1. Introduction
Diabetes mellitus is a chronic disease which has emerged as a significant public health challenge worldwide, both in developed and emerging countries [
1]. In 2015, 415 million people were estimated to be living with Diabetes (8.8% worldwide). The has data doubled in the instance of those with Diabetes since 2000 (4.6%, 151 million people), which is an estimated increase to 10.4% (642 million) by 2040 [
2]. Furthermore, in 2019, this disease was the ninth leading cause of death, responsible for 1.5 million deaths, 48% in people under 70. Between 2000 and 2016, premature mortality due to Diabetes increased by 5% [
3]. As a result, Diabetes was considered a major socio-economic burden for many countries [
4]. In Spain, the total annual direct cost of Diabetes amounts to EUR 5809 million, 8.2% of the total healthcare expenditure; pharmacological costs exerted the greatest influence on the total direct cost (38%) with EUR 2232 million per year [
5]. Moreover, Diabetes has become a major cause of cardiovascular disease, non-traumatic lower limb amputations, blindness, kidney failure and death worldwide [
6]. Furthermore, an association between Diabetes and cancer has been demonstrated, with Diabetes considered a risk factor for cancer in all locations, with a stronger impact on men than women [
7].
There is a significant number of people with Diabetes undiagnosed. In Europe, 37.9% of individuals belong to this group, which could mean that around 22 million individuals with an increased risk of developing cardiovascular disease are unaware of their condition [
8]. In Spain, it was found that almost half of the cases detected were undiagnosed [
9]. Although there are several types of Diabetes, Diabetes mellitus types 1 (DM1) and 2 (DM2) are the most common [
10]. DM1 is associated with deficits in insulin production and requires daily administration of insulin [
11], while DM2 results from a decrease in insulin production due to insulin resistance. Symptoms are similar in both types of Diabetes (thirst, excessive excretion of urine, constant hunger, visual disturbances, etc.), but are less intense in DM2 [
12]. Between 5–10% of cases have DM1, while the remaining 90–95% have DM2 which can be controllable and/or improved by physical activity and healthy lifestyle promotion [
13].
Non-pharmacological interventions such as physical activity (PA) performance and a healthy diet are considered promising methods in the prevention and control of this disease, reducing the socio-economic cost associated with its treatment [
10]. Exercise improves blood glucose control in DM2, influences weight loss, reduces cardiovascular risk factors and improves well-being [
14,
15]. Performing regular exercise can prevent or delay the development of the disease [
16] and, in the case of DM1, lead to improvements in insulin sensitivity, muscle strength and cardiovascular fitness [
17]. In terms of types of exercise training, moderate/high-volume aerobic is associated with lower cardiovascular and mortality risks in both types of Diabetes [
18]. Thus, regular PA increases cardiorespiratory fitness, reduces insulin resistance, and improves lipid levels, and endothelial function [
19], while DM2 decreases A1C, blood pressure, insulin resistance and serum triglycerides [
20]. Resistance exercise reports positive effects in reducing the exercise-induced hypoglycemia risk in DM1 [
21], producing improvements in glycemic control, insulin resistance, strength, and BMI, and reducing blood pressure [
22]. Nevertheless, current evidence shows that PA and diet adherence in diabetic patients is still lower than adherence to medication [
16].
Therefore, this research aims (1) to explore Diabetes prevalence and Diabetes medication use related to sex, age group, Physical Activity Level (PAL) and Body Mass Index (BMI); (2) to study potential differences in the proportions of Diabetes prevalence and Diabetes medication use by the Physical Activity Level (PAL) according to sex, age and Body Mass Index (BMI); and (3) to estimate the Diabetes and Diabetes medication use risk probability risks in the population according to their Physical Activity Level (PAL).
3. Results
Table 1 shows the associations between Diabetes prevalence and sex, age group, PAL, and BMI (
p < 0.001). There were more diabetic men than women (6.8% vs. 4.7%,
p < 0.05). The Diabetes prevalence increased with age, being 0.6% in those under 34, and 18.3% in the 65–69 age group, with differences between all group proportions (
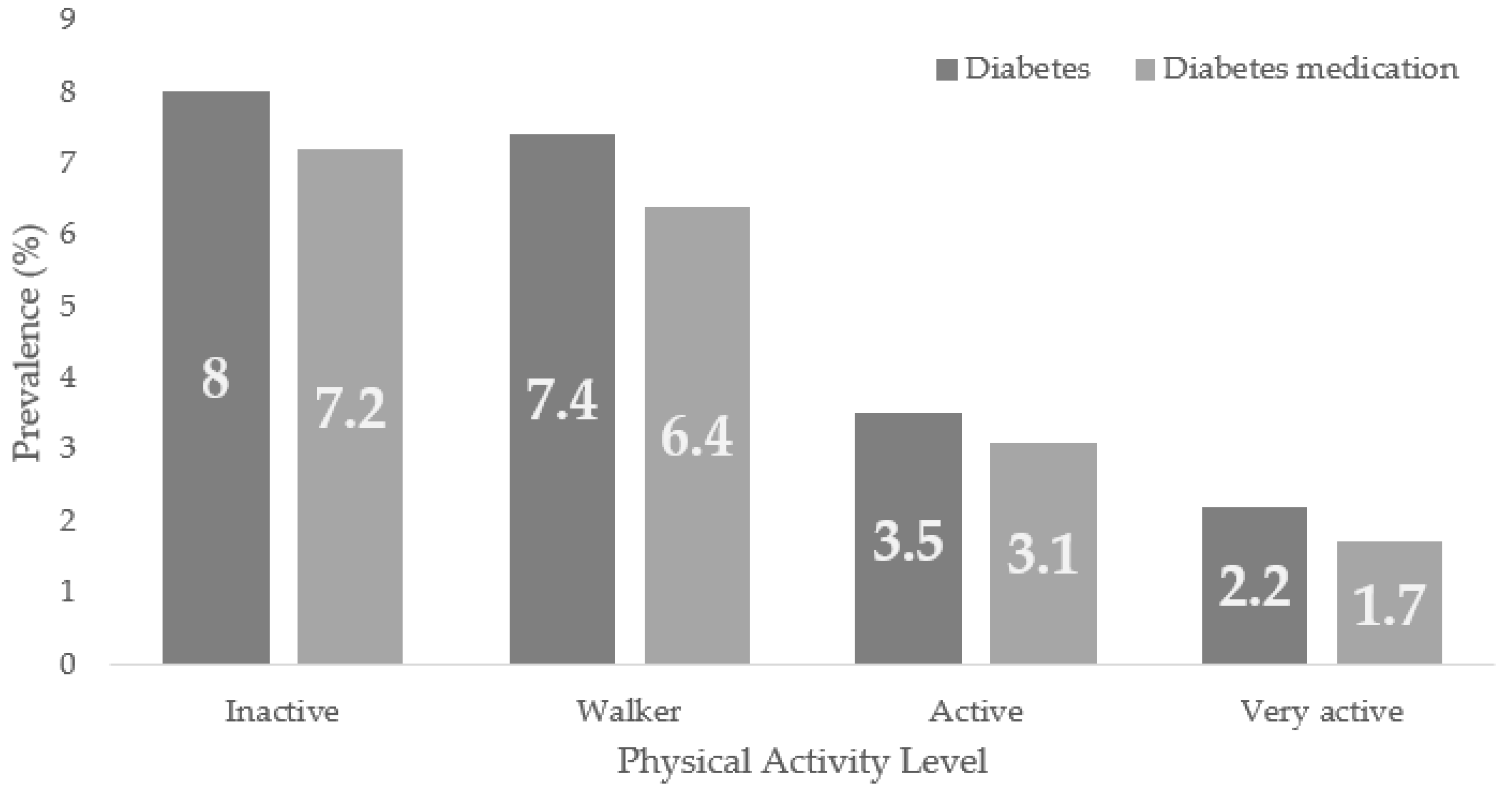
p < 0.05). According to the PAL, the highest prevalence was found in the inactive and walker groups (8.0% and 7.4%) with no significant differences between them, decreasing to 2.2% in the very active group,
p < 0.05. Diabetes was found in 0.5% of underweight people compared to 6.6% in overweight and 13.6% with obesity, with differences in the proportions in these groups (
p < 0.05) and between them (
p < 0.05).
Same dependency relationships were found between Diabetes medication use and sex, age, PAL and BMI (
p < 0.001). Again, men showed higher Diabetes medication use than women (6.2% vs. 3.9%,
p < 0.05). The under-35-year-olds had the lowest prevalence among the age groups (0.4%), with the 65–69-year-old group having the highest (16.3%),
p < 0.05. Similarly, the inactive and very active groups had the highest and lowest prevalence according to PAL (7.2% vs. 1.7%,
p < 0.05), while people with obesity (12.3%) had the highest among the BMI groups (
Table 2).
Figure 2 shows Diabetes and the prevalence of Diabetes medication use according to the PAL in the general population, being, in both cases, higher in the inactive group, with trends to lower prevalence as the population presents higher PAL.
Table 3 displays the Diabetes prevalence related to PAL in men and women from 50–64 years normal and overweight (
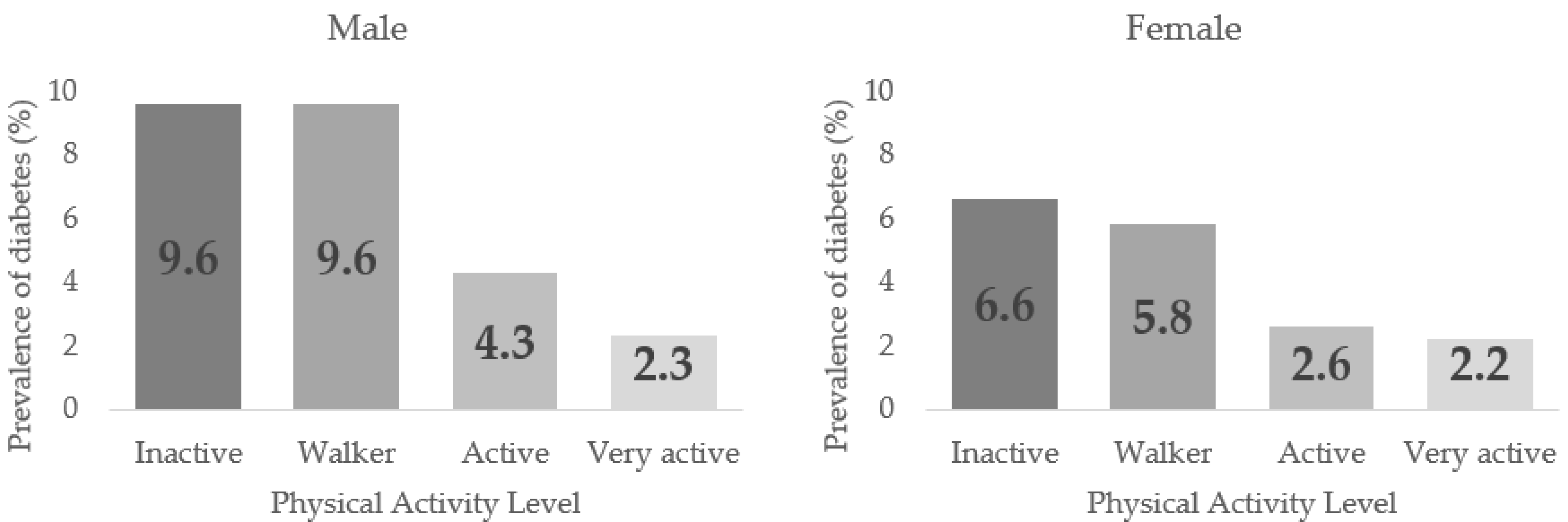
p < 0.001). In all cases, the highest prevalence was found in the Inactive group. A decreasing trend in the Diabetes prevalence could be discerned as higher PAL was in sex, age, and BMI groups, but with no significant differences between the PALs. In men, the highest prevalence were found in inactive and walker (9.6%) groups with no differences between them. In contrast, the active (4.3%) and very active (2.3%) groups showed differences in proportions regarding the previous groups and with each other,
p < 0.05. In females, the inactive and walker groups (6.6% and 5.8%) also had the highest Diabetes prevalence, with no significant differences between them, while there were significant differences between the active and very actives (2.6% and 2.2%),
p < 0.05.
Figure 3 shows the Diabetes prevalence in males and females according to the PAL.
Table 4 shows the associations between PAL and Diabetes prevalence by sex, age, and BMI groups. Significant dependence relationships were found between these variables in men, women, adults between 35–49, and in normal and overweight,
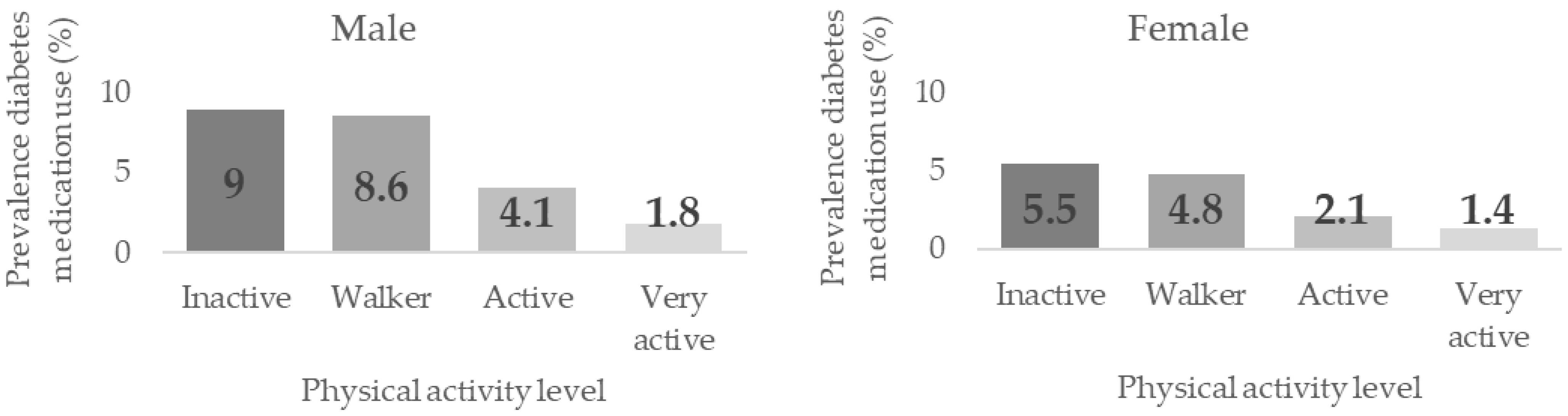
p < 0.001. Prevalence were higher the lower the PAL, although no differences were found between the groups. Significant differences were found in women between the inactive/walker groups (5.5% and 4.8%, respectively) and the active/very active groups (2.1% and 1.4%) prevalence,
p < 0.05. The same significant differences were found in men between the inactive/walker (9.0% and 8.6%), the active (4.1%) and the very active (1.8%) groups (
p < 0.05), with significant differences also found between the latter two groups.
Figure 4 shows the Diabetes medication use prevalence according to the Physical Activity Level (PAL) in men and women.
Table 5 shows the Diabetes risk according to the PAL based on the inactive group. Significantly reduced risks were found in the active and very active groups compared to the inactive group in the general population, in both sexes, in the 35–49 and 50–64 years groups, and most BMI groups.
The Diabetes medication use risk was similarly reduced in the active and very active groups compared to the inactive ones (
Table 6).
According to the binary multiple regression analysis on the Diabetes status and Diabetes medication use, older, male, inactive and obese people showed increased Diabetes and Diabetes medication use risks. These models explained 20.5% and 21.4% of the variance (Nagelkerke R
2) in the Diabetes status and Diabetes medication use, respectively (
Table 7).
4. Discussion
This study found associations between Diabetes prevalence and sex, with men having a higher prevalence than women, whose differences in proportions were statistically significant. One study carried out in the general population was in the same line, with a higher Diabetes prevalence in men than in women and increased prevalence in older people [
30]. Similar results were found in the north-western European population, where the Diabetes mean prevalence was 5.9% for women and 7.9% for men [
31]. In the study carried out by Aregbesola et al., a 61% higher risk in men rather than in women was found [
32]. This higher prevalence in men could be justified by a higher accumulation of body iron in men and a limited capacity for subcutaneous fat expansion in men [
33], so males would accumulate more fat in visceral (liver, spleen, and pancreas) and skeletal muscles, generating greater oxidation of the accumulated fats, leading to increased insulin resistance and glucose homeostasis disturbance [
34,
35]. Dependent relationships were also found between Diabetes prevalence and age groups. Diabetes prevalence increased with increasing age, with the highest prevalence (18.3%) in the older age group (65–69 years). The study performed by Bullard in the USA population, based on data from the 2016 National Health Interview Survey (NHIS) showed that DM2 prevalence increased progressively in the older age group; the highest prevalence was found among adults over 65 years and older [
36].
Diabetes percentage was higher in the BMI groups, with the lowest percentage (0.5%) of diabetic patients in the underweight group and the highest percentage (13.6%) in the obesity group. These data were consistent with those of Zhao with the same group classification. However, percentages were established within the Diabetes group, with 0.54% in the low weight group and 61.94% in the obesity group [
37]. The research conducted by Glovaci with adults with BMI above 40 kg/m
2 showed a higher risk (OR = 7.37, 95 % CI: 6.39–8.5) of Diabetes diagnosis than those with a BMI within the normal range [
38]. Obesity may be one of the most important predictors of DM2 as excess body fat and unfavourable body fat distribution lead to a state of chronic inflammation and insulin resistance, as well as impaired insulin secretion [
39]. The most sedentary individuals had higher BMI, waist circumference, and increased systolic blood pressure was found [
40]. Among the individuals with DM1, the active group had a lower BMI with a low obesity prevalence, a lower fat mass index and a lower waist circumference [
41]. Our study obtained that Diabetes prevalence in obese subjects (BMI ≥ 30) was lower in the groups with higher PAL (Active 10.7 % and Very Active 6.5%) than in those with lower PAL (Inactive 15.2%), being these differences between proportions were significant. Therefore, there could be a strong association between sedentary behaviours (lower PAL) and higher BMI in diabetic and non-diabetic patients. Among the most sedentary individuals, generally, a higher BMI, waist circumference, and increased systolic blood pressure were found [
42]. In individuals with DM1, the active group had lower BMI with a low obesity prevalence, lower fat mass index and a lower waist circumference [
43]. The Diabetes prevalence in our study in Obese subjects (BMI ≥ 30) was lower in the groups with higher PAL (active 10.7% and very active 6.5%) than in those with lower PAL (inactive 15.2%), with these differences being significant proportions [
42]. Therefore, there could be a strong association between sedentary behaviours (lower PAL) and higher BMI in both diabetic and non-diabetic individuals [
42,
43].
The highest Diabetes prevalence were found in the participants with the lowest PAL (inactive and walking groups) and the lowest in those with the highest PAL (active and very active groups). In this line, Colak used the IPAQ-SF Questionnaire [
44] to assess PA and found that in 129 patients with DM2, 39.5% were Inactive and only 8.5% showed high PAL [
45]. Oguntibeju found [
46] reduced Diabetes risks in the active and very active groups compared to the inactive group in the general population, in both sexes, in the age groups 35–49 and 50–64 years, and most BMI groups. Other research has shown this inverse relationship between PA and Diabetes risk [
47,
48,
49,
50]. However, these studies used different instruments to assess PA (quantitatively, qualitatively, or mixed), measured different domains (occupational PA, leisure time PA, etc.) and dimensions (type of PA, intensity, duration, etc.), which could be problematic in making comparisons [
51,
52].
Diabetes medication use prevalence were higher in subjects with lower PAL, with prevalence decreasing the higher the PAL. In this regard, another study showed an association between a daily dose of vigorous exercise and lower odds of Diabetes medication use [
53]. These findings were in line with those of the current study: the higher the PAL, the lower the medication prevalence. Therefore, diabetic individuals taking more medication have more severe symptoms of the disease and, consequently, experience greater challenges or barriers to physical activity or even prevent physical activity, possibly related to the adverse effects of the medication itself.
The importance of this study lies in the analysis of the associations between the physical activity level and Diabetes prevalence and Diabetes medication use in the Spanish population during the last period before the COVID-19 pandemic, serving as a frame of reference for future research examining post-pandemic periods, as the ENSE is addressed every 5 years. This research showed the relationship between PAL and Diabetes. Hence, introducing exercise programs in Diabetes could be considered as a potential tool for its benefits on patients’ health such as improvements in glucose metabolism and insulin sensitivity [
54], though this should be confirmed by studies that allow cause-effect relationships to be established.
This study has some limitations. On the one hand, a cross-sectional design does not allow for establishing cause–effect relations. Thus, further research using designs which allow causal relations to be established would be advisable. This work was based on self-reported Diabetes without any medical history or medical judgement. Additionally, this study lacked data on the type of Diabetes, which could influence the results. In future research, it would be interesting to use means of collecting objective data for Diabetes diagnosis. Moreover, additional sociocultural, socio-demographic, and socio-economic variables that could influence the results of Diabetes prevalence were also not considered [
55,
56,
57].

 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}