
The Effects of Mindfulness-Based Mandala Coloring, Made in Nature, on Chronic Widespread Musculoskeletal Pain: Randomized Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
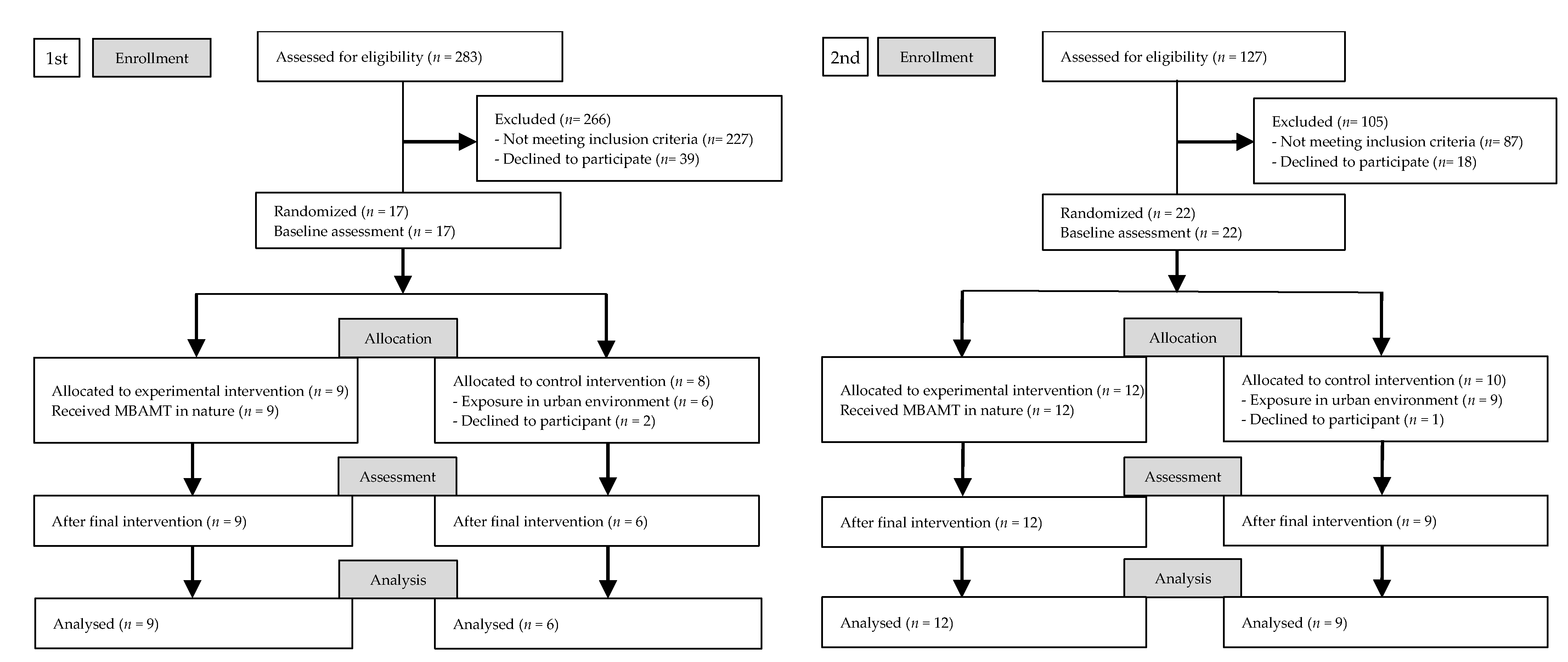
2.2. Participants
2.3. Instruments and Data Collection
2.3.1. Primary Instruments
2.3.2. Secondary Instruments
2.4. Procedure
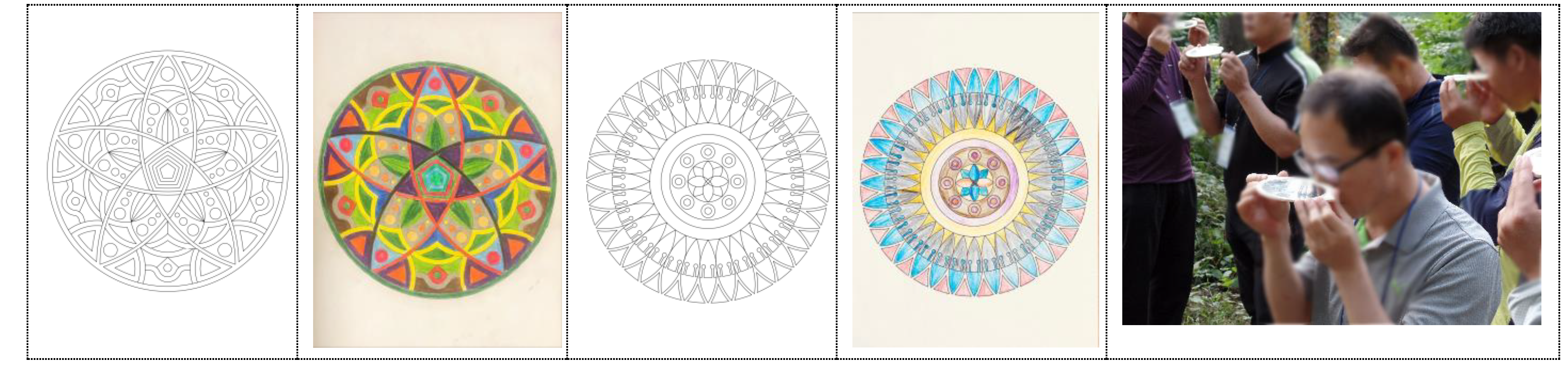
2.5. Interventions
2.6. Ethical Considerations
2.7. Data Analyses
3. Results
3.1. Participant Characteristics
3.2. Environmental and Meteorological Results
3.3. Physiological and Psychological Variables in the Overall Experiment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rustøen, T.; Wahl, A.K.; Hanestad, B.R.; Lerdal, A.; Paul, S.; Miaskowski, C. Gender differences in chronic pain—findings from a population-based study of Norwegian adults. Pain Manag. Nurs. 2004, 5, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Dureja, G.P.; Jain, P.N.; Shetty, N.; Mandal, S.P.; Prabhoo, R.; Joshi, M.; Goswami, S.; Natarajan, K.B.; Iyer, R.; Tanna, D.D.; et al. Prevalence of Chronic Pain, Impact on Daily Life, and Treatment Practices in India. Pain Pr. 2014, 14, E51–E62. [Google Scholar] [CrossRef] [PubMed]
- Lyon, P.; Cohen, M.; Quintner, J. An Evolutionary Stress-Response Hypothesis for Chronic Widespread Pain (Fibromyalgia Syndrome). Pain Med. 2011, 12, 1167–1178. [Google Scholar] [CrossRef] [PubMed]
- Burri, A.; Ogata, S.; Vehof, J.; Williams, F. Chronic widespread pain. Pain 2015, 156, 1458–1464. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Perrot, S.; Sommer, C.; Shir, Y.; Fitzcharles, M.-A. Diagnostic confounders of chronic widespread pain: Not always fibromyalgia. PAIN Rep. 2017, 2, e598. [Google Scholar] [CrossRef]
- De Rooij, A.; Roorda, L.D.; Otten, R.H.; Van Der Leeden, M.; Dekker, J.; Steultjens, M.P. Predictors of multidisciplinary treatment outcome in fibromyalgia:a systematic review. Disabil. Rehabil. 2012, 35, 437–449. [Google Scholar] [CrossRef]
- García, R.F.; Sánchez, L.D.C.S.; Rodríguez, M.D.M.L.; Granados, G.S. Effects of an exercise and relaxation aquatic program in patients with spondyloarthritis: A randomized trial. Med. Clín. (Engl. Ed.) 2015, 145, 380–384. [Google Scholar] [CrossRef]
- Bee, P.; McBeth, J.; Macfarlane, G.J.; Lovell, K. Managing chronic widespread pain in primary care: A qualitative study of patient perspectives and implications for treatment delivery. BMC Musculoskelet. Disord. 2016, 17, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, G.J.; Beasley, M.; Scott, N.; Chong, H.; McNamee, P.; McBeth, J.; Basu, N.; Hannaford, P.C.; Jones, G.T.; Keeley, P.; et al. Maintaining musculoskeletal health using a behavioural therapy approach: A population-based randomised controlled trial (the MAmMOTH Study). Ann. Rheum. Dis. 2021, 1–9. [Google Scholar] [CrossRef]
- Hilton, L.; Hempel, S.; Ewing, B.A.; Apaydin, E.; Xenakis, L.; Newberry, S.; Colaiaco, B.; Maher, A.R.; Shanman, R.M.; Sorbero, M.E.; et al. Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis. Ann. Behav. Med. 2017, 51, 199–213. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, K.H.; Goldenberg, D.L.; Galvin-Nadeau, M. The impact of a meditation-based stress reduction program on fibromyalgia. Gen. Hosp. Psychiatry 1993, 15, 284–289. [Google Scholar] [CrossRef]
- De Jong, M.; Lazar, S.W.; Hug, K.; Mehling, W.E.; Hölzel, B.K.; Sack, A.T.; Peeters, F.; Ashih, H.; Mischoulon, D.; Gard, T. Effects of Mindfulness-Based Cognitive Therapy on Body Awareness in Patients with Chronic Pain and Comorbid Depression. Front. Psychol. 2016, 7, 967. [Google Scholar] [CrossRef] [Green Version]
- Shipley, M. Chronic widespread pain and fibromyalgia syndrome. Medicine 2010, 38, 202–204. [Google Scholar] [CrossRef]
- Kabat-Zinn, J.; Hanh, T.N. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; De-lacorte: New York, NY, USA, 1990. [Google Scholar]
- Shapero, B.G.; Greenberg, J.; Pedrelli, P.; De Jong, M.; Desbordes, G. Mindfulness-Based Interventions in Psychiatry. Focus 2018, 16, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Meghani, S.H.; Peterson, C.; Kaiser, D.H.; Rhodes, J.; Rao, H.; Chittams, J.; Chatterjee, A. A Pilot Study of a Mindfulness-Based Art Therapy Intervention in Outpatients with Cancer. Am. J. Hosp. Palliat. Med. 2018, 35, 1195–1200. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Jung, D.-J.; Jeon, Y.-H.; Kim, M.J. The effects of combining art psychotherapy with pharmacotherapy in treating major depressive disorder: Randomized control study. Arts Psychother. 2020, 70, 101689. [Google Scholar] [CrossRef]
- Bullington, J.; Sjöström-Flanagan, C.; Nordemar, K.; Nordemar, R. From pain through chaos towards new meaning: Two case studies. Arts Psychother. 2005, 32, 261–274. [Google Scholar] [CrossRef]
- Pavlek, M. Paining Out: An Integrative Pain Therapy Model. Clin. Soc. Work. J. 2007, 36, 385–393. [Google Scholar] [CrossRef]
- Hass-Cohen, N.; Bokoch, R.; Goodman, K.; Conover, K.J. Art therapy drawing protocols for chronic pain: Quantitative results from a mixed method pilot study. Arts Psychother. 2021, 73, 101749. [Google Scholar] [CrossRef]
- Hass-Cohen, N.; Findlay, J.C. Pain, attachment, and meaning making: Report on an art therapy relational neuroscience assessment protocol. Arts Psychother. 2009, 36, 175–184. [Google Scholar] [CrossRef]
- O’Neill, A.; Moss, H. A Community Art Therapy Group for Adults with Chronic Pain. Art Ther. 2015, 32, 158–167. [Google Scholar] [CrossRef] [Green Version]
- Rappaport, L. Focusing-Oriented Art Therapy: Accessing the Body’s Wisdom and Creative Intelligence; Jessica Kingsley Publishers: London, UK; Philadelphia, PA, USA, 2009. [Google Scholar]
- Mantzios, M.; Giannou, K. When Did Coloring Books Become Mindful? Exploring the Effectiveness of a Novel Method of Mindfulness-Guided Instructions for Coloring Books to Increase Mindfulness and Decrease Anxiety. Front. Psychol. 2018, 9, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalambadani, Z.; Borji, A. Effectiveness of Mindfulness-Based Art Therapy on Healthy Quality of Life in Women with Breast Cancer. Asia-Pac. J. Oncol. Nurs. 2019, 6, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Monti, D.A.; Peterson, C.; Kunkel, E.J.S.; Hauck, W.W.; Pequignot, E.; Rhodes, L.; Brainard, G.C. A randomized, controlled trial of mindfulness-based art therapy (MBAT) for women with cancer. Psycho-Oncol. 2006, 15, 363–373. [Google Scholar] [CrossRef] [Green Version]
- Campenni, C.E.; Hartman, A. The Effects of Completing Mandalas on Mood, Anxiety, and State Mindfulness. Art Ther. 2019, 37, 25–33. [Google Scholar] [CrossRef]
- Kaimal, G.; Mensinger, J.L.; Drass, J.M.; Dieterich-Hartwell, R.M. Art Therapist-Facilitated Open Studio Versus Coloring: Differences in Outcomes of Affect, Stress, Creative Agency, and Self-Efficacy (Studio ouvert animé par un art-thérapeute versus coloriage: Différences de résultats sur l’affect, le stress, l’agentivité créatrice et l’efficacité personnelle). Can. Art Ther. Assoc. J. 2017, 30, 56–68. [Google Scholar] [CrossRef] [Green Version]
- Abbott, K.A.; Shanahan, M.J.; Neufeld, R.W.J. Artistic Tasks Outperform Nonartistic Tasks for Stress Reduction. Art Ther. 2013, 30, 71–78. [Google Scholar] [CrossRef]
- Huet, V. Case study of an art therapy-based group for work-related stress with hospice staff. Int. J. Art Ther. 2016, 22, 22–34. [Google Scholar] [CrossRef] [Green Version]
- Glinzak, L. Effects of Art Therapy on Distress Levels of Adults with Cancer: A Proxy Pretest Study. Art Ther. 2016, 33, 27–34. [Google Scholar] [CrossRef]
- Waller, D. Art Therapy for Children: How It Leads to Change. Clin. Child Psychol. Psychiatry 2006, 11, 271–282. [Google Scholar] [CrossRef] [PubMed]
- Lobban, J. Factors that influence engagement in an inpatient art therapy group for veterans with Post Traumatic Stress Disorder. Int. J. Art Ther. 2016, 21, 15–22. [Google Scholar] [CrossRef]
- Jung, W.H.; Woo, J.-M.; Ryu, J.S. Effect of a forest therapy program and the forest environment on female workers’ stress. Urban For. Urban Green. 2015, 14, 274–281. [Google Scholar] [CrossRef]
- Sonntag-Öström, E.; Nordin, M.; Järvholm, L.S.; Lundell, Y.; Brännström, R.; Dolling, A. Can the boreal forest be used for rehabilitation and recovery from stress-related exhaustion? A pilot study. Scand. J. For. Res. 2011, 26, 245–256. [Google Scholar] [CrossRef]
- de Vries, S.; van Dillen, S.M.; Groenewegen, P.P.; Spreeuwenberg, P. Streetscape greenery and health: Stress, social cohesion and physical activity as mediators. Soc. Sci. Med. 2013, 94, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Kang, B.; Kim, T.; Kim, M.J.; Lee, K.H.; Choi, S.; Lee, N.H.; Kim, H.R.; Jun, B.; Park, S.Y.; Lee, S.J.; et al. Relief of Chronic Posterior Neck Pain Depending on the Type of Forest Therapy: Comparison of the Therapeutic Effect of Forest Bathing Alone Versus Forest Bathing With Exercise. Ann. Rehabil. Med. 2015, 39, 957–963. [Google Scholar] [CrossRef] [Green Version]
- Han, J.-W.; Choi, H.; Jeon, Y.-H.; Yoon, C.-H.; Woo, J.-M.; Kim, W. The Effects of Forest Therapy on Coping with Chronic Widespread Pain: Physiological and Psychological Differences between Participants in a Forest Therapy Program and a Control Group. Int. J. Environ. Res. Public Health 2016, 13, 255. [Google Scholar] [CrossRef] [Green Version]
- Timmermans, H.; Choi, H.; Jeon, Y.-H.; Song, M.-K.; Kim, W.; Woo, J.-M. Comparison of Effect of Two-Hour Exposure to Forest and Urban Environments on Cytokine, Anti-Oxidant, and Stress Levels in Young Adults. Int. J. Environ. Res. Public Health 2016, 13, 625. [Google Scholar] [CrossRef] [Green Version]
- Mao, G.X.; Lan, X.G.; Cao, Y.B.; Chen, Z.M.; He, Z.H.; Lv, Y.D.; Wang, Y.Z.; Hu, X.L.; Wang, G.F.; Yan, J. Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang Province, China. Biomed. Environ. Sci. 2012, 25, 317–324. [Google Scholar] [PubMed]
- Atchley, R.A.; Strayer, D.L.; Atchley, P. Creativity in the Wild: Improving Creative Reasoning through Immersion in Natural Settings. PLoS ONE 2012, 7, e51474. [Google Scholar] [CrossRef]
- Yu, C.-P.; Hsieh, H. Beyond restorative benefits: Evaluating the effect of forest therapy on creativity. Urban For. Urban Green. 2020, 51, 126670. [Google Scholar] [CrossRef]
- Ulrich, R.S. View through a window may influence recovery from surgery. Science 1984, 224, 420–421. [Google Scholar] [CrossRef] [Green Version]
- Diette, G.B.; Lechtzin, N.; Haponik, E.; Devrotes, A.; Rubin, H.R. Distraction Therapy With Nature Sights and Sounds Reduces Pain During Flexible Bronchoscopya. Chest 2003, 123, 941–948. [Google Scholar] [CrossRef]
- Berger, R. Being in Nature. J. Holist. Nurs. 2009, 27, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Berger, R. Nature Therapy: Incorporating Nature Into Arts Therapy. J. Humanist. Psychol. 2017, 60, 244–257. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, R.D.C.P.; Pataro, S.M.S.; De Carvalho, R.B.; Burdorf, A. Erratum to: The concurrence of musculoskeletal pain and associated work-related factors: A cross sectional study. BMC Public Health 2016, 16, 1131. [Google Scholar] [CrossRef] [Green Version]
- Okifuji, A.; Turk, D.C.; Sinclair, J.D.; Starz, T.W.; Marcus, D. A standardized manual tender point survey. I. Development and determination of a threshold point for the identification of positive tender points in fibromyalgia syndrome. J. Rheumatol. 1997, 24, 377–383. [Google Scholar] [PubMed]
- Dave, N.D.; Xiang, L.; Rehm, K.E.; Marshall, G.D. Stress and Allergic Diseases. Immunol. Allergy Clin. N. Am. 2011, 31, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Fitzcharles, M.-A.; Goldenberg, N.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. Comparison of Physician-Based and Patient-Based Criteria for the Diagnosis of Fibromyalgia. Arthritis Rheum. 2015, 68, 652–659. [Google Scholar] [CrossRef] [Green Version]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The Fatigue Severity Scale: Application to Patients with Multiple Sclerosis and Systemic Lupus Erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Jeong, H.S.; Lim, S.M.; Cho, H.B.; Ma, J.Y.; Ko, E.; Lyoo, I.K.; Jeong, D.U. Reliability and Validity of the Fatigue Severity Scale among University Student in South Korea. Korean J. Biol. Psychiatry 2013, 20, 6–11. [Google Scholar]
- Choi, S.M.; Kang, T.Y.; Woo, J.M. Development and validation of a modified form of the stress response inventory for workers. J. Korean Neuropsychiatr. Assoc. 2006, 45, 541–553. [Google Scholar]
- Hellhammer, D.H.; Wüst, S.; Kudielka, B.M. Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology 2009, 34, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.; Debono, M. Review: Replication of cortisol circadian rhythm: New advances in hydrocortisone replacement therapy. Ther. Adv. Endocrinol. Metab. 2010, 1, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Newman, E.; O’Connor, D.B.; Conner, M. Daily hassles and eating behaviour: The role of cortisol reactivity status. Psychoneuroendocrinology 2007, 32, 125–132. [Google Scholar] [CrossRef]
- Lovallo, W.R.; Farag, N.H.; Vincent, A.S.; Thomas, T.L.; Wilson, M.F. Cortisol responses to mental stress, exercise, and meals following caffeine intake in men and women. Pharmacol. Biochem. Behav. 2006, 83, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Ba, N.A.C.; Kasser, T. Can Coloring Mandalas Reduce Anxiety? Art Ther. 2005, 22, 81–85. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Time Schedule | Experimental Group | Control Group | ||
|---|---|---|---|---|
| Activity | Location | Activity | Location | |
| 07:30–08:00 | Pre-test | Hospital | Pre-test | Hospital |
| 09:30–13:30 | Mindfulness-based Mandala Coloring | Natural Recreation Forest | Sightseeing Tour | Urban Area |
| 14:00–14:30 | Post-test | Hospital | Post-test | Hospital |
| Demographic Characteristics | First Experiment | Second Experiment | p | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Experimental Group | Control Group | Experimental Group | Control Group | ||||||
| M (SD) | n (%) | M (SD) | n (%) | M (SD) | n (%) | M (SD) | n (%) | ||
| Ethnicity | |||||||||
| Korean | 9 (100%) a | 6 (100%) a | 12 (100%) a | 9 (100%) a | |||||
| Gender | |||||||||
| Male | 5 (55.6%) a | 4 (66.7%) a | 9 (75.0%) a | 5 (55.6%) a | 0.676 | ||||
| Female | 4 (44.4%) a | 2 (33.3%) a | 3 (25.0%) a | 4 (44.4%) a | |||||
| Age (years) | 41.67 (4.64) b | 39.17 (6.37) b | 47.42 (5.52) b | 43.56 (4.93) b | 0.712 | ||||
| Height (cm) | 166.56 (8.90) b | 170.17 (8.40) b | 168.67 (7.58) b | 166.67 (7.18) b | 0.313 | ||||
| Weight (kg) | 67.89 (12.03) b | 66.83 (10.53) b | 71.67 (16.23) b | 68.11 (13.67) b | 0.794 | ||||
| Previous experience on treatment | |||||||||
| Yes | 6 (66.7%) a | 4 (66.7%) a | 6 (50.0%) a | 7 (77.8%) a | 0.748 | ||||
| No | 3 (33.3%) a | 2 (33.3%) a | 6 (50.0%) a | 2 (22.2%) a | |||||
| Variables | First Experiment | Second Experiment | Z | p |
|---|---|---|---|---|
| M (SD) | M (SD) | |||
| Temperature (°C) | 19.33 (1.91) | 21.18 (1.19) | −1.443 | 0.200 |
| Diurnal Temperature Range (h) | 11.88 (2.95) | 12.83 (2.06) | −0.289 | 0.886 |
| Relative humidity (%) | 66.55 (11.64) | 60.48 (21.62) | −0.289 | 0.886 |
| Sunshine duration (h) | 7.75 (3.08) | 9.63 (1.81) | −0.866 | 0.486 |
| Average wind speed (m/s) | 1.28 (0.55) | 1.53 (0.80) | −0.441 | 0.686 |
| NVOCs (mg/m3) | 1.00 (1.04) | 1.65 (0.83) | −1.680 | 0.093 |
| Dust (mg/m3) | 2.44 (0.02) | 2.43 (0.01) | −0.420 | 0.672 |
| Variables | Pre-Test | Post-Test | f | p | Post Hoc | ||
|---|---|---|---|---|---|---|---|
| M a (SD b) | M a (SD b) | t | Df | p | |||
| Tender Point | |||||||
| Experimental | 7.52 (3.20) | 3.81 (2.42) | 8.791 | 0.006 | 7.526 *** | 20 | 0.001 |
| Control | 6.73 (2.34) | 5.67 (2.23) | 1.331 | 14 | 0.205 | ||
| FSS | |||||||
| Experimental | 41.19 (9.13) | 37.90 (11.73) | 2.370 | 0.133 | 1.381 | 20 | 0.183 |
| Control | 42.93 (11.36) | 44.73 (13.82) | −0.885 | 14 | 0.391 | ||
| SRI-MF | |||||||
| Somatization Symptom | |||||||
| Experimental | 11.71 (8.31) | 7.29 (8.93) | 6.374 | 0.016 | 4.217 *** | 20 | 0.001 |
| Control | 13.53 (10.51) | 12.87 (11.07) | 0.688 | 14 | 0.503 | ||
| Depressive Symptom | |||||||
| Experimental | 9.48 (8.73) | 6.05 (8.82) | 15.205 | 0.000 | 5.056 *** | 20 | 0.001 |
| Control | 9.27 (10.14) | 9.73 (10.38) | −0.664 | 14 | 0.517 | ||
| Anger Symptom | |||||||
| Experimental | 5.57 (4.63) | 3.67 (5.16) | 7.263 | 0.011 | 4.119 ** | 20 | 0.001 |
| Control | 7.80 (6.20) | 7.47 (6.45) | 1.435 | 14 | 0.173 | ||
| Total Stress Level | |||||||
| Experimental | 28.10 (21.80) | 18.05 (23.47) | 14.570 | 0.001 | 5.691 *** | 20 | 0.001 |
| Control | 32.13 (26.63) | 31.53 (27.74) | 0.384 | 14 | 0.707 | ||
| Cortisol | |||||||
| Experimental | 0.24 (0.15) | 0.18 (0.13) | 10.619 | 0.003 | 4.045 ** | 20 | 0.001 |
| Control | 0.27 (0.20) | 0.30 (0.21) | −1.206 | 14 | 0.248 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.; Hahm, S.-C.; Jeon, Y.-H.; Han, J.-W.; Kim, S.-Y.; Woo, J.-M. The Effects of Mindfulness-Based Mandala Coloring, Made in Nature, on Chronic Widespread Musculoskeletal Pain: Randomized Trial. Healthcare 2021, 9, 642. https://doi.org/10.3390/healthcare9060642
Choi H, Hahm S-C, Jeon Y-H, Han J-W, Kim S-Y, Woo J-M. The Effects of Mindfulness-Based Mandala Coloring, Made in Nature, on Chronic Widespread Musculoskeletal Pain: Randomized Trial. Healthcare. 2021; 9(6):642. https://doi.org/10.3390/healthcare9060642
Chicago/Turabian StyleChoi, Han, Suk-Chan Hahm, Yo-Han Jeon, Jin-Woo Han, Soo-Yeon Kim, and Jong-Min Woo. 2021. "The Effects of Mindfulness-Based Mandala Coloring, Made in Nature, on Chronic Widespread Musculoskeletal Pain: Randomized Trial" Healthcare 9, no. 6: 642. https://doi.org/10.3390/healthcare9060642
APA StyleChoi, H., Hahm, S. -C., Jeon, Y. -H., Han, J. -W., Kim, S. -Y., & Woo, J. -M. (2021). The Effects of Mindfulness-Based Mandala Coloring, Made in Nature, on Chronic Widespread Musculoskeletal Pain: Randomized Trial. Healthcare, 9(6), 642. https://doi.org/10.3390/healthcare9060642