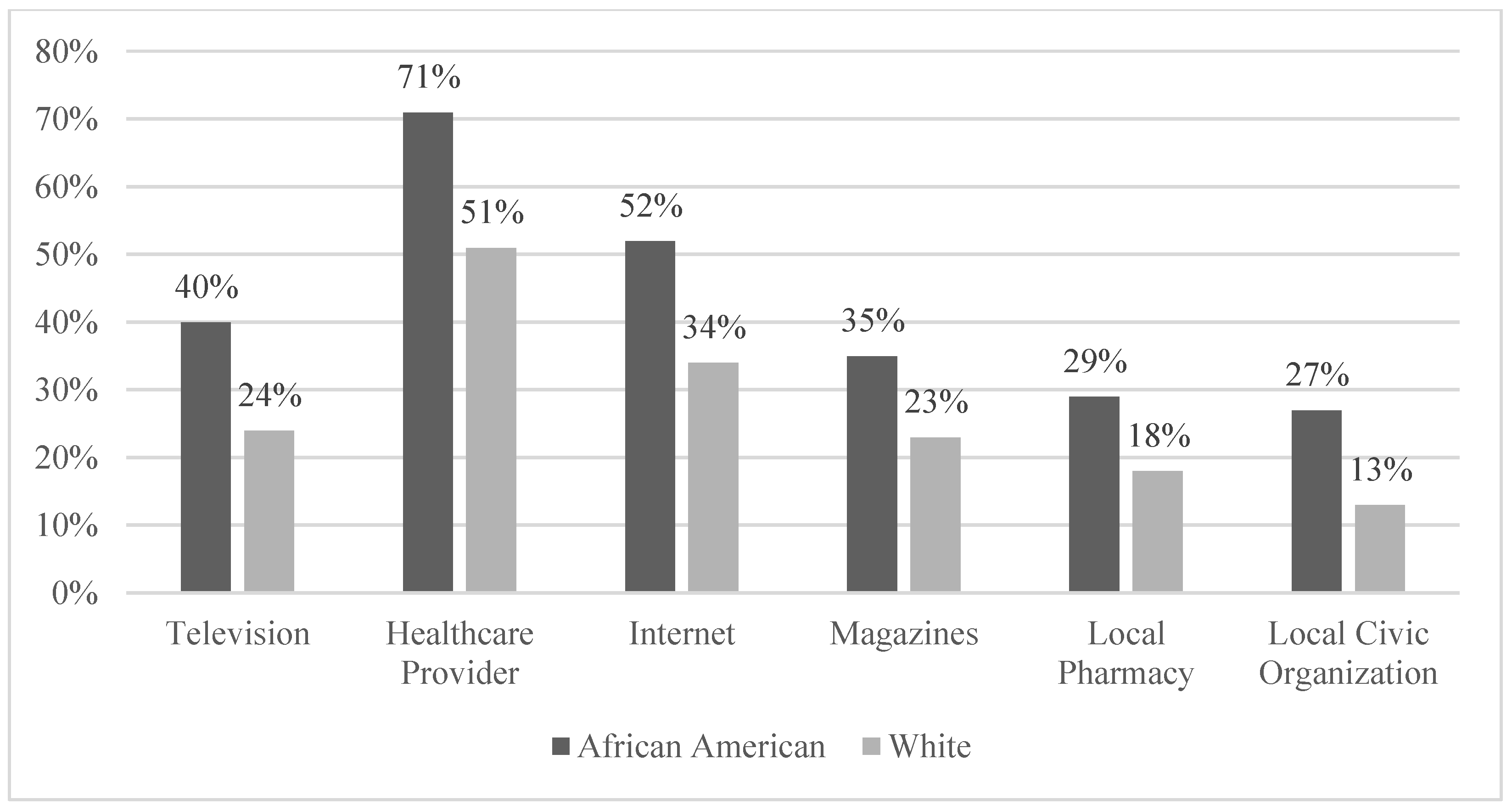
2.4.1. Exposure to Breastfeeding Promotion
2.4.2. Prevalence of Breastfeeding in Primary Social Networks
2.4.3. Predictor and Control Variables
2.5. Data Analysis
3. Results
4. Discussion
4.1. Implications for Policy and Practice
4.2. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anstey, E.H.; Chen, J.; Elam-Evans, L.D.; Perrine, C.G. Racial and geographic differences in breastfeeding—United States, 2011–2015. Morb. Mortal. Wkly. Rep. 2017, 66, 723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healthypeople.gov. Maternal, infant, and child health: Healthy people 2020. Available online: https://www.healthypeople.gov/2020/topics-objectives/topic/maternal-infant-and-child-health/objectives (accessed on 8 October 2020).
- Health.gov. Infants: Healthy people 2030. 2015. Available online: https://health.gov/healthypeople/objectives-and-data/browse-objectives/infants (accessed on 1 June 2021).
- Merewood, A.; Bugg, K.; Burnham, L.; Krane, K.; Nickel, N.; Broom, S.; Edwards, R.; Feldman-Winter, L. Addressing racial inequities in breastfeeding in the Southern United States. Pediatrics 2019, 143, e20181897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, K.; Fial, A.; Hanson, L. Racism, bias, and discrimination as modifiable barriers to breastfeeding for African American women: A scoping review of the literature. J. Midwifery Women’s Health 2019, 64, 734–742. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture. WIC participant and program characteristics 2010 report. 2011. Available online: www.fns.usda.gov/sites/default/files/WICPC2010.pdf (accessed on 1 June 2021).
- Johnson, A.M.; Kirk, R.; Rosenblum, K.L.; Muzik, M. Enhancing breastfeeding rates among African American women: A systematic review of current psychosocial interventions. Breastfeed. Med. 2015, 10, 45–62. [Google Scholar] [CrossRef] [Green Version]
- Meyerink, R.O.; Marquis, G.S. Breastfeeding initiation and duration among low-income women in Alabama: The importance of personal and familial experiences in making infant-feeding choices. J. Hum. Lact. 2002, 18, 38–45. [Google Scholar] [CrossRef]
- Alakaam, A.; Lemacks, J.; Yadrick, K.; Connell, C.; Choi, H.W.; Newman, R.G. Breastfeeding practices and barriers to implementing the ten steps to successful breastfeeding in Mississippi hospitals. J. Hum. Lact. 2018, 34, 322–330. [Google Scholar] [CrossRef]
- Alakaam, A.; Lemacks, J.; Yadrick, K.; Connell, C.; Choi, H.W.; Newman, R.G. Maternity nurses’ knowledge and practice of breastfeeding in Mississippi. MCN: Am. J. Matern. /Child Nurs. 2018, 43, 225–230. [Google Scholar] [CrossRef]
- Deubel, T.F.; Miller, E.M.; Hernandez, I.; Boyer, M.; Louis-Jacques, A. Perceptions and practices of infant feeding among African American women. Ecol. Food Nutr. 2019, 58, 301–316. [Google Scholar] [CrossRef]
- DeVane-Johnson, S.; Woods-Giscombé, C.; Thoyre, S.; Fogel, C.; Williams, R. Integrative literature review of factors related to breastfeeding in African American women: Evidence for a potential paradigm shift. J. Hum. Lact. 2017, 33, 435–447. [Google Scholar] [CrossRef]
- Jones, K.M.; Power, M.L.; Queenan, J.T.; Schulkin, J. Racial and ethnic disparities in breastfeeding. Breastfeed. Med. 2015, 10, 186–196. [Google Scholar] [CrossRef]
- Reeves, E.A.; Woods-Giscombé, C. Infant-feeding practices among African American women: Social-ecological analysis and implications for practice. J. Transcult. Nurs. 2015, 26, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.M.; Kirk, R.; Muzik, M. Overcoming workplace barriers: A focus group study exploring African American mothers’ needs for workplace breastfeeding support. J. Hum. Lact. 2015, 31, 425–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spencer, B.S.; Grassley, J.S. African American women and breastfeeding: An integrative literature review. Health Care Women Int. 2013, 34, 607–625. [Google Scholar] [CrossRef] [PubMed]
- Satcher, D.S. DHHS blueprint for action on breastfeeding. Public Health Rep. 2001, 116, 72–73. [Google Scholar] [CrossRef] [Green Version]
- Gallo, S.; Kogan, K.; Kitsantas, P. Racial and ethnic differences in reasons for breastfeeding cessation among women participating in the special supplemental nutrition program for women, infants, and children. J. Midwifery Women’s Health 2019, 64, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Shipp, G.M.; Weatherspoon, L.J.; Norman, G.S.; Alexander, G.L.; Kelleher, D.; Kerver, J.M. Understanding Factors Influencing Breastfeeding Outcomes in a Sample of African American Women. Matern. Child Health J. 2021, 26, 853–862. [Google Scholar] [CrossRef]
- Hinson, T.D.; Skinner, A.C.; Lich, K.H.; Spatz, D.L. Factors that influence breastfeeding initiation among African American women. J. Obstet. Gynecol. Neonatal Nurs. 2018, 47, 290–300. [Google Scholar] [CrossRef]
- Johnson, A.M.; Kirk, R.; Rooks, A.J.; Muzik, M. Enhancing breastfeeding through healthcare support: Results from a focus group study of African American mothers. Matern. Child Health J. 2016, 20, 92–102. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Ten steps to successful breastfeeding. 2020. Available online: https://www.who.int/activities/promoting-baby-friendly-hospitals/ten-steps-to-successful-breastfeeding (accessed on 1 June 2021).
- Ware, J.L.; Love, D.; Ladipo, J.; Paddy, K.; Starr, M.; Gilliam, J.; Miles, N.; Leatherwood, S.; Reese, L.; Baker, T. African American breastfeeding peer support: All moms empowered to nurse. Breastfeed. Med. 2021, 16, 156–164. [Google Scholar] [CrossRef]
- World Health Organization. Member States Consultation on the Draft Regional Action Framework on Protecting Children from the Harmful Impact of Food Marketing: 2020–2030, Manila, Philippines, 26–28 March 2019: Meeting Report; WHO Regional Office for the Western Pacific: Manila, Philippines, 2019. [Google Scholar]
- Orchard, L.J.; Nicholls, W. A systematic review exploring the impact of social media on breastfeeding practices. Curr. Psychol. 2022, 41, 6107–6123. [Google Scholar] [CrossRef]
- Kornides, M.; Kitsantas, P. Evaluation of breastfeeding promotion, support, and knowledge of benefits on breastfeeding outcomes. J. Child Health Care 2013, 17, 264–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, A.; Davis, M.; Hall, J.; Lauckner, L.; Anderson, A.K. It takes an e-village: Supporting African American mothers in sustaining breastfeeding through Facebook communities. J. Hum. Lact. 2019, 35, 569–582. [Google Scholar] [CrossRef] [PubMed]
- Thomson, J.L.; Tussing-Humphreys, L.M.; Goodman, M.H.; Landry, A.S.; Olender, S.E. Low rate of initiation and short duration of breastfeeding in maternal and infant home visiting project targeting rural, Southern, African American women. Int. Breastfeed. J. 2017, 12, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Mississippi Public Health Institute. Healthy Food Access, Tobacco Use Norms, and Breastfeeding Support a Baseline Assessment of Racial Differences on the Mississippi Gulf Coast. 2019. Available online: https://sheahealth.org/wp-content/uploads/2020/08/MSPHI-Social-Climate-Survey-082120.pdf (accessed on 1 June 2021).
- National Network of Public Health Institutes. Mississippi Public Health Institute. 2019. Available online: https://nnphi.org/member/mississippi-public-health-institute/ (accessed on 1 June 2021).
- REACH. Centers for Disease Control and Prevention Racial and Ethnic Approaches to Community Health Program. 2020. Available online: www.cdc.gov/chronicdisease/resources/publications/factsheets/reach.htm (accessed on 1 June 2021).
- Gulf Coast Community Exchange. Gulf Coast Healthy Communities Collaborative. 2020. Available online: http://www.gulfcoastcommunityexchange.org/ (accessed on 1 June 2021).
- Mississippi Public Health Institute. Gulf Coast Healthy Families, Mothers, and Babies Initiative. 2019. Available online: http://msphi.org/wp-content/uploads/2019/04/MSPHI-Reach-One-Pager-040519.pdf (accessed on 1 June 2021).
- U.S. Census Bureau. QuickFacts: Jackson County, Mississippi; Hancock County, Mississippi; Harrison County, Mississippi; Mississippi. 2021. Available online: https://www.census.gov/quickfacts/fact/table/harrisoncountymississippi,MS/IPE120221#IPE120221 (accessed on 1 June 2021).
- Wang, S.; Guendelman, S.; Harley, K.; Eskenazi, B. When fathers are perceived to share in the maternal decision to breastfeed: Outcomes from the infant feeding practices study II. Matern. Child Health J. 2018, 22, 1676–1684. [Google Scholar] [CrossRef] [PubMed]
- Whipps, M.D.; Demirci, J.R. The sleeper effect of perceived insufficient milk supply in US mothers. Public Health Nutr. 2021, 24, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Government Accountability Office. Breastfeeding some strategies used to market infant formula may discourage breastfeeding. In State Contracts Should Better Protect against Misuse of WIC Name: Report to Congressional Addressees; Diane Publishing: Darby, PA, USA, 2006. [Google Scholar]
- Schindler-Ruwisch, J.; Roess, A.; Robert, R.C.; Napolitano, M.; Woody, E.; Thompson, P.; Ilakkuvan, V. Determinants of Breastfeeding Initiation and Duration Among African American DC WIC Recipients: Perspectives of Recent Mothers. Women’s Health Issues 2019, 29, 513–521. [Google Scholar] [CrossRef] [Green Version]
- Chimoriya, R.; Scott, J.A.; John, J.R.; Bhole, S.; Hayen, A.; Kolt, G.S.; Arora, A. Determinants of Full Breastfeeding at 6 Months and Any Breastfeeding at 12 and 24 Months among Women in Sydney: Findings from the HSHK Birth Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 5384. [Google Scholar] [CrossRef]
- Ajami, M.; Abdollahi, M.; Salehi, F.; Oldewage-Theron, W.; Jamshidi-Naeini, Y. The Association between Household Socioeconomic Status, Breastfeeding, and Infants’ Anthropometric Indices. Int. J. Prev. Med. 2018, 9, 89. [Google Scholar] [CrossRef]
- Amir, L.H.; Donath, S. A systematic review of maternal obesity and breastfeeding intention, initiation and duration. BMC Pregnancy Childbirth 2007, 7, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Niles, P.M.; Asiodu, I.V.; Crear-Perry, J.; Julian, Z.; Lyndon, A.; McLemore, M.R.; Planey, A.M.; Scott, K.A.; Vedam, S. Reflecting on equity in perinatal care during a pandemic. Health Equity 2020, 4, 330–333. [Google Scholar] [CrossRef]
- Ray, R.; Rojas, F. Inequality during the coronavirus pandemic. Contexts (blog). Available online: https://contexts.org/blog/inequality-during-the-coronavirus-pandemic/ (accessed on 16 April 2021).



{kind=link}
{kind=link}
| White | African American | Other Race | |||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Statistical Significance (p-Value) | |
| Exposure to Breastfeeding Promotion (index) | 2.5 | 2.4 | 3.7 | 2.7 | 2.8 | 2.6 | <0.001 |
| Prevalence of Breastfeeding in Primary Social Networks | 3.9 | 1.5 | 3.0 | 1.6 | 4.0 | 1.7 | <0.001 |
| Race a | - | - | - | - | - | - | - |
| White (reference) | 223.8 | 53.4 | - | - | - | - | - |
| African American | - | - | 173.0 | 41.3 | - | - | - |
| Other Races | - | - | - | - | 22.0 | 5.3 | - |
| Employment Status a | - | - | - | - | 0.025 | ||
| Yes | 127.6 | 57.0 | 121.0 | 69.9 | 12.2 | 55.5 | - |
| No (reference) | 96.2 | 42.9 | 51.8 | 29.9 | 10.2 | 46.4 | - |
| Education (grade attended) | 4.5 | 1.5 | 4.3 | 1.4 | 4.1 | 1.4 | 0.483 |
| Household Income (dollars) | 6.4 | 2.6 | 4.9 | 3.0 | 5.1 | 2.2 | - |
| Gender a | - | - | - | - | - | - | 0.005 |
| Male (reference) | 102.6 | 45.8 | 52.2 | 30.2 | 9.2 | 41.8 | - |
| Female | 121.2 | 54.1 | 120.6 | 69.7 | 13.2 | 60.0 | - |
| Age (years) | 48.5 | 16.9 | 37.1 | 11.7 | 33.2 | 14.9 | <0.001 |
| Income | N | % |
|---|---|---|
| Less than $10,000 | 26 | 6.2 |
| $10,000 to under $15,000 | 25 | 6.0 |
| $15,000 to under $20,000 | 33 | 7.9 |
| $20,000 to under $25,000 | 22 | 5.3 |
| $25,000 to under $35,000 | 40 | 9.5 |
| $35,000 to under $50,000 | 49 | 11.7 |
| $50,000 to under $75,000 | 47 | 11.2 |
| $75,000 to under $100,000 | 38 | 9.1 |
| $100,000 to under $150,000 | 36 | 8.6 |
| $150,000 to under $200,000 | 11 | 2.6 |
| $200,000 or more | 13 | 3.1 |
| Total | 340 | 81.1 |
| B | SE B | p-Value | |
|---|---|---|---|
| Model | |||
| Constant | 1.100 | 0.241 | <0.001 |
| African American | 0.276 | 0.103 | 0.007 |
| Other Race | 0.032 | 0.214 | 0.881 |
| Employed | 0.149 | 0.101 | 0.139 |
| Education | −0.039 | 0.036 | 0.277 |
| Household Income | 0.008 | 0.026 | 0.768 |
| Female | 0.390 | 0.100 | <0.001 |
| Age | −0.008 | 0.003 | 0.016 |
| Likelihood Ratio Chi-square | 41.627 | <0.001 |
| B | SE B | p-Value | β | |
|---|---|---|---|---|
| Model | ||||
| African American | −1.010 | 0.199 | <0.001 | −0.311 |
| Other Race | 0.070 | 0.364 | 0.845 | 0.010 |
| Employed | 0.453 | 0.193 | 0.058 | 0.137 |
| Education | 0.104 | 0.062 | 0.083 | 0.094 |
| Household Income | 0.003 | 0.049 | 0.644 | 0.005 |
| Female | 0.104 | 0.173 | 0.407 | 0.032 |
| Age | 0.000 | 0.006 | 0.902 | −0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartkowski, J.P.; Kohler, J.; Xu, X.; Collins, T.; Roach, J.B.; Newkirk, C.; Klee, K. Racial Differences in Breastfeeding on the Mississippi Gulf Coast: Making Sense of a Promotion-Prevalence Paradox with Cross-Sectional Data. Healthcare 2022, 10, 2444. https://doi.org/10.3390/healthcare10122444
Bartkowski JP, Kohler J, Xu X, Collins T, Roach JB, Newkirk C, Klee K. Racial Differences in Breastfeeding on the Mississippi Gulf Coast: Making Sense of a Promotion-Prevalence Paradox with Cross-Sectional Data. Healthcare. 2022; 10(12):2444. https://doi.org/10.3390/healthcare10122444
Chicago/Turabian StyleBartkowski, John P., Janelle Kohler, Xiaohe Xu, Tennille Collins, Jacinda B. Roach, Caroline Newkirk, and Katherine Klee. 2022. "Racial Differences in Breastfeeding on the Mississippi Gulf Coast: Making Sense of a Promotion-Prevalence Paradox with Cross-Sectional Data" Healthcare 10, no. 12: 2444. https://doi.org/10.3390/healthcare10122444
APA StyleBartkowski, J. P., Kohler, J., Xu, X., Collins, T., Roach, J. B., Newkirk, C., & Klee, K. (2022). Racial Differences in Breastfeeding on the Mississippi Gulf Coast: Making Sense of a Promotion-Prevalence Paradox with Cross-Sectional Data. Healthcare, 10(12), 2444. https://doi.org/10.3390/healthcare10122444