

Metabolic Syndrome and Chronic Disease Risk in South Asian Immigrants: A Review of Prevalence, Factors, and Interventions



Abstract
:1. Introduction
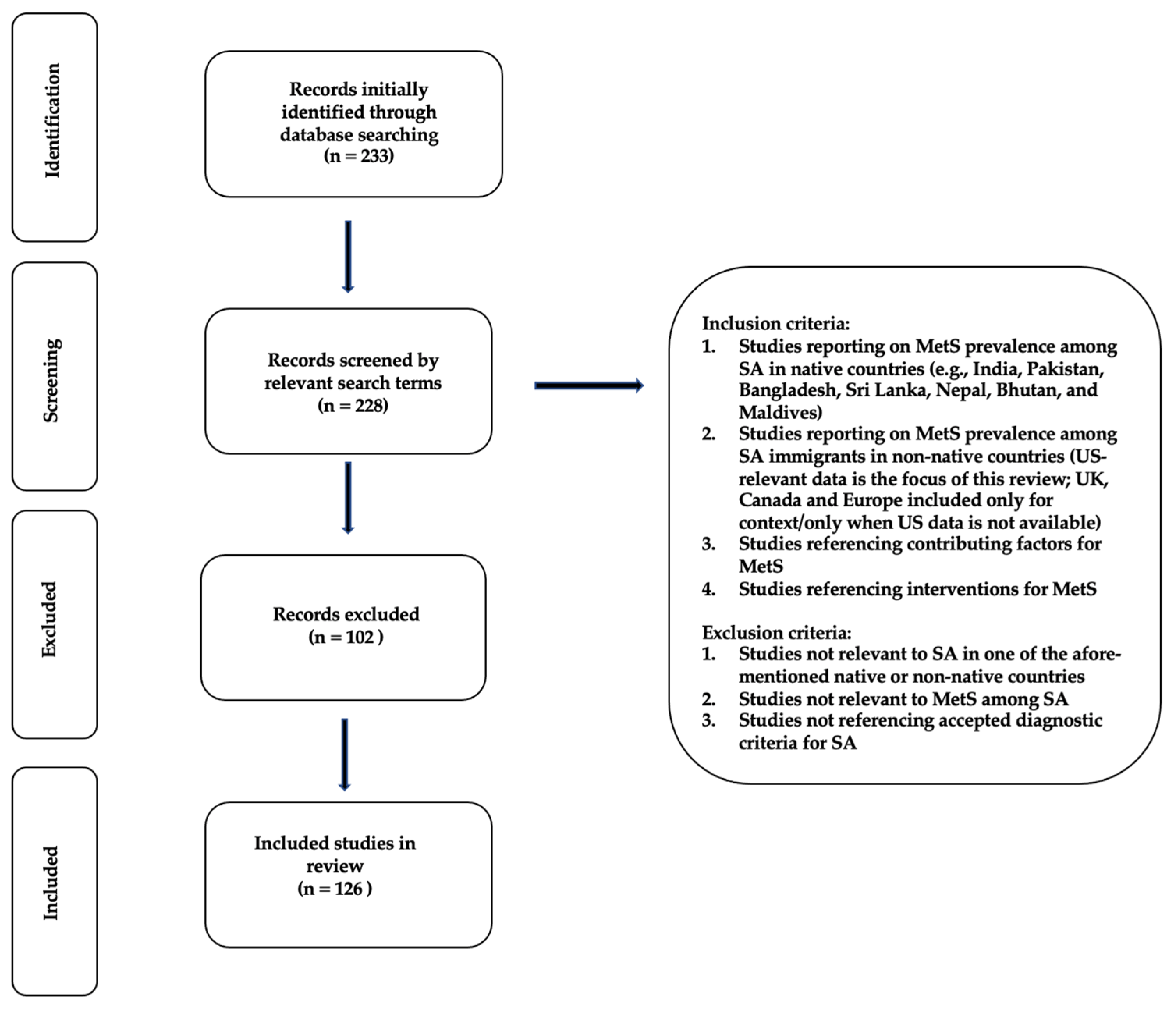
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grundy, S.M. Metabolic syndrome scientific statement by the American Heart Association and the National Heart, Lung, and Blood Institute. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 2243–2244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, J.-A.; Lee, J.-H.; Lim, S.-Y.; Ha, H.-S.; Kwon, H.-S.; Park, Y.-M.; Lee, W.-C.; Kang, M.-I.; Yim, H.-W.; Yoon, K.-H.; et al. Metabolic syndrome as a predictor of type 2 diabetes, and its clinical interpretations and usefulness. J. Diabetes Investig. 2013, 4, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Mottillo, S.; Filion, K.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.; Eisenberg, M. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF diabetes atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Kolovou, G.D.; Anagnostopoulou, K.K.; Salpea, K.D.; Mikhailidis, D.P. The prevalence of metabolic syndrome in various populations. Am. J. Med. Sci. 2007, 333, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Hirode, G.; Wong, R.J. Trends in the prevalence of metabolic syndrome in the United States, 2011–2016. JAMA 2020, 323, 2526–2528. [Google Scholar] [CrossRef]
- Kassi, E.; Pervanidou, P.; Kaltsas, G.; Chrousos, G. Metabolic syndrome: Definitions and controversies. BMC Med. 2011, 9, 48. [Google Scholar] [CrossRef] [Green Version]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- U.S. Census Bureau. Asian-American and Pacific Islander Heritage Month: May 2022. Census.gov. Available online: https://www.census.gov/newsroom/facts-for-features/2022/asian-american-pacific-islander.html (accessed on 1 February 2023).
- Bajaj, H.S.; Pereira, M.A.; Anjana, R.M.; Deepa, R.; Mohan, V.; Mueller, N.T.; Rao, G.H.; Gross, M.D. Comparison of relative waist circumference between Asian Indian and US adults. J. Obes. 2014, 2014, 461956. [Google Scholar] [CrossRef] [Green Version]
- Mohanty, S.A.; Woolhandler, S.; Himmelstein, D.U.; Bor, D.H. Diabetes and cardiovascular disease among Asian Indians in the United States. J. Gen. Intern. Med. 2005, 20, 474–478. [Google Scholar] [CrossRef] [Green Version]
- Kanaya, A.M.; Herrington, D.; Vittinghoff, E.; Ewing, S.K.; Liu, K.; Blaha, M.J.; Dave, S.S.; Qureshi, F.; Kandula, N.R. Understanding the high prevalence of diabetes in U.S. South Asians compared with four racial/ethnic groups: The MASALA and MESA studies. Diabetes Care 2014, 37, 1621–1628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karter, A.J.; Schillinger, D.; Adams, A.S.; Moffet, H.H.; Liu, J.; Adler, N.E.; Kanaya, A.M. Elevated rates of diabetes in Pacific Islanders and Asian subgroups: The Diabetes Study of Northern California (DISTANCE). Diabetes Care 2013, 36, 574–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.W.R.; Brancati, F.L.; Yeh, H.C. Trends in the prevalence of type 2 diabetes in Asians versus Whites: Results from the United States National Health Interview Survey, 1997–2008. Diabetes Care 2011, 34, 353–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajra, A.; Li, Y.; Siu, S.; Udaltsova, N.; Armstrong, M.A.; Friedman, G.D.; Klatsky, A.L. Risk of coronary disease in the South Asian American population. J. Am. Coll. Cardiol. 2013, 62, 644–645. [Google Scholar] [CrossRef]
- Palaniappan, L.; Wang, Y.; Fortmann, S.P. Coronary heart disease mortality for six ethnic groups in California, 1990–2000. Ann. Epidemiol. 2004, 14, 499–506. [Google Scholar] [CrossRef]
- Anand, S.S.; Tarnopolsky, M.A.; Rashid, S.; Schulze, K.M.; Desai, D.; Mente, A.; Rao, S.; Yusuf, S.; Gerstein, H.C.; Sharma, A.M. Adipocyte hypertrophy, fatty liver, and metabolic risk factors in South Asians: The Molecular Study of Health and Risk in Ethnic Groups (mol-SHARE). PLoS ONE 2011, 6, e22112. [Google Scholar] [CrossRef] [Green Version]
- Chandalia, M.; Lin, P.; Seenivasan, T.; Livingston, E.H.; Snell, P.G.; Grundy, S.M.; Abate, N. Insulin resistance and body fat distribution in South Asian men compared to Caucasian men. PLoS ONE 2007, 2, e812. [Google Scholar] [CrossRef]
- Raji, A.; Seely, E.W.; Arky, R.A.; Simonson, D.C. Body fat distribution and insulin resistance in healthy Asian Indians and Caucasians. J. Clin. Endocrinol. Metab. 2001, 86, 5366–5371. [Google Scholar] [CrossRef]
- Tillin, T.; Forouhi, N.; Johnston, D.G.; McKeigue, P.M.; Chaturvedi, N.; Godsland, I.F. Metabolic syndrome and coronary heart disease in South Asians, African-Caribbeans and white Europeans: A UK population-based cross-sectional study. Diabetologia 2005, 48, 649–656. [Google Scholar] [CrossRef] [Green Version]
- Forouhi, N.G.; Sattar, N.; Tillin, T.; McKeigue, P.M.; Chaturvedi, N. Do known risk factors explain the higher coronary heart disease mortality in South Asian compared with European men? Prospective follow-up of the Southall and Brent studies, UK. Diabetologia 2006, 49, 2580–2588. [Google Scholar] [CrossRef] [Green Version]
- Ajjan, R.; Carter, A.M.; Somani, R.; Kain, K.; Grant, P.J. Ethnic differences in cardiovascular risk factors in healthy Caucasian and South Asian individuals with the metabolic syndrome. J. Thromb. Haemost. 2007, 5, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Rajpathak, S.N.; Gupta, L.S.; Waddell, E.N.; Upadhyay, U.D.; Wildman, R.P.; Kaplan, R.; Wassertheil-Smoller, S.; Wylie-Rosett, J. Elevated risk of type 2 diabetes and metabolic syndrome among Asians and South Asians: Results from the 2004 New York City HANES. Ethn. Dis. 2010, 20, 225–230. [Google Scholar] [PubMed]
- Geragotou, T.; Jainandunsing, S.; Özcan, B.; de Rooij, F.W.M.; Kokkinos, A.; Tentolouris, N.; Sijbrands, E.J.G. The relationship of metabolic syndrome traits with beta-cell function and insulin sensitivity by oral minimal model assessment in South Asian and European families residing in the Netherlands. J. Diabetes Res. 2016, 2016, 9286303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anand, S.S.; Yi, Q.; Gerstein, H.; Lonn, E.; Jacobs, R.; Vuksan, V.; Teo, K.; Davis, B.; Montague, P.; Yusuf, S. Relationship of metabolic syndrome and fibrinolytic dysfunction to cardiovascular disease. Circulation 2003, 108, 420–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Khan, S.; Jackson, R.T. The prevalence of metabolic syndrome among low-income South Asian Americans. Public Health Nutr. 2016, 19, 418–428. [Google Scholar] [CrossRef] [Green Version]
- Flowers, E.; Molina, C.; Mathur, A.; Prasad, M.; Abrams, L.; Sathe, A.; Malhotra, D.; Basra, R.; Malgesini, N.; Ratnam, G.; et al. Prevalence of metabolic syndrome in South Asians residing in the United States. Metab. Syndr. Relat. Disord. 2010, 8, 417–423. [Google Scholar] [CrossRef]
- Misra, R.; Patel, T.; Kotha, P.; Raji, A.; Ganda, O.; Banerji, M.; Shah, V.; Vijay, K.; Mudaliar, S.; Iyer, D.; et al. Prevalence of diabetes, metabolic syndrome, and cardiovascular risk factors in US Asian Indians: Results from a national study. J. Diabetes Its Complicat. 2010, 24, 145–153. [Google Scholar] [CrossRef]
- Misra, K.B.; Endemann, S.W.; Ayer, M. Leisure time physical activity and metabolic syndrome in Asian Indian immigrants residing in northern California. Ethn. Dis. 2005, 15, 627–634. [Google Scholar]
- Balasubramanyam, A.; Rao, S.; Misra, R.; Sekhar, R.V.; Ballantyne, C.M. Prevalence of metabolic syndrome and associated risk factors in Asian Indians. J. Immigr. Minor. Health 2008, 10, 313–323. [Google Scholar] [CrossRef]
- Rianon, N.J.; Rasu, R.S. Metabolic syndrome and its risk factors in Bangladeshi immigrant men in the USA. J. Immigr. Minor. Health 2009, 12, 781–787. [Google Scholar] [CrossRef]
- Adil, S.O.; Islam, M.A.; Musa, K.I.; Shafique, K. Prevalence of Metabolic Syndrome among Apparently Healthy Adult Population in Pakistan: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 531. [Google Scholar] [CrossRef] [PubMed]
- Sundarakumar, J.S.; Stezin, A.; Menesgere, A.L.; Ravindranath, V. Rural-urban and gender differences in metabolic syndrome in the aging population from southern India: Two parallel, prospective cohort studies. EClinicalMedicine 2022, 47, 101395. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Miah, R.; Hasan, M.; Barman, Z.; Mou, A.D.; Hafsa, J.M.; Das Trisha, A.; Hasan, A.; Islam, F. Association between serum uric acid and metabolic syndrome: A cross-sectional study in Bangladeshi adults. Sci. Rep. 2020, 10, 7841. [Google Scholar] [CrossRef] [PubMed]
- Subramani, S.K.; Mahajan, S.; Chauhan, P.; Yadav, D.; Mishra, M.; Pakkirisamy, U.; Prasad, G. Prevalence of metabolic syndrome in Gwalior region of Central India: A comparative study using NCEP ATP III, IDF and Harmonized criteria. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 816–821. [Google Scholar] [CrossRef] [PubMed]
- De Silva, S.T.; Niriella, M.A.; Ediriweera, D.S.; Kottahachchi, D.; Kasturiratne, A.; de Silva, A.P.; Dassanayaka, A.S.; Pathmeswaran, A.; Wickramasinghe, R.; Kato, N.; et al. Incidence and risk factors for metabolic syndrome among urban, adult Sri Lankans: A prospective, 7-year community cohort, follow-up study. Diabetol. Metab. Syndr. 2019, 11, 66. [Google Scholar] [CrossRef] [PubMed]
- Mehata, S.; Shrestha, N.; Mehta, R.K.; Bista, B.; Pandey, A.R.; Mishra, S.R. Prevalence of the metabolic syndrome and its determinants among Nepalese adults: Findings from a nationally representative cross-sectional study. Sci. Rep. 2018, 8, 14995. [Google Scholar] [CrossRef] [Green Version]
- Sinha, S.; Misra, P.; Kant, S.; Krishnan, A.; Nongkynrih, B.; Vikram, N.K. Prevalence of metabolic syndrome and its selected determinants among urban adult women in South Delhi, India. Postgrad. Med. J. 2013, 89, 68–72. [Google Scholar] [CrossRef]
- Mehta, A.; Singh, S.; Saeed, A.; Mahtta, D.; Bittner, V.A.; Sperling, L.S.; Virani, S.S. Pathophysiological Mechanisms Underlying Excess Risk for Diabetes and Cardiovascular Disease in South Asians: The Perfect Storm. Curr. Diabetes Rev. 2021, 17, e070320183447. [Google Scholar] [CrossRef]
- Satija, A.; Hu, F.B.; Bowen, L.; Bharathi, A.V.; Vaz, M.; Prabhakaran, D.; Reddy, K.S.; Ben-Shlomo, Y.; Smith, G.D.; Kinra, S.; et al. Dietary patterns in India and their association with obesity and central obesity. Public Health Nut. 2015, 18, 3031–3041. [Google Scholar] [CrossRef] [Green Version]
- Safdar, N.F.; Bertone-Johnson, E.; Cordeiro, L.; Jafar, T.H.; Cohen, N.L. Dietary patterns of Pakistani adults and their associations with sociodemographic, anthropometric and life-style factors. J. Nutr. Sci. 2014, 2, e42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misra, A.; Khurana, L.; Isharwal, S.; Bhardwaj, S. South Asian diets and insulin resistance. Br. J. Nutr. 2009, 101, 465–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohan, V.; Radhika, G.; Sathya, R.M.; Tamil, S.R.; Ganesan, A.; Sudha, V. Dietary carbohydrates, glycemic load, food groups and newly detected type 2 diabetes among urban Asian Indian population in Chennai, India (Chennai Urban Rural Epidemiology Study 59). Br. J. Nutr. 2009, 102, 1498–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranasinghe, C.D.; Ranasinghe, P.; Jayawardena, R.; Misra, A. Physical activity patterns among South-Asian adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AAnand, S.S.; Hawkes, C.; de Souza, R.J.; Mente, A.; Dehghan, M.; Nugent, R.; Zulyniak, M.A.; Weis, T.; Bernstein, A.M.; Krauss, R.M. Food Consumption and its Impact on Cardiovascular Disease: Importance of Solutions Focused on the Globalized Food System: A Report From the Work-shop Convened by the World Heart Federation. J. Am. Coll. Cardiol. 2015, 66, 1590–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hills, A.P.; Arena, R.; Khunti, K.; Yajnik, C.S.; Jayawardena, R.; Henry, C.J.; Street, S.J.; Soares, M.J.; Misra, A. Epidemiology and determinants of type 2 diabetes in south Asia. Lancet Diabetes Endocrinol. 2018, 26, 966–978. [Google Scholar] [CrossRef]
- Cosselman, K.E.; Navas-Acien, A.; Kaufman, J.D. Environmental factors in cardiovascular disease. Nat. Rev. Cardiol. 2015, 12, 627–642. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.D.; Kooner, I.; Steptoe, A.; Kooner, J.S. Psychosocial factors related to cardiovascular disease risk in UK South Asian men: A preliminary study. Br. J. Health Psychol. 2007, 12, 559–570. [Google Scholar] [CrossRef]
- Patel, D.; Winterbotham, M.; Britt, R.; Sutton, G.; Bhatnagar, D.; Mackness, M.; Creed, F.; Tomenson, B.; Durrington, P.; Anand, I.; et al. Coronary risk factors in people from the Indian subcontinent living in west London and their siblings in India. Lancet 1995, 345, 405–409. [Google Scholar] [CrossRef]
- Patel, J.; Vyas, A.; Cruickshank, J.; Prabhakaran, D.; Hughes, E.; Reddy, K.; Mackness, M.; Bhatnagar, D.; Durrington, P. Impact of migration on coronary heart disease risk factors: Comparison of Gujaratis in Britain and their contemporaries in villages of origin in India. Atherosclerosis 2006, 185, 297–306. [Google Scholar] [CrossRef]
- Zahid, N.; Meyer, H.E.; Kumar, B.N.; Claussen, B.; Hussain, A. High levels of cardiovascular risk factors among Pakistanis in Norway compared to Pakistanis in Pakistan. J. Obes. 2011, 2011, 163749. [Google Scholar] [CrossRef] [PubMed]
- Tennakoon, S.U.; Kumar, B.N.; Nugegoda, D.B.; Meyer, H.E. Comparison of cardiovascular risk factors between Sri Lankans living in Kandy and Oslo. BMC Public Health 2010, 10, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gujral, U.P.; Narayan, K.V.; Pradeepa, R.G.; Deepa, M.; Ali, M.K.; Anjana, R.M.; Kandula, N.R.; Mohan, V.; Kanaya, A.M. Comparing Type 2 Diabetes, Prediabetes, and Their Associated Risk Factors in Asian Indians in India and in the U.S.: The CARRS and MASALA Studies. Diabetes Care 2015, 38, 1312–1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez, R.; Miranda, C.; Everett, B. Prevalence of obesity among migrant Asian Indians: A systematic review and meta-analysis. Int. J. Evid.-Based Health 2011, 9, 420–428. [Google Scholar] [CrossRef]
- Gujral, U.P.; Pradeepa, R.; Weber, M.B.; Narayan, K.V.; Mohan, V. Type 2 diabetes in South Asians: Similarities and differences with white Caucasian and other populations. Ann. N. Y. Acad. Sci. 2013, 1281, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Misra, A.; Khurana, L. Obesity-related non-communicable diseases: South Asians vs White Caucasians. Int. J. Obes. 2010, 35, 167–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guettier, J.-M.; Georgopoulos, A.; Tsai, M.Y.; Radha, V.; Shanthirani, S.; Deepa, R.; Gross, M.; Rao, G.H.; Mohan, V. Polymorphisms in the Fatty Acid-Binding Protein 2 and Apolipoprotein C-III Genes Are Associated with the Metabolic Syndrome and Dyslipidemia in a South Indian Population. J. Clin. Endocrinol. Metab. 2005, 90, 1705–1711. [Google Scholar] [CrossRef] [Green Version]
- Vimaleswaran, K.S.; Radha, V.; Mohan, V. Thr54 allele carriers of the Ala54Thr variant of FABP2 gene have associations with metabolic syndrome and hypertriglyceridemia in urban South Indians. Metabolism 2006, 55, 1222–1226. [Google Scholar] [CrossRef]
- Naran, N.H.; Chetty, N.; Crowther, N.J. The influence of metabolic syndrome components on plasma PAI-1 concentrations is modified by the PAI-1 4G/5G genotype and ethnicity. Atherosclerosis 2008, 196, 155–163. [Google Scholar] [CrossRef]
- Bajaj, H.; Pereira, M.; Anjana, R.M.; Deepa, R.; Mohan, V.; Mueller, N.; Rao, G.; Gross, M. Uncoupling protein 2 promoter polymorphism -866G/A, central adiposity, and metabolic syndrome in Asians. Obesity 2006, 14, 656–661. [Google Scholar]
- Zabaneh, D.; Balding, D.J. A Genome-Wide Association Study of the Metabolic Syndrome in Indian Asian Men. PLoS ONE 2010, 5, e11961. [Google Scholar] [CrossRef] [Green Version]
- Dodani, S.; Henkhaus, R.; Dong, L.; Butler, M.G. Apo lipoprotein A1 gene polymorphisms predict cardio-metabolic risk in South Asian immigrants. Dis. Markers 2012, 32, 9–19. [Google Scholar] [CrossRef]
- Lear, S.A.; Humphries, K.H.; Hage-Moussa, S.; Chockalingam, A.; Mancini, G.B.J. Immigration presents a potential increased risk for atherosclerosis. Atherosclerosis 2009, 205, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Class, M.; Castro, F.G.; Ramirez, A.G. Conceptions of acculturation: A review and statement of critical issues. Soc. Sci. Med. 2011, 72, 1555–1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Escamilla, R.; Putnik, P. The Role of Acculturation in Nutrition, Lifestyle, and Incidence of Type 2 Diabetes among Latinos. J. Nutr. 2007, 137, 860–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazuda, H.P.; Haffner, S.M.; Stern, M.P.; Eifler, C.W. Effects of Acculturation and Socioeconomic Status on Obesity and Diabetes in Mexican Americans: The San Antonio Heart Study. Am. J. Epidemiol. 1988, 128, 1289–1301. [Google Scholar] [CrossRef] [PubMed]
- Kandula, N.R.; Diez-Roux, A.V.; Chan, C.; Daviglus, M.L.; Jackson, S.A.; Ni, H.; Schreiner, P.J. Association of Acculturation Levels and Prevalence of Diabetes in the Multi-Ethnic Study of Atherosclerosis (MESA). Diabetes Care 2008, 31, 1621–1628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lutsey, P.L.; Roux, A.V.D.; Jacobs, D.R.; Burke, G.L.; Harman, J.; Shea, S.; Folsom, A.R. Associations of Acculturation and Socioeconomic Status With Subclinical Cardiovascular Disease in the Multi-Ethnic Study of Atherosclerosis. Am. J. Public Health 2008, 98, 1963–1970. [Google Scholar] [CrossRef]
- O’Brien, M.J.; Alos, V.A.; Davey, A.; Bueno, A.; Whitaker, R.C. Acculturation and the Prevalence of Diabetes in US Latino Adults, National Health and Nutrition Examination Survey 2007–2010. Prev. Chronic Dis. 2014, 11, E176. [Google Scholar] [CrossRef] [Green Version]
- Satia-Abouta, J.; Patterson, R.E.; Neuhouser, M.L.; Elder, J. Dietary acculturation: Applications to nutrition research and dietetics. J. Am. Diet. Assoc. 2002, 102, 1105–1118. [Google Scholar] [CrossRef]
- Lesser, I.A.; Gasevic, D.; Lear, S.A. The Association between Acculturation and Dietary Patterns of South Asian Immigrants. PLoS ONE 2014, 9, e88495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talegawkar, S.A.; Kandula, N.R.; Gadgil, M.D.; Desai, D.; Kanaya, A.M. Dietary intakes among South Asian adults differ by length of residence in the USA. Public Health Nutr. 2015, 19, 348–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhupathiraju, S.N.; Guasch-Ferré, M.; Gadgil, M.D.; Newgard, C.B.; Bain, J.R.; Muehlbauer, M.J.; Ilkayeva, O.R.; Scholtens, D.M.; Hu, F.B.; Kanaya, A.M.; et al. Dietary Patterns among Asian Indians Living in the United States Have Distinct Metabolomic Profiles That Are Associated with Cardiometabolic Risk. J. Nutr. 2018, 148, 1150–1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garduno-Diaz, S.D.; Khokhar, S. South Asian dietary patterns and their association with risk factors for the metabolic syndrome. J. Hum. Nutr. Diet. 2013, 26, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Gadgil, M.D.; Anderson, C.A.; Kandula, N.R.; Kanaya, A.M. Dietary Patterns Are Associated with Metabolic Risk Factors in South Asians Living in the United States. J. Nutr. 2015, 145, 1211–1217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadgil, M.D.; Anderson, C.A.; Kandula, N.R.; Kanaya, A.M. Dietary patterns in Asian Indians in the United States: An analysis of the Metabolic Syndrome and Atherosclerosis in South Asians Living in America (MASALA) study. J. Acad. Nutr. Diet. 2014, 114, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.D.; Vittinghoff, E.; Kandula, N.R.; Srivastava, S.; Kanaya, A.M. Correlates of prediabetes and type II diabetes in US South Asians: Findings from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) study. Ann. Epidemiol. 2015, 25, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.A.; Jackson, R.T. Polyunsaturated fatty acids, inflammation, and metabolic syndrome in South Asian Americans in Maryland. Food Sci. Nutr. 2018, 6, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Goel, M.S.; McCarthy, E.P.; Phillips, R.S.; Wee, C.C. Obesity among US immigrant subgroups by duration of residence. JAMA 2004, 292, 2860–2867. [Google Scholar] [CrossRef] [Green Version]
- Bharmal, N.; Kaplan, R.M.; Shapiro, M.F.; Mangione, C.M.; Kagawa-Singer, M.; Wong, M.D.; McCarthy, W.J. The Association of Duration of Residence in the United States with Cardiovascular Disease Risk Factors Among South Asian Immigrants. J. Immigr. Minor. Health 2014, 17, 781–790. [Google Scholar] [CrossRef] [Green Version]
- Wang, E.T.; De Koning, L.; Kanaya, A.M. Higher protein intake is associated with diabetes risk in South Asian Indians: The Metabolic Syndrome and Atherosclerosis in South Asians Living in America (MASALA) study. J. Am. Coll. Nutr. 2010, 29, 130–135. [Google Scholar] [CrossRef] [Green Version]
- Wandel, M.; Råberg, M.; Kumar, B.; Holmboe-Ottesen, G. Changes in food habits after migration among South Asians settled in Oslo: The effect of demographic, socio-economic and integration factors. Appetite 2008, 50, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J. BMI-related errors in the measurement of obesity. Int. J. Obes. 2008, 32, S56–S59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, A.; Stanforth, P.; Gagnon, J.; Rankinen, T.; Leon, A.; Rao, D.; Skinner, J.; Bouchard, C.; Wilmore, J. The effect of sex, age and race on estimating percentage body fat from body mass index: The Heritage Family Study. Int. J. Obes. 2002, 26, 789–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donini, L.M.; Pinto, A.; Giusti, A.M.; Lenzi, A.; Poggiogalle, E. Obesity or BMI Paradox? Beneath the Tip of the Iceberg. Front. Nutr. 2020, 7, 53. [Google Scholar] [CrossRef]
- Deurenberg, P.; Andreoli, A.; Borg, P.; Kukkonen-Harjula, K.; de Lorenzo, A.; Lichtenbelt, W.V.M.; Testolin, G.; Vigano, R.; Vollaard, N. The validity of predicted body fat percentage from body mass index and from impedance in samples of five European populations. Eur. J. Clin. Nutr. 2001, 55, 973–979. [Google Scholar] [CrossRef] [Green Version]
- Daniel, M.; Wilbur, J. Physical Activity Among South Asian Indian Immigrants: An Integrative Review. Public Health Nurs. 2011, 28, 389–401. [Google Scholar] [CrossRef]
- Walker, G.J.; Caperchione, C.M.; Mummery, W.K.; Chau, S. Examining the role of acculturation in the leisure-time physical activity of South Asians living in Canada. J. Sci. Med. Sport 2015, 18, 156–160. [Google Scholar] [CrossRef]
- Kolt, G.S.; Schofield, G.M.; Rush, E.C.; Oliver, M.; Chadha, N.K. Body fatness, physical activity, and nutritional behaviors in Asian Indian immigrants to New Zealand. Asia Pacific J. Clin. Nutr. 2007, 16, 663–670. [Google Scholar]
- Misra, A.; Alappan, N.K.; Vikram, N.K.; Goel, K.; Gupta, N.; Mittal, K.; Bhatt, S.; Luthra, K. Effect of Supervised Progressive Resistance-Exercise Training Protocol on Insulin Sensitivity, Glycemia, Lipids, and Body Composition in Asian Indians With Type 2 Diabetes. Diabetes Care 2008, 31, 1282–1287. [Google Scholar] [CrossRef] [Green Version]
- Fischbacher, C.M.; Hunt, S.; Alexander, L. How physically active are South Asians in the United Kingdom? A literature review. J. Public Health 2004, 26, 250–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rush, E.C.; Chandu, V.; Plank, L.D. Reduction of abdominal fat and chronic disease factors by lifestyle change in migrant Asian Indians older than 50 years. Asia Pac. J. Clin. Nutr. 2007, 16, 671–676. [Google Scholar] [PubMed]
- Brown, T.; Smith, S.; Bhopal, R.; Kasim, A.; Summerbell, C. Diet and Physical Activity Interventions to Prevent or Treat Obesity in South Asian Children and Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2015, 12, 566–594. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.A.; Gowda, U.; Smith, B.J.; Renzaho, A.M.N. Systematic Review of the Effect of Lifestyle Interventions on the Components of the Metabolic Syndrome in South Asian Migrants. J. Immigr. Minor. Health 2016, 20, 231–244. [Google Scholar] [CrossRef] [PubMed]
- Kanaya, A.M.; Araneta, M.R.G.; Pawlowsky, S.B.; Barrett-Connor, E.; Grady, D.; Vittinghoff, E.; Schembri, M.; Chang, A.; Carrion-Petersen, M.L.; Coggins, T.; et al. Restorative yoga and metabolic risk factors: The Practicing Restorative Yoga vs. Stretching for the Metabolic Syndrome (PRYSMS) randomized trial. J. Diabetes Complicat. 2013, 28, 406–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, E.; Høstmark, A.T.; Anderssen, S.A. Effect of a Physical Activity Intervention on the Metabolic Syndrome in Pakistani Immigrant Men: A Randomized Controlled Trial. J. Immigr. Minor. Health 2012, 14, 738–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Telle-Hjellset, V.; Kjøllesdal MK, R.; Bjørge, B.; Holmboe-Ottesen, G.; Wandel, M.; Birkeland, K.I.; Eriksen, H.; Høstmark, A.T. The InnvaDiab-DE-PLAN study: A randomized controlled trial with a culturally adapted education program for improving the risk profile for type 2 diabetes in Pakistani immigrant women. Br. J. Nutr. 2013, 109, 529–538. [Google Scholar] [CrossRef] [Green Version]
- Kousar, R.; Burns, C.; Lewandowski, P. A culturally appropriate diet and lifestyle intervention can successfully treat the components of metabolic syndrome in female Pakistani immigrants residing in Melbourne, Australia. Metabolism 2008, 57, 1502–1508. [Google Scholar] [CrossRef]
- Mohan, V.; Gayathri, R.; Jaacks, L.M.; Lakshmipriya, N.; Anjana, R.M.; Spiegelman, D.; Jeevan, R.G.; Balasubramaniam, K.K.; Shobana, S.; Jayanthan, M.; et al. Cashew Nut Consumption Increases HDL Cholesterol and Reduces Systolic Blood Pressure in Asian Indians with Type 2 Diabetes: A 12-Week Randomized Controlled Trial. J. Nutr. 2018, 148, 63–69. [Google Scholar] [CrossRef] [Green Version]
- Gulati, S.; Misra, A.; Pandey, R.M.; Bhatt, S.P.; Saluja, S. Effects of pistachio nuts on body composition, metabolic, inflammatory and oxidative stress parameters in Asian Indians with metabolic syndrome: A 24-wk, randomized control trial. Nutrition 2014, 30, 192–197. [Google Scholar] [CrossRef]
- Roberts, C.K.; Hevener, A.L.; Barnard, R.J. Metabolic Syndrome and Insulin Resistance: Underlying Causes and Modification by Exercise Training. Compr. Physiol. 2013, 3, 158. [Google Scholar] [CrossRef] [Green Version]
- Volgman, A.S.; Palaniappan, L.S.; Aggarwal, N.T.; Gupta, M.; Khandelwal, A.; Krishnan, A.V.; Lichtman, J.H.; Mehta, L.S.; Patel, H.N.; Shah, K.S.; et al. Atherosclerotic Cardiovascular Disease in South Asians in the United States: Epidemiology, Risk Factors, and Treatments: A Scientific Statement From the American Heart Association. Circulation 2018, 138, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Nair, M.; Ali, M.K.; Ajay, V.S.; Shivashankar, R.; Mohan, V.; Pradeepa, R.; Deepa, M.; Khan, H.M.; Kadir, M.M.; Fatmi, Z.A.; et al. CARRS Surveillance study: Design and methods to assess burdens from multiple perspectives. BMC Public Health 2012, 12, 701. [Google Scholar] [CrossRef] [Green Version]
- Gujral, U.P.; Kanaya, A.M. Epidemiology of diabetes among South Asians in the United States: Lessons from the MASALA study. Ann. N. Y. Acad. Sci. 2020, 1495, 24–39. [Google Scholar] [CrossRef]
- Bajaj, M.; Banerji, M.A. Type 2 diabetes in South Asians: A pathophysiologic focus on the Asian-Indian epidemic. Curr. Diabetes Rep. 2004, 4, 213–218. [Google Scholar] [CrossRef]
- Enas, E.A.; Mohan, V.; Deepa, M.; Farooq, S.; Pazhoor, S.; Chennikkara, H. The Metabolic Syndrome and Dyslipidemia Among Asian Indians: A Population With High Rates of Diabetes and Premature Coronary Artery Disease. J. Cardiometab. Syndr. 2007, 2, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.; Ashcraft, A. Type 2 Diabetes Risk among Asian Indians in the US: A Pilot Study. Nurs. Res. Pr. 2013, 2013, 492893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savadatti, S.S.; Bell, E.M.; Gates, M.A.; Hosler, A.; Yucel, R.M.; Misra, R. Metabolic Syndrome Among Asian Indians in the United States. J. Public Health Manag. Pr. 2019, 25, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, U.; Fatma, M.; Mohan, S.; Singh, P.; Misra, A. Randomized Control Trial for Reduction of Body Weight, Body Fat Patterning, and Cardiometabolic Risk Factors in Overweight Worksite Employees in Delhi, India. J. Diabetes Res. 2017, 2017, 7254174. [Google Scholar] [CrossRef] [Green Version]
- Anjana, R.M.; Pradeepa, R.; Das, A.K.; Deepa, M.; Bhansali, A.; Joshi, S.R.; Joshi, P.P.; Dhandhania, V.K.; Rao, P.V.; Sudha, V.; et al. Physical activity and inactivity patterns in India—results from the ICMR-INDIAB study (Phase-1) [ICMR-INDIAB-5]. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 26. [Google Scholar] [CrossRef] [Green Version]
- Manchanda, S.C.; Mehrotra, U.C.; Makhija, A.; Mohanty, A.; Dhawan, S.; Sawhney, J.P.S. Reversal of early atherosclerosis in metabolic syndrome by yoga-a randomized controlled trial. J. Yoga Phys. Ther. 2013, 3, 1. [Google Scholar]
- Dodani, S.; Henkhaus, R.; Wick, J.; Vacek, J.; Gupta, K.; Dong, L.; Butler, M.G. Metabolic syndrome in South Asian immigrants: More than low HDL requiring aggressive management. Lipids Health Dis. 2011, 10, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, W.C.; Araneta, M.R.G.; Kanaya, A.M.; Chiang, J.L.; Fujimoto, W. BMI Cut Points to Identify At-Risk Asian Americans for Type 2 Diabetes Screening. Diabetes Care 2015, 38, 150–158. [Google Scholar] [CrossRef] [Green Version]
- Khunti, K.; Taub, N.; Tringham, J.; Jarvis, J.; Farooqi, A.; Skinner, T.C.; Davies, M.J. Screening for the metabolic syndrome using simple anthropometric measurements in south Asian and white Europeans: A population-based screening study. The Leicester Ethnic Atherosclerosis and Diabetes Risk (LEADER) Study. Prim. Care Diabetes 2010, 4, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Cross-Bardell, L.; George, T.; Bhoday, M.; Tuomainen, H.; Qureshi, N.; Kai, J. Perspectives on enhancing physical activity and diet for health promotion among at-risk urban UK South Asian communities: A qualitative study. BMJ Open 2015, 5, e007317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, S.R.; Ghimire, S.; Joshi, C.; Gyawali, B.; Shrestha, A.; Neupane, D.; Sharma, S.R.; Pokharel, Y.; Virani, S.S. Cardio-metabolic disease risk factors among South Asian labour migrants to the Middle East: A scoping review and policy analysis. Glob. Health 2019, 15, 33. [Google Scholar] [CrossRef]
- Health Development Agency. Black and Minority Ethnic Groups in England: The Second Health and Lifestyles Survey; Health Education Authority: London, UK, 2000. [Google Scholar]
- Stanner, S. Health Survey for England 1999: The health of minority ethnic groups. Nutr. Bull. 2001, 26, 227–230. [Google Scholar] [CrossRef]
- Vasudevan, D.; Stotts, A.; Anabor, O.L.; Mandayam, S. Primary Care Physician’s Knowledge of Ethnicity-Specific Guidelines for Obesity Diagnosis and Readiness for Obesity Intervention Among South Asian Indians. J. Immigr. Minor. Health 2011, 14, 759–766. [Google Scholar] [CrossRef]
- Bodicoat, D.H.; Gray, L.J.; Henson, J.; Webb, D.; Guru, A.; Misra, A.; Gupta, R.; Vikram, N.; Sattar, N.; Davies, M.; et al. Body Mass Index and Waist Circumference Cut-Points in Multi-Ethnic Populations from the UK and India: The ADDITION-Leicester, Jaipur Heart Watch and New Delhi Cross-Sectional Studies. PLoS ONE 2014, 9, e90813. [Google Scholar] [CrossRef] [Green Version]
- Celis-Morales, C.A.; Ghouri, N.; Bailey, M.E.; Sattar, N.; Gill, J.M. Should physical activity recommendations be ethnicity-specific?: Evidence from a cross-sectional study of South Asian and European men. PLoS ONE 2013, 8, e82568. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Hochberg, M.C.; Chang, R.W.; Hootman, J.M.; Manheim, L.M.; Lee, J.; Semanik, P.A.; Sharma, L.; Dunlop, R.D. Osteoarthritis Initiative Investigators Racial and ethnic differences in physical activity guidelines attainment among people at high risk of or having knee osteoarthritis. Arthritis Care Res. 2012, 65, 195–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregson, J.; Foerster, S.B.; Orr, R.; Jones, L.; Benedict, J.; Clarke, B.; Hersey, J.; Lewis, J.; Zotz, K. System, Environmental, and Policy Changes: Using the Social-Ecological Model as a Framework for Evaluating Nutrition Education and Social Marketing Programs with Low-Income Audiences. J. Nutr. Educ. 2001, 33, S4–S15. [Google Scholar] [CrossRef] [PubMed]
- Kumanyika, S.K.; Morssink, C.B. Bridging domains in efforts to reduce disparities in health and health care. Health Educ. Behav. 2006, 33, 440–458. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.P.; Christakis, N.A. Social networks and health. Annu. Rev. Sociol. 2008, 34, 405–429. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Institution, Year | ||||||
|---|---|---|---|---|---|---|
| Consensus definition, developed by IDF and AHA/NHLBI, 2009 | IDF, 2005 | AHA/NHLBI, 2004 | NCEP ATP III, 2001 | EGIR, 1999 | WHO, 1998 | |
| BMI | N/A | ≥30 kg/m2 | N/A | ≥25 kg/m2 | N/A | ≥30 kg/m2 |
| Central Obesity | WC cutoffs specific to the ethnicity being developed, currently using IDF criteria | WC for European: ≥94 cm (men) ≥80 cm (women) WC for Asian: ≥90 cm (men) ≥80 cm (women) | WC for all: ≥102 cm (men) ≥88 cm (women) | WC for all: ≥102 cm (men) ≥88 cm (women) | WC for all: ≥94 cm (men) ≥80 cm (women) | WHR ≥0.90 (men) ≥0.85 (women) |
| Fasting Glucose | ≥100 mg/dL | ≥100 mg/dL | ≥100 mg/dL | ≥110 mg/dL | ≥110 mg/dL | ≥100 mg/dL (as criteria for IR) |
| TGL | ≥150 mg/dL | ≥150 mg/dL | ≥150 mg/dL | ≥150 mg/dL | ≥150 mg/dL | ≥150 mg/dL |
| HDL-C | <40 mg/dL (men) <50 mg/dL (women) | <40 mg/dL (men) <50 mg/dL (women) | <40 mg/dL (men) <50 mg/dL (women) | <40 mg/dL (men) <50 mg/dL (women) | <39 mg/dL | <40 mg/dL (men) <50 mg/dL (women) |
| Blood Pressure | ≥130/85 mm Hg | ≥130/85 mm Hg | ≥130/85 mm Hg | ≥130/85 mm Hg | ≥140/90 mm Hg, or hypertensive drug usage | ≥140/90 mm Hg |
| Author, Year (SA Group Studied) | Non-Native Country | Criteria Used | Prevalence |
|---|---|---|---|
| Khan et al., 2016 (Pakistan, India, Bangladesh, Nepal, Iran, Sri Lanka, Afghanistan, Bhutan) | US | Modified harmonized definition by IDF and NHLBI | 47%; Highest prevalence among Bangladeshi men |
| Garduno-Diaz et al., 2013 (India, Pakistan) | UK | IDF | 20% |
| Andersen et al., 2012 (Pakistan) | Norway | IDF | 47–51% |
| Dodani et al., 2011 (India) | US | IDF, WHO, NCEP ATP III, | 29.7% (IDF), 13.3% (WHO), 40% (NCEP ATP III) |
| Flowers et al., 2010 (India, Pakistan, Sri Lanka) | US | IDF | 27%; Prevalence significantly higher in men (31%) than in women (17%) |
| Misra et al., 2010 (India) | US | IDF, NCEP ATP III | 37.6% (IDF), 32.4% (NCEP ATP III); Prevalence significantly increased with age in women, but not with men |
| Telle-Hjellset et al., 2010 (Pakistan) | Norway | IDF | 41% |
| Rianon et al., 2009 (Bangladesh) | US | Modified AHA/NHLBI | 38% |
| Balusubramanyam et al., 2008 (India) | US | NCEP ATP III | 32%; Prevalence was higher in the older population |
| Ajjan et al., 2007 (India, Pakistan, Bangladesh) | US | IDF | 39%; Prevalence was significantly higher compared to those of Caucasian descent |
| Williams et al., 2007 (India, Pakistan, Bangladesh, Sri Lanka) | UK | NCEP ATP III | 22.2% |
| Forouhi et al., 2006 (India, Pakistan, Bangladesh) | UK | IDF | 44.6%; Prevalence was significantly higher in South Asians compared to Europeans |
| Tillin et al., 2005 (India, Pakistan, Bangladesh) | UK | WHO, NCEP ATP III | 46% Male, 31% Female (WHO), 29% Male, 32% Female (NCEP ATP III); Prevalence, using both criteria, was significantly higher compared to Europeans |
| Misra et al., 2005 (India) | US | NCEP ATP III | 33.9% |
| Anand et al., 2003 (Not specified) | Canada | NCEP ATP III | 25.8%; Prevalence was significantly higher compared to Chinese immigrants, but not those of European descent |
| Author, Year | Native Country | Criteria Used | Prevalence/Contributing Factors |
|---|---|---|---|
| Adil et al., 2023 | Pakistan | NCE ATP III | 28.8% |
| Sundarakumar et al., 2022 | India | NCEP ATP III | 46.2% (rural) 54.8% (urban) |
| Ali et al., 2020 | Bangladesh | NCE ATP III | 22% |
| Subramani et al., 2019 | India | NCE ATP III, IDF | 72.7% (NCEP ATP III) 50.2% (IDF) |
| DeSilva et al., 2019 | Sri Lanka | IDF | 47.2% |
| Mehata et al., 2018 | Nepal | NCE ATP III, IDF | 15% (NCEP ATP III) 16% (IDF) |
| Sinha et al., 2013 | India | NCEP ATP III, IDF | 29.6% (NCEP ATP III) 20.4% (IDF) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahadevan, M.; Bose, M.; Gawron, K.M.; Blumberg, R. Metabolic Syndrome and Chronic Disease Risk in South Asian Immigrants: A Review of Prevalence, Factors, and Interventions. Healthcare 2023, 11, 720. https://doi.org/10.3390/healthcare11050720
Mahadevan M, Bose M, Gawron KM, Blumberg R. Metabolic Syndrome and Chronic Disease Risk in South Asian Immigrants: A Review of Prevalence, Factors, and Interventions. Healthcare. 2023; 11(5):720. https://doi.org/10.3390/healthcare11050720
Chicago/Turabian StyleMahadevan, Meena, Mousumi Bose, Kelly M. Gawron, and Renata Blumberg. 2023. "Metabolic Syndrome and Chronic Disease Risk in South Asian Immigrants: A Review of Prevalence, Factors, and Interventions" Healthcare 11, no. 5: 720. https://doi.org/10.3390/healthcare11050720
APA StyleMahadevan, M., Bose, M., Gawron, K. M., & Blumberg, R. (2023). Metabolic Syndrome and Chronic Disease Risk in South Asian Immigrants: A Review of Prevalence, Factors, and Interventions. Healthcare, 11(5), 720. https://doi.org/10.3390/healthcare11050720