

Integrated Osteoporosis Care to Reduce Denosumab-Associated Hypocalcemia for Patients with Advanced Chronic Kidney Disease and End-Stage Renal Disease

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Integrated Osteoporosis Care Program among Patients with Advanced CKD and ESRD
2.2. Study Design and Subjects
2.3. Statistical Analysis
3. Results
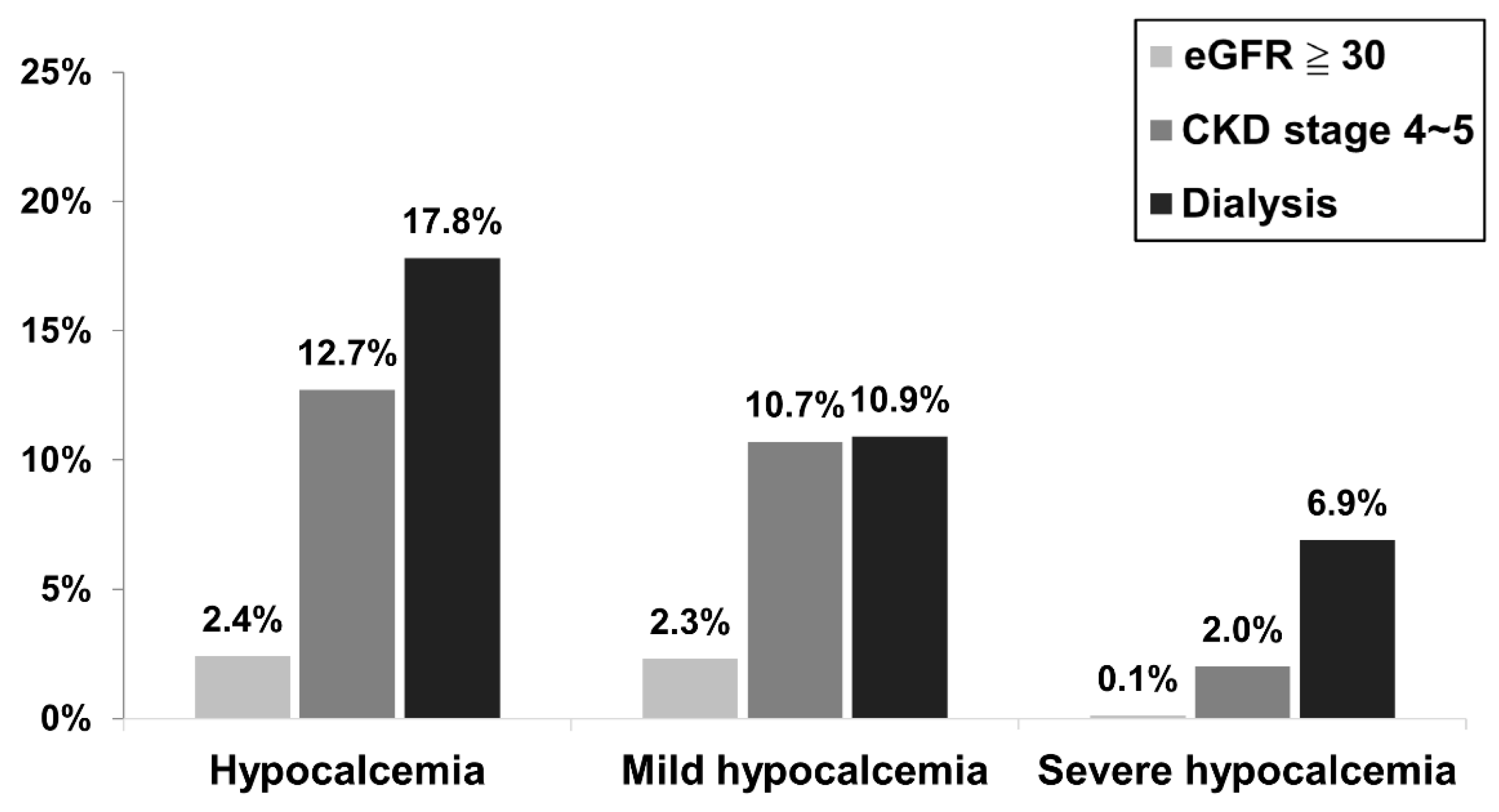
3.1. Comparing the Incidence of Post-Treatment Hypocalcemia within 30 Days among Different Renal Function Groups on Denosumab
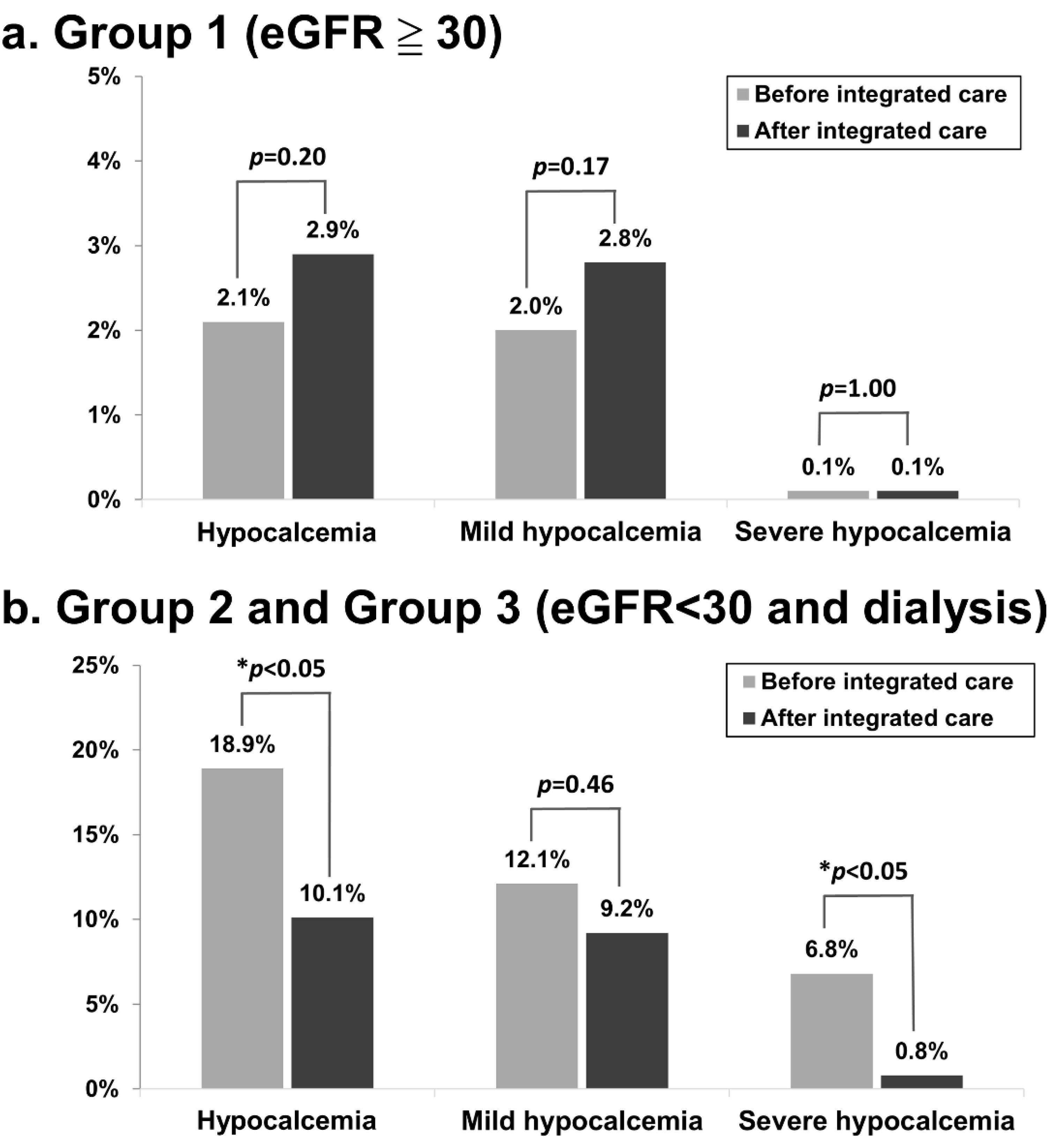
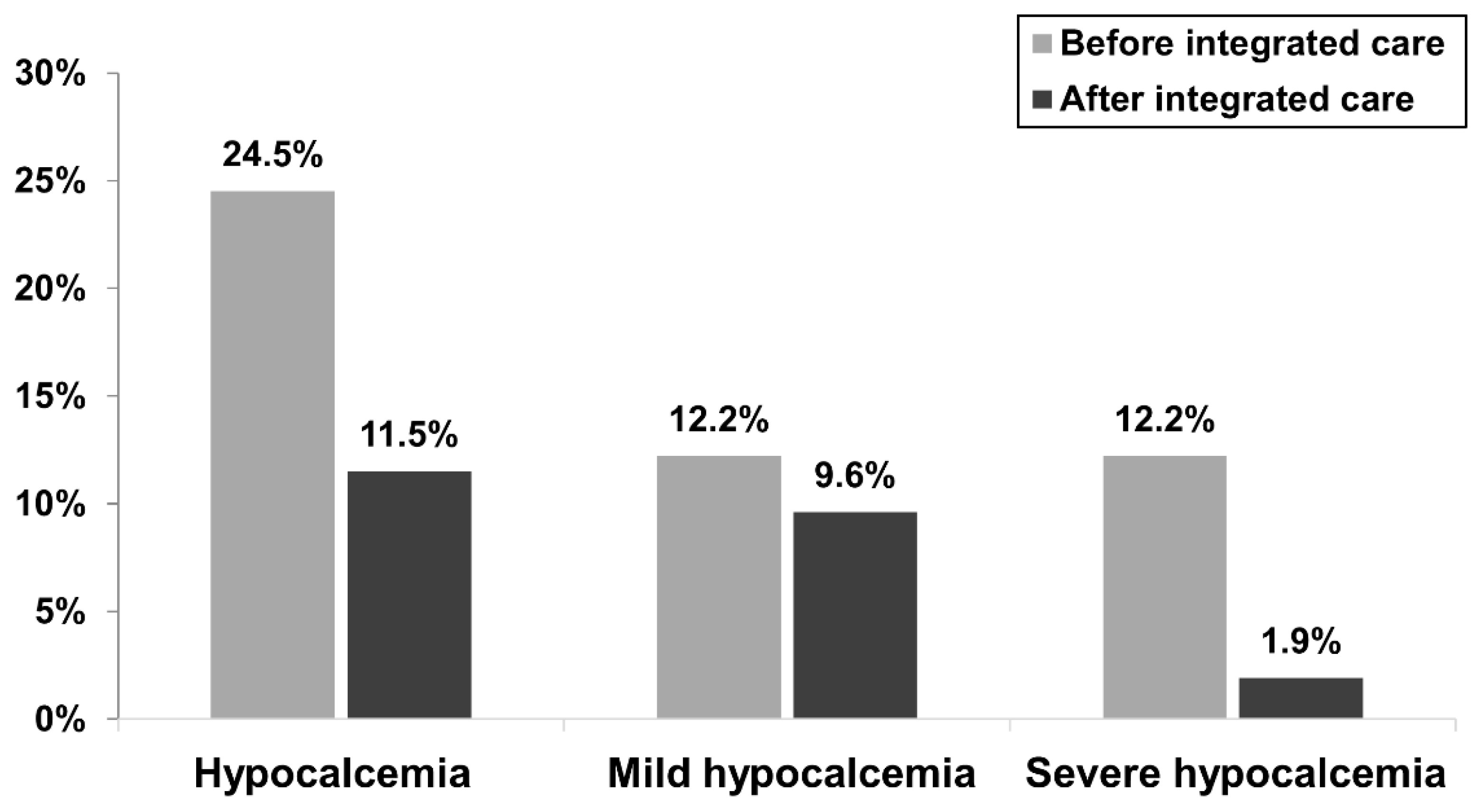
3.2. The Incidence of Hypocalcemia within 30 Days Following the First Dose of Denosumab Treatment before and after the Implementation of the Integrated Care Program
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int. Suppl. 2017, 7, 1–59. [CrossRef] [PubMed] [Green Version]
- Alem, A.M.; Sherrard, D.J.; Gillen, D.L.; Weiss, N.S.; Beresford, S.A.; Heckbert, S.R.; Wong, C.; Stehman-Breen, C. Increased risk of hip fracture among patients with end-stage renal disease. Kidney Int. 2000, 58, 396–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nickolas, T.L.; Leonard, M.B.; Shane, E. Chronic kidney disease and bone fracture: A growing concern. Kidney Int. 2008, 74, 721–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nickolas, T.L.; McMahon, D.J.; Shane, E. Relationship between moderate to severe kidney disease and hip fracture in the United States. J. Am. Soc. Nephrol. 2006, 17, 3223–3232. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, A.; Urena-Torres, P.; Zillikens, M.C.; Bover, J.; Cohen-Solal, M. Fractures in patients with CKD—Diagnosis, treatment, and prevention: A review by members of the European Calcified Tissue Society and the European Renal Association of Nephrology Dialysis and Transplantation. Kidney Int. 2017, 92, 1343–1355. [Google Scholar] [CrossRef] [Green Version]
- Dave, V.; Chiang, C.Y.; Booth, J.; Mount, P.F. Hypocalcemia post denosumab in patients with chronic kidney disease stage 4-5. Am. J. Nephrol. 2015, 41, 129–137. [Google Scholar] [CrossRef]
- Festuccia, F.; Jafari, M.T.; Moioli, A.; Fofi, C.; Barberi, S.; Amendola, S.; Sciacchitano, S.; Punzo, G.; Menè, P. Safety and efficacy of denosumab in osteoporotic hemodialysed patients. J. Nephrol. 2017, 30, 271–279. [Google Scholar] [CrossRef]
- Gopaul, A.; Kanagalingam, T.; Thain, J.; Khan, T.; Cowan, A.; Sultan, N.; Clemens, K.K. Denosumab in chronic kidney disease: A narrative review of treatment efficacy and safety. Arch. Osteoporos. 2021, 16, 116. [Google Scholar] [CrossRef]
- Hiramatsu, R.; Ubara, Y.; Sawa, N.; Sakai, A. Hypocalcemia and bone mineral changes in hemodialysis patients with low bone mass treated with denosumab: A 2-year observational study. Nephrol. Dial. Transplant. 2021, 36, 1900–1907. [Google Scholar] [CrossRef]
- Jalleh, R.; Basu, G.; Le Leu, R.; Jesudason, S. Denosumab-induced severe hypocalcaemia in chronic kidney disease. Case Rep. Nephrol. 2018, 2018, 7384763. [Google Scholar] [CrossRef]
- McCormick, B.B.; Davis, J.; Burns, K.D. Severe hypocalcemia following denosumab injection in a hemodialysis patient. Am. J. Kidney Dis. 2012, 60, 626–628. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Acharya, P.; Acharya, C.; Chenbhanich, J.; Bathini, T.; Boonpheng, B.; Sharma, K.; Wijarnpreecha, K.; Ungprasert, P.; Gonzalez Suarez, M. Hypocalcemia and bone mineral density changes following denosumab treatment in end-stage renal disease patients: A meta-analysis of observational studies. Osteoporos. Int. 2018, 29, 1737–1745. [Google Scholar] [CrossRef] [PubMed]
- Tsvetov, G.; Amitai, O.; Shochat, T.; Shimon, I.; Akirov, A.; Diker-Cohen, T. Denosumab-induced hypocalcemia in patients with osteoporosis: Can you know who will get low? Osteoporos. Int. 2020, 31, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Mac Way, F.; Lessard, M.; Lafage-Proust, M.-H. Pathophysiology of chronic kidney disease-mineral and bone disorder. Jt. Bone Spine. 2012, 79, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Sexton, J.; Vincent, M. Remedying calcium and phosphate problems in chronic kidney disease. Pharm. J. 2005, 274, 561–564. [Google Scholar]
- Cummings, S.R.; Martin, J.S.; McClung, M.R.; Siris, E.S.; Eastell, R.; Reid, I.R.; Delmas, P.; Zoog, H.B.; Austin, M.; Wang, A. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N. Engl. J. Med. 2009, 361, 756–765. [Google Scholar] [CrossRef] [Green Version]
- Block, G.A.; Bone, H.G.; Fang, L.; Lee, E.; Padhi, D. A single-dose study of denosumab in patients with various degrees of renal impairment. J. Bone Miner. Res. 2012, 27, 1471–1479. [Google Scholar] [CrossRef]
- Chen, C.-L.; Chen, N.-C.; Hsu, C.-Y.; Chou, K.-J.; Lee, P.-T.; Fang, H.-C.; Renn, J.-H. An open-label, prospective pilot clinical study of denosumab for severe hyperparathyroidism in patients with low bone mass undergoing dialysis. J. Clin. Endocrinol. Metab. 2014, 99, 2426–2432. [Google Scholar] [CrossRef] [Green Version]
- Kunizawa, K.; Hiramatsu, R.; Hoshino, J.; Mizuno, H.; Ozawa, Y.; Sekine, A.; Kawada, M.; Sumida, K.; Hasegawa, E.; Yamanouchi, M. Denosumab for dialysis patients with osteoporosis: A cohort study. Sci. Rep. 2020, 10, 2496. [Google Scholar] [CrossRef] [Green Version]
- Pepe, J.; Colangelo, L.; Biamonte, F.; Sonato, C.; Danese, V.C.; Cecchetti, V.; Occhiuto, M.; Piazzolla, V.; De Martino, V.; Ferrone, F. Diagnosis and management of hypocalcemia. Endocrine 2020, 69, 485–495. [Google Scholar] [CrossRef]
- Koppel, R.; Metlay, J.P.; Cohen, A.; Abaluck, B.; Localio, A.R.; Kimmel, S.E.; Strom, B.L. Role of computerized physician order entry systems in facilitating medication errors. J. Am. Med. Assoc. 2005, 293, 1197–1203. [Google Scholar] [CrossRef] [PubMed]
- Evenepoel, P.; Cunningham, J.; Ferrari, S.; Haarhaus, M.; Javaid, M.K.; Lafage-Proust, M.-H.; Prieto-Alhambra, D.; Torres, P.U.; Cannata-Andia, J. European Consensus Statement on the diagnosis and management of osteoporosis in chronic kidney disease stages G4–G5D. Nephrol. Dial. Transplant. 2021, 36, 42–59. [Google Scholar] [CrossRef] [PubMed]
- Laskowski, L.K.; Goldfarb, D.S.; Howland, M.A.; Kavcsak, K.; Lμgassy, D.M.; Smith, S.W. A RANKL wrinkle: Denosumab-induced hypocalcemia. J. Med. Toxicol. 2016, 12, 305–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waziri, B.; Duarte, R.; Naicker, S. Chronic kidney disease–mineral and bone disorder (CKD-MBD): Current perspectives. Int. J. Nephrol. Renov. Dis. 2019, 12, 263. [Google Scholar] [CrossRef] [Green Version]
- Saito, Y.; Takekuma, Y.; Komatsu, Y.; Sμgawara, M. Risk Analysis of Denosumab-Induced Hypocalcemia in Bone Metastasis Treatment: Renal Dysfunction Is Not a Risk Factor for Its Incidence in a Strict Denosumab Administration Management System with Calcium/Vitamin D Supplementation. Biol. Pharm. Bull. 2021, 44, 1819–1823. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group 1 eGFR ≥ 30 (n = 2957) | Group 2 CKD Stage 4 and 5 (n = 150) | Group 3 Dialysis (n = 101) | p Value | H-Statistic/ Chi-Square Statistic | ||||
|---|---|---|---|---|---|---|---|---|
| Demographic characteristics | ||||||||
| Age † | 73.5 | (65.9–80.8) | 79.6 | (72.2–86.2) | 69.0 | (61.0–76.1) | <0.001 ** | 52.003 |
| Male sex ‡ | 543 | (18.4%) | 33 | (22.0%) | 26 | (25.7%) | 0.102 | 4.569 |
| Weight † | 55.4 | (49.7–62.0) | 57.8 | (47.1–65.0) | 54.0 | (48.0–63.2) | 0.567 | 1.135 |
| Height † | 154.0 | (149.4–159.0) | 153.0 | (148.6–159.4) | 156.5 | (150.1–161.9) | 0.193 | 3.290 |
| BMI † | 23.3 | (20.9–26.0) | 23.3 | (20.2–27.3) | 23.0 | (20.3–24.8) | 0.382 | 1.923 |
| Comorbidity | ||||||||
| Diabetes ‡ | 1002 | (33.9%) | 75 | (50.0%) | 48 | (47.5%) | <0.001 ** | 23.386 |
| Hypertension ‡ | 1357 | (45.9%) | 120 | (80.0%) | 88 | (87.1%) | <0.001 ** | 127.841 |
| Stroke ‡ | 423 | (14.3%) | 35 | (23.3%) | 22 | (21.8%) | 0.002 ** | 12.957 |
| CAD ‡ | 827 | (28.0%) | 50 | (33.3%) | 57 | (56.4%) | <0.001 ** | 39.709 |
| PAD ‡ | 263 | (8.9%) | 19 | (12.7%) | 21 | (20.8%) | <0.001 ** | 18.074 |
| CHF ‡ | 331 | (11.2%) | 21 | (18.0%) | 42 | (41.6%) | <0.001 ** | 87.056 |
| Baseline laboratory data | ||||||||
| eGFR § | 78.3 | (62.4–94.3) | 21.9 | (14.1–26.4) | - | - | <0.001 ** | 428.137 |
| Corrected Calcium † | 9.10 | (8.82–9.40) | 9.00 | (8.50–9.36) | 9.35 | (8.81–10.10) | <0.001 ** | 18.146 |
| Phosphate † | 3.6 | (3.3–4.0) | 4.0 | (3.5–4.5) | 4.4 | (3.7–5.9) | <0.001 ** | 64.366 |
| ALP † | 103.0 | (81.0–134.0) | 127.0 | (96.3–174.8) | 135.5 | (106.0–189.0) | <0.001 ** | 40.994 |
| Intact-PTH † | 52.3 | (37.6–71.3) | 178.0 | (84.2–303.9) | 341.9 | (124.3–677.3) | <0.001 ** | 135.188 |
| Post-treatment hypocalcemia within 30 days following the first dose of denosumab treatment | ||||||||
| Hypocalcemia ‡ | 71 | (2.4%) | 19 | (12.7%) | 18 | (17.8%) | <0.001 ** | 113.224 |
| Mild hypocalcemia ‡ | 68 | (2.3%) | 16 | (10.7%) | 11 | (10.9%) | <0.001 ** | 57.598 |
| Severe hypocalcemia ‡ | 3 | (0.1%) | 3 | (2.0%) | 7 | (6.9%) | <0.001 ** | 122.774 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p Value | Hazard Ratio | 95% CI | p Value | |
| Integrated care | 0.26 | (0.06–1.19) | 0.083 | |||
| Renal function group | 8.18 | (4.43–15.08) | <0.001 ** | 8.31 | (1.20-57.30) | 0.032 * |
| Age | 0.94 | (0.90–0.98) | 0.003 ** | |||
| Male sex | 1.30 | (0.36–4.74) | 0.687 | |||
| BMI | 0.81 | (0.67–0.98) | 0.027 * | |||
| Diabetes | 2.17 | (0.73–6.46) | 0.163 | |||
| Hypertension | 5.82 | (1.29–26.26) | 0.021 * | |||
| Stroke | 2.55 | (0.79–8.28) | 0.119 | |||
| CAD | 1.10 | (0.34–3.57) | 0.877 | |||
| PAD | 2.89 | (0.79–10.49) | 0.107 | |||
| CHF | 1.30 | (0.29–5.88) | 0.732 | |||
| Baseline corrected Ca | 0.25 | (0.13–0.49) | <0.001 ** | 0.29 | (0.09–0.93) | 0.038 * |
| Baseline phosphate | 1.99 | (1.48–2.67) | <0.001 ** | |||
| Baseline ALP | 1.01 | (1.00–1.01) | <0.001 ** | |||
| Baseline intact-PTH | 1.00 | (1.00–1.00) | <0.001 ** | 1.00 | (1.00–1.00) | 0.096 |
| Before Integrated Care (n = 132) | After Integrated Care (n = 119) | p Value | Z-Statistic/ Chi-Square Statistic | |||
|---|---|---|---|---|---|---|
| Demographic characteristics | ||||||
| Age † | 75.2 | (65.5–83.8) | 76.1 | (67.2–84.6) | 0.206 | −1.264 |
| Male sex ‡ | 31 | (23.5%) | 28 | (23.5%) | 0.993 | 0.000 |
| Weight † | 55.3 | (43.9–62.5) | 56.2 | (48.5–65.0) | 0.203 | −1.273 |
| Height † | 153.0 | (147.2–160.3) | 155.8 | (151.5–159.8) | 0.660 | −0.440 |
| BMI † | 23.0 | (19.8–26.5) | 23.3 | (20.8–25.6) | 0.430 | −0.788 |
| Renal function group | ||||||
| CKD stage 4 and 5 ‡ | 83 | (62.9%) | 67 | (56.3%) | 0.290 | 1.121 |
| Dialysis ‡ | 49 | (37.1%) | 52 | (47.3%) | 0.290 | 1.121 |
| Comorbidity | ||||||
| Diabetes ‡ | 57 | (43.2%) | 66 | (55.5%) | 0.052 | 3.762 |
| Hypertension ‡ | 107 | (81.1%) | 101 | (84.9%) | 0.424 | 0.638 |
| Stroke ‡ | 29 | (22.0%) | 28 | (23.5%) | 0.769 | 0.086 |
| CAD ‡ | 54 | (40.9%) | 53 | (44.5%) | 0.562 | 0.336 |
| PAD ‡ | 23 | (17.4%) | 17 | (14.3%) | 0.498 | 0.458 |
| CHF ‡ | 32 | (24.2%) | 37 | (31.1%) | 0.226 | 1.467 |
| Baseline laboratory data | ||||||
| eGFR (CKD stage 4 and 5) † | 22.0 | (14.25–27.0) | 21.0 | (14.0–25.0) | 0.704 | −0.380 |
| Corrected Ca † | 9.0 | (8.6–9.4) | 9.2 | (8.7–9.4) | 0.369 | −0.898 |
| Phosphate † | 4.2 | (3.7–4.9) | 4.1 | (3.5–5.2) | 0.964 | −0.045 |
| ALP † | 129.0 | (105.0–175.0) | 128.0 | (96.8–180.8) | 0.977 | −0.029 |
| Intact-PTH † | 227.2 | (83.9–570.2) | 246.3 | (124.5–629.3) | 0.984 | −0.001 |
| Post-treatment hypocalcemia within 30 days following the first dose of denosumab treatment | ||||||
| Hypocalcemia ‡ | 25 | (18.9%) | 12 | (10.1%) | 0.049 * | 3.899 |
| Mild hypocalcemia ‡ | 16 | (12.1%) | 11 | (9.2%) | 0.463 | 0.538 |
| Severe hypocalcemia § | 9 | (6.8%) | 1 | (0.8%) | 0.021 * | 5.823 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p Value | Hazard Ratio | 95% CI | p Value | |
| Integrated care | 0.12 | (0.02–0.95) | 0.045 * | 0.15 | (0.02–1.23) | 0.077 |
| Renal function group | 3.74 | (0.97–14.46) | 0.056 | 2.66 | (0.46–15.38) | 0.275 |
| Age | 0.94 | (0.90–0.98) | 0.006 ** | 0.97 | (0.91–1.02) | 0.222 |
| Male sex | 0.82 | (0.17–3.86) | 0.802 | 0.99 | (0.20–5.03) | 0.993 |
| BMI | 0.82 | (0.67–1.01) | 0.057 | 0.87 | (0.70–1.07) | 0.177 |
| Diabetes | 1.08 | (0.31–3.73) | 0.903 | |||
| Hypertension | 1.98 | (0.25–15.62) | 0.517 | |||
| Stroke | 2.32 | (0.66–8.23) | 0.192 | |||
| CAD | 0.94 | (0.27–3.33) | 0.924 | |||
| PAD | 1.33 | (0.28–6.28) | 0.716 | |||
| CHF | 0.71 | (0.15–3.34) | 0.663 | |||
| Baseline corrected Ca | 0.54 | (0.24–0.49) | 0.129 | |||
| Baseline phosphate | 1.35 | (0.88–2.06) | 0.165 | |||
| Baseline ALP | 1.00 | (1.00–1.01) | 0.347 | |||
| Baseline intact-PTH | 1.00 | (1.00–1.00) | 0.311 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-T.; Deng, Y.-L.; Chung, M.-C.; Tsai, S.-F.; Lin, S.-Y.; Chen, C.-H. Integrated Osteoporosis Care to Reduce Denosumab-Associated Hypocalcemia for Patients with Advanced Chronic Kidney Disease and End-Stage Renal Disease. Healthcare 2023, 11, 313. https://doi.org/10.3390/healthcare11030313
Hsu C-T, Deng Y-L, Chung M-C, Tsai S-F, Lin S-Y, Chen C-H. Integrated Osteoporosis Care to Reduce Denosumab-Associated Hypocalcemia for Patients with Advanced Chronic Kidney Disease and End-Stage Renal Disease. Healthcare. 2023; 11(3):313. https://doi.org/10.3390/healthcare11030313
Chicago/Turabian StyleHsu, Chia-Tien, Ya-Lian Deng, Mu-Chi Chung, Shang-Feng Tsai, Shih-Yi Lin, and Cheng-Hsu Chen. 2023. "Integrated Osteoporosis Care to Reduce Denosumab-Associated Hypocalcemia for Patients with Advanced Chronic Kidney Disease and End-Stage Renal Disease" Healthcare 11, no. 3: 313. https://doi.org/10.3390/healthcare11030313
APA StyleHsu, C. -T., Deng, Y. -L., Chung, M. -C., Tsai, S. -F., Lin, S. -Y., & Chen, C. -H. (2023). Integrated Osteoporosis Care to Reduce Denosumab-Associated Hypocalcemia for Patients with Advanced Chronic Kidney Disease and End-Stage Renal Disease. Healthcare, 11(3), 313. https://doi.org/10.3390/healthcare11030313