
AI for Doctors—A Course to Educate Medical Professionals in Artificial Intelligence for Medical Imaging

 , , , , ,
, , , , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Course Curriculum
2.2. Pre- and Post-Course Questionnaires
2.3. Statistical Analysis
2.4. Ethics Statement
3. Results
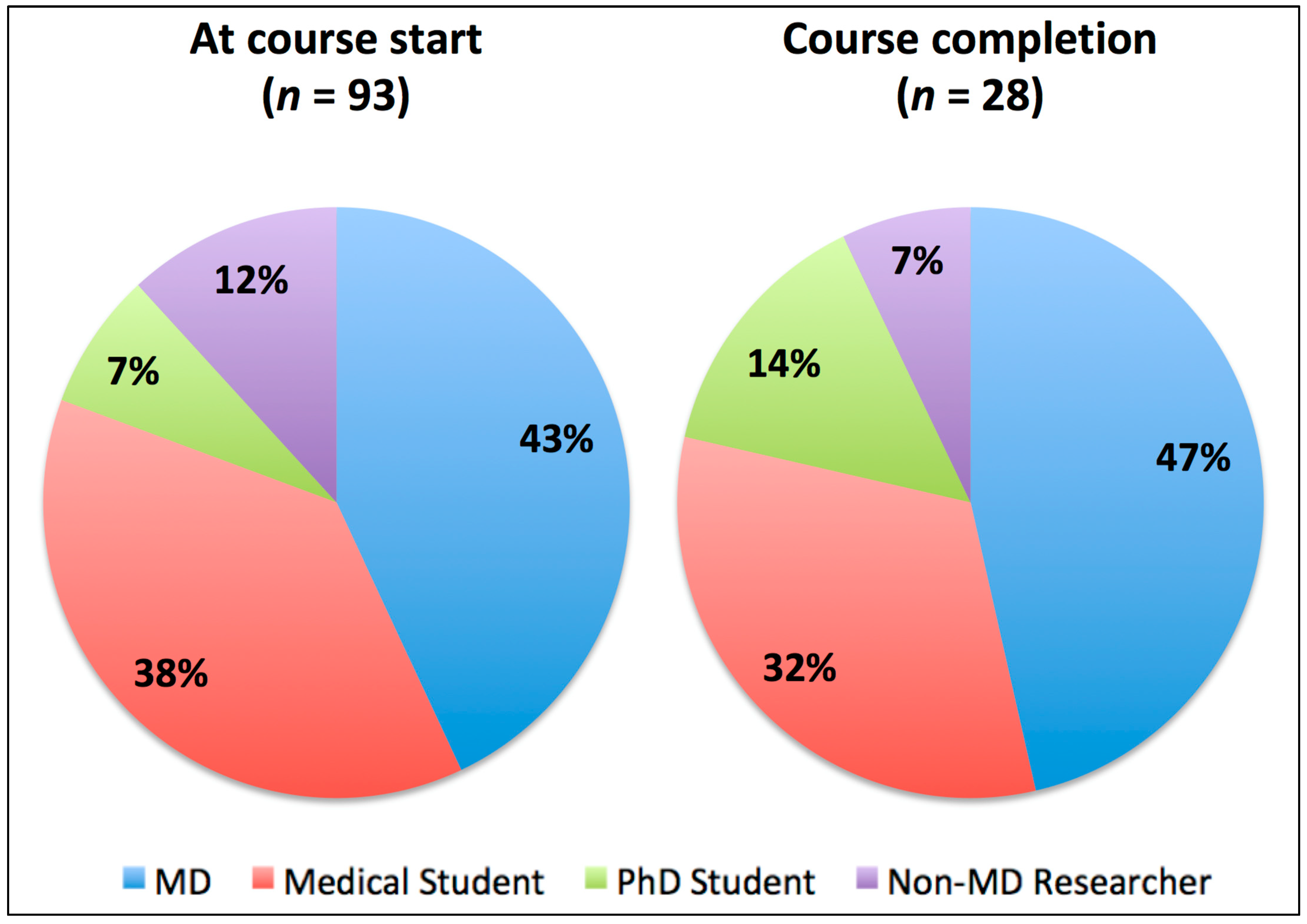
3.1. Course Participants
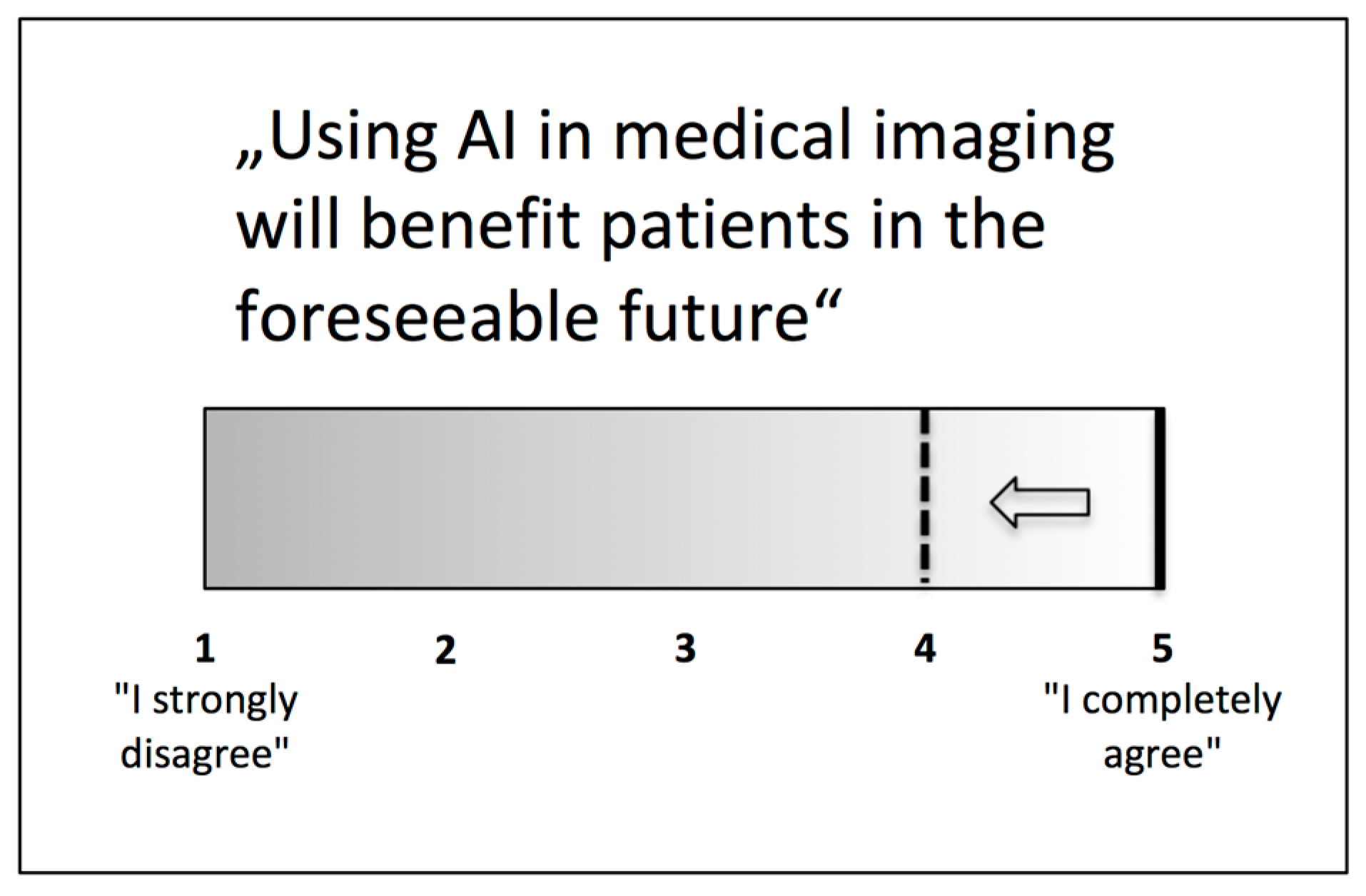
3.2. Opinions towards AI in Medical Imaging
3.3. Self-Perceived Skills Relating to AI and Medical Imaging
3.4. Overall Appraisal of the Course
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hinton, G. Deep Learning—A Technology With the Potential to Transform Health Care. JAMA 2018, 320, 1101–1102. [Google Scholar] [CrossRef] [PubMed]
- Jha, S.; Topol, E.J. Adapting to Artificial Intelligence: Radiologists and Pathologists as Information Specialists. JAMA 2016, 316, 2353–2354. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Faes, L.; Kale, A.U.; Wagner, S.K.; Fu, D.J.; Bruynseels, A.; Mahendiran, T.; Moraes, G.; Shamdas, M.; Kern, C.; et al. A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: A systematic review and meta-analysis. Lancet Digit. Health 2019, 1, e271–e297. [Google Scholar] [CrossRef]
- Nagendran, M.; Chen, Y.; Lovejoy, C.A.; Gordon, A.C.; Komorowski, M.; Harvey, H.; Topol, E.J.; Ioannidis, J.P.A.; Collins, G.S.; Maruthappu, M. Artificial intelligence versus clinicians: Systematic review of design, reporting standards, and claims of deep learning studies. BMJ 2020, 368, m689. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.P.; Hom, G.L.; Abramoff, M.D.; Campbell, J.P.; Chiang, M.F. Current Challenges and Barriers to Real-World Artificial Intelligence Adoption for the Healthcare System, Provider, and the Patient. Transl. Vis. Sci. Technol. 2020, 9, 45. [Google Scholar] [CrossRef]
- Pesapane, F.; Volonté, C.; Codari, M.; Sardanelli, F. Artificial intelligence as a medical device in radiology: Ethical and regulatory issues in Europe and the United States. Insights Imaging 2018, 9, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Huisman, M.; Ranschaert, E.; Parker, W.; Mastrodicasa, D.; Koci, M.; Pinto dos Santos, D.; Coppola, F.; Morozov, S.; Zins, M.; Bohyn, C.; et al. An international survey on AI in radiology in 1041 radiologists and radiology residents part 1: Fear of replacement, knowledge, and attitude. Eur. Radiol. 2021, 31, 7058–7066. [Google Scholar] [CrossRef] [PubMed]
- Jungmann, F.; Jorg, T.; Hahn, F.; Pinto dos Santos, D.; Jungmann, S.M.; Düber, C.; Mildenberger, P.; Kloeckner, R. Attitudes Toward Artificial Intelligence Among Radiologists, IT Specialists, and Industry. Acad. Radiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lindqwister, A.L.; Hassanpour, S.; Lewis, P.J.; Sin, J.M. AI-RADS: An Artificial Intelligence Curriculum for Residents. Acad. Radiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Waymel, Q.; Badr, S.; Demondion, X.; Cotten, A.; Jacques, T. Impact of the rise of artificial intelligence in radiology: What do radiologists think? Diagn. Interv. Imaging 2019, 100, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Pinto Dos Santos, D.; Giese, D.; Brodehl, S.; Choon, S.H.; Staab, W.; Kleinert, R.; Maintz, D.; Baeßler, B. Medical students’ attitude towards artificial intelligence: A multicentre survey. Eur. Radiol. 2019, 29, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Neri, E.; de Souza, N.; Brady, A.; Bayarri, A.A.; Becker, C.D.; Coppola, F.; Visser, J. What the radiologist should know about artificial intelligence—An ESR white paper. Insights Imaging 2019, 10, 44. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Participant Group | MD | Medical Student | PhD Student | Non-MD Researcher |
|---|---|---|---|---|
| At course start | 40 | 35 | 7 | 11 |
| Successful course completion | 13 | 9 | 4 | 2 |
| Question (Answers Ranging from 1 = Strongly Disagree to 5 = Completely Agree) | Median | Minimum | Maximum | 25th Percentile | 75th Percentile |
|---|---|---|---|---|---|
| Using AI in medical imaging will benefit patients in the foreseeable future. | 5 | 3 | 5 | 4 | 5 |
| It is important to understand how an AI algorithm works in order to use its results in clinical decision making. | 5 | 2 | 5 | 4 | 5 |
| I would use an AI algorithm in medical decision making if it has been thoroughly evaluated by others with good performance, although I don’t understand how it works. | 4 | 1 | 5 | 3 | 4 |
| I will not use AI in medical imaging algorithms unless I can fully explain them to my patients. | 3 | 1 | 5 | 2 | 4 |
| Education about AI must be integrated in medical training in university. | 4 | 1 | 5 | 4 | 5 |
| Education about AI must be integrated in medical training in residency. | 4 | 1 | 5 | 4 | 5 |
| Using AI in medical imaging will reduce the workload of physicians. | 4 | 2 | 5 | 3 | 4 |
| Clinical adoption of AI in medical imaging will replace physicians e.g., radiologists in the next 10 years. | 2 | 1 | 5 | 1 | 3 |
| Image-analysis tasks in general can be performed by an AI algorithm today at medical-expert level. | 3 | 1 | 5 | 2 | 4 |
| Some particular tasks can be performed by an AI algorithm today at medical-expert level. | 4 | 2 | 5 | 4 | 5 |
| Clinical adoption of AI algorithms in medical imaging is mostly hindered by regulatory barriers and traditions, not by the performance of the developed algorithms. | 3 | 1 | 5 | 3 | 4 |
| Doctors should have basic programming skills. | 3 | 1 | 5 | 2 | 4 |
| Timepoint | Before Course | After Course | |||||
|---|---|---|---|---|---|---|---|
| Areas of self-Assessment (Ranging from 1 = No Skills to 5 = Expert Skills) | Median | 25th Percentile | 75th Percentile | Median | 25th Percentile | 75th Percentile | p |
| Understanding Python code when reading it. | 1 | 1 | 2 | 2.5 | 2 | 3 | 0.001 |
| Creating Python code for statistical analysis. | 1 | 1 | 2 | 2 | 2 | 3 | 0.002 |
| Understanding concepts in linear algebra pertaining to machine learning. | 2 | 1.5 | 2 | 3 | 2 | 3.25 | 0.006 |
| Assessing a machine-learning paper validating AI algorithms for medical imaging. | 2 | 1 | 2 | 2.5 | 2 | 3.25 | 0.005 |
| Applying a ML algorithm in a clinical setting. | 1 | 1 | 2 | 2 | 2 | 2.25 | 0.013 |
| Incorporating decisions made by a ML algorithm into clinical decision making. | 1 | 1 | 3 | 2.5 | 2 | 3.25 | 0.042 |
| Question (Answers Ranging from 1 = Strongly Disagree to 5 = Completely Agree) | Median | Minimum | Maximum | 25th Percentile | 75th Percentile |
|---|---|---|---|---|---|
| The course was well organized | 5 | 2 | 5 | 4 | 5 |
| Overall, the study material was well prepared | 5 | 3 | 5 | 4 | 5 |
| The content of the course was important for my work as a clinician | 3,5 | 2 | 5 | 3 | 4 |
| The content of the course was important for my work as a scientist | 4 | 2 | 5 | 4 | 5 |
| The course could easily be taken alongside clinical work | 3 | 1 | 5 | 2 | 3 |
| I expected the workload to participate in the course to be | 3 | 2 | 3 | 2 | 3 |
| I missed in-person lectures and meetings with teachers and other students. | 4 | 1 | 5 | 2 | 4 |
| I feel more competent at dealing with AI in medical imaging than before the course | 4 | 1 | 5 | 4 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hedderich, D.M.; Keicher, M.; Wiestler, B.; Gruber, M.J.; Burwinkel, H.; Hinterwimmer, F.; Czempiel, T.; Spiro, J.E.; Pinto dos Santos, D.; Heim, D.; et al. AI for Doctors—A Course to Educate Medical Professionals in Artificial Intelligence for Medical Imaging. Healthcare 2021, 9, 1278. https://doi.org/10.3390/healthcare9101278
Hedderich DM, Keicher M, Wiestler B, Gruber MJ, Burwinkel H, Hinterwimmer F, Czempiel T, Spiro JE, Pinto dos Santos D, Heim D, et al. AI for Doctors—A Course to Educate Medical Professionals in Artificial Intelligence for Medical Imaging. Healthcare. 2021; 9(10):1278. https://doi.org/10.3390/healthcare9101278
Chicago/Turabian StyleHedderich, Dennis M., Matthias Keicher, Benedikt Wiestler, Martin J. Gruber, Hendrik Burwinkel, Florian Hinterwimmer, Tobias Czempiel, Judith E. Spiro, Daniel Pinto dos Santos, Dominik Heim, and et al. 2021. "AI for Doctors—A Course to Educate Medical Professionals in Artificial Intelligence for Medical Imaging" Healthcare 9, no. 10: 1278. https://doi.org/10.3390/healthcare9101278
APA StyleHedderich, D. M., Keicher, M., Wiestler, B., Gruber, M. J., Burwinkel, H., Hinterwimmer, F., Czempiel, T., Spiro, J. E., Pinto dos Santos, D., Heim, D., Zimmer, C., Rückert, D., Kirschke, J. S., & Navab, N. (2021). AI for Doctors—A Course to Educate Medical Professionals in Artificial Intelligence for Medical Imaging. Healthcare, 9(10), 1278. https://doi.org/10.3390/healthcare9101278