Living the Full Catastrophe: A Mindfulness-Based Program to Support Recovery from Stroke


Abstract
:1. Introduction
1.1. Mindfulness-Based Stress Reduction
1.2. Prevalence of Stroke and the Challenges for Recovery from Stroke
1.3. Mindfulness Skills to Support Stroke Recovery
1.4. Rationale for MBSR Adaptation and Introduction of MBRfS Model
- Review the literature to identify, frame, and affirm the beneficial effects of mindfulness skills training within the context of stroke recovery, as this opportunity has not been widely reviewed.
- Explore the existing literature and personal documents for unique challenges and adaptations to consider when offering a mindfulness-based intervention for stroke survivors, their caregivers, and those offering healthcare to this population.
- Propose a series of adaptations to Kabat-Zinn’s [1] MBSR framework to create a mindfulness-based curriculum tailored to stroke recovery.
- Establish a preliminary conceptual model for Mindfulness-Based Recovery from Stroke (MBRfS), based on themes that emerged in the process of MBSR curriculum adaptation.
- Illustrate the conceptual model and its potential contribution via a series of autoethnographic vignettes of the author’s direct experiences.
2. Materials and Methods
2.1. Overview of Research Design
2.2. Mindfulness-Based Stress Reduction (MBSR) Curriculum Adaptation
2.3. Autoethnography to Identify Themes and Illustrate the Framework for the Proposed Model
- What is my lived experience of stroke and stroke recovery (up to this point)?
- How has my stroke recovery been impacted by my prior MBSR training (first as a participant and later as a teacher)?
- How did my mindfulness skills influence my navigation of the healthcare system and interactions with healthcare providers?
- What effects did MBSR training have on my choice to view my stroke and the recovery as a journey and pathway to greater wholeness?
- How does MBSR continue to contribute to my perceptions of physical health and emotional well-being in stroke recovery?
- How have I adapted the MBSR model to best serve my own stroke recovery and perhaps also serve other stroke survivors?
2.4. Emergent Themes and Principles as a Conceptual Model for Stroke Recovery: MBRfS
3. Results
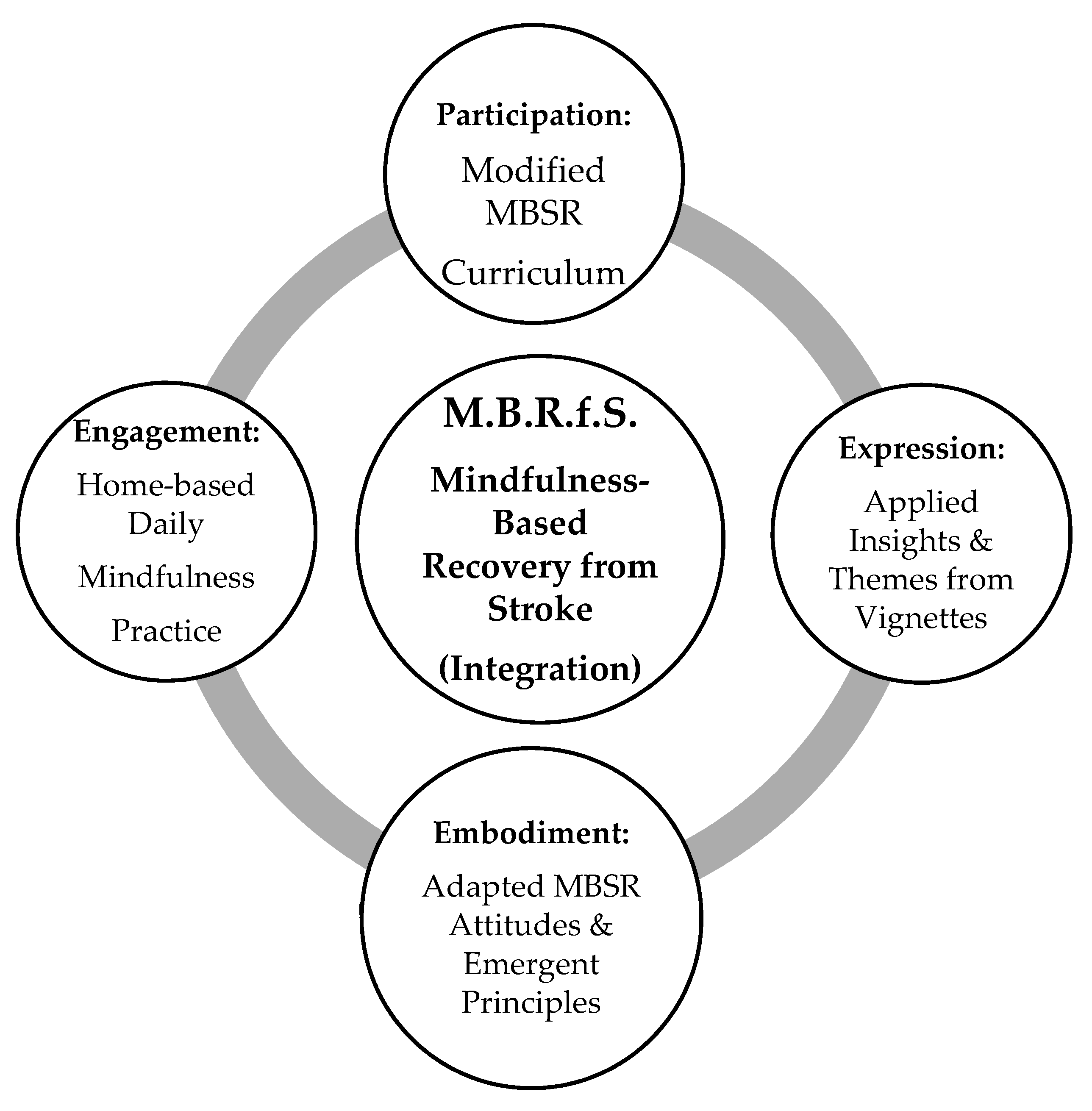
3.1. Mindfulness-Based Recovery from Stroke (MBRfS): The Proposed Conceptual Model
- Participation: Taking part in the modified eight-week MBSR curriculum.
- Embodiment: Intention to practice and strengthen the mindfulness-based attitudes and emergent principles (ways of being).
- Engagement: Commitment to following a home-based daily mindfulness practice during the eight weeks of classes.
- Expression: Reflect and express personal insights of the stroke recovery journey in the spirit of the author’s autoethnographic explorations and thematic outcomes.
3.2. Modifications to MBSR Curriculum (Participation)
- Budgeted time for frequent collective and individual rest breaks.
- Shorter versions of the formal mindfulness practices.
- Modifications for all physical movement practices to allow for varying degrees of abilities and energy levels.
- Earlier introduction of modified versions of Mindful Walking as sensory support for walking.
- Offering many versions of shorter practices with easy access for home practice (e.g., MP3, weblinks, CDs).
- Offering summary handouts to support memory for each class and video links to watch or listen to between classes.
3.3. Expanded MBSR Attitudes and Overarching Themes of MBRfS (Embodiment)
- Recognition of loss (body feeling, capacity, identity, and self) and the role of grief.
- Non-linear experiences of stroke recovery.
- Attention to change, including progress in strength, flexibility, mobility, and speech.
- Life-long gains in stroke recovery, acceptance that stroke recovery never officially ends.
- Challenges in communication (connected to interpersonal elements of MBSR).
3.4. Home-Based Daily Mindfulness Practice (Engagement)
3.5. Autoethnography
It seems most fitting to first offer reflection on what it is to write this academic paper three years after a major stroke, this act of sharing my thoughts by translating them to paper. I feel a mix of gratitude for the returning abilities and some frustration for the amount of time and combination of strategies the process requires. I take a slow breath and jump into the task, assessing what is needed. Prior to the stroke, I could accurately type almost to the pace of my thoughts, fingers flying across the keyboard in a stream-of-consciousness pace. Now, three years post-stroke, I type using a combination of my non-affected (non-dominant) hand, the pointer finger of my stroke-affected (dominant) hand, and the dictation function, which can listen to my spoken words and transcribe.
I find that a dance can occur when I work patiently with whatever shows up at any given moment. Sometimes, my speech is punctuated with stuttering and word searching, which makes dictating more frustrating and less productive. I have also learned to write my thoughts longhand, which sometimes supports better dictation, or I return once again to my slow, modified typing. Sometimes I forget how to spell words, I am not able to envision the words in my mind’s eye, so I also keep my smart phone nearby to dictate the word I want. When I then can see the proper spelling, I recognize it instantly. I gently remind myself that this deficit will continue to improve as I maintain my daily cognitive rehabilitation routine, practicing with a spelling application on my electronic tablet.
I return to the concentration of writing, over and over, taking short breaks as needed. I write the first draft with many words spelled phonetically, not worrying beyond that point until I can go back and update for spelling and grammar. And so, my words and intentions gradually come together to be shared with another, whether in an email or a manuscript. A few sentences later, frustrated by the keyboard that used to be so fluid for me, I pick up my cell phone to use the texting and autocorrect that I now find easier. I move along, slowly, deliberately, patiently, as if I have nowhere else to go and I have all the time in the world. The snail has become my symbol and an animal totem to remind me to go slow.
I share this as an immediate and simple example of the way I approach life and each cognitive and fine motor task since my experience of a major ischemic stroke in the summer of 2017. At that time, I was a daily runner, avid fan of the Mediterranean diet, and a long-time meditation practitioner and teacher. I did not appear to be at risk for stroke. With low blood pressure and ideal cholesterol levels that caused my doctor to ask with enthusiasm what my diet consisted of, I did not have this particular worry on my radar. And yet, an internal carotid artery on the left side of my face spontaneously occluded and in an instant, my life changed. I became a stroke survivor.
The image and teaching metaphor of a tsunami has come to me many times as I attempt to express my personal experience of stroke and these relatively early years of recovery. Before a tsunami hits, there is often a receding of the water along a coastline, a calm before the storm. This is the stage when animals and wise indigenous people can read the signs and head for higher ground. I knew something was not right with me, but I easily dismissed it as jetlag from recent international travel. Next, the tsunami hits, a wall of water slamming with such ferocity to destroy in its path, creating confusion, panic, and devastation. The artery split, and the “wall of water” hit, cutting the blood flow from my brain, depriving my left hemisphere of oxygen, leaving me instantly without the knowledge of how to use my phone to call for help. The tsunami floods and invades the coastline, drowning and breaking apart everything it touches. After the trauma, the water slowly recedes back into the ocean, but the landscape will never be the same. Some parts of the landscape are forever lost, unrecognizable. There is a new vigilance when looking toward the horizon for the possibility of another treacherous wave. Some aspects of the terrain will be repaired, rebuilt, and made anew with time and effort. Unexpected moments of beauty and grace, alongside the sorrows, are the discoveries over time only the strength of the tsunami could reveal: all the hidden gifts under the sand that could not be seen before. This process of repair, discovery, and revealing of hidden treasures never ends.
Giant waves, calm seas, the treasures of my mind buried in the sand—this is the way I experience stroke recovery. It is a process that is at times, calm and gradual, other times harsh and unpredictable. It is yet another manifestation of living the “full catastrophe” of life. I am a new and humbled student in this curriculum, vulnerable in the sharing of my lived experience. At the same time, I am deeply aware that I am not alone in this journey, which gives courage to persevere and reach out to share my story with the wish that it be helpful to others.
As I reviewed my photos, audio reflection, and journals, I held the questions in mind that I posited in the methods, paying particular attention to the ways in which I deliberately, and sometimes instinctively, relied on my mindfulness skills. This includes what I already knew to be true in regards to the value of MBSR. Simply stated, I have no idea how I could be navigating a lifelong, harrowing journey without a grounding in mindfulness meditation and Mindfulness-Based Stress Reduction (MBSR). I cannot imagine that possibility, and I am grateful that I do not need to. I will share the major themes that spoke to me as I reviewed my recorded experiences, which are reflective of the guiding research questions and informed my proposed adaptations to the MBSR curriculum.
3.6. Autoethnographic Vignettes to Inform the MBRfS Model (Expression)
- Acceptance: A readiness and psychological agility to accept the stroke event and the sudden impact of experiencing a stroke and acquired brain injury.
- Navigating Uncertainties: Expressing and navigating the uncertainties of stroke recovery (both personally and in relationship with healthcare professionals) with mindful awareness and self-responsibility for my recovery outcomes.
- Somatic Wisdom: Trusting the inherent wisdom of the body and mind to serve metaphorically as stroke recovery “guides” and teachers to accompany stroke survivors on the journey.
- Meeting Complexities with Compassionate Dignity: The growing capacity over time to integrate (“turn toward”) complex post-stroke emotions, such as fear, grief, vulnerability, and frustration, with greater self-compassion, dignity, and sense of wholeness as a human being.
- Theme 1.
- Readiness and agility to accept the experience and outcomes
- Theme 2.
- Expressing and navigating the uncertainties of stroke recovery
- Theme 3.
- Trusting the inherent wisdom of the body and mind
- Theme 4.
- Capacity to integrate complex emotions with self-compassion and sense of wholeness
4. Discussion
4.1. Offering a Proposed Integrated Mindfulness-Based Model to Support Recovery from Stroke
4.2. Curriculum Integrity of MBSR as a Modified Curricular Intervention for Recovery from Stroke
4.3. Themes and Challenges Specific to the MBRfS Program
4.4. Future Directions
4.5. Limitations
4.6. Implications for Future Studies
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Kabat-Zinn, J. Full Catastrophe Living, Revised Edition: How to Cope with Stress, Pain and Illness Using Mindfulness Meditation; Little, Brown Book Group: London, UK, 2013; ISBN 1-4055-1700-X. [Google Scholar]
- Carmody, J.; Baer, R.A. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. J. Behav. Med. 2008, 31, 23–33. [Google Scholar] [CrossRef]
- Lamothe, M.; Rondeau, É.; Malboeuf-Hurtubise, C.; Duval, M.; Sultan, S. Outcomes of MBSR or MBSR-based interventions in health care providers: A systematic review with a focus on empathy and emotional competencies. Complementary Ther. Med. 2016, 24, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Bernhard, J.D.; Kristeller, J.; Kabat-Zinn, J. Effectiveness of relaxation and visualization techniques as an adjunct to phototherapy and photochemotherapy of psoriasis. J. Am. Acad. Dermatol. 1988, 19, 572–573. [Google Scholar] [CrossRef]
- Kabat-Zinn, J.; Lipworth, L.; Burney, R. The clinical use of mindfulness meditation for the self-regulation of chronic pain. J. Behav. Med. 1985, 8, 163–190. [Google Scholar] [CrossRef] [PubMed]
- Bablas, V.; Yap, K.; Cunnington, D.; Swieca, J.; Greenwood, K.M. Mindfulness-based stress reduction for restless legs syndrome: A proof of concept trial. Mindfulness 2016, 7, 396–408. [Google Scholar] [CrossRef]
- Bluth, K.; Gaylord, S.; Nguyen, K.; Bunevicius, A.; Girdler, S. Mindfulness-based stress reduction as a promising intervention for amelioration of premenstrual dysphoric disorder symptoms. Mindfulness 2015, 6, 1292–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carmody, J.; Crawford, S.; Churchill, L. A pilot study of mindfulness-based stress reduction for hot flashes. Menopause 2006, 13, 760–769. [Google Scholar] [CrossRef]
- Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-based stress reduction and health benefits: A meta-analysis. J. Psychosom. Res. 2004, 57, 35–43. [Google Scholar] [CrossRef]
- Eberth, J.; Sedlmeier, P. The effects of mindfulness meditation: A meta-analysis. Mindfulness 2012, 3, 174–189. [Google Scholar] [CrossRef]
- Miller, J.J.; Fletcher, K.; Kabat-Zinn, J. Three-year follow-up and clinical implications of a mindfulness meditation-based stress reduction intervention in the treatment of anxiety disorders. Gen. Hosp. Psychiatry 1995, 17, 192–200. [Google Scholar] [CrossRef]
- Teasdale, J.D.; Segal, Z.V.; Williams, J.M.G.; Ridgeway, V.A.; Soulsby, J.M.; Lau, M.A. Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. J. Consult. Clin. Psychol. 2000, 68, 615. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.M.; Fleming, M.F.; Bonus, K.A.; Baker, T.B. A pilot study on mindfulness based stress reduction for smokers. BMC Complementary Altern. Med. 2007, 7, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omidi, A.; Mohammadi, A.; Zargar, F.; Akbari, H. Efficacy of mindfulness-based stress reduction on mood states of veterans with post-traumatic stress disorder. Arch. Trauma Res. 2013, 1, 151. [Google Scholar] [CrossRef] [PubMed]
- Davidson, R.J.; Lutz, A. Buddha’s brain: Neuroplasticity and meditation [in the spotlight]. IEEE Signal Process. Mag. 2008, 25, 174–176. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, F.; Emerson, N.M.; Farris, S.R.; Ray, J.N.; Jung, Y.; McHaffie, J.G.; Coghill, R.C. Mindfulness meditation-based pain relief employs different neural mechanisms than placebo and sham mindfulness meditation-induced analgesia. J. Neurosci. 2015, 35, 15307–15325. [Google Scholar] [CrossRef]
- Creswell, J.D.; Taren, A.A.; Lindsay, E.K.; Greco, C.M.; Gianaros, P.J.; Fairgrieve, A.; Marsland, A.L.; Brown, K.W.; Way, B.M.; Rosen, R.K. Alterations in resting-state functional connectivity link mindfulness meditation with reduced interleukin-6: A randomized controlled trial. Biol. Psychiatry 2016, 80, 53–61. [Google Scholar] [CrossRef]
- Lazar, S.W.; Kerr, C.E.; Wasserman, R.H.; Gray, J.R.; Greve, D.N.; Treadway, M.T.; McGarvey, M.; Quinn, B.T.; Dusek, J.A.; Benson, H. Meditation experience is associated with increased cortical thickness. Neuroreport 2005, 16, 1893. [Google Scholar] [CrossRef] [Green Version]
- Lindsay, M.P.; Norrving, B.; Sacco, R.L.; Brainin, M.; Hacke, W.; Martins, S.; Pandian, J.; Feigin, V. World stroke organization global stroke fact sheet. Int. J. Stroke 2019, 14, 12. [Google Scholar] [CrossRef]
- Tsgoyna, T. Hope after Stroke for Caregivers and Survivors: The Holistic Guide to Getting Your Life Back; XETROV: Monee, IL, USA, 2019; ISBN 978-1-73295-380-2. [Google Scholar]
- Kim, J.S. Post-stroke pain. Expert Rev. Neurother. 2009, 9, 711–721. [Google Scholar] [CrossRef]
- Tatemichi, T.; Desmond, D.; Stern, Y.; Paik, M.; Sano, M.; Bagiella, E. Cognitive impairment after stroke: Frequency, patterns, and relationship to functional abilities. J. Neurol. Neurosurg. Psychiatry 1994, 57, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Hackett, M.L.; Yapa, C.; Parag, V.; Anderson, C.S. Frequency of depression after stroke: A systematic review of observational studies. Stroke 2005, 36, 1330–1340. [Google Scholar] [CrossRef] [PubMed]
- Vohora, R.; Ogi, L. Addressing the emotional needs of stroke survivors. Nurs. Times 2008, 104, 32–35. [Google Scholar] [PubMed]
- Anderson, S.; Whitfield, K. Social identity and stroke: ‘They don’t make me feel like, there’s something wrong with me’. Scand. J. Caring Sci. 2013, 27, 820–830. [Google Scholar] [CrossRef] [PubMed]
- Michael, K. Call to action: Enhancing poststroke resilience. Top. Geriatr. Rehabil. 2014, 30, 195–198. [Google Scholar] [CrossRef]
- Sarre, S.; Redlich, C.; Tinker, A.; Sadler, E.; Bhalla, A.; McKevitt, C. A systematic review of qualitative studies on adjusting after stroke: Lessons for the study of resilience. Disabil. Rehabil. 2014, 36, 716–726. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Liu, Z.; Zhou, X.; Zhou, L. Resilience among stroke survivors: A cohort study of the first 6 months. J. Adv. Nurs. 2020, 76, 504–513. [Google Scholar] [CrossRef]
- Lazaridou, A.; Philbrook, P.; Tzika, A.A. Yoga and mindfulness as therapeutic interventions for stroke rehabilitation: A systematic review. Evid. Based Complementary Altern. Med. 2013, 2013, 357108. [Google Scholar] [CrossRef]
- Love, M.F.; Sharrief, A.; Chaoul, A.; Savitz, S.; Beauchamp, J.E.S. Mind-body interventions, psychological stressors, and quality of life in stroke survivors: A systematic review. Stroke 2019, 50, 434–440. [Google Scholar] [CrossRef] [Green Version]
- Ji, H.; Yu, L. Effect of yoga exercise on cognitive ability and motor function recovery in stroke patients. Neuro-Quantology 2018, 16, 822–827. [Google Scholar] [CrossRef]
- Zou, L.; Sasaki, J.E.; Zeng, N.; Wang, C.; Sun, L. A systematic review with meta-analysis of mindful exercises on rehabilitative outcomes among poststroke patients. Arch. Phys. Med. Rehabil. 2018, 99, 2355–2364. [Google Scholar] [CrossRef]
- Harris, A.; Austin, M.; Blake, T.; Bird, M. Perceived benefits and barriers to yoga participation after stroke: A focus group approach. Complementary Ther. Clin. Pract. 2019, 34, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Thayabaranathan, T.; Andrew, N.E.; Immink, M.A.; Hillier, S.; Stevens, P.; Stolwyk, R.; Kilkenny, M.; Cadilhac, D.A. Determining the potential benefits of yoga in chronic stroke care: A systematic review and meta-analysis. Top. Stroke Rehabil. 2017, 24, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Wathugala, M.; Saldana, D.; Juliano, J.M.; Chan, J.; Liew, S.-L. Mindfulness meditation effects on poststroke spasticity: A feasibility study. J. Evid. Based Integr. Med. 2019, 24, 2515690X19855941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laures-Gore, J.; Marshall, R.S. Mindfulness meditation in aphasia: A case report. NeuroRehabilitation 2016, 38, 321–329. [Google Scholar] [CrossRef]
- Marshall, R.S.; Laures-Gore, J.; Love, K. Brief mindfulness meditation group training in aphasia: Exploring attention, language and psychophysiological outcomes. Int. J. Lang. Commun. Disord. 2018, 53, 40–54. [Google Scholar] [CrossRef]
- Johansson, B.; Bjuhr, H.; Rönnbäck, L. Evaluation of an advanced mindfulness program following a mindfulness-based stress reduction program for participants suffering from mental fatigue after acquired brain injury. Mindfulness 2015, 6, 227–233. [Google Scholar] [CrossRef]
- Ulrichsen, K.M.; Kaufmann, T.; Dørum, E.S.; Kolskår, K.K.; Richard, G.; Alnæs, D.; Arneberg, T.J.; Westlye, L.T.; Nordvik, J.E. Clinical utility of mindfulness training in the treatment of fatigue after stroke, traumatic brain injury and multiple sclerosis: A systematic literature review and meta-analysis. Front. Psychol. 2016, 7, 912. [Google Scholar] [CrossRef]
- Wang, X.; Smith, C.; Ashley, L.; Hyland, M.E. Tailoring self-help mindfulness and relaxation techniques for stroke survivors: Examining preferences, feasibility and acceptability. Front. Psychol. 2019, 10, 391. [Google Scholar] [CrossRef]
- Wang, M.; Liao, W.; Chen, X. Effects of a short-term mindfulness-based intervention on comfort of stroke survivors undergoing inpatient rehabilitation. Rehabil. Nurs. J. 2019, 44, 78–86. [Google Scholar] [CrossRef]
- Jani, B.D.; Simpson, R.; Lawrence, M.; Simpson, S.; Mercer, S.W. Acceptability of mindfulness from the perspective of stroke survivors and caregivers: A qualitative study. Pilot Feasibility Stud. 2018, 4, 57. [Google Scholar] [CrossRef] [Green Version]
- Denzin, N.K.; Lincoln, Y.S. The Landscape of Qualitative Research. Theories and Issues, 1st ed.; SAGE Publications: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Chang, H. Autoethnography as Method; Left Coast Press, Inc.: Walnut Creek, CA, USA, 2008; ISBN 1-59874-123-3. [Google Scholar]
- Sparkes, A.C. The fatal flaw: A narrative of the fragile body-self. Qual. Inq. 1996, 2, 463–494. [Google Scholar] [CrossRef]
- Wall, S. An autoethnography on learning about autoethnography. Int. J. Qual. Methods 2006, 5, 146–160. [Google Scholar] [CrossRef] [Green Version]
- Ellis, C. Heartful autoethnography. Qual. Health Res. 1999, 9, 669–683. [Google Scholar] [CrossRef]
- Bochner, A.P.; Ellis, C. Autoethnography, personal narrative, reflexivity: Researcher as subject. In Handbook of Qualitative Research; Denzin, N.K., Lincoln, Y.S., Eds.; Sage Publications: Thousand Oaks, CA, USA, 2000; pp. 733–768. [Google Scholar]
- Goodall, J. What is Interpretive Ethnography? In Expressions of Ethnography: Novel Approaches to Qualitative Methods; State University of New York Press: Albany, NY, USA, 2003; pp. 55–63. ISBN 0-7914-5824-5. [Google Scholar]
- Taylor-Powell, E.; Renner, M. Analyzing Qualitative Data; Program Development & Evaluation; University of Wisconsin—Extension: Madison, WI, USA, 2003; pp. 1–12. [Google Scholar]
- Santorelli, S.F.; Kabat-Zinn, J.; Blacker, M.; Meleo-Meyer, F.; Koerbel, L. Mindfulness-Based Stress Reduction (MBSR) Authorized Curriculum Guide; Center for Mindfulness in Medicine, Health Care, and Society (CFM); University of Massachusetts Medical School: Worcester, MA, USA, 2017. [Google Scholar]
- Stahl, B.; Goldstein, E. A Mindfulness-Based Stress Reduction Workbook; New Harbinger Publications: Oakland, CA, USA, 2019; ISBN 1-68403-357-8. [Google Scholar]
- Brach, T. RAIN: A Practice of Radical Compassion. Available online: https://www.tarabrach.com/rain-practice-radical-compassion/ (accessed on 1 September 2020).
- Crane, R.; Brewer, J.; Feldman, C.; Kabat-Zinn, J.; Santorelli, S.; Williams, J.; Kuyken, W. What defines mindfulness-based programs? The warp and the weft. Psychol. Med. 2017, 47, 990–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabat-Zinn, J. Some reflections on the origins of MBSR, skillful means, and the trouble with maps. Contemp. Buddhism 2011, 12, 281–306. [Google Scholar] [CrossRef]
- Crane, R.S.; Kuyken, W. The mindfulness-based interventions: Teaching assessment criteria (MBI: TAC): Reflections on implementation and development. Curr. Opin. Psychol. 2019, 28, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Crane, R.S.; Reid, B. Training mindfulness teachers: Principles, practices and challenges. In Resources for Teaching Mindfulness; McCown, D., Reibel, D., Micozzi, M., Eds.; Springer: Cham, Switzerland, 2016; pp. 121–140. [Google Scholar]
- Crane, R.S.; Hecht, F.M. Intervention integrity in mindfulness-based research. Mindfulness 2018, 9, 1370–1380. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| MBSR Classes 1 | Themes and Formal Mindfulness Practices | Home Practice Invitations | Suggested Modifications for MBRfS Classes |
|---|---|---|---|
| Week One: Introductions and Establishing Group | The Seven “Attitudes of Practice”. Introduction to definition of mindfulness. Mindful Eating Experience. Body Scan Practice. | Body Scan Meditation. Reminders of Attitudes. Eat a mindful meal. Noticing informal mindfulness. | Introductions and establishing the group. Recognizing that we are all on the same journey, but no two journeys are alike. Introducing the seven attitudes through the lens of stroke recovery Introduction to the body scan practice, with participant encouragement to “sense into” the stroke-affected side. Introduce a seated version of Mindful Walking practice, encouraging sensing into feet and the act of placing footsteps. Movement can be imagined if not possible on affected side. Honoring the need for rest. Sensing when brain is approaching neurofatigue and knowing when to slow down and take breaks. |
| Week Two: Perception and Stressors | Body Scan Meditation. Standing Yoga/Mindful Movement. Reflections of perception and stress. Introduction to seated Awareness of Breath (AOB) practice. | Body Scan Meditation. Awareness of Breathing Meditation. Fill out “Pleasant Events” calendar. Informal mindfulness. | Balancing compensation techniques with the importance to challenge current deficits in stroke recovery. Invitation to explore the unique stressors for stroke survivors. Very brief introduction to AOB practice, incorporated into body scan and offered as a very abbreviated “brain break” in working with neurofatigue. Mindful Walking (or seated walking) and modified Chair Yoga for standing postures. (imagining the movement if unable on affected side). |
| Week Three: Pleasant and Unpleasant experiences | AOB practice. Lying down Yoga/Mindful Movement Practice. Discussion of “Pleasant Events” homework. | Body Scan Meditation. Mindful Movement. Fill out “Unpleasant Event” Calendar. Awareness of Breathing Meditation. | Short practice sessions, including very short (3 min) breathe awareness practices as “brain breaks”. Teaching acronym: STOP (Stop, take a breath, Observe, and Proceed). 2 Mindful Walking (Standing or sitting options/modifications). Combine body scan with short sequence of lying down movements (imagining the movement if unable on affected side). Focused expression (invitation) on the experience of a pleasant events in the midst of stroke recovery. (“As long as you’re breathing, there’s more right than wrong happening with you, no matter what’s wrong.” 1) Hold this in your mind as you are able, expressing it either verbally or non-verbally. |
| Week Four: The Stress Cycle and responding to stressful events | Seated Mindfulness Meditation. Exploring how thoughts can contribute to stress. Responses to “Pleasant” and “Unpleasant” Events. Standing and lying down Yoga practice | Body Scan Meditation Yoga/Mindful Movement. Seated Mindfulness Meditation. Noting stress reactions and behaviors. | Short practice sessions, including very short (3 min) breath awareness practices as “brain breaks”. Mindful Walking and stretches (Standing or sitting options/modifications), Short practice sessions, including very short (3 min) breath awareness practices as “brain breaks”. Mindful Walking (Standing or sitting options/modifications). Combine Body Scan with short sequence of lying down movements, imagining the movement if unable on affected side). Combine Body Scan with seated meditation guidance. Invitation to express the experience of a pleasant and the additional element of unpleasant event in the midst of stroke recovery (e.g., allowing others to help, experiencing vulnerability as a stroke survivor). Hold this in your mind as you are able, expressing it either verbally or non-verbally. |
| Week Five: Moving from stress reactivity to responsivity. | Seated Mindfulness Meditation. Stress Reactivity vs. Stress Responsivity: What’s the difference? Introduction to Mindful Walking. | Alternate daily between Body Scan, Seated Meditation, and Yoga/Mindful Movement. Complete the “Difficult Communications” Calendar. Find informal moments to respond with responsive awareness. | Invite seated mindfulness practice lying down, standing, or sitting, encouraging change of posture as needed by sensing what the body needs and adjusting. Challenge, but not overwhelm. Mindful Walking (Standing or sitting options/modifications). Continue discussion of stressors related to recovery and possibilities for responding to stress rather than reacting. Positive neuroplasticity and the negativity bias. Challenging stressful thoughts and behaviors surrounding stroke recovery. Naming the common pitfalls of self-defeating beliefs about stroke recovery. Invitation to explore the challenge of navigating new and complex emotions, fear and developing courage. Teaching acronyms: RAIN (Recognize, Accept, Investigate, Nurture).3 |
| Week Six: Interpersonal mindfulness. | Seated Mindfulness Meditation. Mindful Walking Practice. Discussion of Difficult Communication Calendar and interpersonal stress. | Alternate daily between Body Scan, Seated Meditation, and Yoga/Mindful Movement. Mindful walking once this week. Awareness of interpersonal mindfulness and responding in communications with awareness. Informally pause and notice your breath throughout the day. | Invite seated mindfulness practice lying down, standing, or sitting, encouraging change of posture as needed. Challenge, but not overwhelm. Mindful Walking. (Standing or sitting options/modifications.) Invitation to express the experience of difficult communication. (Challenge in communication with caregivers, family, friends, and healthcare providers about your experience and needs in stroke recovery.) |
| Day of Mindfulness. | A Day of Silence during the weekend between class six and class seven to practice the formal mindfulness meditations together, including a mindful meal. Loving Kindness Meditation. Lake or Mountain guided imagery meditations. | Continue homework from Week Six. | Include rest breaks and a dedicated area for participants to rest/sleep as needed through the day. Loving Kindness meditation. Lake or Mountain guided imagery meditations. Provide simple and easy to eat, nutritious snacks for breaks (e.g., protein drinks, cut up fruit, nuts). Invitation to reflect on the role and relationship to rest as restoration and as an important companion for recovery. |
| Week Seven: Developing a home practice and continuing interpersonal mindfulness | Seated Mindfulness Meditation. Reflection on the Day of Mindfulness. Mindful Communication. Loving Kindness meditation. Lake or Mountain guided imagery meditations. | Practice with no audio guidance this week. Alternate practices daily (30–45 min) choosing a combination of Body Scan, Walking, Yoga, and Seated Mindful Meditation. Use the audio guidance if this feels frustrating to go without. | Invite Seated Mindfulness practice lying down, standing, or sitting, encouraging change of posture as needed. Challenge, but not overwhelm. Loving Kindness meditation. Lake or Mountain guided imagery meditations. Invitation to express, reflect, and acknowledge: Who am I now? How have my relationships been impacted? What do I need to care for my emotional health? |
| Week Eight: Coming Full Circle | Body Scan Meditation. Review and taking stock. Reflections and discussion. Closing the circle and saying goodbye. | Return to home practices in any combination, with and without guided audio recordings. | Combine Body Scan with guided Loving-Kindness practice, emphasizing Loving-Kindness for our bodies. Allow space for expression and review. Intention setting: The importance of the fundamental mindfulness attitudes and self-compassion to help us stay on the path. Practice Loving-Kindness. The end of this week creates a space filled with potential emotion, including fear. The eight weeks created a loving, compassionate, and thoughtful container that patients are now leaving. What elements of this transition might need to be considered? Allow space for expression of emotion and grief that may emerge with this ending. Offer a guided meditation that draws attention to the space of transition. Ongoing needed resources, social support, maintaining motivation. Continuing to make life-long gains in stroke recovery, accepting that recovery never ends. Life and rehab/recovery are our teachers and the “curriculum”. |
| Overarching Practices Across All Weeks (Emphasis on process) | Embodiment of practices and attitudes. Social Support. Commitment. | Classes weekly; Expand availability to include two identical sessions each week. This allows opportunity for missed days or the benefits of repetition and social contact. Create a resting space where participants can easily lie down or take additional breaks as needed. |
| Attitude | Definition of Attitude in Traditional MBSR Context | Suggested Expansion and/or Adaptation of Attitude in MBRfS Context |
|---|---|---|
| 1. Non-judgment | Practice of not being caught up in our ongoing assessments (both internal and external). Noticing ongoing automatic thoughts of judgments and self-criticism. | Noting self-criticism, judgments, or imposing stigma about having a stroke and efforts toward recovery. |
| 2. Patience | Recognizing that everything unfolds in its own time, some processes cannot be expedited. Patience contains its own kind of wisdom. | Patience in the stroke recovery journey and the length of the time it takes to heal the brain and regain lost abilities, also patience with setbacks during the recovery process. |
| 3. Beginner’s Mind | A willingness to see our experience with fresh eyes, a sense of newness rather than the patterns of our opinions, feelings and cognitions. Staying curious. | Using curiosity in assessing gains and not concluding that a recovery plateau has occurred. Staying open minded to see recovery with new eyes every day. |
| 4. Trust | Honoring and staying in tune with our instincts and our own inner compass for guidance. Relying on our basic goodness and wholeness. | Learning to trust the body and especial the brain to heal and guide us, seeing we are “whole” as stroke survivors. |
| 5. Non-Striving | To back off on the intensity to achieve or excessively pushing goal behaviors in hopes of getting desired results. | In stroke recovery, we must learn when and how far to challenge, but not push into overwhelm or regression. |
| 6. Acceptance | A willingness to see things as there presently are, not as we might wish them to be. Coming to terms with a situation rather than forcing or denying. Not to be confused with resignation or giving up. | Acceptance of experiencing stroke is critical to engaging in recovery. We do grieve, but accept what has happened. Acceptance means we engage more fully in recovery efforts sooner, which maximizes recovery potential. |
| 7. Letting Go | Practice of not grasping on to the things we want, while rejecting that which we do not want. Sometimes saying we can “leave it be” is a first step toward letting go. | For stroke survivors, we are challenged over and over, to let go of what our bodies and identities were before the stroke, while still engaging in recovery. |
| Formal Mindfulness Practice | Description in Traditional MBSR Context | Suggested Expansion and/or Adaptation in MBRfS Context |
|---|---|---|
| 1. Body Scan Meditation | Practiced while lying on back and sensing into the body from toes up through the top of the head, including invitations to breathe into each region of the body. Length of practice is approximately 45 min. | With all practices, offer a shorter version as an option to accommodate fatigue and concentration difficulties. Incorporate simple “sensory support” mechanisms on a person-by-person basis to stimulate sensory awareness and integration between the stroke-affected and non-affected sides, such as holding or squeezing small objects (e.g., a ball or stuffed animal). This may also include laying weighted objects gently across sections of the body, such as a weighted blanket. Guiding the Body Scan, similarly, adapting language to incorporate awareness of the stroke affected side of the body. More time encouraging somatic awareness, especially if there is numbness (very common). Still an emphasis on breathing into the whole body and imagining the body in its totality, with participant encouragement to “sense into” the stroke-affected side with whole body breath and with kindness, recognizing that participant may not have feeling in many places across the body. |
| 2. Mindful Walking Meditation | Practicing a deliberate walking pace that is slow and generally moves in a circle (if practicing in a group) or walking slowly and pivoting back and forth in a short row, focusing on the sensations in the feet and the movement of walking. Length of practice varies. | Offer a sitting version that allows just the practice of lifting and placing feet in the ground, or standing up in one place, placing each foot up and down. Or, placing the non-affected side but imagining the stroke affected foot moving (if there is paralysis on stroke affected side). With all practices, offer a shorter version as an option to accommodate fatigue and concentration difficulties. |
| 3. Yoga/Mindful Movement Sequences | Gentle stretching sequences of either standing or lying down Yoga postures. The emphasis is to practice very slowly as an exploration of breath and inviting movement into the body. Length of practice is approximately 30–45 min (two sequences offered, either standing or lying down postures). | Offer Chair Yoga versions of the Yoga postures. Invite visualization of all movements, with or without the ability to also move physically. Encourage “beginner’s mind” to challenge but not overwhelm. With all practices, offer a shorter version as an option to accommodate fatigue and concentration difficulties. Include invitations for the greatest possible movement in the present moment even if that is simply the extension of a finger or a foot placement (e.g., Finger Yoga). Visualization of exercise can offer benefits even if the individual is incapable of conventional kinds of physical exercise. |
| 4. Seated Mindfulness Meditations | Considered the central formal practice, Seated Mindfulness Meditation is practiced usually on a chair, cushion, or bench, with an upright posture with primary attention on the breath. When the mind is distracted, notice, and return attention gently again to the breath. Formal practice is variable, but the intention is to practice daily for around 45 min (may be combined with other formal practices listed above). | Invite any posture that feels right, and the permission to shift postures as needed. With all practices, offer a shorter version as an option to accommodate fatigue and concentration difficulties. |
| 5. Additional mindfulness meditation practices: Loving Kindness, imagery-based guided meditations (e.g., Lake and Mountain) | Loving-Kindness is a meditative practice from Buddhist traditions which encourages sending good wishes for health, happiness, and well-being, first to oneself and then to others. The Lake and Mountain Meditations are examples of guided imagery which suggest the embodiment of the symbolic qualities that different scenes of nature can teach us. | Invite any posture that feels right, and the permission to shift postures as needed. With all practices, offer a shorter version as an option to accommodate fatigue and concentration difficulties. Adapt Loving-Kindness to include compassion for the body and emphasize aspects of courage and strength with the nature-based guided imagery. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gray, L.A. Living the Full Catastrophe: A Mindfulness-Based Program to Support Recovery from Stroke. Healthcare 2020, 8, 498. https://doi.org/10.3390/healthcare8040498
Gray LA. Living the Full Catastrophe: A Mindfulness-Based Program to Support Recovery from Stroke. Healthcare. 2020; 8(4):498. https://doi.org/10.3390/healthcare8040498
Chicago/Turabian StyleGray, Lori A. 2020. "Living the Full Catastrophe: A Mindfulness-Based Program to Support Recovery from Stroke" Healthcare 8, no. 4: 498. https://doi.org/10.3390/healthcare8040498
APA StyleGray, L. A. (2020). Living the Full Catastrophe: A Mindfulness-Based Program to Support Recovery from Stroke. Healthcare, 8(4), 498. https://doi.org/10.3390/healthcare8040498