
Violence against Women during the COVID-19 Pandemic in Mexico

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Variables
Household Violence against Women
2.3. Covariates
2.3.1. Sociodemographic Characteristics
2.3.2. COVID-19 Pandemic Variables
2.4. Data Analysis
3. Results
3.1. Sample Characteristics
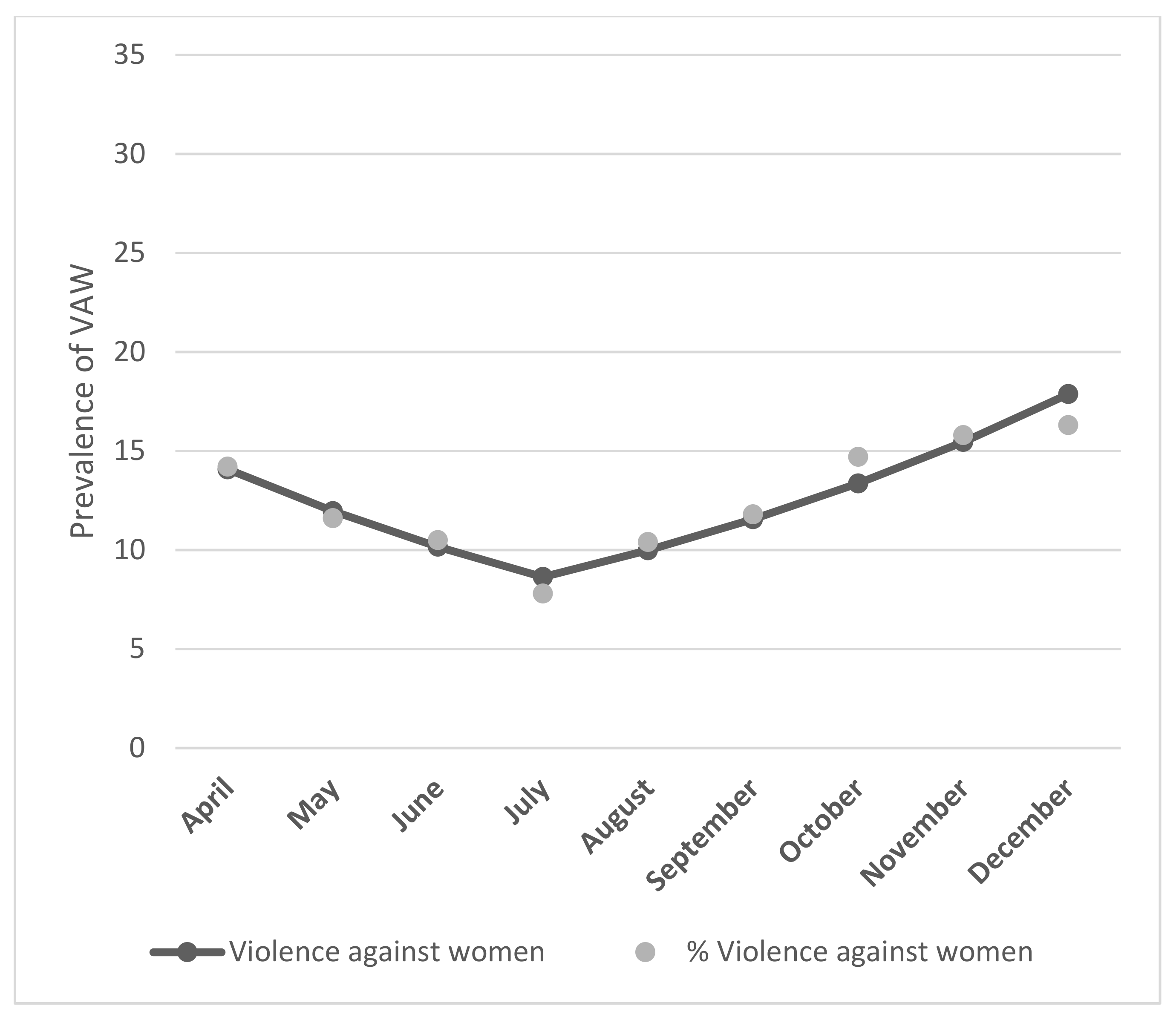
3.2. Prevalence of Violence against Women
3.3. Factors Associated with Household Violence against Women
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nigam, S.; Soperna, N. A study of the understated violence within social contexts against adolescent girls. J. Educ. Cult. Soc. 2017, 8, 29–41. [Google Scholar] [CrossRef]
- Krug, E.G.; Dahlberg, L.L.; Mercy, J.A.; Zwi, A.B.; Lozano, R. (Eds.) World Report on Violence and Health; WHO: Geneva, Switzerland, 2002; Available online: https://apps.who.int/iris/bitstream/handle/10665/42495/9241545615_eng.pdf (accessed on 22 January 2022).
- World Health Organization. Global Status Report on Violence; WHO: Washington, DC, USA, 2014; Available online: https://www.who.int/publications/i/item/9789241564793 (accessed on 5 October 2021).
- De Mendonça, M.F.S.; Ludermir, A.B. Intimate partner violence and incidence of common mental disorder. Rev. Saúde Pública 2017, 51, 32. [Google Scholar] [CrossRef]
- World Health Organization; London School of Hygiene and Tropical Medicine. Preventing Intimate Partner and Sexual Violence against Women: Taking Action and Generating Evidence; World Health Organization: Genava, Switzerland; London School of Hygiene and Tropical Medicine: London, UK, 2010. [Google Scholar]
- García-Moreno, C.; Watts, C. Violence against women: An urgent public health priority. Bull. World Health Org. 2011, 89, 2. [Google Scholar] [CrossRef]
- Naudi, M. For Many Women and Children, the Home is not a Safe Place Statement by the President of GREVIO, Istanbul Convention, Action against Violence against Women and Domestic Violence; Istanbul Convention: Istanbul, Turkey, 2020. [Google Scholar]
- Mojahed, A.; Alaidarous, N.; Shabta, H.; Hegewald, J.; Garhus-Niegel, S. Intimate partner violence against women in the Arab countries: A systematic review of risk factors. Trauma Violence Abuse 2022, 23, 390–407. [Google Scholar] [CrossRef]
- Marques, E.S.; Moraes, C.L.; Hasselmann, M.H.; Deslandes, S.F.; Reichenheim, M.E. A violência contra mulheres, crianças e adolescentes em tempos de pandemia pela COVID-19: Panorama, motivações e formas de enfrentamento. Cad Saúde Pública 2020, 36, e00074420. [Google Scholar] [CrossRef]
- Bourgault, S.; Peterman, A.; O’Donnell, M. Violence against Women and Children During COVID-19—One Year on and 100 Papers in; Center for Global Development: Washington, DC, USA, 2021. [Google Scholar]
- Mannell, J.; Lowe, H.; Brown, L.; Mukerji, R.; Devakumar, D.; Gram, L.; Jansen, H.A.F.M.; Minckas, N.; Osrin, D.; Prost, A.; et al. Risk factors for violence against women in high-prevalence settings: A mixed-methods systematic review and meta-synthesis. BMJ Glob. Health 2022, 7, e007704. [Google Scholar] [CrossRef] [PubMed]
- Rennison, C.M.; DeKeseredy, W.S.; Dragiewicz, M. Intimate relationship status variations in violence against women: Urban, suburban, and rural differences. Violence Women 2013, 19, 1312–1330. [Google Scholar] [CrossRef] [PubMed]
- OAS/MESECVI. Violence against Women and the Measures to Contain the Spread of COVID-19. 2020. Available online: https://www.oas.org/es/cim/docs/COVID-19-RespuestasViolencia-EN.pdf (accessed on 5 October 2021).
- Taub, A. A new COVID-19 crisis: Domestic abuse rises worldwide. The New York Times, 6 April 2020. Available online: https://www.nytimes.com/2020/04/06/world/coronavirus-domestic-violence.html(accessed on 5 October 2021).
- International Rescue Committee. Everything on Her Shoulders: Rapid Assessment on Gender and Violence against Women and Girls in the Ebola Outbreak in Beni, DRC. 2019. Available online: https://www.rescue.org/report/everythingher-shoulders-rapid-assessment-gender-andviolence-against-women-and-girls-ebola (accessed on 5 October 2021).
- Akel, M.; Berro, J.; Rahme, C.; Obeid, S.; Hallit, S. Violence against women during COVID-19 pandemic. J. Interpers. Violence 2022, 37, NP12284–NP12309. [Google Scholar] [CrossRef]
- Campbell, A.M. An increasing risk of family violence during the COVID-19 pandemic: Strengthening community collaborations to save lives. Forensic Sci. Int. Rep. 2020, 2, 100089. [Google Scholar] [CrossRef]
- Jetelina, K.K.; Knell, G.; Molsberry, R.J. Changes in intimate partner violence during the early stages of the COVID-19 pandemic in the USA. Inj. Prev. 2021, 27, 93–97. [Google Scholar] [CrossRef]
- Valdez-Santiago, R.; Villalobos-Hernández, A.; Arenas-Monreal, L.; Flores, K.; Ramos-Lira, L. Violencia en el hogar contra mujeres adultas durante el confinamiento por la pandemia de COVID-19 en México. Salud Publica Mex. 2021, 63, 782–788. [Google Scholar] [CrossRef] [PubMed]
- INEGI; ENDIREH Nacional. Violencia Contra las Mujeres en México. Encuesta Nacional Sobre la Dinámica de las Relaciones en los Hogares 2021. 2022. Available online: https://www.inegi.org.mx/programas/endireh/2021/ (accessed on 16 October 2022).
- Chainé, S.M.; Montoya, A.L.; Maldonado, A.B.; Aguirre, A.B.; García, R.R.; Rubio, C.R.G.; García, C.I.A.; Chávez, I.A.L.; Gómez, M.G.I. Mental Health Symptoms, Binge Drinking, and the Experience of Abuse During the COVID-19 Lockdown in Mexico. Front. Public Health 2021, 9, 979. [Google Scholar] [CrossRef]
- Gillis, D.; Edwards, B.P.M. The utility of joinpoint regression for estimating population parameters given changes in population structure. Heliyon 2019, 5, e02515. [Google Scholar] [CrossRef] [PubMed]
- Secretaría de Salud; Gobierno de México. Lineamientos de Respuesta y de Acción en Salud Mental y Adicciones Para el Apoyo Psicosocial durante la Pandemia por COVID-19 en México; Gobierno de Mexico: Mexico City, Mexico, 2020.
- INEGI; ENDIREH Nacional. Encuesta Nacional Sobre la Dinámica de las Relaciones en Los Hogares 2016. 2017. Available online: https://www.inegi.org.mx/programas/endireh/2016/ (accessed on 16 October 2022).
- Adibelli, D.; Sümen, A.; Teskereci, G. Domestic violence against women during the COVID-19 pandemic: Turkey sample. Health Care Women Int. 2021, 42, 335–350. [Google Scholar] [CrossRef] [PubMed]
- Yari, A.; Zahednezhad, H.; Gheshlagh, R.G.; Kurdi, A. Frequency and determinants of domestic violence against Iranian women during the COVID-19 pandemic: A national cross-sectional survey. BMC Public Health 2021, 21, 1727. [Google Scholar] [CrossRef]
- Walker, L.E. The Battered Women; Harper and Row: Manhattan, NY, USA, 1979. [Google Scholar]
- Øverup, C.S.; DiBello, A.M.; Brunson, J.A.; Acitelli, L.K.; Neighbors, C. Drowning the pain: Intimate partner violence and drinking to cope prospectively predict problem drinking. Addict. Behav. 2015, 41, 152–161. [Google Scholar] [CrossRef]
- Kushnir, V.; Cunningham, J.A. Event-specific drinking in the general population. J. Stud. Alcohol Drugs 2014, 75, 968–972. [Google Scholar] [CrossRef]
- Gebrewahd, G.T.; Gebremeskel, G.G.; Tadesse, D.B. Intimate partner violence against reproductive age women during COVID-19 pandemic in northern Ethiopia 2020: A community-based cross-sectional study. Reprod. Health 2020, 17, 152. [Google Scholar] [CrossRef] [PubMed]
- Abramsky, T.; Watts, C.H.; Garcia-Moreno, C.; Devries, K.; Kiss, L.; Ellsberg, M.; Jansen, H.A.; Heise, L. What factors are associated with recent intimate partner violence? findings from the WHO multi-country study on women’s health and domestic violence. BMC Public Health. 2011, 11, 109. [Google Scholar] [CrossRef]
- Iman’ishimwe Mukamana, J.; Machakanja, P.; Adjei, N.K. Trends in prevalence and correlates of intimate partner violence against women in Zimbabwe, 2005–2015. BMC Int. Health Hum. Rights 2020, 20, 2. [Google Scholar] [CrossRef] [Green Version]
- Peterman, A.; Potts, A.; O’Donnell, M.; Kelly, T.; Shah, N.; Oertelt-Prigione, S. Pandemics and Violence against Women and Children. CGD Working Paper 528; Center for Global Development: Washington, DC, USA, 2020; Available online: https://www.cgdev.org/publication/pandemics-and-violence-against-women-and-children (accessed on 5 November 2021).
- Aizer, A. The Gender Wage Gap and Domestic Violence. Am. Econ. Review. 2010, 100, 1847–1859. [Google Scholar] [CrossRef]
- Pattojoshi, A.; Sidana, A.; Garg, S.; Miishra, S.N.; Singh, L.K.; Goyal, N.; Tikka, S.K. Staying home is NOT ‘staying safe’: A rapid 8-day online survey on spousal violence against women during the COVID-19 lockdown in India. Psychiatr. Clin. Neurosci. 2021, 75, 64–66. [Google Scholar] [CrossRef] [PubMed]
- Mazza, M.; Marano, G.; Lai, C.; Janiri, L.; Sani, G. Danger in danger: Interpersonal violence during COVID-19 quarantine. Psychiatr. Res. 2020, 289, 113046. [Google Scholar] [CrossRef] [PubMed]
- Bradbury-Jones, C.; Isham, L. The pandemic paradox: The consequences of COVID-19 on domestic violence. J. Clin. Nurs. 2020, 29, 2047–2049. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Rivera, L.; Natera-Rey, G.; Séris-Martínez, M.; Leyva-López, A.; Zavala-Arciniega, L.; Ortega-Ceballos, P.A.; Reynales-Shigematsu, L.M. Encodat 2016: Violencia de pareja y uso de tabaco, alcohol y drogas. Nuevos retos para la salud mental. Salud Publica Mex. 2021, 63, 630–640. (In Spanish) [Google Scholar] [CrossRef]
- Nduna, M.; Tshona, S.O. Domesticated Poly-Violence Against Women During the 2020 COVID-19 Lockdown in South Africa. Psychol. Stud. 2021, 66, 347–353. [Google Scholar] [CrossRef]
- Htun, M.; Jensenius, F.R. Expressive Power of Anti-Violence Legislation: Changes in Social Norms on Violence Against Women in Mexico. In World Politics; Cambridge University Press: Cambridge, UK, 2022; Volume 74, pp. 1–36. [Google Scholar] [CrossRef]
- Levandowski, M.L.; Stahnke, D.N.; Munhoz, T.N.; Hohendorff, J.V.; Salvador-Silva, R. Impacto do distanciamento social nas notificações de violência contra crianças e adolescentes no Rio Grande do Sul, Brasil. Cad. Saúde Pública 2021, 37, e00140020. [Google Scholar] [CrossRef]


{kind=link}
| Sociodemographic Variables | na | % |
|---|---|---|
| Age group | ||
| 15–19 | 4848 | 10.1 |
| 20–29 | 12,762 | 26.7 |
| 30–39 | 14,086 | 29.5 |
| 40–49 | 9684 | 20.3 |
| 50 and older | 6439 | 13.5 |
| Educational level | ||
| Junior high school or less | 6021 | 12.6 |
| High School | 13,796 | 28.9 |
| Undergraduate or graduate degree | 28,002 | 58.6 |
| Marital status | ||
| Single | 24,528 | 51.3 |
| Married/domestic partner | 18,534 | 38.8 |
| Separated, widowed, divorced | 4757 | 10.0 |
| COVID-19 pandemic variables | ||
| Employment status | ||
| Unemployed | 13,591 | 28.5 |
| Employed | 34,123 | 71.5 |
| Isolation status | ||
| No | 7698 | 16.1 |
| Partially | 22,446 | 46.9 |
| Yes | 17,675 | 37.0 |
| Caregiver of child | ||
| No | 29,501 | 61.7 |
| Yes | 18,318 | 38.3 |
| Caregiver of elder and/or chronically ill person | ||
| No | 32,535 | 68.0 |
| Caregiver of elder or chronically ill person | 9199 | 19.3 |
| Caregiver of elder and chronically ill person | 6085 | 12.7 |
| Loss of family member due to COVID-19 | ||
| No | 44,874 | 93.8 |
| Yes | 2945 | 6.2 |
| Excessive alcohol use in the past month b | ||
| No | 43,225 | 91.2 |
| Yes | 4150 | 8.8 |
| Prevalence in General Population | 11.5% | ||
|---|---|---|---|
| Sociodemographic Variables | na | % | p-Value |
| Age group | |||
| 15–19 | 767 | 15.8 | <0.001 |
| 20–29 | 1585 | 12.4 | |
| 30–39 | 1450 | 10.3 | |
| 40–49 | 1007 | 10.4 | |
| 50 and older | 687 | 10.7 | |
| Educational level | |||
| Junior high school or less | 598 | 9.9 | <0.001 |
| High School | 1660 | 12.0 | |
| Undergraduate or graduate degree | 3238 | 11.6 | |
| Marital status | |||
| Single | 2774 | 11.3 | 0.086 |
| Married/domestic partner | 2131 | 11.5 | |
| Separated, widowed, divorced | 591 | 12.4 | |
| COVID-19 pandemic variables | |||
| Employment status | |||
| Unemployed | 2411 | 17.8 | <0.001 |
| Employed | 3076 | 9.0 | |
| Isolation status | |||
| No | 557 | 7.2 | <0.001 |
| Partially | 2609 | 11.6 | |
| Yes | 2330 | 13.2 | |
| Caregiver of child | |||
| No | 3212 | 10.9 | <0.001 |
| Yes | 2284 | 12.5 | |
| Caregiver of elder and/or chronically ill person | |||
| No | 3315 | 10.2 | <0.001 |
| Caregiver of elder or chronically ill person | 1274 | 13.9 | |
| Caregiver of elder and chronically ill person | 907 | 14.9 | |
| Loss of family member due to COVID-19 | |||
| No | 5055 | 11.3 | <0.001 |
| Yes | 441 | 15.0 | |
| Excessive alcohol use in the past month b | |||
| No | 4597 | 10.6 | <0.001 |
| Yes | 806 | 19.4 | |
| OR (95% CI) a | OR (95% CI) b | |
|---|---|---|
| Sociodemographic Variables | ||
| Age group | ||
| 50 and older | 1 (reference) | 1 (reference) |
| 15–19 | 1.57 (1.41–1.76) * | 1.40 (1.22–1.60) * |
| 20–29 | 1.19 (1.08–1.31) * | 1.26 (1.13–1.41) * |
| 30–39 | 0.96 (0.87–1.06) | 1.02 (0.92–1.13) |
| 40–49 | 0.97 (0.88–1.08) | 1.00 (0.90–1.11) |
| Educational level | ||
| High school or less | 1 (reference) | 1 (reference) |
| High School | 1.24 (1.12–1.37) * | 1.03 (0.93–1.15) |
| Undergraduate or graduate degree | 1.19 (1.08–1.30) * | 1.08 (0.98–1.20) |
| Marital status | ||
| Single | 1 (reference) | 1 (reference) |
| Married/domestic partner | 1.02 (0.96–1.08) | 1.28 (1.19–1.38) * |
| Separated, widowed, divorced | 1.11 (1.01–1.22) | 1.47 (1.32–1.65) * |
| COVID-19 pandemic variables | ||
| Employment status | ||
| Employed | 1 (reference) | 1 (reference) |
| Unemployed | 2.18 (2.06–2.31) * | 2.01 (1.89–2.16) |
| Isolation status | ||
| No | 1 (reference) | 1 (reference) |
| Partially | 1.69 (1.53–1.86) * | 1.58 (1.43–1.75) * |
| Yes | 1.95 (1.77–2.15) * | 1.47 (1.32–1.63) * |
| Month answered survey c | ||
| July | 1 (reference) | 1 (reference) |
| April | 1.96 (1.76–2.19) * | 1.61 (1.43–1.81) * |
| May | 1.56 (1.40–1.74) * | 1.32 (1.18–1.48) * |
| June | 1.39 (1.25–1.55) * | 1.21 (1.08–1.35) * |
| August | 1.37 (1.22–1.55) * | 1.29 (1.14–1.46) * |
| September | 1.59 (1.40–1.80) * | 1.48 (1.30–1.69) * |
| October | 2.04 (1.80–2.31) * | 1.76 (1.54–2.00) * |
| November | 2.22 (1.93–2.57) * | 1.77 (1.53–2.06) * |
| December | 2.31 (1.91–2.81) * | 1.93 (1.58–2.36) * |
| Caregiver of child | ||
| No | 1 (reference) | 1 (reference) |
| Yes | 1.17 (1.10–1.23) * | 1.27 (1.19–1.36) * |
| Caregiver of elder and/or chronically ill person | ||
| No | 1 (reference) | 1 (reference) |
| Caregiver of elder or chronically ill person | 1.42 (1.32–1.52) * | 1.42 (1.33–1.53) |
| Loss of family member due to COVID-19 d | ||
| No | 1 (reference) | 1 (reference) |
| Yes | 1.39 (1.25–1.54) * | 1.26 (1.13–1.41) |
| Excessive alcohol use in the past month | ||
| No | 1 (reference) | 1 (reference) |
| Yes | 2.03 (1.86–2.20) * | 1.94 (1.78–2.12) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera Rivera, L.; Séris Martínez, M.; Reynales Shigematsu, L.M.; Gómez García, J.A.; Austria Corrales, F.; Toledano-Toledano, F.; Jiménez Tapia, A.; Tejadilla Orozco, D.I.; Astudillo García, C.I. Violence against Women during the COVID-19 Pandemic in Mexico. Healthcare 2023, 11, 419. https://doi.org/10.3390/healthcare11030419
Rivera Rivera L, Séris Martínez M, Reynales Shigematsu LM, Gómez García JA, Austria Corrales F, Toledano-Toledano F, Jiménez Tapia A, Tejadilla Orozco DI, Astudillo García CI. Violence against Women during the COVID-19 Pandemic in Mexico. Healthcare. 2023; 11(3):419. https://doi.org/10.3390/healthcare11030419
Chicago/Turabian StyleRivera Rivera, Leonor, Marina Séris Martínez, Luz Myriam Reynales Shigematsu, José Alberto Gómez García, Fernando Austria Corrales, Filiberto Toledano-Toledano, Alberto Jiménez Tapia, Diana Iris Tejadilla Orozco, and Claudia I. Astudillo García. 2023. "Violence against Women during the COVID-19 Pandemic in Mexico" Healthcare 11, no. 3: 419. https://doi.org/10.3390/healthcare11030419
APA StyleRivera Rivera, L., Séris Martínez, M., Reynales Shigematsu, L. M., Gómez García, J. A., Austria Corrales, F., Toledano-Toledano, F., Jiménez Tapia, A., Tejadilla Orozco, D. I., & Astudillo García, C. I. (2023). Violence against Women during the COVID-19 Pandemic in Mexico. Healthcare, 11(3), 419. https://doi.org/10.3390/healthcare11030419