
Relationship between Smartphone Addiction and Sleep Satisfaction: A Cross-Sectional Study on Korean Adolescents


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Subjects and Data Collection Methods
2.2. Questionnaire Content and Variable Definition
2.2.1. Independent Variables
2.2.2. Dependent Variable
2.2.3. Confounding Variables
2.3. Statistical Analysis
3. Results
3.1. General Characteristics of Survey Subjects and Results of Chi-Squared Test
3.2. Relationship between Smartphone Addiction and Sleep Satisfaction
3.3. Relationship between Smartphone Usage Time and Sleep Satisfaction
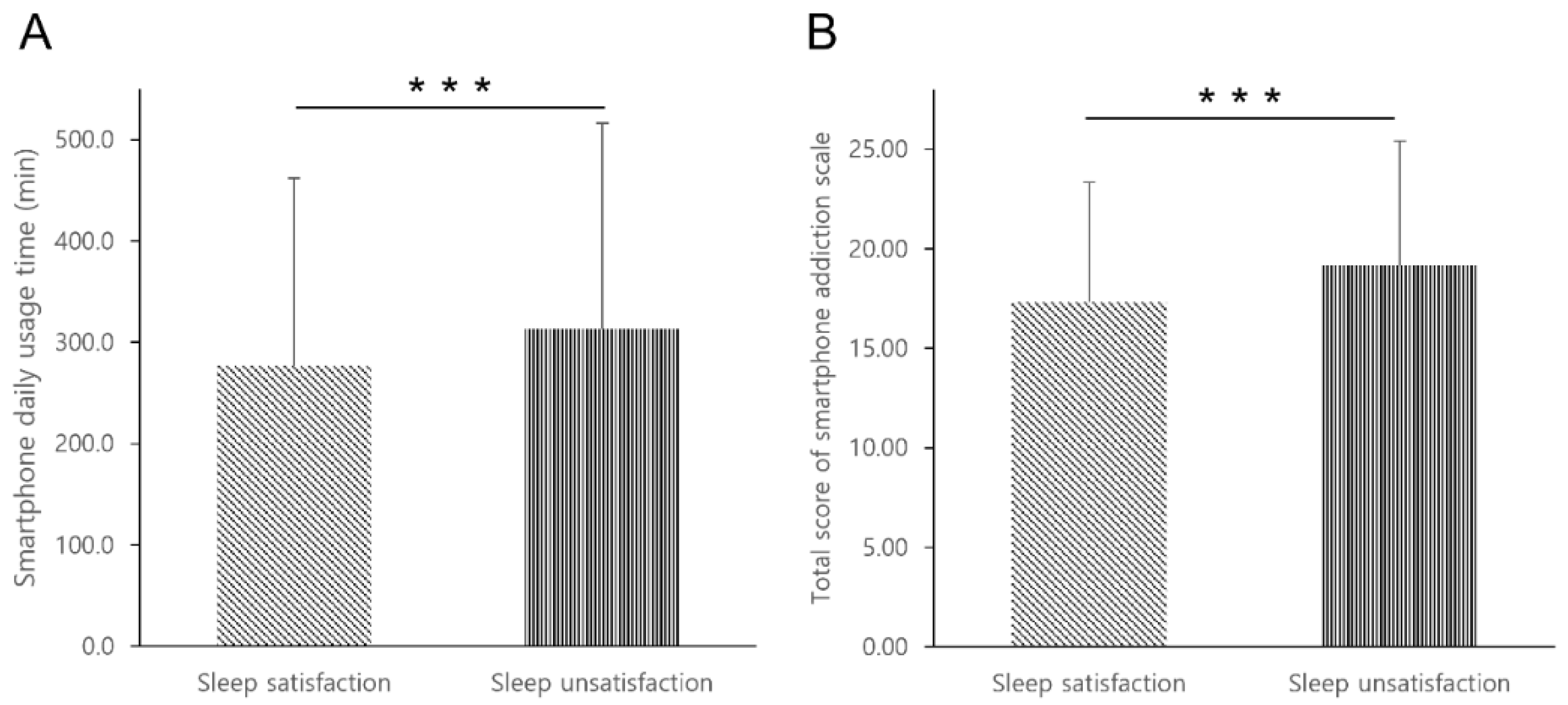
3.4. Differences in Daily Average Smartphone Usage Time and Smartphone Addiction According to Sleep Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cirelli, C. Sleep disruption, oxidative stress, and aging: New insights from fruit flies. Proc. Natl. Acad. Sci. USA 2006, 103, 13901–13902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhola, P.; Polo-Kantola, P. Sleep deprivation: Impact on cognitive performance. Neuropsychiatr. Dis. Treat. 2007, 3, 553–567. [Google Scholar] [PubMed]
- Korea Disease Control and Prevention Agency. 2020 Reports on the Korea Youth Risk Behavior Web-Based Survey. Available online: https://www.kdca.co.kr/yhs/ (accessed on 31 May 2022).
- Paruthi, S.; Brooks, L.J.; D’Ambrosio, C.; Hall, W.; Kotagal, S.; Lloyd, R.M.; Malow, B.A.; Maski, K.; Nichols, C.; Quan, S.F.; et al. Consensus Statement of the American Academy of Sleep Medicine on the Recommended Amount of Sleep for Healthy Children: Methodology and Discussion. J. Clin. Sleep Med. 2016, 12, 1549–1561. [Google Scholar] [CrossRef] [PubMed]
- Banks, S.; Dinges, D.F. Behavioral and Physiological Consequences of Sleep Restriction. J. Clin. Sleep Med. 2007, 3, 519–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taheri, S. The link between short sleep duration and obesity: We should recommend more sleep to prevent obesity. Arch. Dis. Child. 2006, 91, 881–884. [Google Scholar] [CrossRef] [Green Version]
- Mrug, S.; Tyson, A.; Turan, B.; Granger, D.A. Sleep problems predict cortisol reactivity to stress in urban adolescents. Physiol. Behav. 2016, 155, 95–101. [Google Scholar] [CrossRef]
- Dewald, J.F.; Meijer, A.M.; Oort, F.J.; Kerkhof, G.A.; Bögels, S.M. The influence of sleep quality, sleep duration and sleepiness on school performance in children and adolescents: A meta-analytic review. Sleep Med. Rev. 2010, 14, 179–189. [Google Scholar] [CrossRef]
- Bélanger, M.; Sabiston, C.M.; Barnett, T.A.; O’Loughlin, E.; Ward, S.; Contreras, G.; O’Loughlin, J. Number of years of participation in some, but not all, types of physical activity during adolescence predicts level of physical activity in adulthood: Results from a 13-year study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 76. [Google Scholar] [CrossRef] [Green Version]
- Samaha, M.; Hawi, N.S. Relationships among smartphone addiction, stress, academic performance, and satisfaction with life. Comput. Hum. Behav. 2016, 57, 321–325. [Google Scholar] [CrossRef]
- Ma, Z.; Wang, J.; Li, J.; Jia, Y. The association between obesity and problematic smartphone use among school-age children and adolescents: A cross-sectional study in Shanghai. BMC Public Health 2021, 21, 2067. [Google Scholar] [CrossRef]
- Billieux, J.; Maurage, P.; Lopez-Fernandez, O.; Kuss, D.J.; Griffiths, M.D. Can Disordered Mobile Phone Use Be Considered a Behavioral Addiction? An Update on Current Evidence and a Comprehensive Model for Future Research. Curr. Addict. Rep. 2015, 2, 156–162. [Google Scholar] [CrossRef] [Green Version]
- Islam, M. Link between Excessive Smartphone Use and Sleeping Disorders and Depression among South Korean University Students. Healthcare 2021, 9, 1213. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Science and ICT. 2020 the Survey on Smartphone Overdependence. Available online: https://www.nia.or.kr/site/nia_kor/ex/bbs/View.do?cbIdx=65914&bcIdx=23109&parentSeq=23109 (accessed on 31 May 2022).
- Romer, D. Adolescent risk taking, impulsivity, and brain development: Implications for prevention. Dev. Psychobiol. 2010, 52, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Liu, T.-Q.; Liao, Y.-H.; Qi, C.; He, H.-Y.; Chen, S.-B.; Billieux, J. Prevalence and correlates of problematic smartphone use in a large random sample of Chinese undergraduates. BMC Psychiatry 2016, 16, 408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Science and ICT. 2019 the Survey on Smartphone Overdependence. Available online: https://www.nia.or.kr/site/nia_kor/ex/bbs/View.do?cbIdx=65914&bcIdx=21939&parentSeq=21939 (accessed on 31 May 2022).
- Lepp, A.; Barkley, J.E.; Sanders, G.J.; Rebold, M.; Gates, P. The relationship between cell phone use, physical and sedentary activity, and cardiorespiratory fitness in a sample of U.S. college students. Int. J. Behav. Nutr. Phys. Act. 2013, 21, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alaca, N. The impact of internet addiction on depression, physical activity level and trigger point sensitivity in Turkish uni-versity students. J. Back Musculoskelet. Rehabil. 2020, 33, 623–630. [Google Scholar] [CrossRef]
- Boulos, M.N.K.; Wheeler, S.; Tavares, C.; Jones, R. How smartphones are changing the face of mobile and participatory healthcare: An overview, with example from eCAALYX. Biomed. Eng. Online 2011, 10, 24. [Google Scholar] [CrossRef] [Green Version]
- Sohn, S.Y.; Krasnoff, L.; Rees, P.; Kalk, N.J.; Carter, B. The Association Between Smartphone Addiction and Sleep: A UK Cross-Sectional Study of Young Adults. Front. Psychiatry 2021, 176, 629407. [Google Scholar] [CrossRef]
- Kim, G.M.; Jeong, M.K.; Kwon, Y.C. The Effect of Daily Smart Phone Usage on Sleep Quality and Sedentary Behavior in Uni-versity Students. Korea J. Sports Sci. 2016, 25, 1515–1522. [Google Scholar]
- Kim, Y.; Choi, S.; Chun, C.; Park, S.; Khang, Y.-H.; Oh, K. Data Resource Profile: The Korea Youth Risk Behavior Web-based Survey (KYRBS). Int. J. Epidemiol. 2016, 45, 1076–1076e. [Google Scholar] [CrossRef] [Green Version]
- Jun, W. A Study on Correlation Analysis of Smart Phone Addiction and Age Groups in Korea. Int. J. Adv. Smart Converg. 2020, 9, 106–114. [Google Scholar]
- Kim, J.; Lee, K. The Association between Physical Activity and Smartphone Addiction in Korean Adolescents: The 16th Korea Youth Risk Behavior Web-Based Survey, 2020. Healthcare 2022, 10, 702. [Google Scholar] [CrossRef] [PubMed]
- Park, S. Associations of physical activity with sleep satisfaction, perceived stress, and problematic Internet use in Korean adolescents. BMC Public Health 2014, 14, 1143. [Google Scholar] [CrossRef] [Green Version]
- Oh, W.O.; Im, Y.; Suk, M.H. The mediating effect of sleep satisfaction on the relationship between stress and perceived health of adolescents suffering atopic disease: Secondary analysis of data from the 2013 9th Korea Youth Risk Behavior Web-based Survey. Int. J. Nurs. Stud. 2016, 63, 132–138. [Google Scholar] [CrossRef]
- Li, S.H.; Graham, B.M.; Werner-Seidler, A. Gender Differences in Adolescent Sleep Disturbance and Treatment Response to Smartphone App–Delivered Cognitive Behavioral Therapy for Insomnia: Exploratory Study. JMIR Form. Res. 2021, 5, e22498. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-K.; Kim, J.K.; Patel, S.R.; Lee, J.-H. Age-Related Changes in Sleep/Wake Patterns Among Korean Teenagers. Pediatrics 2005, 115 (Suppl. S1), 250–256. [Google Scholar] [CrossRef] [PubMed]
- Hartanto, A.; Quek, F.Y.X.; Tng, G.Y.Q.; Yong, J.C. Does Social Media Use Increase Depressive Symptoms? A Reverse Causation Perspective. Front. Psychiatry 2021, 12, 641934. [Google Scholar] [CrossRef]
- Carter, B.; Rees, P.; Hale, L.; Bhattacharjee, D.; Paradkar, M.S. Association between portable screen-based media device access or use and sleep outcomes a systematic review and meta-analysis. JAMA Pediatr. 2016, 170, 1202–1208. [Google Scholar] [CrossRef] [Green Version]
- Alshobaili, F.A.; Alyousefi, N.A. The effect of smartphone usage at bedtime on sleep quality among Saudi non- medical staff at King Saud University Medical City. J. Fam. Med. Prim. Care 2019, 8, 1953. [Google Scholar] [CrossRef]
- Chung, J.E.; Choi, S.A.; Kim, K.T.; Yee, J.; Kim, J.H.; Seong, J.W.; Seong, J.M.; Kim, J.Y.; Lee, K.E.; Gwak, H.S. Smartphone addiction risk and daytime sleepiness in Korean adolescents. J. Paediatr. Child Health 2018, 54, 800–806. [Google Scholar] [CrossRef]
- Kim, S.Y.; Han, S.R.; Park, E.-J.; Yoo, H.-J.; Park, D.S.; Suh, S.; Shin, Y.M. The relationship between smartphone overuse and sleep in younger children: A prospective cohort study. J. Clin. Sleep Med. 2020, 16, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Panova, T.; Carbonell, X. Is smartphone addiction really an addiction? J. Behav. Addict. 2018, 7, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Khouja, J.N.; Munafò, M.R.; Tilling, K.; Wiles, N.J.; Joinson, C.; Etchells, P.J.; John, A.; Hayes, F.M.; Gage, S.H.; Cornish, R.P. Is screen time associated with anxiety or depression in young people? Results from a UK birth cohort. BMC Public Health 2019, 19, 82. [Google Scholar] [CrossRef] [PubMed]
- Kredlow, M.A.; Capozzoli, M.C.; Hearon, B.A.; Calkins, A.W.; Otto, M.W. The effects of physical activity on sleep: A me-ta-analytic review. J. Behav. Med. 2015, 38, 427–449. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.E.; Kim, J.W.; Jee, Y.S. Relationship between smartphone addiction and physical activity in Chinese international stu-dents in Korea. J. Behav. Addict. 2015, 4, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Kline, C.E.; Hillman, C.H.; Sheppard, B.B.; Tennant, B.; Conroy, D.E.; Macko, R.F.; Marquez, D.X.; Petruzzello, S.J.; Powell, K.E.; Erickson, K.I. Physical activity and sleep: An updated umbrella review of the 2018 Physical Activity Guidelines Advisory Committee report. Sleep Med. Rev. 2021, 58, 101489. [Google Scholar] [CrossRef]
- Mochón-Benguigui, S.; Carneiro-Barrera, A.; Castillo, M.J.; Amaro-Gahete, F.J. Role of physical activity and fitness on sleep in sedentary middle-aged adults: The FIT-AGEING study. Sci. Rep. 2021, 11, 539. [Google Scholar] [CrossRef]


{kind=link}
| Factor | Questions |
|---|---|
| Self-Control Failure | ① Every time I try to reduce my smartphone time, it fails ② It is difficult to control the smartphone usage time ③ It is hard to keep proper usage time for smartphones |
| Salience | ④ If a smartphone is next to me, it’s difficult to focus on other tasks. ⑤ Smartphone thoughts do not leave my mind ⑥ I strongly feel the urge to use my smartphone |
| Serious Consequences | ⑦ I have had health problems because of smartphone use ⑧ I had a hard time fighting with my family because of my smartphone ⑨ I have experienced severe conflicts in my friends, colleagues or social relationships because of my smartphone ⑩ I have difficulties in carrying out work (study or job) due to smartphone |
| Total Users (n = 54,948) | x2 (p) | |||
|---|---|---|---|---|
| Sleep Satisfaction (n = 16,824) | Sleep Unsatisfaction (n = 38,124) | Total (n = 54,948) | ||
| Gender | ||||
| Male | 9960 (35.5) | 18,393 (64.5) | 28,353 (100.0) | 594.704 |
| Female | 6864 (25.9) | 19,731 (74.1) | 26,595 (100.0) | <0.001 |
| School grade | ||||
| 7th | 4104 (41.2) | 5901 (58.8) | 10,005 (100.0) | 1042.677 |
| 8th | 3333 (34.6) | 6231 (65.4) | 9564 (100.0) | <0.001 |
| 9th | 2916 (31.1) | 6476 (68.9) | 9392 (100.0) | |
| 10th | 2221 (24.5) | 6686 (75.5) | 8907 (100.0) | |
| 11th | 2317 (25.9) | 6590 (74.1) | 8907 (100.0) | |
| 12th | 1933 (23.7) | 6240 (76.3) | 8173 (100.0) | |
| Stress | ||||
| No | 6112 (51.9) | 5795 (48.1) | 11,907 (100.0) | 3208.805 |
| Yes | 10,712 (24.8) | 32,329 (75.2) | 43,041 (100.0) | <0.001 |
| Depression | ||||
| No | 14,218 (34.7) | 26,890 (65.3) | 41,108 (100.0) | 1231.316 |
| Yes | 2606 (18.8) | 11,234 (81.2) | 13,840 (100.0) | <0.001 |
| Regular physical activity | ||||
| No | 9104 (28.5) | 22,890 (71.5) | 31,994 (100.0) | 179.951 |
| Yes | 7720 (33.8) | 15,234 (66.2) | 22,954 (100.0) | <0.001 |
| Asthma | ||||
| No | 16,679 (30.8) | 37,674 (69.2) | 54,353 (100.0) | 11.642 |
| Yes | 145 (24.3) | 450 (75.7) | 595 (100.0) | <0.001 |
| Allergic rhinitis | ||||
| No | 14,541 (31.6) | 31,452 (68.4) | 45,993 (100.0) | 118.796 |
| Yes | 2283 (25.9) | 6672 (74.1) | 8955 (100.0) | <0.001 |
| Atopic dermatitis | ||||
| No | 15,913 (31.0) | 35,470 (69.0) | 51,383 (100.0) | 39.345 |
| Yes | 911 (26.0) | 2654 (74.0) | 3565 (100.0) | <0.001 |
| Total Users (n = 54,948) | x2 (p) | |||
|---|---|---|---|---|
| Sleep Satisfaction (n = 16,824) | Sleep Unsatisfaction (n = 38,124) | Total (n = 54,948) | ||
| Smartphone addiction | ||||
| Normal user | 13,759 (33.6) | 27,414 (66.4) | 41,173 (100.0) | 645.733 |
| Potential-risk user | 2750 (22.5) | 9392 (77.5) | 12,142 (100.0) | <0.001 |
| High-risk user | 315 (19.2) | 1318 (80.8) | 1633 (100.0) | |
| Smartphone usage time | ||||
| Over 8 h | 2159 (24.4) | 6607 (75.6) | 8766 (100.0) | 440.627 |
| Over 6 h to under 8 h | 2122 (27.2) | 5736 (72.8) | 7858 (100.0) | <0.001 |
| Over 4 h to under 6 h | 4456 (29.6) | 10,593 (70.4) | 15,049 (100.0) | |
| Over 2 h to under 4 h | 5611 (34.0) | 10,994 (66.0) | 16,605 (100.0) | |
| Under 2 h | 2476 (37.5) | 4194 (62.5) | 6670 (100.0) | |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| Smartphone Addiction | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p |
| High-risk user | Reference | - | Reference | - | Reference | - |
| Potential-risk user | 1.220 (1.068–1.394) | 0.003 | 1.028 (0.894–1.181) | 0.701 | 1.016 (0.883–1.168) | 0.828 |
| Normal user | 2.123 (1.871–2.410) | <0.001 | 1.390 (1.216–1.589) | <0.001 | 1.372 (1.199–1.568) | <0.001 |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| Smartphone Usage Time | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p |
| Over 8 h | Reference | - | Reference | - | Reference | - |
| Over 6 h to under 8 h | 1.156 (1.079–1.239) | <0.001 | 1.094 (1.017–1.178) | 0.016 | 1.096 (1.018–1.180) | 0.014 |
| Over 4 h to under 6 h | 1.299 (1.222–1.381) | <0.001 | 1.148 (1.076–1.225) | <0.001 | 1.151 (1.079–1.229) | <0.001 |
| Over 2 h to under 4 h | 1.590 (1.493–1.694) | <0.001 | 1.240 (1.159–1.326) | <0.001 | 1.244 (1.163–1.331) | <0.001 |
| Under 2 h | 1.855 (1.733–1.985) | <0.001 | 1.339 (1.245–1.439) | <0.001 | 1.347 (1.252–1.448) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.; Lee, K. Relationship between Smartphone Addiction and Sleep Satisfaction: A Cross-Sectional Study on Korean Adolescents. Healthcare 2022, 10, 1326. https://doi.org/10.3390/healthcare10071326
Kim E, Lee K. Relationship between Smartphone Addiction and Sleep Satisfaction: A Cross-Sectional Study on Korean Adolescents. Healthcare. 2022; 10(7):1326. https://doi.org/10.3390/healthcare10071326
Chicago/Turabian StyleKim, Eonho, and Kihyuk Lee. 2022. "Relationship between Smartphone Addiction and Sleep Satisfaction: A Cross-Sectional Study on Korean Adolescents" Healthcare 10, no. 7: 1326. https://doi.org/10.3390/healthcare10071326
APA StyleKim, E., & Lee, K. (2022). Relationship between Smartphone Addiction and Sleep Satisfaction: A Cross-Sectional Study on Korean Adolescents. Healthcare, 10(7), 1326. https://doi.org/10.3390/healthcare10071326