
Cross-Cultural Adaptation and Validation of the Functional, Communicative and Critical Health Literacy Instrument (FCCHL-SR) for Diabetic Patients in Serbia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Instrument
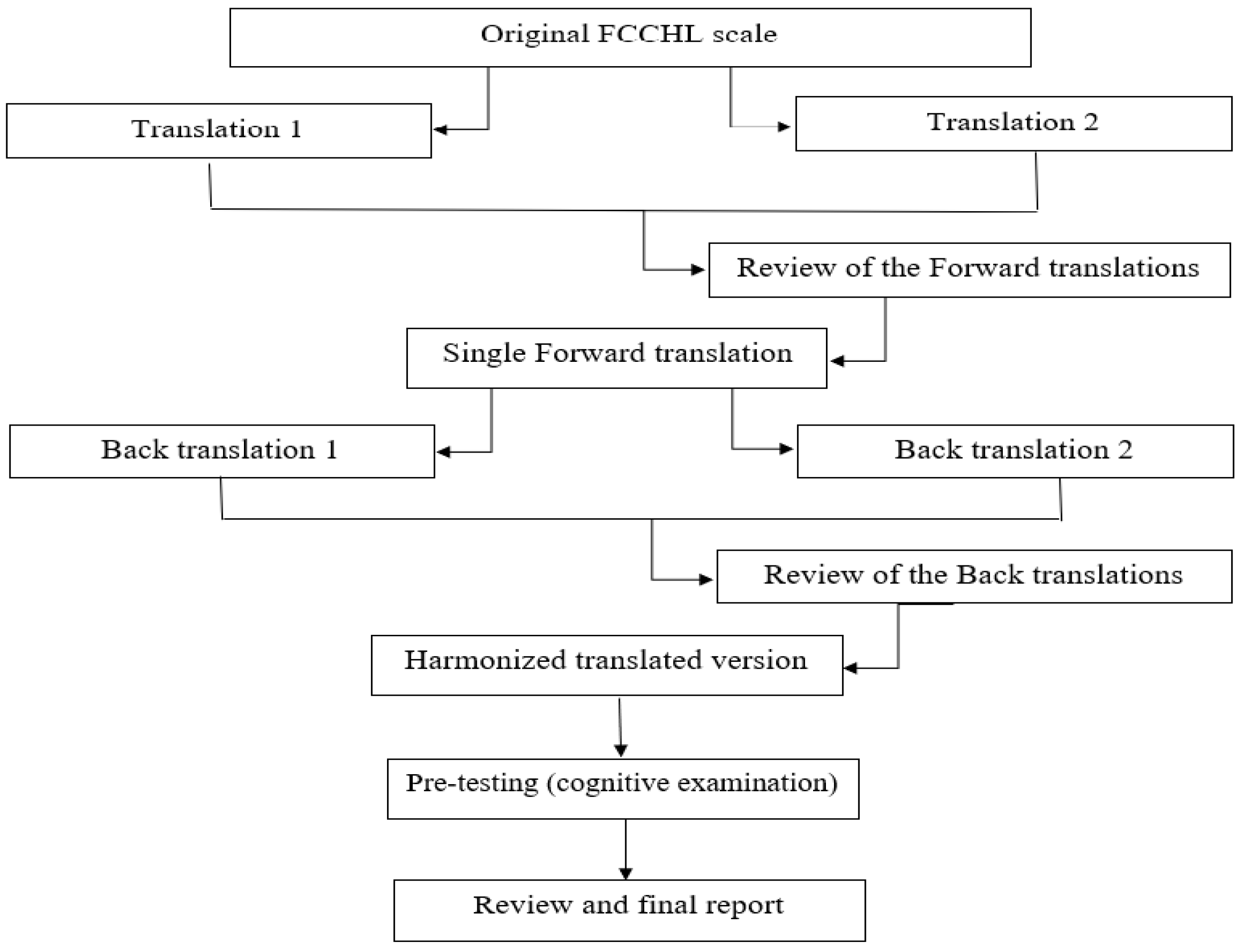
2.2. Translation and Cultural Adaptation
- In preparation for translation, people were selected to do the translation (A1, A2, T3 and T4). The methodology is defined, and the author of the instrument was contacted to gain approval for use of the FCCHL instrument.
- “Forward” translation in our case was the translation of the instrument from the source language (English) into target language (Serbian). This step was performed by two -researches (A1 and A2) whose native language is Serbian, and the other language is the source language of the scale being translated. Both authors were familiar with the concept of the research. They were independent of each other, i.e., all items, answers and instructions were translated separately. When translating, focus was maintained on ensuring that the concept is adequately conveyed and that the wording is clear.
- Single “forward” translation or the formation of a unified version of the translation involved merging these two researches into one (A12) and this was done by a third person from the team and after discussion between the researchers. This version was with a minimum of disagreement and with the clearest questions in translations.
- “Backward” translation was done by translating from target language into the source language. It was conducted by two translators (T3 and T4) who are native speakers of the source language and are fluent in the target language. Both back translators were unfamiliar with the content of the instrument.
- A review of the “backwards” translations considered a comparison of back-translated versions of an instrument with the original to highlight and explore the differences between the original and the aligned translation.
- The harmonization implies a central place in the whole process and involved comparison of both versions of the “backwards” translations, testing the degree of agreement of the concepts of all items, making corrections, controlling language errors, and forming a version for the testing phase.
- The penultimate step in the cultural adaptation process is pre-testing. It is a process in which the final version was introduced into testing on the population for which the instrument was made. Pre-testing was done using the cognitive interviewing technique “probing” with required patients at a health-care institution by a researcher (A1) [29,43]. To gain a better understanding of the cognitive processes the participant used to answer the items thinking aloud, as explicitly instructed. Ten diabetic patients were eligible to fill-in the instrument and discuss it with the interviewer. Interviews were conducted until data saturation was reached; meaning that no more new information of value was obtained. It lasted from 5–6 min.
- In the review process all reports from previous stages were reviewed in detail, the test results were included in the translation and all disagreements were eliminated. The degree of equality between the target version and the original was assessed, and the result of this step is the creation of the final version of the instrument.
- The final report considered a review of the final version of the instrument and submission of reports with all collected documents to the author. The authors evaluated and approved the final version of the FCCHL to be used for the validation study. (Figure 1).
2.3. Quantitative Study
2.4. Sample and Data Collection
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Report of Translation
3.2. Pre-Testing
3.3. Subjects
3.4. Distributional Properties
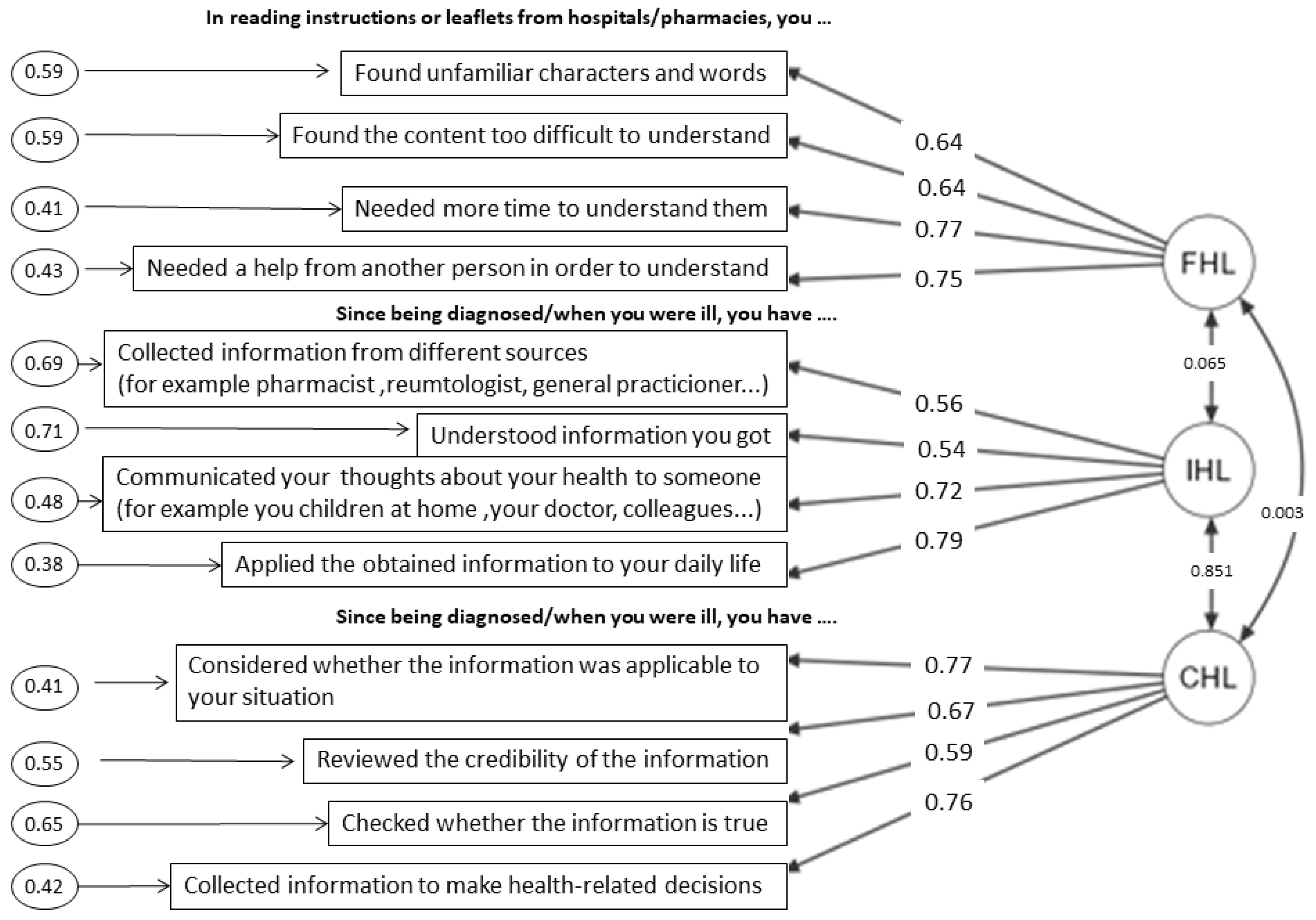
3.5. Structural Validity and Reliability and Suggested Modifications to the FCCHL-SR14
4. Discussion
4.1. Cultural and Linguistic Adaptation of the FCCHL-SR Instrument
4.2. The 12-Item FCCHL-SR
4.3. Methodological Considerations
4.4. Advantages of FCCHL Scale
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Heritage Dictionary, 3rd ed.; Bantam Doubleday Dell Publishing Group, Inc.: New York, NY, USA, 1994.
- Kirsch, I.; Jungeblunt, A.; Jenkins, L.; Koldtad, A. Adult Literacy in America: A First Look at the Findings of the National Adult Literacy Survey; National Center for Education Statistics, U.S. Department of Education: Washington, DC, USA, 1993.
- Simonds, S.K. Health Education as a Social Policy. Health Educ. Monogr. 1974, 2, 1–25. [Google Scholar] [CrossRef]
- Institute of Medicine. Health Literacy: A Prescription to End Confusion; National Academic Press: Washington, DC, USA, 2004. [Google Scholar]
- Kickbush, I.; Pelikan, J.; Apfel, F.; Agis, T. (Eds.) Health Literacy: The Solid Facts, 1st ed.; WHO Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- European Commission. Together for Health. In A Strategic Approach for the EU 2008–2013; COM. 630 Final Brussels; European Commission: Brussels, Belgium, 2007. [Google Scholar]
- World Health Organisation Regional Office for Europe. Health 2020. In A European Policy Framework Supporting Action across Government and Society for Health and Wellbeing; World Health Organisation Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. (HLS-EU) Consortium Health Literacy Project European. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar]
- World Health Organization [WHO]. Health Promotion Glossary; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Kickbusch, I.; Maag, D. Health literacy. In International Encyclopedia of Public Health; Heggenhougen, K., Quah, S., Eds.; Academic Press: San Diego, CA, USA, 2008; pp. 204–211. [Google Scholar]
- Nguyen, T.H.; Paasche-Orlow, M.K.; McCormack, L.A. The State of the Science of Health Literacy Measurement. Stud. Health Technol. Inform. 2017, 240, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Ratzan, S.C.; Parker, R.M. Introduction. In National Library of Medicine Current Bibliographies in Medicine: Health Literacy; Selden, C.R., Zorn, M., Ratzan, S.C., Parker, R.M., Eds.; National Institutes of Health, U.S. Department of Health and Human Services: Bethesda, MD, USA, 2000. [Google Scholar]
- Santana, S.; Brach, C.; Harris, L. Updating Health Literacy for Healthy People 2030: Defining Its Importance for a New Decade in Public Health. J. Public Health Manag. Pract. 2021, 27, 258–264. [Google Scholar] [CrossRef]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E. Health literacy interventions and outcomes: An updated systematic review. Evid. Rep. Technol. Assess Full Rep. 2011, 199, 1–941. [Google Scholar]
- Ozdemir, H.; Alper, Z.; Uncu, Y.; Bilgel, N. Health literacy among adults: A study from Turkey. Health Educ Res. 2010, 25, 464–477. [Google Scholar] [CrossRef] [PubMed]
- Durusu Tanrıöver, M.; Yıldırım, H.H.; Demiray Ready, F.N.; Cakir, B.; Akalin, H.E. Türkïye Sağlık Okuryazarlığı Araştırması [Health Literacy Survey, Turkey], 1st ed.; Sağlık-Sen Yayınları: Ankara, Turkish, 2014. [Google Scholar]
- Sorensen, K.; Pelikan, J.M.; Rothlin, F. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Hardin, L.R. Counseling patients with low health literacy. Am. J. Health Syst. Pharm. 2005, 62, 364–365. [Google Scholar] [CrossRef]
- Nutbeam, D. Defining, measuring and improving health literacy. Health Eval. Promot. 2015, 42, 450–455. [Google Scholar] [CrossRef]
- Van der Vaart, R.; Drossaert, C.H.; Taal, E.; ten Klooster, P.M.; Hilderink-Koertshuis, R.T.; Klaase, J.M.; van de Laar, M.A. Validation of the Dutch functional, communicative and critical health literacy scales. Patient Educ. Couns. 2012, 89, 82–88. [Google Scholar] [CrossRef]
- Levic, M.; Bogavac-Stanojevic, N.; Krajnovic, D. The Instruments Used to Assess Health Literacy and Pharmacotherapy Literacy of Diabetes Mellitus Type 2 Patients: A Scoping Review. Front. Public Health 2021, 9, 1424–1440. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Prom. Inter. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Al Sayah, F.; Williams, B.; Johnson, J.A. Measuring health literacy in individuals with diabetes: A systematic review and evaluation of available measures. Health Educ. Behav. 2013, 40, 42–55. [Google Scholar] [CrossRef]
- Lee, E.-H.; Kim, C.-J.; Lee, J.; Moon, S.H. Self-administered health literacy instruments for people with diabetes: Systematic review of measurement properties. J. Adv. Nurs. 2017, 73, 2035–2048. [Google Scholar] [CrossRef]
- Bailey, S.C.; Brega, A.G.; Crutchfield, T.M.; Elasy, T.; Herr, H.; Kaphingst, K.; Karter, A.J.; Moreland-Russell, S.; Osborn, C.Y.; Pignone, M.; et al. Update on health literacy and diabetes. Diabetes Educ. 2014, 40, 581–604. [Google Scholar] [CrossRef]
- Osborn, C.Y.; Cavanaugh, K.; Wallston, K.A.; Kripalani, S.; Elasy, T.A.; Rothman, R.L.; White, R.O. Health literacy explains racial disparities in diabetes medication adherence. J. Health Commun. 2011, 16, 268–278. [Google Scholar] [CrossRef]
- Barton, J.L.; Trupin, L.; Tonner, C.; Imboden, J.; Katz, P.; Schillinger, D.; Yelin, E. English language proficiency, health literacy, and trust in physician are associated with shared decision making in rheumatoid arthritis. J. Rheumatol. 2014, 41, 1290–1297. [Google Scholar] [CrossRef]
- Marais, I.; Andrich, D. Effects of varying magnitude and patterns of response dependence in the unidimensional Rasch model. J. Appl. Meas. 2008, 9, 105–124. [Google Scholar]
- Altin, S.V.; Finke, I.; Kautz-Freimuth, S.; Stock, S. The evolution of health literacy assessment tools: A systematic review. BMC Public Health 2014, 14, 1207. [Google Scholar] [CrossRef]
- Fransen, M.P.; Van Schaik, T.M.; Twickler, T.B.; Essink-Bot, M.L. Applicability of internationally available health literacy measures in the Netherlands. J. Health Commun. 2011, 16, 134–149. [Google Scholar] [CrossRef]
- Dwinger, S.; Kriston, L.; Härter, M.; Dirmaier, J. Translation and validation of a multidimensional instrument to assess health literacy. Health Expect. 2015, 18, 2776–2786. [Google Scholar] [CrossRef] [PubMed]
- McDonald, F.E.; Patterson, P.; Costa, D.S.; Shepherd, H.L. Validation of a Health Literacy Measure for Adolescents and Young Adults Diagnosed with Cancer. J. Adolesc. Young Adult Oncol. 2016, 5, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Ousseine, Y.M.; Rouquette, A.; Bouhnik, A.D.; Rigal, L.; Ringa, V.; Smith, A.; Mancini, J. Validation of the French version of the Functional, Communicative and Critical Health Literacy scale (FCCHL). J. Patient Rep. Outcomes 2018, 2, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finbråten, H.S.; Guttersrud, Ø.; Nordström, G.; Pettersen, K.S.; Trollvik, A.; Wilde-Larsson, B. Validating the Functional, Communicative, and Critical Health Literacy Scale Using Rasch Modeling and Confirmatory Factor Analysis. J. Nurs. Meas. 2018, 26, 341–363. [Google Scholar] [CrossRef]
- Ishikawa, H.; Takeuchi, T.; Yano, E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care 2008, 31, 874–879. [Google Scholar] [CrossRef]
- Finbråten, H.S. Measuring Health Literacy–Evaluating Psychometric Properties of the HLS-EU-Q47 and the FCCHL, Suggesting Instrument Refinements and Exploring Health Literacy in People with Type 2 Diabetes and in the General Norwegian Population. Ph.D. Thesis, Karlstads Universitet, Karlstad, Sweden, 2018. [Google Scholar]
- Baur, C.; Harris, L.; Squire, E. The U.S. National action plan to improve health literacy: A model for positive organizational change. Stud. Health Technol. Inform. 2017, 240, 186–202. [Google Scholar] [PubMed]
- Heijmans, M.; Waverijn, G.; Rademakers, J.; van der Vaart, R.; Rijken, M. Functional, communicative and critical health literacy of chronic disease patients and their importance for self-management. Patient Educ. Couns. 2015, 98, 41–48. [Google Scholar] [CrossRef]
- Caruso, R.; Magon, A.; Baroni, I.; Dellafiore, F.; Arrigoni, C.; Pittella, F.; Ausili, D. Health literacy in type 2 diabetes patients: A systematic review of systematic reviews. Acta Diabetol. 2018, 55, 1–12. [Google Scholar] [CrossRef]
- Mantwill, S.; Monestel-Umaña, S.; Schulz, P.J. The relationship between health literacy and health disparities: A systematic review. PLoS ONE 2015, 10, 1–22. [Google Scholar]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef]
- Acquardro, C. ERIQA recommendations for translation and cultural adaptation of HRQL measures. In Proceedings of the ISPOR 6th Annual European Congress, Barcelona, Spain, 10–14 November 2003. [Google Scholar]
- Sousa, V.D.; Rojjanasrirat, W. Translation, Adaptation and Validation of Instruments or Scales for Use in Cross-Cultural Health Care Research: A Clear and User-Friendly Guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef]
- Comrey, A.L.; Lee, H.B. A First Course in Factor Analysis, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1992; ISBN 0805810625. [Google Scholar]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Press: New York, NY, USA, 1998. [Google Scholar]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Hair, J.F. Multivariate Data Analysis, 7th ed.; Pearson: Harlow, UK, USA, 2014. [Google Scholar]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Streiner, D.L.; Norman, G.R. Health Measurement Scales: A Practical Guide to Their Development and Use, 3rd ed.; Oxford University Press: New York, NY, USA, 2003; ISBN 0198528477. [Google Scholar]
- Suka, M.; Odajima, T.; Kasai, M.; Igarashi, A.; Ishikawa, H.; Kusama, M.; Nakayama, T.; Sumitani, M.; Sugimori, H. The 14-item health literacy scale for Japanese adults (HLS-14). Environ. Health Prev. Med. 2013, 18, 407–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Initial Variant of the Item | Suggestions after Pre-Testing | Changes | |
|---|---|---|---|
| FHL1 | Found that the print is too small to read | It was unclear for respondents whether it is applicable in the case of wearing glasses Suggestion: to add ‘even with glasses’ | Found that the print is too small to read even though you wear glasses |
| FHL4 | Found the content too difficult | It was unclear what it meant to be too difficult Suggestion: to add ‘to understand’ | Found the content too difficult to understand |
| FHL5 | Needed someone to help you read them | Needed help from another person in order to understand | |
| IHL1 | Collected information from different sources | Respondents were not sure what the different sources represent Suggestion: to add examples | Collected information from different sources (for example pharmacist, rheumatologist, general practitioner...) |
| IHL2 | Extracted the information you wanted | It was unclear for participants what this item presents Suggestion: to clarify with adding ‘only’ | Extracted (only) information you wanted |
| IHL4 | Communicated your thoughts about your health to someone | Respondents were confused by the term someone Suggestion: To clarify the term with examples | Communicated your thoughts about your health to someone (for example you children at home, your doctor, colleagues...) |
| Initial Variant of the Item | Suggestions after Pre-Testing | Changes | |
|---|---|---|---|
| FHL2 | Found characters and words that you did not know | Rephrased from “did not know” to “unfamiliar” for better understanding | Found unfamiliar characters and words |
| CHL4 | Collected information to make decisions about your health | Changed to be in the spirit of the language | Collected information to make health-related decisions |
| n (%) | |
|---|---|
| Marital status | |
| Unmarried | 15 (11.5%) |
| Married/Common-law | 85 (65.4%) |
| Divorced | 17 (13.1%) |
| Widow | 13 (10%) |
| Children | |
| Yes | 102 (78.5) |
| No | 28 (21.5) |
| Number of children | |
| One child | 30 (24.6) |
| Two children | 57 (46.7) |
| Three or more children | 14 (11.4) |
| Education | |
| 4 classes or no school | 1 (0.8%) |
| Primary school | 5 (3.8%) |
| High school | 44 (33.8%) |
| Higher school (VI grade) | 29 (22.3%) |
| University | 48 (36.9%) |
| Master’s degree/Specialization/PhD grade | 3 (2.3%) |
| Employment | |
| Incapable | 2 (1.5 %) |
| Unemployed | 10 (7.7 %) |
| Student | 1 (0.8 %) |
| Employed | 77 (59.2 %) |
| Pensioner | 39 (30.0 %) |
| Monthly income per family member | |
| ≤27,000 RSD * | 16 (12.3%) |
| 27,000–40,000 RSD | 22 (16.9%) |
| ≥40,000–60,000 RSD | 86 (66.2%) |
| ≥60,000 RSD | 6 (4.6%) |
| Chronic diseases | |
| T2DM T2DM and additional chronic diseases | 43 (33%) 87 (67%) |
| Therapy for T2DM | |
| Diet | 1 (0.8 %) |
| Tablets | 83 (63.8 %) |
| Tablets and Insulin | 36 (27.7 %) |
| Insulin | 10 (7.7 %) |
| Frequency of drug administration for T2DM | |
| Once a day | 8 (6.2%) |
| Twice a day | 69 (53.1%) |
| Three times a day | 37 (28.5%) |
| Four times a day | 15 (11.5%) |
| I don’t use drugs for T2DM | 1 (0.8%) |
| Active exercise | |
| Never | 27 (20.8%) |
| Less than once a week | 46 (35.4%) |
| 1–2 times a week | 37 (28.5%) |
| 3 and more times a week | 20 (15.4%) |
| Smoker | |
| ≤1 box a day | 35 (26.9%) |
| >1 box a day | 18 (13.8%) |
| Not smoker | 68 (52.3%) |
| Ex-smoker | 9 (6.9%) |
| Alcohol | |
| Never | 74 (56.9%) |
| Once a month | 35 (26.9%) |
| 2 or more times a month | 21 (16.2%) |
| Source of health information | |
| Doctors | 67 (51.5 %) |
| Pharmacists | 9 (6.9 %) |
| Parents | 1 (0.8 %) |
| Internet | 18 (13.8 %) |
| Friends | 1 (0.8 %) |
| Books/Magazines/TV | 3 (2.3 %) |
| Doctors and Pharmacists | 27 (20.8 %) |
| Doctors and Internet | 1 (0.8 %) |
| Doctors, Pharmacists, and Internet | 3 (2.3 %) |
| Interest in health | |
| Not interested | 3 (2.3%) |
| Little | 22 (16.9%) |
| Medium | 66 (50.8%) |
| Much | 21 (16.2%) |
| Very interested | 18 (13.8%) |
| Self-estimation of health status | |
| Very bad | 6 (4.6 %) |
| Bad | 31 (23.8 %) |
| Good | 77 (59.2 %) |
| Very good | 16 (12.3 %) |
| FHL | (1) Small Print | (2) Unfamiliar Characters and Words | (3) Difficult Content | (4) More Time Needed | (5) Needed Help |
| Mean | 2.05 | 2.17 | 2.32 | 2.19 | 2.51 |
| Median | 2.00 | 2.00 | 2.00 | 2.00 | 3.00 |
| Standard deviation | 0.951 | 0.916 | 0.856 | 0.872 | 0.950 |
| Skewness | 0.331 | 0.147 | 0.077 | 0.183 | −0.022 |
| Kurtosis | −1.05 | −1.00 | −0.653 | −0.756 | −0.899 |
| Standardized factor loadings | 0.543 | 0.722 | 0.641 | 0.733 | 0.689 |
| IHL | (1) Information sources | (2) Wanted information | (3) Understanding the information gathered | (4) Sharing thoughts with someone | (5) Application of information |
| Mean | 2.48 | 2.52 | 2.78 | 2.79 | 2.60 |
| Median | 2.00 | 2.50 | 3.00 | 3.00 | 3.00 |
| Standard deviation | 0.865 | 0.799 | 0.853 | 0.938 | 0.886 |
| Skewness | 0.048 | 0.062 | −0.177 | −0.202 | −0.003 |
| Kurtosis | −0.628 | −0.436 | −0.660 | −0.929 | −0.734 |
| Standardized factor loadings | 0.599 | 0.490 | 0.549 | 0.696 | 0.756 |
| CHL | (1) Considered the applicability of the information | (2) Credibility of information | (3) Checking the accuracy of information | (4) Collecting information | |
| Mean | 2.72 | 2.47 | 2.48 | 2.65 | |
| Median | 3.00 | 2.00 | 3.00 | 3.00 | |
| Standard deviation | 0.872 | 0.873 | 0.837 | 0.929 | |
| Skewness | −0.283 | −0.011 | −0.071 | −0.019 | |
| Kurtosis | −0.543 | −0.663 | −0.550 | −0.911 | |
| Standardized factor loadings | 0.772 | 0.675 | 0.604 | 0.752 |
| Model | χ2 | df | p | CFI | SRMR | RMSEA (90%CI) |
|---|---|---|---|---|---|---|
| FCCHL-SR14 | 192 | 74 | <0.001 | 0.819 | 0.0779 | 0.111 0.092–0.130 |
| Modified FCCHL-SR14 with one correlated error | 173 | 73 | <0.001 | 0.846 | 0.0753 | 0.103 0.084–0.123 |
| Modified FCCHL-SR14 with two correlated error | 158 | 72 | <0.001 | 0.867 | 0.0731 | 0.0961 0.0761–0.117 |
| FCCHL-SR12 | 96 | 51 | <0.001 | 0.916 | 0.0676 | 0.0831 (0.057–0.108) |
| Δ FCCHL-SR14-FCCHL-SR12 | 96 | 23 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levic, M.; Bogavac-Stanojevic, N.; Krajnovic, D. Cross-Cultural Adaptation and Validation of the Functional, Communicative and Critical Health Literacy Instrument (FCCHL-SR) for Diabetic Patients in Serbia. Healthcare 2022, 10, 1667. https://doi.org/10.3390/healthcare10091667
Levic M, Bogavac-Stanojevic N, Krajnovic D. Cross-Cultural Adaptation and Validation of the Functional, Communicative and Critical Health Literacy Instrument (FCCHL-SR) for Diabetic Patients in Serbia. Healthcare. 2022; 10(9):1667. https://doi.org/10.3390/healthcare10091667
Chicago/Turabian StyleLevic, Marija, Natasa Bogavac-Stanojevic, and Dusanka Krajnovic. 2022. "Cross-Cultural Adaptation and Validation of the Functional, Communicative and Critical Health Literacy Instrument (FCCHL-SR) for Diabetic Patients in Serbia" Healthcare 10, no. 9: 1667. https://doi.org/10.3390/healthcare10091667
APA StyleLevic, M., Bogavac-Stanojevic, N., & Krajnovic, D. (2022). Cross-Cultural Adaptation and Validation of the Functional, Communicative and Critical Health Literacy Instrument (FCCHL-SR) for Diabetic Patients in Serbia. Healthcare, 10(9), 1667. https://doi.org/10.3390/healthcare10091667