


Validity of On-Line Supervised Fitness Tests in People with Low Back Pain

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
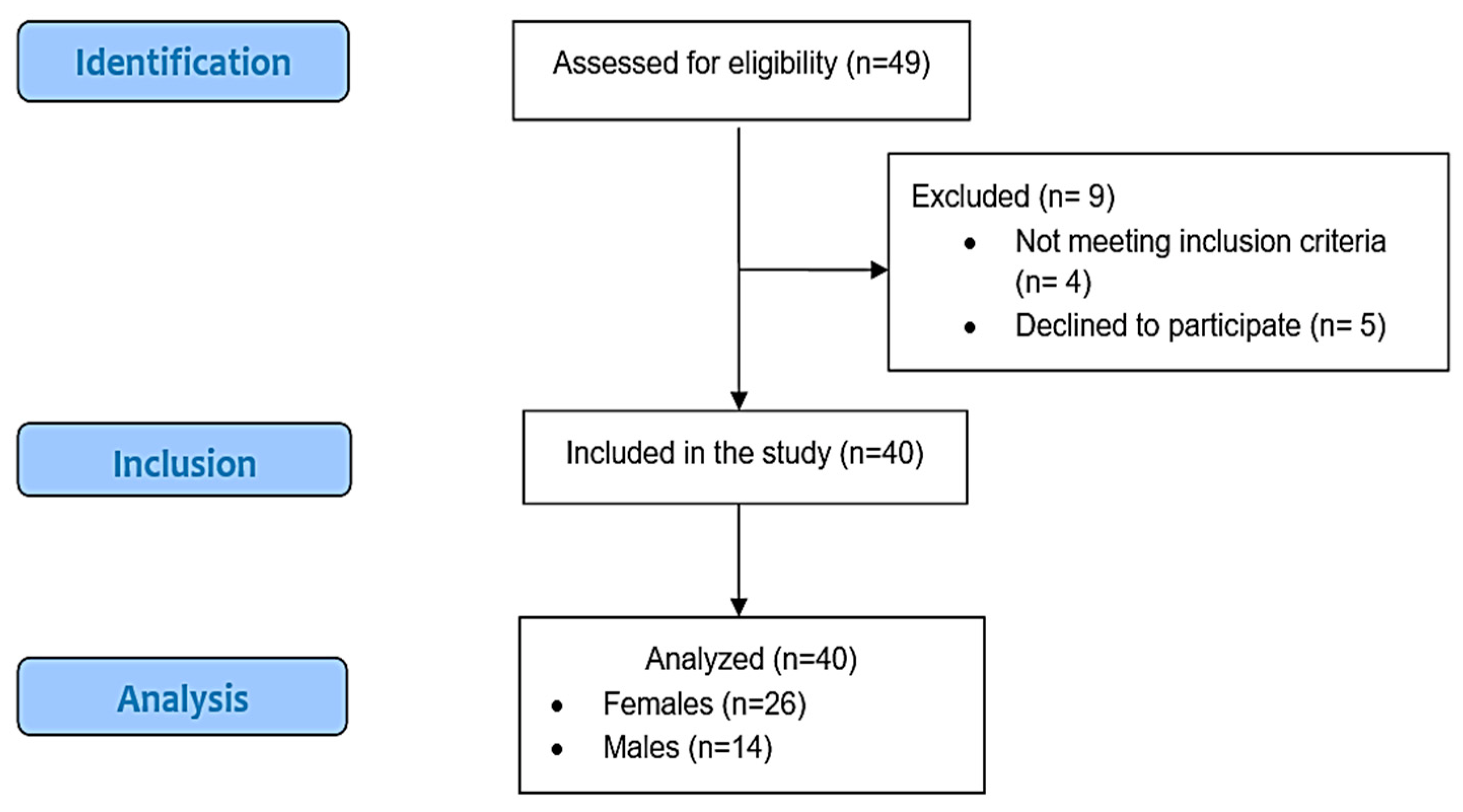
2.1. Study Design and Participants
2.2. Procedures and Assessments
2.3. Demographic Information and Quality of Life
2.3.1. The 30 s Chair Stand-Up Test
2.3.2. Arm Curl Test
2.3.3. 2 Min Step Test in Place
2.3.4. Chair-Sit and Reach Test
2.3.5. Back Scratch Test
2.3.6. Eight-Foot Up-and-Go Test
2.3.7. Sharpened Romberg Test
2.3.8. One-Legged Stance Test
2.4. Statistical Analytics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.; March, L.; Zheng, X.; Huang, J.; Wang, X.; Zhao, J.; Blyth, F.M.; Smith, E.; Buchbinder, R.; Hoy, D. Global low back pain prevalence and years lived with disability from 1990 to 2017: Estimates from the Global Burden of Disease Study 2017. Ann. Transl. Med. 2020, 8, 299. [Google Scholar] [CrossRef] [PubMed]
- Grabovac, I.; Dorner, T.E. Association between low back pain and various everyday performances. Wien. Klin. Wochenschr. 2019, 131, 541–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macías-Toronjo, I.; Rojas-Ocaña, M.J.; Sánchez-Ramos, J.L.; García-Navarro, E.B. Pain catastrophizing, kinesiophobia and fear-avoidance in non-specific work-related low-back pain as predictors of sickness absence. PLoS ONE 2020, 15, e0242994. [Google Scholar] [CrossRef]
- Alsufiany, M.B.; Lohman, E.B.; Daher, N.S.; Gang, G.R.; Shallan, A.I.; Jaber, H.M. Non-specific chronic low back pain and physical activity: A comparison of postural control and hip muscle isometric strength: A cross-sectional study. Medicine 2020, 99, e18544. [Google Scholar] [CrossRef]
- Alonso-García, M.; Sarría-Santamera, A. The economic and social burden of low back pain in Spain: A national assessment of the economic and social impact of low back pain in Spain. Spine 2020, 45, E1026–E1032. [Google Scholar] [CrossRef]
- Wun, A.; Kollias, P.; Jeong, H.; Rizzo, R.R.N.; Cashin, A.G.; Bagg, M.K.; McAuley, J.H.; Jones, M.D. Why is exercise prescribed for people with chronic low back pain? A review of the mechanisms of benefit proposed by clinical trialists. Musculoskelet. Sci. Pract. 2021, 51, 102307. [Google Scholar] [CrossRef]
- Buckinx, F.; Croisier, J.L.; Reginster, J.Y.; Dardenne, N.; Beaudart, C.; Slomian, J.; Leonard, S.; Bruyère, O. Reliability of muscle strength measures obtained with a hand-held dynamometer in an elderly population. Clin. Physiol. Funct. Imaging 2017, 37, 332–340. [Google Scholar] [CrossRef]
- Picelli, A.; Buzzi, M.G.; Cisari, C.; Gandolfi, M.; Porru, D.; Bonadiman, S.; Brugnera, A.; Carone, R.; Cerbo, R.; Del Carro, U. Headache, low back pain, other nociceptive and mixed pain conditions in neurorehabilitation. Evidence and recommendations from the Italian Consensus Conference on Pain in Neurorehabilitation. Eur. J. Phys. Rehabil. Med. 2016, 52, 867–880. [Google Scholar]
- Kim, J.G.; Park, S.-M.; Kim, H.-J.; Yeom, J.S. Development and Validation of a Risk-Prediction Nomogram for Chronic Low Back Pain Using a National Health Examination Survey: A Cross-Sectional Study. Healthcare 2023, 11, 468. [Google Scholar] [CrossRef]
- Pescatello, L.S.; Riebe, D.; Thompson, P.D. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Rikli, R.E.; Jones, C.J. Senior Fitness Test Manual; Human Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Mientjes, M.I.V.; Frank, J.S. Balance in chronic low back pain patients compared to healthy people under various conditions in upright standing. Clin. Biomech. 1999, 14, 710–716. [Google Scholar] [CrossRef]
- Caffaro, R.R.; França, F.J.R.; Burke, T.N.; Magalhães, M.O.; Ramos, L.A.V.; Marques, A.P. Postural control in individuals with and without non-specific chronic low back pain: A preliminary case–control study. Eur. Spine J. 2014, 23, 807–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luoto, S.; Aalto, H.; Taimela, S.; Hurri, H.; Pyykkö, I.; Alaranta, H. One-footed and externally disturbed two-footed postural control in patients with chronic low back pain and healthy control subjects: A controlled study with follow-up. Spine 1998, 23, 2081–2089. [Google Scholar] [CrossRef]
- Da Silva, R.A.; Vieira, E.R.; Carvalho, C.E.; Oliveira, M.R.; Amorim, C.F.; Neto, E.N. Age-related differences on low back pain and postural control during one-leg stance: A case–control study. Eur. Spine J. 2016, 25, 1251–1257. [Google Scholar] [CrossRef]
- da Silva, R.A.; Vieira, E.R.; Fernandes, K.B.P.; Andraus, R.A.; Oliveira, M.R.; Sturion, L.A.; Calderon, M.G. People with chronic low back pain have poorer balance than controls in challenging tasks. Disabil. Rehabil. 2018, 40, 1294–1300. [Google Scholar] [CrossRef]
- Narici, M.; Vito, G.D.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur. J. Sport Sci. 2021, 21, 614–635. [Google Scholar] [CrossRef]
- Lai, B.; Chiu, C.-Y.; Pounds, E.; Tracy, T.; Mehta, T.; Young, H.-J.; Riser, E.; Rimmer, J. COVID-19 modifications for remote teleassessment and teletraining of a complementary alternative medicine intervention for people with multiple sclerosis: Protocol for a randomized controlled trial. JMIR Res. Protoc. 2020, 9, e18415. [Google Scholar] [CrossRef]
- Holland, A.E.; Malaguti, C.; Hoffman, M.; Lahham, A.; Burge, A.T.; Dowman, L.; May, A.K.; Bondarenko, J.; Graco, M.; Tikellis, G. Home-based or remote exercise testing in chronic respiratory disease, during the COVID-19 pandemic and beyond: A rapid review. Chronic Respir. Dis. 2020, 17, 1479973120952418. [Google Scholar] [CrossRef]
- Hwang, R.; Fan, T.; Bowe, R.; Louis, M.; Bertram, M.; Morris, N.R.; Adsett, J. Home-based and remote functional exercise testing in cardiac conditions, during the COVID-19 pandemic and beyond: A systematic review. Physiotherapy 2022, 115, 27–35. [Google Scholar] [CrossRef]
- Blair, C.K.; Harding, E.; Herman, C.; Boyce, T.; Demark-Wahnefried, W.; Davis, S.; Kinney, A.Y.; Pankratz, V.S. Remote Assessment of Functional Mobility and Strength in Older Cancer Survivors: Protocol for a Validity and Reliability Study. JMIR Res. Protoc. 2020, 9, e20834. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, E.F.; Harris, R.; Dufour, A.B.; Morey, M.C.; Bean, J. Reliability of Virtual Physical Performance Assessments in Veterans During the COVID-19 Pandemic. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100146. [Google Scholar] [CrossRef] [PubMed]
- Winters-Stone, K.; Lipps, C.; Guidarelli, C.; Herrera-Fuentes, P. Converting physical function testing to the remote setting: Adapting our research protocol during COVID-19. Innov. Aging 2020, 4, 936–937. [Google Scholar] [CrossRef]
- Hoenemeyer, T.W.; Cole, W.W.; Oster, R.A.; Pekmezi, D.W.; Pye, A.; Demark-Wahnefried, W. Test/Retest Reliability and Validity of Remote vs. In-Person Anthropometric and Physical Performance Assessments in Cancer Survivors and Supportive Partners. Cancers 2022, 14, 1075. [Google Scholar] [CrossRef] [PubMed]
- Rozenberg, S. Chronic low back pain: Definition and treatment. Rev Prat 2008, 58, 265–272. [Google Scholar]
- McGuigan, M. Principles of test selection and administration. In Essentials of Strength Training and Conditioning, 4th ed.; Haff, G.G., Triplett, N.T., Eds.; Human Kinetics: Champaign, IL, USA, 2016; pp. 249–258. [Google Scholar]
- Franchignoni, F.; Tesio, L.; Martino, M.; Ricupero, C. Reliability of four simple, quantitative tests of balance and mobility in healthy elderly females. Aging Clin. Exp. Res. 1998, 10, 26–31. [Google Scholar] [CrossRef]
- Izquierdo, M. Multicomponent physical exercise program: Vivifrail. Nutr. Hosp. 2019, 36, 50–56. [Google Scholar]
- Lee, C. Sharpening the Sharpened Romberg. SPUMS J. 1998, 28, 125–132. [Google Scholar]
- da Silva, R.A.; Vieira, E.R.; Léonard, G.; Beaulieu, L.-D.; Ngomo, S.; Nowotny, A.H.; Amorim, C.F. Age-and low back pain-related differences in trunk muscle activation during one-legged stance balance task. Gait Posture 2019, 69, 25–30. [Google Scholar] [CrossRef]
- Balestroni, G.; Bertolotti, G. EuroQol-5D (EQ-5D): An instrument for measuring quality of life. Monaldi Arch. Chest Dis. 2012, 78, 155–159. [Google Scholar] [CrossRef]
- Badia, X.; Roset, M.; Montserrat, S.; Herdman, M.; Segura, A. The Spanish version of EuroQol: A description and its applications. European Quality of Life scale. Med. Clin. 1999, 112, 79–85. [Google Scholar]
- Thomas, J.; Silverman, S.; Nelson, J. Research Methods in Physical Activity, 7th ed.; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Bellamy, N. Principles of Clinical Outcome Assessment. In Rheumatology; Mosby: Philadelphia, PA, USA, 2014. [Google Scholar]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2009; Volume 892. [Google Scholar]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding bland altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis forthe Behavioural Sciences; Baskı: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Plagg, B.; Piccoliori, G.; Oschmann, J.; Engl, A.; Eisendle, K. Primary health care and hospital management during COVID-19: Lessons from lombardy. Risk Manag. Healthc. Policy 2021, 14, 3987–3992. [Google Scholar] [CrossRef]
- Podlog, L.W.; Brown, W.J. Self-determination theory: A framework for enhancing patient-centered care. J. Nurse Pract. 2016, 12, e359–e362. [Google Scholar] [CrossRef]
- Borrega-Mouquinho, Y.; Sánchez-Gómez, J.; Fuentes-García, J.P.; Collado-Mateo, D.; Villafaina, S. Effects of High-Intensity Interval Training and Moderate-Intensity Training on Stress, Depression, Anxiety, and Resilience in Healthy Adults During Coronavirus Disease 2019 Confinement: A Randomized Controlled Trial. Front. Psychol. 2021, 12, 270. [Google Scholar] [CrossRef]
- Schneider, S.; Brümmer, V.; Carnahan, H.; Kleinert, J.; Piacentini, M.F.; Meeusen, R.; Strüder, H.K. Exercise as a countermeasure to psycho-physiological deconditioning during long-term confinement. Behav. Brain Res. 2010, 211, 208–214. [Google Scholar] [CrossRef]
- Lin, I.I.; Chen, Y.-L.; Chuang, L.-L. Test-Retest Reliability of Home-Based Fitness Assessments Using a Mobile App (R Plus Health) in Healthy Adults: Prospective Quantitative Study. JMIR Form. Res. 2021, 5, e28040. [Google Scholar] [CrossRef]
- Holland, A.E.; Rasekaba, T.; Fiore, J.F., Jr.; Burge, A.T.; Lee, A.L. The 6-minute walk distance cannot be accurately assessed at home in people with COPD. Disabil. Rehabil. 2015, 37, 1102–1106. [Google Scholar] [CrossRef]
- Cox, N.S.; Alison, J.A.; Button, B.M.; Wilson, J.W.; Holland, A.E. Assessing exercise capacity using telehealth: A feasibility study in adults with cystic fibrosis. Respir. Care 2013, 58, 286–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Original Measure | Adaptions for the Face-to-Face Evaluation | Adaptions for the Online Evaluation |
|---|---|---|
| 30 s Chair Stand-Up Test [13] | Same as original | Participants controlled the stopwatch by starting the test at second 10 and finishing it at second 40. Repetitions were counted by participants. |
| Arm Curl Test [13] | The weight was added to a sturdy cloth or plastic bag until 2.300 kg and 3.600 kg was reached (e.g., packets of rice, nuts, yogurt, etc.). | |
| Participants controlled the stopwatch by starting the test at second 10 and finishing it at second 40. Repetitions were counted by participants. | ||
| 2-min Step Test in Place [13] | Same as original | Repetitions were counted by participants. Time was controlled by each participant. |
| Chair-sit and Reach Test [13] | Same as original | A light object, such as a ruler, was held with both hands by the participants. Participants positioned the end of the object touching the toe tips and slid their hands elongating the trunk. The score was obtained by measuring the distance between the fingertip and the end of the object. |
| Back Scratch Test [13] | Same as original | A light object, such as a ruler, was held with the upper hand until the end touched the fingertip of the lower hand. The upper hand slid in the object as low as possible. The score was obtained by measuring the distance between the fingertip and the end of the object. |
| 8-Foot Up-and-go Test [13] | Same as original | Participants started and stopped their stopwatch holding it during the test. |
| Sharpened Romberg Test [31] | Same as original | Participants controlled the stopwatch by pressing start and stop finishing the test when 60 s was reached or balance was lost. |
| One-Legged Stance Test [32] | Same as original | Participants controlled the stopwatch by pressing start and stop finishing the test when 60 s was reached or balance was lost. |
| Participants’ Characteristics | Total Sample Size | Women (n = 26) | Men (n = 14) |
|---|---|---|---|
| Mean (SD) [range of variability] | Mean (SD) [range of variability] | Mean (SD) [range of variability] | |
| Age | 58.48 (9.87) [45–72] | 58.46 (9.23) [45–72] | 58.50 (10.14) [47–69] |
| Height (cm) | 166.00 (9.72) [145–184] | 164.38 (10.27) [145–176] | 169.00 (8.09) [165–184] |
| Body mass (Kg) | 71.10 (13.08) [53–107] | 69.92 (14.52) [53–88] | 73.29 (10.01) [65–107] |
| BMI | 25.69 (3.37) [18.78–35.34] | 25.74 (3.82) [18.78–31.55] | 25.59 (2.42) [21.50–35.34] |
| EuroQol-5D (coefficient) | 0.85 (0.14) [0.32–1] | 0.87 (0.12) [0.74–1] | 0.81 (0.18) [0.32–1] |
| EuroQol-5D (VAS) | 76.25 (10.49) [60–100] | 76.73 (11.13) [60–100] | 69.87 (9.50) [60–90] |
| Mobility | 1.08 (0.27) [1–2] | 0.87 (0.12) [1–2] | 1.21 (0.43) [1–2] |
| Self-Care | 1.03 (0.16) [1–2] | 1.04 (0.20) [1–2] | 1.00 (0.00) [1] |
| Activities Of Daily Life | 1.20 (0.41) [1–2] | 1.19 (0.40) [1–2] | 1.21 (0.43) [1–2] |
| Pain | 1.63 (0.54) [1–2] | 1.62 (0.50) [1–2] | 1.64 (0.63) [1–2] |
| Anxiety/Depression | 1.05 (0.22) [1–2] | 1.00 (0.00) [1] | 1.14 (0.36) [1–2] |
| Variable | Online Evaluation Mean (SD) | Face-to-Face Evaluation Mean (SD) | p-Value | ICC (95% CI) | Correlation Coefficient |
|---|---|---|---|---|---|
| 30 s Chair Stand-Up test | 19.00 (3.76) | 18.18 (3.91) | 0.108 | 0.79 (0.610–0.891) | 0.66 *** |
| Arm-curl test | 21.38 (4.42) | 20.70 (4.28) | 0.385 | 0.55 (0.143–0.760) | 0.38 * |
| 2 min step-test in place | 107.50 (23.12) | 110.10 (23.13) | 0.306 | 0.87 (0.748–0.930) | 0.76 *** |
| Chair-sit and reach test | −1.46 (9.59) | −0.93 (10.50) | 0.528 | 0.93 (0.859–0.961) | 0.86 *** |
| Back scratch test | −4.89 (8.53) | −2.68 (9.25) | 0.305 | 0.79 (0.596–0.887) | 0.64 *** |
| 8-foot up-and-go test | 4.89 (0.85) | 4.45 (1.06) | 0.007 | 0.64 (0.313–0.808) | 0.48 ** |
| Sharpened Romberg test | 59.00 (4.41) | 58.63 (3.92) | 0.334 | 0.89 (0.792–0.942) | 0.66 ††† |
| One-legged stance test | 50.57 (16.34) | 47.88 (19.44) | 0.363 | 0.83 (0.675–0.909) | 0.75 ††† |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavín-Pérez, A.M.; León-Llamas, J.L.; Salas Costilla, F.J.; Collado-Mateo, D.; López de las Heras, R.; Gasque Celma, P.; Villafaina, S. Validity of On-Line Supervised Fitness Tests in People with Low Back Pain. Healthcare 2023, 11, 1019. https://doi.org/10.3390/healthcare11071019
Lavín-Pérez AM, León-Llamas JL, Salas Costilla FJ, Collado-Mateo D, López de las Heras R, Gasque Celma P, Villafaina S. Validity of On-Line Supervised Fitness Tests in People with Low Back Pain. Healthcare. 2023; 11(7):1019. https://doi.org/10.3390/healthcare11071019
Chicago/Turabian StyleLavín-Pérez, Ana Myriam, Juan Luis León-Llamas, Francisco José Salas Costilla, Daniel Collado-Mateo, Raúl López de las Heras, Pablo Gasque Celma, and Santos Villafaina. 2023. "Validity of On-Line Supervised Fitness Tests in People with Low Back Pain" Healthcare 11, no. 7: 1019. https://doi.org/10.3390/healthcare11071019
APA StyleLavín-Pérez, A. M., León-Llamas, J. L., Salas Costilla, F. J., Collado-Mateo, D., López de las Heras, R., Gasque Celma, P., & Villafaina, S. (2023). Validity of On-Line Supervised Fitness Tests in People with Low Back Pain. Healthcare, 11(7), 1019. https://doi.org/10.3390/healthcare11071019