Structure and Validity of Questionnaire for Oral Frail Screening

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Structure of the Oral Frailty Screening Questionnaire
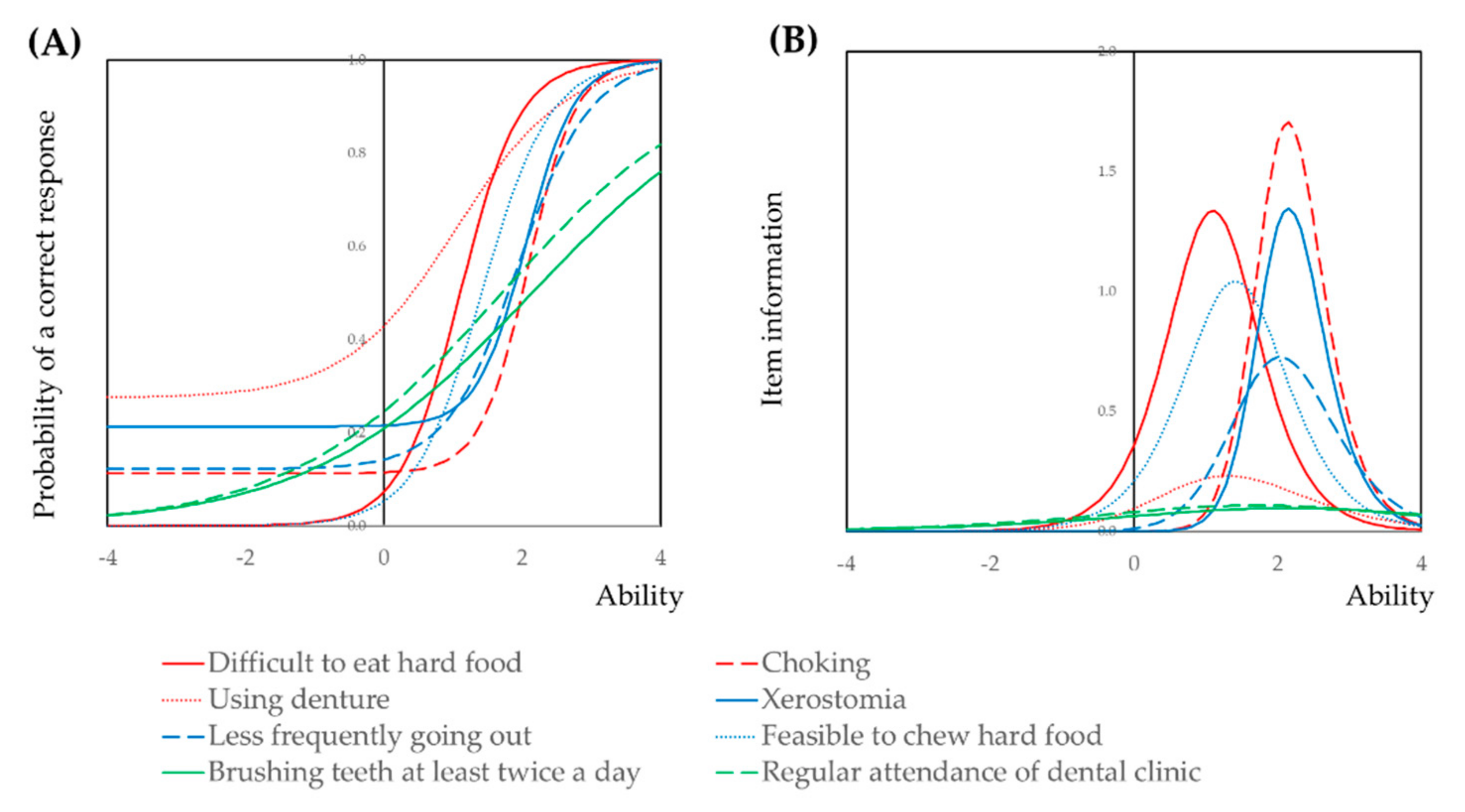
3.2. Item Response Theory Analysis of the Oral Frailty Screening Questionnaire
3.3. Effect of Number of Remaining Teeth on the Oral Frailty Screening Questionnaire
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arai, H.; Ouchi, Y.; Toba, K.; Endo, T.; Shimokado, K.; Tsubota, K.; Matsuo, S.; Mori, H.; Yumura, W.; Yokode, M.; et al. Japan as the front-runner of super-aged societies: Perspectives from medicine and medical care in Japan. Geriatr. Gerontol. Int. 2015, 15, 673–687. [Google Scholar] [CrossRef] [PubMed]
- Genkai, S.; Kikutani, T.; Suzuki, R.; Tamura, F.; Yamashita, Y.; Yoshida, M. Loss of occlusal support affects the decline in activities of daily living in elderly people receiving home care. J. Prosthodont. Res. 2015, 59, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, S.; Yoshioka, M.; Shirayama, Y. Survey on Nursing Home Caregivers’ Basic Knowledge of Oral Health Management: Dental Terminology. Dent. J. 2018, 6, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, Q.L.; Roche, K.B.; Varadhan, R.; Zhou, J.; Fried, L.P. Initial manifestations of frailty criteria and the development of frailty phenotype in the Women’s Health and Aging Study II. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 984–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jentoft, C.A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, E.; Ishibashi, Y.; Tsuda, E.; Ono, A.; Yamamoto, Y.; Inoue, R.; Takahashi, I.; Umeda, T.; Nakaji, S. Evaluation of locomotive disability using loco-check: A cross-sectional study in the Japanese general population. J. Orthop. Sci. 2013, 18, 121–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iijima, K. Upstream preventive strategy for age-related sarcopenia in the elderly: Why do the elderly fall into inadequate nutrition? Ann. Jpn. Prosthodont. Soc. 2015, 7, 92–101. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tsuji, T.; Akishita, M.; Iijima, K. Oral Frailty as a Risk Factor for Physical Frailty and Mortality in Community-Dwelling Elderly. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1661–1667. [Google Scholar] [CrossRef] [PubMed]
- Kera, T.; Kawai, H.; Yoshida, H.; Hirano, H.; Kojima, M.; Fujiwara, Y.; Ihara, K.; Obuchi, S. Classification of frailty using the Kihon checklist: A cluster analysis of older adults in urban areas. Geriatr. Gerontol. Int. 2017, 17, 69–77. [Google Scholar] [CrossRef]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef]
- Nomura, Y.; Ishii, Y.; Suzuki, S.; Morita, K.; Suzuki, A.; Suzuki, S.; Tanabe, J.; Ishiwata, Y.; Yamakawa, K.; Chiba, Y.; et al. Nutritional Status and Oral Frailty: A Community Based Study. Nutrients 2020, 12, 2886. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Kakuta, E.; Okada, A.; Otsuka, R.; Shimada, M.; Tomizawa, Y.; Taguchi, C.; Arikawa, K.; Daikoku, H.; Sato, T.; et al. Impact of the Serum Level of Albumin and Self-Assessed Chewing Ability on Mortality, QOL, and ADLs for Community-Dwelling Older Adults at the Age of 85: A 15 Year Follow up Study. Nutrients 2020, 12, E3315. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Kakuta, E.; Okada, A.; Yamamoto, Y.; Tomonari, H.; Hosoya, N.; Hanada, N.; Yoshida, N.; Takei, N. Prioritization of the Skills to Be Mastered for the Daily Jobs of Japanese Dental Hygienists. Int. J. Dent. 2020, 2020, 4297646. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Matsuyama, T.; Fukai, K.; Okada, A.; Ida, M.; Yamauchi, N.; Hanamura, H.; Yabuki, Y.; Watanabe, K.; Sugawara, M.; et al. PRECEDE-PROCEED model based questionnaire and saliva tests for oral health checkup in adult. J. Oral Sci. 2019, 61, 544–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nomura, Y.; Okada, A.; Miyoshi, J.; Mukaida, M.; Akasaka, E.; Saigo, K.; Daikoku, H.; Maekawa, H.; Sato, T.; Hanada, N. Willingness to Work and the Working Environment of Japanese Dental Hygienists. Int. J. Dent. 2018, 2018, 2727193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imanaka, M.; Nomura, Y.; Tamaki, Y.; Akimoto, N.; Ishikawa, C.; Takase, H.; Ishii, H.; Yamachika, S.; Noda, K.; Ide, M.; et al. Validity and reliability of patient satisfaction questionnaires in a dental school in Japan. Eur. J. Dent. Educ. 2007, 11, 29–37. [Google Scholar] [CrossRef]
- Nomura, Y.; Otsuka, R.; Wint, W.Y.; Okada, A.; Hasegawa, R.; Hanada, N. Tooth-Level Analysis of Dental Caries in Primary Dentition in Myanmar Children. Int. J. Environ. Res. Public Health 2020, 17, 7613. [Google Scholar] [CrossRef]
- Nomura, Y.; Kakuta, E.; Okada, A.; Otsuka, R.; Shimada, M.; Tomizawa, Y.; Taguchi, C.; Arikawa, K.; Daikoku, H.; Sato, T.; et al. Effects of self-assessed chewing ability, tooth loss and serum albumin on mortality in 80-year-old individuals: A 20-year follow-up study. BMC Oral Health 2020, 20, 122. [Google Scholar] [CrossRef]
- Nomura, Y.; Okada, A.; Kakuta, E.; Otsuka, R.; Saito, H.; Maekawa, H.; Daikoku, H.; Hanada, N.; Sato, T. Workforce and Contents of Home Dental Care in Japanese Insurance System. Int. J. Dent. 2020, 2020, 7316796. [Google Scholar] [CrossRef]
- Morita, K.; Tsuka, H.; Kimura, H.; Mori, T.; Yoshikawa, M.; Yoshida, M.; Kimura, M.; Tsuga, K. Oral function and vertical jump height among healthy older people in Japan. Community Dent. Health 2019, 36, 275–279. [Google Scholar] [CrossRef]
- Ikebe, K.; Matsuda, K.; Morii, K.; Nokubi, T.; Ettinger, R.L. The relationship between oral function and body mass index among independently living older Japanese people. Int. J. Prosthodont. 2006, 19, 539–546. [Google Scholar] [PubMed]
- Ikebe, K.; Matsuda, K.; Kagawa, R.; Enoki, K.; Yoshida, M.; Maeda, Y.; Nokubi, T. Association of masticatory performance with age, gender, number of teeth, occlusal force and salivary flow in Japanese older adults: Is ageing a risk factor for masticatory dysfunction? Arch. Oral Biol. 2011, 56, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Sagawa, K.; Furuya, H.; Ohara, Y.; Yoshida, M.; Hirano, H.; Iijima, K.; Kikutani, T. Tongue function is important for masticatory performance in the healthy elderly: A cross-sectional survey of community-dwelling elderly. J. Prosthodont. Res. 2019, 63, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, P.; Olai, L.; Ståhlnacke, K.; Persenius, M.; Hägg, M.; Andersson, M.; Koistinen, S.; Carlsson, E. Study protocol for the SOFIA project: Swallowing function, Oral health, and Food Intake in old Age: A descriptive study with a cluster randomized trial. BMC Geriatr. 2017, 17, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furuta, M.; Takeuchi, K.; Adachi, M.; Kinoshita, T.; Eshima, N.; Akifusa, S.; Kikutani, T.; Yamashita, Y. Tooth loss, swallowing dysfunction and mortality in Japanese older adults receiving home care services. Geriatr. Gerontol. Int. 2018, 18, 873–880. [Google Scholar] [CrossRef]
- Hägglund, P.; Koistinen, S.; Olai, L.; Ståhlnacke, K.; Wester, P.; Jäghagen, E.L. Older people with swallowing dysfunction and poor oral health are at greater risk of early death. Community Dent. Oral Epidemiol. 2019, 47, 494–501. [Google Scholar] [CrossRef] [Green Version]
- Arakawa, I.; Ayash, A.S.; Genton, L.; Tsuga, K.; Leles, C.R.; Schimmel, M. Reliability and comparability of methods for assessing oral function: Chewing, tongue pressure and lip force. J. Oral Rehabil. 2020, 47, 862–871. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Ability | Score | ||||
|---|---|---|---|---|---|
| Number of Remaining Teeth | N | Mean ± SD | Median (25th–75th) | Mean ± SD | Median (25th–75th) |
| 0 | 34 | 0.84 ± 0.14 | 0.81 (0.22–1.34) | 3.36 ± 0.37 | 3 (2–5) |
| 1–4 | 19 | 0.97 ± 0.17 | 0.94 (0.22–1.48) | 3.47 ± 0.34 | 3 (3–4) |
| 5–9 | 37 | 0.72 ± 0.12 | 0.72 (−0.14–1.41) | 3.05 ± 0.27 | 3 (2–5) |
| 10–14 | 54 | 0.59 ± 0.09 | 0.63 (−0.14–1.15) | 2.57 ± 0.18 | 2 (1–4) |
| 15–19 | 62 | 0.43 ± 0.09 | 0.20 (−0.15–0.88) | 2.36 ± 0.18 | 2 (1–3) |
| 21–24 | 156 | 0.12 ± 0.05 | −0.14 (−0.26–0.54) | 1.75 ± 0.11 | 1 (1–2) |
| 25≤ | 48 | −0.13 ± 0.03 | −0.15 (−0.51–0.01) | 1.32 ± 0.06 | 1 (0–2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nomura, Y.; Ishii, Y.; Chiba, Y.; Suzuki, S.; Suzuki, A.; Suzuki, S.; Morita, K.; Tanabe, J.; Yamakawa, K.; Ishiwata, Y.; et al. Structure and Validity of Questionnaire for Oral Frail Screening. Healthcare 2021, 9, 45. https://doi.org/10.3390/healthcare9010045
Nomura Y, Ishii Y, Chiba Y, Suzuki S, Suzuki A, Suzuki S, Morita K, Tanabe J, Yamakawa K, Ishiwata Y, et al. Structure and Validity of Questionnaire for Oral Frail Screening. Healthcare. 2021; 9(1):45. https://doi.org/10.3390/healthcare9010045
Chicago/Turabian StyleNomura, Yoshiaki, Yoshimasa Ishii, Yota Chiba, Shunsuke Suzuki, Akira Suzuki, Senichi Suzuki, Kenji Morita, Joji Tanabe, Koji Yamakawa, Yasuo Ishiwata, and et al. 2021. "Structure and Validity of Questionnaire for Oral Frail Screening" Healthcare 9, no. 1: 45. https://doi.org/10.3390/healthcare9010045
APA StyleNomura, Y., Ishii, Y., Chiba, Y., Suzuki, S., Suzuki, A., Suzuki, S., Morita, K., Tanabe, J., Yamakawa, K., Ishiwata, Y., Ishikawa, M., Sogabe, K., Kakuta, E., Okada, A., Otsuka, R., & Hanada, N. (2021). Structure and Validity of Questionnaire for Oral Frail Screening. Healthcare, 9(1), 45. https://doi.org/10.3390/healthcare9010045