
Challenges and Opportunities of Targeted Behavioral Interventions for Groups at Risk for Developing Rheumatoid Arthritis

Abstract
:1. Introduction
2. Methods
3. Findings
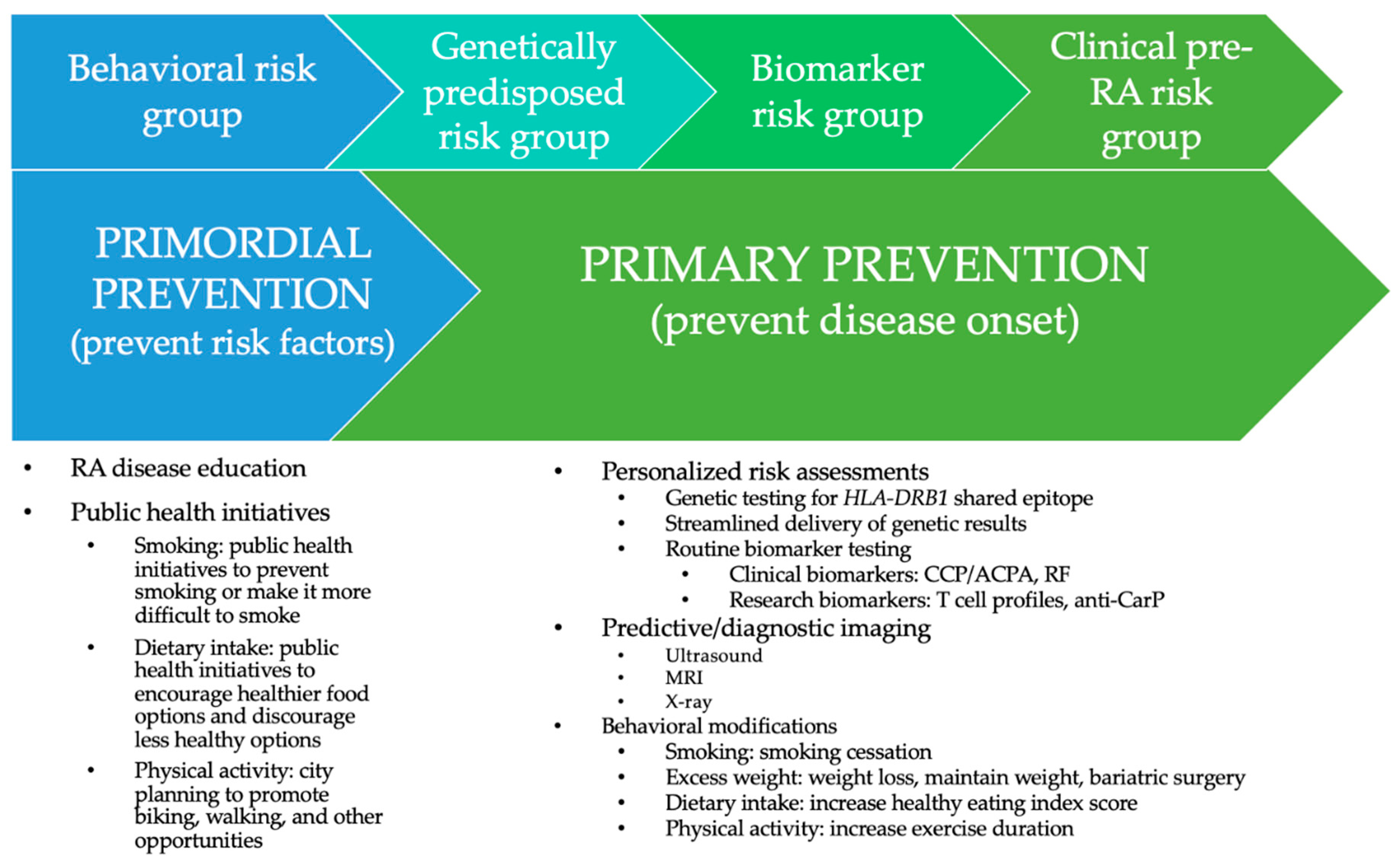
3.1. RA At-Risk Group 1: Behaviors
3.2. RA At-Risk Group 2: Genetics
3.3. RA At-Risk Group 3: Elevated Autoantibodies
3.4. RA At-Risk Group 4: Clinical RA Features
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alpizar-Rodriguez, D.; Finckh, A. Is the prevention of rheumatoid arthritis possible? Clin. Rheumatol. 2020, 39, 1383–1389. [Google Scholar] [CrossRef]
- Finckh, A.; Escher, M.; Liang, M.H.; Bansback, N. Preventive Treatments for Rheumatoid Arthritis: Issues Regarding Patient Preferences. Curr. Rheumatol. Rep. 2016, 18, 51. [Google Scholar] [CrossRef]
- Di Giuseppe, D.; Discacciati, A.; Orsini, N.; Wolk, A. Cigarette smoking and risk of rheumatoid arthritis: A dose-response meta-analysis. Arthritis Res. Ther. 2014, 16, R61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prisco, L.C.; Martin, L.W.; Sparks, J.A. Inhalants other than personal cigarette smoking and risk for developing rheumatoid arthritis. Curr. Opin. Rheumatol. 2020, 32, 279–288. [Google Scholar] [CrossRef]
- Feng, J.; Chen, Q.; Yu, F.; Wang, Z.; Chen, S.; Jin, Z.; Cai, Q.; Liu, Y.; He, J. Body Mass Index and Risk of Rheumatoid Arthritis: A Meta-Analysis of Observational Studies. Medicine 2016, 95, e2859. [Google Scholar] [CrossRef] [PubMed]
- Qin, B.; Yang, M.; Fu, H.; Ma, N.; Wei, T.; Tang, Q.; Hu, Z.; Liang, Y.; Yang, Z.; Zhong, R. Body mass index and the risk of rheumatoid arthritis: A systematic review and dose-response meta-analysis. Arthritis Res. Ther. 2015, 17, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Sun, M. A meta-analysis of the relationship between body mass index and risk of rheumatoid arthritis. EXCLI J. 2018, 17, 1079–1089. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Xu, X.; Shi, Y.; Liu, X.; Liu, H.; Hou, H.; Ji, L.; Li, Y.; Wang, W.; Wang, Y.; et al. Body Mass Index and the Risk of Rheumatoid Arthritis: An Updated Dose-Response Meta-Analysis. BioMed Res. Int. 2019, 2019, 3579081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Tedeschi, S.K.; Lu, B.; Zaccardelli, A.; Speyer, C.B.; Costenbader, K.H.; Karlson, E.W.; Sparks, J.A. Long-Term Physical Activity and Subsequent Risk for Rheumatoid Arthritis Among Women: A Prospective Cohort Study. Arthritis Rheumatol. 2019, 71, 1460–1471. [Google Scholar] [CrossRef]
- Di Giuseppe, D.; Crippa, A.; Orsini, N.; Wolk, A. Fish consumption and risk of rheumatoid arthritis: A dose-response meta-analysis. Arthritis Res. Ther. 2014, 16, 446. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira Ferreira, R.; de Brito Silva, R.; Magno, M.B.; Carvalho Almeida, A.; Fagundes, N.C.F.; Maia, L.C.; Lima, R.R. Does periodontitis represent a risk factor for rheumatoid arthritis? A systematic review and meta-analysis. Ther. Adv. Musculoskelet. Dis. 2019, 11, 1759720X19858514. [Google Scholar] [CrossRef]
- Alpizar-Rodriguez, D.; Lesker, T.R.; Gronow, A.; Gilbert, B.; Raemy, E.; Lamacchia, C.; Gabay, C.; Finckh, A.; Strowig, T. Prevotella copri in individuals at risk for rheumatoid arthritis. Ann. Rheum. Dis. 2019, 78, 590–593. [Google Scholar] [CrossRef] [PubMed]
- Scher, J.U.; Sczesnak, A.; Longman, R.S.; Segata, N.; Ubeda, C.; Bielski, C.; Rostron, T.; Cerundolo, V.; Pamer, E.G.; Abramson, S.B.; et al. Expansion of intestinal Prevotella copri correlates with enhanced susceptibility to arthritis. Elife 2013, 2, e01202. [Google Scholar] [CrossRef]
- Lee, Y.C.; Agnew-Blais, J.; Malspeis, S.; Keyes, K.; Costenbader, K.; Kubzansky, L.D.; Roberts, A.L.; Koenen, K.C.; Karlson, E.W. Post-Traumatic Stress Disorder and Risk for Incident Rheumatoid Arthritis. Arthritis Care Res. 2016, 68, 292–298. [Google Scholar] [CrossRef] [Green Version]
- Sparks, J.A.; Malspeis, S.; Hahn, J.; Wang, J.; Roberts, A.L.; Kubzansky, L.D.; Costenbader, K.H. Depression and Subsequent Risk for Incident Rheumatoid Arthritis Among Women. Arthritis Care Res. 2021, 73, 78–89. [Google Scholar] [CrossRef]
- Zaccardelli, A.; Friedlander, H.M.; Ford, J.A.; Sparks, J.A. Potential of Lifestyle Changes for Reducing the Risk of Developing Rheumatoid Arthritis: Is an Ounce of Prevention Worth a Pound of Cure? Clin. Ther. 2019, 41, 1323–1345. [Google Scholar] [CrossRef]
- Zaccardelli, A.; Liu, X.; Ford, J.A.; Cui, J.; Lu, B.; Chu, S.H.; Schur, P.H.; Speyer, C.B.; Costenbader, K.H.; Robinson, W.H.; et al. Asthma and elevation of anti-citrullinated protein antibodies prior to the onset of rheumatoid arthritis. Arthritis Res. Ther. 2019, 21, 246. [Google Scholar] [CrossRef] [Green Version]
- Zaccardelli, A.; Liu, X.; Ford, J.A.; Cui, J.; Lu, B.; Chu, S.H.; Schur, P.H.; Speyer, C.B.; Costenbader, K.H.; Robinson, W.H.; et al. Elevated anti-citrullinated protein antibodies prior to rheumatoid arthritis diagnosis and risks for chronic obstructive pulmonary disease or asthma. Arthritis Care Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sparks, J.A.; Karlson, E.W. The Roles of Cigarette Smoking and the Lung in the Transitions Between Phases of Preclinical Rheumatoid Arthritis. Curr. Rheumatol. Rep. 2016, 18, 15. [Google Scholar] [CrossRef]
- Klareskog, L.; Stolt, P.; Lundberg, K.; Kallberg, H.; Bengtsson, C.; Grunewald, J.; Ronnelid, J.; Harris, H.E.; Ulfgren, A.K.; Rantapaa-Dahlqvist, S.; et al. A new model for an etiology of rheumatoid arthritis: Smoking may trigger HLA-DR (shared epitope)-restricted immune reactions to autoantigens modified by citrullination. Arthritis Rheum. 2006, 54, 38–46. [Google Scholar] [CrossRef]
- Karlson, E.W.; Chang, S.C.; Cui, J.; Chibnik, L.B.; Fraser, P.A.; De Vivo, I.; Costenbader, K.H. Gene-environment interaction between HLA-DRB1 shared epitope and heavy cigarette smoking in predicting incident rheumatoid arthritis. Ann. Rheum. Dis. 2010, 69, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Too, C.L.; Yahya, A.; Murad, S.; Dhaliwal, J.S.; Larsson, P.T.; Muhamad, N.A.; Abdullah, N.A.; Mustafa, A.N.; Klareskog, L.; Alfredsson, L.; et al. Smoking interacts with HLA-DRB1 shared epitope in the development of anti-citrullinated protein antibody-positive rheumatoid arthritis: Results from the Malaysian Epidemiological Investigation of Rheumatoid Arthritis (MyEIRA). Arthritis Res. Ther. 2012, 14, R89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padyukov, L.; Silva, C.; Stolt, P.; Alfredsson, L.; Klareskog, L. A gene-environment interaction between smoking and shared epitope genes in HLA-DR provides a high risk of seropositive rheumatoid arthritis. Arthritis Rheum. 2004, 50, 3085–3092. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Irigoyen, P.; Kern, M.; Lee, A.; Batliwalla, F.; Khalili, H.; Wolfe, F.; Lum, R.F.; Massarotti, E.; Weisman, M.; et al. Interaction between smoking, the shared epitope, and anti-cyclic citrullinated peptide: A mixed picture in three large North American rheumatoid arthritis cohorts. Arthritis Rheum. 2007, 56, 1745–1753. [Google Scholar] [CrossRef]
- Linn-Rasker, S.P.; van der Helm-van Mil, A.H.; van Gaalen, F.A.; Kloppenburg, M.; de Vries, R.R.; le Cessie, S.; Breedveld, F.C.; Toes, R.E.; Huizinga, T.W. Smoking is a risk factor for anti-CCP antibodies only in rheumatoid arthritis patients who carry HLA-DRB1 shared epitope alleles. Ann. Rheum. Dis. 2006, 65, 366–371. [Google Scholar] [CrossRef] [Green Version]
- Sugiyama, D.; Nishimura, K.; Tamaki, K.; Tsuji, G.; Nakazawa, T.; Morinobu, A.; Kumagai, S. Impact of smoking as a risk factor for developing rheumatoid arthritis: A meta-analysis of observational studies. Ann. Rheum. Dis. 2010, 69, 70–81. [Google Scholar] [CrossRef] [Green Version]
- Kallberg, H.; Ding, B.; Padyukov, L.; Bengtsson, C.; Ronnelid, J.; Klareskog, L.; Alfredsson, L.; Group, E.S. Smoking is a major preventable risk factor for rheumatoid arthritis: Estimations of risks after various exposures to cigarette smoke. Ann. Rheum. Dis. 2011, 70, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Symmons, D.P.; Bankhead, C.R.; Harrison, B.J.; Brennan, P.; Barrett, E.M.; Scott, D.G.; Silman, A.J. Blood transfusion, smoking, and obesity as risk factors for the development of rheumatoid arthritis: Results from a primary care-based incident case-control study in Norfolk, England. Arthritis Rheum. 1997, 40, 1955–1961. [Google Scholar] [CrossRef]
- de Hair, M.J.; Landewe, R.B.; van de Sande, M.G.; van Schaardenburg, D.; van Baarsen, L.G.; Gerlag, D.M.; Tak, P.P. Smoking and overweight determine the likelihood of developing rheumatoid arthritis. Ann. Rheum. Dis. 2013, 72, 1654–1658. [Google Scholar] [CrossRef] [PubMed]
- Ohno, T.; Aune, D.; Heath, A.K. Adiposity and the risk of rheumatoid arthritis: A systematic review and meta-analysis of cohort studies. Sci. Rep. 2020, 10, 16006. [Google Scholar] [CrossRef]
- Mora, S.; Cook, N.; Buring, J.E.; Ridker, P.M.; Lee, I.M. Physical activity and reduced risk of cardiovascular events: Potential mediating mechanisms. Circulation 2007, 116, 2110–2118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, L.; Zhu, J.; Ling, Y.; Mi, S.; Li, Y.; Wang, T.; Li, Y. Physical activity and the risk of rheumatoid arthritis: Evidence from meta-analysis and Mendelian randomization. Int. J. Epidemiol. 2021. [Google Scholar] [CrossRef]
- Pattison, D.J.; Symmons, D.P.; Lunt, M.; Welch, A.; Luben, R.; Bingham, S.A.; Khaw, K.T.; Day, N.E.; Silman, A.J. Dietary risk factors for the development of inflammatory polyarthritis: Evidence for a role of high level of red meat consumption. Arthritis Rheum. 2004, 50, 3804–3812. [Google Scholar] [CrossRef] [PubMed]
- Benito-Garcia, E.; Feskanich, D.; Hu, F.B.; Mandl, L.A.; Karlson, E.W. Protein, iron, and meat consumption and risk for rheumatoid arthritis: A prospective cohort study. Arthritis Res. Ther. 2007, 9, R16. [Google Scholar] [CrossRef] [Green Version]
- Linos, A.; Kaklamani, V.G.; Kaklamani, E.; Koumantaki, Y.; Giziaki, E.; Papazoglou, S.; Mantzoros, C.S. Dietary factors in relation to rheumatoid arthritis: A role for olive oil and cooked vegetables? Am. J. Clin. Nutr. 1999, 70, 1077–1082. [Google Scholar] [CrossRef] [Green Version]
- Rosell, M.; Wesley, A.M.; Rydin, K.; Klareskog, L.; Alfredsson, L. Dietary fish and fish oil and the risk of rheumatoid arthritis. Epidemiology 2009, 20, 896–901. [Google Scholar] [CrossRef]
- Di Giuseppe, D.; Wallin, A.; Bottai, M.; Askling, J.; Wolk, A. Long-term intake of dietary long-chain n-3 polyunsaturated fatty acids and risk of rheumatoid arthritis: A prospective cohort study of women. Ann. Rheum. Dis. 2014, 73, 1949–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, J.A.; Koepsell, T.D.; Voigt, L.F.; Dugowson, C.E.; Kestin, M.; Nelson, J.L. Diet and rheumatoid arthritis in women: A possible protective effect of fish consumption. Epidemiology 1996, 7, 256–263. [Google Scholar] [CrossRef]
- Mikuls, T.R.; Cerhan, J.R.; Criswell, L.A.; Merlino, L.; Mudano, A.S.; Burma, M.; Folsom, A.R.; Saag, K.G. Coffee, tea, and caffeine consumption and risk of rheumatoid arthritis: Results from the Iowa Women’s Health Study. Arthritis Rheum. 2002, 46, 83–91. [Google Scholar] [CrossRef]
- Heliovaara, M.; Aho, K.; Knekt, P.; Impivaara, O.; Reunanen, A.; Aromaa, A. Coffee consumption, rheumatoid factor, and the risk of rheumatoid arthritis. Ann. Rheum. Dis. 2000, 59, 631–635. [Google Scholar] [CrossRef] [Green Version]
- Pattison, D.; Silman, A.; Goodson, N.; Lunt, M.; Bunn, D.; Luben, R.; Welch, A.; Bingham, S.; Khaw, K.; Day, N. Vitamin C and the risk of developing inflammatory polyarthritis: Prospective nested case-control study. Ann. Rheum. Dis. 2004, 63, 843–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Y.; Sparks, J.A.; Malspeis, S.; Costenbader, K.H.; Hu, F.B.; Karlson, E.W.; Lu, B. Long-term dietary quality and risk of developing rheumatoid arthritis in women. Ann. Rheum. Dis. 2017, 76, 1357–1364. [Google Scholar] [CrossRef]
- Sparks, J.A.; Chen, C.Y.; Hiraki, L.T.; Malspeis, S.; Costenbader, K.H.; Karlson, E.W. Contributions of familial rheumatoid arthritis or lupus and environmental factors to risk of rheumatoid arthritis in women: A prospective cohort study. Arthritis Care Res. 2014, 66, 1438–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahn, J.; Choi, M.; Malspeis, S.; Stevens, E.; Karlson, E.W.; Yoshida, K.; Kubzansky, L.; Sparks, J.A.; Costenbader, K.H. Healthy Lifestyle and Risk of Rheumatoid Arthritis in Women: A Prospective Cohort Study. In Proceedings of the ACR Convergence, Online, 8 November 2020. [Google Scholar]
- Liu, X.; Tedeschi, S.K.; Barbhaiya, M.; Leatherwood, C.L.; Speyer, C.B.; Lu, B.; Costenbader, K.H.; Karlson, E.W.; Sparks, J.A. Impact and Timing of Smoking Cessation on Reducing Risk of Rheumatoid Arthritis Among Women in the Nurses’ Health Studies. Arthritis Care Res. 2019, 71, 914–924. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, D.; Orsini, N.; Alfredsson, L.; Askling, J.; Wolk, A. Cigarette smoking and smoking cessation in relation to risk of rheumatoid arthritis in women. Arthritis Res. Ther. 2013, 15, R56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costenbader, K.H.; Feskanich, D.; Mandl, L.A.; Karlson, E.W. Smoking intensity, duration, and cessation, and the risk of rheumatoid arthritis in women. Am. J. Med. 2006, 119, 503.e1–503.e9. [Google Scholar] [CrossRef]
- Marchand, N.; Sparks, J.A.; Yoshida, K.; Malspeis, S.; Xuehong, Z.; Costenbader, K.H.; Karlson, E.W.; Lu, B. Long-term Weight Changes and Risk of Rheumatoid Arthritis Among Women in a Prospective Cohort: A Marginal Structural Model Approach. In Proceedings of the ACR Convergence, Online, 8 November 2020. [Google Scholar]
- Maglio, C.; Zhang, Y.; Peltonen, M.; Andersson-Assarsson, J.; Svensson, P.A.; Herder, C.; Rudin, A.; Carlsson, L. Bariatric surgery and the incidence of rheumatoid arthritis—A Swedish Obese Subjects study. Rheumatology 2020, 59, 303–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Stadt, L.A.; van Schaardenburg, D. Alcohol consumption protects against arthritis development in seropositive arthralgia patients. Ann. Rheum. Dis. 2012, 71, 1431–1432. [Google Scholar] [CrossRef]
- Pattison, D.J.; Symmons, D.P.; Lunt, M.; Welch, A.; Bingham, S.A.; Day, N.E.; Silman, A.J. Dietary β-cryptoxanthin and inflammatory polyarthritis: Results from a population-based prospective study. Am. J. Clin. Nutr. 2005, 82, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Marchand, N.; Chiu, Y.; Yoshida, K.; Malspeis, S.; Sparks, J.A.; Costenbader, K.H.; Karlson, E.W.; Lu, B. Threshold Level for Long-term Healthy Diet Adherence to Reduce the Risk of Rheumatoid Arthritis Among Women in a Prospective Cohort Using a Marginal Structural Model Approach. In Proceedings of the ACR Convergence, Online, 8 November 2020. [Google Scholar]
- Simons, G.; Mason, A.; Falahee, M.; Kumar, K.; Mallen, C.D.; Raza, K.; Stack, R.J. Qualitative Exploration of Illness Perceptions of Rheumatoid Arthritis in the General Public. Musculoskelet. Care 2017, 15, 13–22. [Google Scholar] [CrossRef]
- Prado, M.G.; Iversen, M.D.; Yu, Z.; Miller Kroouze, R.; Triedman, N.A.; Kalia, S.S.; Lu, B.; Green, R.C.; Karlson, E.W.; Sparks, J.A. Effectiveness of a Web-Based Personalized Rheumatoid Arthritis Risk Tool with or Without a Health Educator for Knowledge of Rheumatoid Arthritis Risk Factors. Arthritis Care Res. 2018, 70, 1421–1430. [Google Scholar] [CrossRef] [Green Version]
- Sparks, J.A.; Iversen, M.D.; Yu, Z.; Triedman, N.A.; Prado, M.G.; Miller Kroouze, R.; Kalia, S.S.; Atkinson, M.L.; Mody, E.A.; Helfgott, S.M.; et al. Disclosure of Personalized Rheumatoid Arthritis Risk Using Genetics, Biomarkers, and Lifestyle Factors to Motivate Health Behavior Improvements: A Randomized Controlled Trial. Arthritis Care Res. 2018, 70, 823–833. [Google Scholar] [CrossRef]
- Sparks, J.A.; Iversen, M.D.; Miller Kroouze, R.; Mahmoud, T.G.; Triedman, N.A.; Kalia, S.S.; Atkinson, M.L.; Lu, B.; Deane, K.D.; Costenbader, K.H.; et al. Personalized Risk Estimator for Rheumatoid Arthritis (PRE-RA) Family Study: Rationale and design for a randomized controlled trial evaluating rheumatoid arthritis risk education to first-degree relatives. Contemp. Clin. Trials 2014, 39, 145–157. [Google Scholar] [CrossRef] [Green Version]
- Marshall, A.A.; Zaccardelli, A.; Yu, Z.; Prado, M.G.; Liu, X.; Miller Kroouze, R.; Kalia, S.S.; Green, R.C.; Triedman, N.A.; Lu, B.; et al. Effect of communicating personalized rheumatoid arthritis risk on concern for developing RA: A randomized controlled trial. Patient Educ. Couns. 2019, 102, 976–983. [Google Scholar] [CrossRef]
- Stack, R.J.; Stoffer, M.; Englbrecht, M.; Mosor, E.; Falahee, M.; Simons, G.; Smolen, J.; Schett, G.; Buckley, C.D.; Kumar, K.; et al. Perceptions of risk and predictive testing held by the first-degree relatives of patients with rheumatoid arthritis in England, Austria and Germany: A qualitative study. BMJ Open 2016, 6, e010555. [Google Scholar] [CrossRef] [Green Version]
- Simons, G.; Stack, R.J.; Stoffer-Marx, M.; Englbrecht, M.; Mosor, E.; Buckley, C.D.; Kumar, K.; Hansson, M.; Hueber, A.; Stamm, T.; et al. Perceptions of first-degree relatives of patients with rheumatoid arthritis about lifestyle modifications and pharmacological interventions to reduce the risk of rheumatoid arthritis development: A qualitative interview study. BMC Rheumatol. 2018, 2, 31. [Google Scholar] [CrossRef] [PubMed]
- Perez-Barbosa, L.; Garza-Elizondo, M.A.; Vega-Morales, D.; Esquivel-Valerio, J.A.; Pelaez-Ballestas, I.; Vazquez-Fuentes, B.R.; Galarza-Delgado, D.A. High frequency of rheumatic regional pain syndromes in first-degree relatives of patients with rheumatoid arthritis. Clin. Rheumatol. 2020, 39, 3303–3307. [Google Scholar] [CrossRef]
- Raychaudhuri, S.; Sandor, C.; Stahl, E.A.; Freudenberg, J.; Lee, H.S.; Jia, X.; Alfredsson, L.; Padyukov, L.; Klareskog, L.; Worthington, J.; et al. Five amino acids in three HLA proteins explain most of the association between MHC and seropositive rheumatoid arthritis. Nat. Genet. 2012, 44, 291–296. [Google Scholar] [CrossRef]
- Schulz, S.; Zimmer, P.; Putz, N.; Jurianz, E.; Schaller, H.G.; Reichert, S. rs2476601 in PTPN22 gene in rheumatoid arthritis and periodontitis-a possible interface? J. Transl. Med. 2020, 18, 389. [Google Scholar] [CrossRef]
- Okada, Y.; Wu, D.; Trynka, G.; Raj, T.; Terao, C.; Ikari, K.; Kochi, Y.; Ohmura, K.; Suzuki, A.; Yoshida, S.; et al. Genetics of rheumatoid arthritis contributes to biology and drug discovery. Nature 2014, 506, 376–381. [Google Scholar] [CrossRef]
- Silman, A.J.; MacGregor, A.J.; Thomson, W.; Holligan, S.; Carthy, D.; Farhan, A.; Ollier, W.E. Twin concordance rates for rheumatoid arthritis: Results from a nationwide study. Br. J. Rheumatol. 1993, 32, 903–907. [Google Scholar] [CrossRef]
- Munro, S.; Spooner, L.; Milbers, K.; Hudson, M.; Koehn, C.; Harrison, M. Perspectives of patients, first-degree relatives and rheumatologists on preventive treatments for rheumatoid arthritis: A qualitative analysis. BMC Rheumatol. 2018, 2, 18. [Google Scholar] [CrossRef] [Green Version]
- Falahee, M.; Simons, G.; Buckley, C.D.; Hansson, M.; Stack, R.J.; Raza, K. Patients’ Perceptions of Their Relatives’ Risk of Developing Rheumatoid Arthritis and of the Potential for Risk Communication, Prediction, and Modulation. Arthritis Care Res. 2017, 69, 1558–1565. [Google Scholar] [CrossRef]
- Mosor, E.; Stoffer-Marx, M.; Steiner, G.; Raza, K.; Stack, R.J.; Simons, G.; Falahee, M.; Skingle, D.; Dobrin, M.; Schett, G.; et al. I Would Never Take Preventive Medication! Perspectives and Information Needs of People Who Underwent Predictive Tests for Rheumatoid Arthritis. Arthritis Care Res. 2020, 72, 360–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novotny, F.; Haeny, S.; Hudelson, P.; Escher, M.; Finckh, A. Primary prevention of rheumatoid arthritis: A qualitative study in a high-risk population. Jt. Bone Spine 2013, 80, 673–674. [Google Scholar] [CrossRef] [PubMed]
- Falahee, M.; Finckh, A.; Raza, K.; Harrison, M. Preferences of Patients and At-risk Individuals for Preventive Approaches to Rheumatoid Arthritis. Clin. Ther. 2019, 41, 1346–1354. [Google Scholar] [CrossRef]
- Lautenbach, D.M.; Christensen, K.D.; Sparks, J.A.; Green, R.C. Communicating genetic risk information for common disorders in the era of genomic medicine. Annu. Rev. Genom. Hum. Genet. 2013, 14, 491–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamacchia, C.; Calderin Sollet, Z.; Courvoisier, D.; Mongin, D.; Palmer, G.; Studer, O.; Gabay, C.; Villard, J.; Buhler, S.; Finckh, A. Detection of circulating highly expanded T-cell clones in at-risk individuals for rheumatoid arthritis before the clinical onset of the disease. Rheumatology 2020. [Google Scholar] [CrossRef]
- Lamacchia, C.; Courvoisier, D.S.; Jarlborg, M.; Bas, S.; Roux-Lombard, P.; Moller, B.; Ciurea, A.; Finckh, A.; Bentow, C.; Martinez-Prat, L.; et al. Predictive value of anti-CarP and anti-PAD3 antibodies alone or in combination with RF and ACPA on the severity of rheumatoid arthritis. Rheumatology 2021. [Google Scholar] [CrossRef] [PubMed]
- van Zanten, A.; Arends, S.; Roozendaal, C.; Limburg, P.C.; Maas, F.; Trouw, L.A.; Toes, R.E.M.; Huizinga, T.W.J.; Bootsma, H.; Brouwer, E. Presence of anticitrullinated protein antibodies in a large population-based cohort from the Netherlands. Ann. Rheum. Dis. 2017, 76, 1184–1190. [Google Scholar] [CrossRef]
- Alpizar-Rodriguez, D.; Brulhart, L.; Mueller, R.B.; Moller, B.; Dudler, J.; Ciurea, A.; Walker, U.A.; Von Muhlenen, I.; Kyburz, D.; Zufferey, P.; et al. The prevalence of anticitrullinated protein antibodies increases with age in healthy individuals at risk for rheumatoid arthritis. Clin. Rheumatol. 2017, 36, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Cambre, I.; Gaublomme, D.; Burssens, A.; Jacques, P.; Schryvers, N.; De Muynck, A.; Meuris, L.; Lambrecht, S.; Carter, S.; de Bleser, P.; et al. Mechanical strain determines the site-specific localization of inflammation and tissue damage in arthritis. Nat. Commun. 2018, 9, 4613. [Google Scholar] [CrossRef] [Green Version]
- Newsum, E.C.; van der Helm-van Mil, A.H.; Kaptein, A.A. Views on clinically suspect arthralgia: A focus group study. Clin. Rheumatol. 2016, 35, 1347–1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duquenne, L.; Chowdhury, R.; Mankia, K.; Emery, P. The Role of Ultrasound Across the Inflammatory Arthritis Continuum: Focus on “At-Risk” Individuals. Front. Med. 2020, 7, 587827. [Google Scholar] [CrossRef] [PubMed]
- Matthijssen, X.M.E.; Wouters, F.; Boeters, D.M.; Boer, A.C.; Dakkak, Y.J.; Niemantsverdriet, E.; van der Helm-van Mil, A.H.M. A search to the target tissue in which RA-specific inflammation starts: A detailed MRI study to improve identification of RA-specific features in the phase of clinically suspect arthralgia. Arthritis Res. Ther. 2019, 21, 249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boer, A.C.; Wouters, F.; Dakkak, Y.J.; Niemantsverdriet, E.; van der Helm-van Mil, A.H.M. Improving the feasibility of MRI in clinically suspect arthralgia for prediction of rheumatoid arthritis by omitting scanning of the feet. Rheumatology 2020, 59, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Sparks, J.A.; Chen, C.Y.; Jiang, X.; Askling, J.; Hiraki, L.T.; Malspeis, S.; Klareskog, L.; Alfredsson, L.; Costenbader, K.H.; Karlson, E.W. Improved performance of epidemiologic and genetic risk models for rheumatoid arthritis serologic phenotypes using family history. Ann. Rheum. Dis. 2015, 74, 1522–1529. [Google Scholar] [CrossRef] [Green Version]
- Rakieh, C.; Nam, J.L.; Hunt, L.; Hensor, E.M.; Das, S.; Bissell, L.A.; Villeneuve, E.; McGonagle, D.; Hodgson, R.; Grainger, A.; et al. Predicting the development of clinical arthritis in anti-CCP positive individuals with non-specific musculoskeletal symptoms: A prospective observational cohort study. Ann. Rheum. Dis. 2015, 74, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- van de Stadt, L.A.; Witte, B.I.; Bos, W.H.; van Schaardenburg, D. A prediction rule for the development of arthritis in seropositive arthralgia patients. Ann. Rheum. Dis. 2013, 72, 1920–1926. [Google Scholar] [CrossRef]
- Niemantsverdriet, E.; van den Akker, E.B.; Boeters, D.M.; van den Eeden, S.J.F.; Geluk, A.; van der Helm-van Mil, A.H.M. Gene expression identifies patients who develop inflammatory arthritis in a clinically suspect arthralgia cohort. Arthritis Res. Ther. 2020, 22, 266. [Google Scholar] [CrossRef]


{kind=link}
| Behavioral Risk Factor and Comparisons | Sex | Direction of Association | RR or OR for RA (95% CI) | Author (Year) of Reference |
|---|---|---|---|---|
| Smoking | ||||
| 1–10 pack-years/>20 pack-years/>40 pack-years vs. never smoker | All | ↑ | RR 1.26 (1.14–1.39) RR 1.95 (1.65–2.27) RR 2.07 (1.15–3.73) | Di Giuseppe (2014) [3] |
| High (>40 pack-years) vs. low (never smoker) | All * | ↑ | RR 2.47 (2.02–3.02) | Di Giuseppe (2014) [3] |
| Ever vs. never | Men | ↑ | OR 1.89 (1.56–2.28) | Sugiyama (2010) [26] |
| RR 1.47 (1.29–1.68) | Ding (2021) | |||
| Current vs. never | Men | ↑ | OR 1.87 (1.49–2.34) | Sugiyama (2010) [26] |
| RR 1.27 (1.09–1.48) | Ding (2021) | |||
| Past vs. never | Men | ↑ | OR 1.76 (1.33–2.31) | Sugiyama (2010) [26] |
| Ever vs. never | Men * | ↑↑ * | OR 3.02 (2.35–3.88) * | Sugiyama (2010) [26] |
| Current vs. never | Men * | ↑↑ * | OR 3.91 (2.78–5.50) * | Sugiyama (2010) [26] |
| Past vs. never | Men * | ↑↑ * | OR 2.46 (1.74–3.47) * | Sugiyama (2010) [26] |
| Ever vs. never | Women | ↑ | OR 1.27 (1.12–1.44) | Sugiyama (2010) [26] |
| Current vs. never | Women | ↑ | OR 1.31 (1.12–1.54) | Sugiyama (2010) [26] |
| Past vs. never | Women | ↑ | OR 1.22 (1.06–1.40) | Sugiyama (2010) [26] |
| Ever vs. never | Women * | ↑ * | OR 1.34 (0.99–1.80) * | Sugiyama (2010) [26] |
| Current vs. never | Women * | ↑ * | OR 1.29 (0.94–1.77) * | Sugiyama (2010) [26] |
| Past vs. never | Women * | ↑ | OR 1.21 (0.83–1.77) | Sugiyama (2010) [26] |
| >20 pack-years vs. never smoker | Men | ↑ | OR 2.31 (1.55–3.41) | Sugiyama (2010) [26] |
| >20 pack-years vs. never smoker | Women | ↑ | OR 1.75 (1.52–2.02) | Sugiyama (2010) [26] |
| Excess weight | ||||
| Obese/overweight vs. normal | All | ↑ | RR 1.31 (1.12–1.53) RR 1.15 (1.03–1.29) RR 1.21 (1.02–1.44) RR 1.05 (0.97–1.13) RR 1.32 (1.11–1.54) RR 1.08 (1.00–1.15) RR 1.23 (1.09–1.39) RR 1.12 (1.04–1.20) | Qin (2015) [6] Feng (2016) [5] Zhou (2018) [7] Feng (2019) [8] |
| Obese vs. normal | Women | ↑ | RR 1.26 (1.12–1.40) | Feng (2016) [5] |
| RR 1.40 (1.24–1.57) | Zhou (2018) [7] | |||
| Obese vs. normal | Men | NS | RR 0.83 (0.65–1.05) | Feng (2016) [5] |
| RR 0.89 (0.01–1.77) | Zhou (2018) [7] | |||
| Obese vs. normal | All ** | ↑ ** | RR 1.47 (1.11–1.96) ** | Feng (2016) [5] |
| Per 5 kg/m2 BMI increase | All | ↑ | RR 1.11 (1.05–1.18) | Ohno (2020) |
| RR 1.09 (1.04–1.15) | Ding (2021) | |||
| Per 5 kg/m2 BMI increase | Women | ↑ | RR 1.15 (1.08–1.21) | Ohno (2020) [30] |
| Per 5 kg/m2 BMI increase | Men | NS | RR 0.89 (0.73–1.09) | Ohno (2020) [30] |
| Physical Activity | ||||
| Highest vs. lowest | Men and women | ↓ | RR 0.79 (0.72–0.87) | Sun (2021) [32] |
| Physically active vs. inactive/occasional active | Men and women | ↓ | RR 0.85 (0.79–0.92) | Sun (2021) [32] |
| Dietary intake | ||||
| Fish: 1 to 3 servings per week vs. never | Men and women | ↓ | RR 0.76 (0.57–1.02) | Di Giuseppe (2014) [10] |
| Periodontitis | ||||
| Periodontal disease (disease vs. no disease) | Men and women | ↑ | OR 1.97 (1.68–2.31) | Railson de Oliveira Ferreira (2019) [11] |
| Behavior Modification | Sex | Direction of Association | HR or RR for RA (95% CI) | Author (Year) of Reference |
|---|---|---|---|---|
| Smoking cessation | ||||
| Quit ≥ 30 years vs. quit < 5 years | Women | ↓ | HR 0.63 (0.44–0.90) | Liu (2019) [45] |
| Quit > 15 years, quit > 1 year, current smoker | Women and men | ↓ | RR 0.70 (0.24–2.02) | Di Giuseppe (2013) [46] |
| Bariatric surgery | ||||
| Bariatric surgery vs. no bariatric surgery | Women and men | NS | HR 0.86 (0.54–1.38) | Maglio (2020) [49] |
| Alternative Healthy Eating Index score * adherence | ||||
| ≥75 points vs. <75 points | Women | ↓ | RR 0.43 (0.27–0.67) | Marchand (2020) [52] |
| ≥75 points vs. <75 points | Women ** | ↓ ** | RR 0.41 (0.22–0.74) | Marchand (2020) [52] |
| ≥75 points vs. <75 points | Women *** | ↓ ** | RR 0.47 (0.25–0.91) | Marchand (2020) [52] |
| At-Risk Group | Challenges | Opportunities |
|---|---|---|
| General population | Low general understanding or motivation related to RA Potential unwillingness to change behaviors Low absolute risk for RA | Education about RA, risk factors, early symptoms, and prevention strategies Targeted behavioral interventions Public health initiatives for other reasons may impact RA risk (legislations against smoking, legislation to promote healthy eating, etc.) |
| Genetic risk (e.g., HLA-DRB1 shared epitope) | Unclear cost-benefit of testing for genetics Interpretation of direct-to-consumer genetic testing Risk of anxiety about genetic results | Education about genetic risks Personalized risk assessments Increased genetic testing and precautions when delivering genetic results |
| Family history (FDR without RA) | Perceptions of RA decrease likelihood of seeking predictive help Lack of information when making decisions about risk Potential unwillingness to make and sustain lifestyle changes Concerns about accuracy of predictive testing Concerns about anxiety of predictive test | Education about risk factors, early symptoms, and prevention strategies Personalized risk assessments Increased genetic testing and precautions when delivering genetic results |
| Biomarker risk (CCP+, RF, anti-CarP, anti-PAD3) | Lack of understanding of RA risk Need more information on RA and risk Anxiety about test results | Improve self-efficacy and health literacy Build on existing willingness to make lifestyle changes Build on expressed interest in gaining information, assurance, confirmation of meaning of clinical test |
| Clinical pre-RA risk (e.g., palindromic rheumatism, arthralgias, undifferentiated IA) | Some do not view themselves as patients or already feel they have RA Difficulty in understanding statistical risk of progression to RA Fear of pain, uncertainty of pain progression, developing functional limitations and prognosis | Education about early symptoms and risks Personalized risk assessments Present information in a way that makes sense to patients Learning risk group made risk groups more likely to adopt healthier habits changes, haptonomy, yoga and mindfulness. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaccardelli, A.; Sparks, J.A. Challenges and Opportunities of Targeted Behavioral Interventions for Groups at Risk for Developing Rheumatoid Arthritis. Healthcare 2021, 9, 641. https://doi.org/10.3390/healthcare9060641
Zaccardelli A, Sparks JA. Challenges and Opportunities of Targeted Behavioral Interventions for Groups at Risk for Developing Rheumatoid Arthritis. Healthcare. 2021; 9(6):641. https://doi.org/10.3390/healthcare9060641
Chicago/Turabian StyleZaccardelli, Alessandra, and Jeffrey A. Sparks. 2021. "Challenges and Opportunities of Targeted Behavioral Interventions for Groups at Risk for Developing Rheumatoid Arthritis" Healthcare 9, no. 6: 641. https://doi.org/10.3390/healthcare9060641
APA StyleZaccardelli, A., & Sparks, J. A. (2021). Challenges and Opportunities of Targeted Behavioral Interventions for Groups at Risk for Developing Rheumatoid Arthritis. Healthcare, 9(6), 641. https://doi.org/10.3390/healthcare9060641