
Isolated Resistance Training Programs to Improve Peripheral Muscle Function in Outpatients with Chronic Obstructive Pulmonary Diseases: A Systematic Review

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
3.1. Study Selection
3.2. Quality Rating
3.3. Study Characteristics
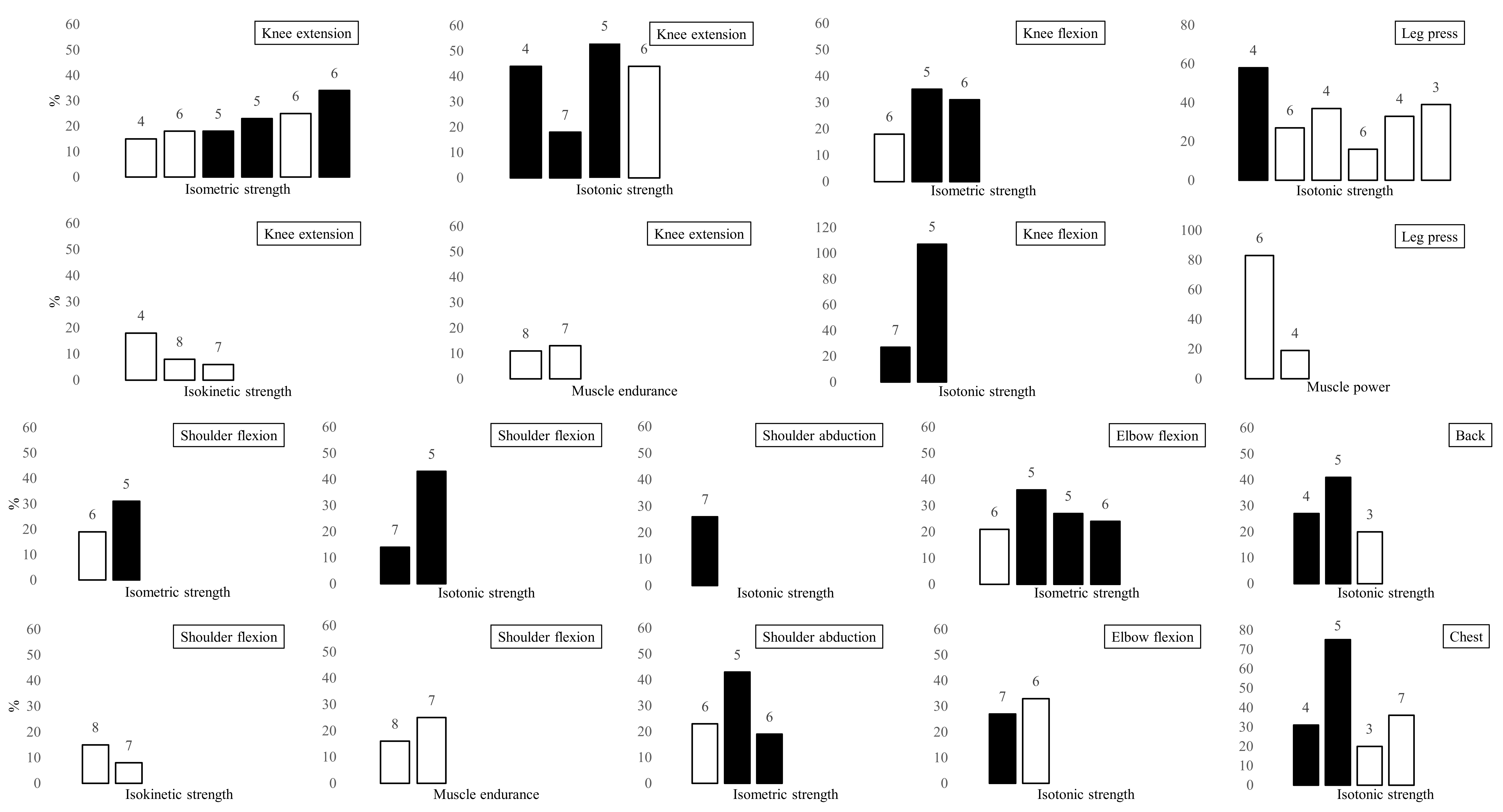
3.4. Outcome Measures
4. Discussion
4.1. RT Program Design
4.2. Impact of RT on Trainable Muscle Characteristics
4.3. Training Modes
4.4. Methods to Assess Muscle Function in Clinical Practice
4.5. Structural and Systemic Effects of RT
4.6. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Maltais, F.; Decramer, M.; Casaburi, R.; Barreiro, E.; Burelle, Y.; Debigaré, R.; Dekhuijzen, P.N.R.; Franssen, F.; Gayan-Ramirez, G.; Gea, J.; et al. An Official American Thoracic Society/European Respiratory Society statement: Update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2014, 189, e15–e62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopkinson, N.S.; Tennant, R.C.; Dayer, M.J.; Swallow, E.B.; Hansel, T.T.; Moxham, J.; Polkey, M.I. A prospective study of decline in fat free mass and skeletal muscle strength in chronic obstructive pulmonary disease. Respir. Res. 2007, 8, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swallow, E.B.; Reyes, D.; Hopkinson, N.S.; Man, W.D.; Porcher, R.; Cetti, E.J.; Moore, A.J.; Moxham, J.; Polkey, M.I. Quadriceps strength predicts mortality in patients with moderate to severe chronic obstructive pulmonary disease. Thorax 2007, 62, 115–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Decramer, M.; Gosselink, R.; Troosters, T.; Verschueren, M.; Evers, G. Muscle weakness is related to utilization of health care resources in copd patients. Eur. Respir. J. 1997, 10, 417–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef]
- American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef]
- De Brandt, J.; Spruit, M.A.; Derave, W.; Hansen, D.; Vanfleteren, L.E.G.W.; Burtin, C. Changes in structural and metabolic muscle characteristics following exercise-based interventions in patients with copd: A systematic review. Expert Rev. Respir. Med. 2016, 10, 521–545. [Google Scholar] [CrossRef]
- Bui, K.-L.; Maia, N.; Saey, D.; Dechman, G.; Maltais, F.; Camp, P.G.; Mathur, S. Reliability of quadriceps muscle power and explosive force, and relationship to physical function in people with chronic obstructive pulmonary disease: An observational prospective multicenter study. Physiother. Theory Pract. 2021, 37, 945–953. [Google Scholar] [CrossRef]
- Houchen, L.; Steiner, M.C.; Singh, S.J. How sustainable is strength training in chronic obstructive pulmonary disease? physiotherapy 2009, 95, 1–7. [Google Scholar] [CrossRef]
- Marklund, S.; Bui, K.-L.; Nyberg, A. Measuring and monitoring skeletal muscle function in copd: Current perspectives. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 1825–1838. [Google Scholar] [CrossRef] [Green Version]
- Jaitovich, A.; Barreiro, E. Skeletal muscle dysfunction in chronic obstructive pulmonary disease. what we know and can do for our patients. Am. J. Respir. Crit. Care Med. 2018, 198, 175–186. [Google Scholar] [CrossRef]
- Campos, G.E.; Luecke, T.J.; Wendeln, H.K.; Toma, K.; Hagerman, F.C.; Murray, T.F.; Ragg, K.E.; Ratamess, N.A.; Kraemer, W.J.; Staron, R.S. Muscular adaptations in response to three different resistance-training regimens: Specificity of repetition maximum training zones. Eur. J. Appl. Physiol. 2002, 88, 50–60. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Ratamess, N.A. Fundamentals of resistance training: Progression and exercise prescription. Med. Sci. Sports Exerc. 2004, 36, 674–688. [Google Scholar] [CrossRef]
- Spruit, M.A.; Pitta, F.; Garvey, C.; ZuWallack, R.L.; Roberts, C.M.; Collins, E.G.; Goldstein, R.; McNamara, R.; Surpas, P.; Atsuyoshi, K.; et al. Differences in content and organisational aspects of pulmonary rehabilitation programmes. Eur. Respir. J. 2014, 43, 1326–1337. [Google Scholar] [CrossRef] [Green Version]
- Mathur, S.; Dechman, G.; Bui, K.-L.; Camp, P.G.; Saey, D. Evaluation of limb muscle strength and function in people with chronic obstructive pulmonary disease. Cardiopulm. Phys. Ther. J. 2019, 30, 24–34. [Google Scholar] [CrossRef]
- Nyberg, A.; Saey, D.; Maltais, F. Why and how limb muscle mass and function should be measured in patients with chronic obstructive pulmonary disease. Ann. Am. Thorac. Soc. 2015, 12, 1269–1277. [Google Scholar] [CrossRef]
- Li, N.; Li, P.; Lu, Y.; Wang, Z.; Li, J.; Liu, X.; Wu, W. Effects of resistance training on exercise capacity in elderly patients with chronic obstructive pulmonary disease: A meta-analysis and systematic review. Aging Clin. Exp. Res. 2020, 32, 1911–1922. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Tong, S.; Wu, Y.; Abdelrahim, M.E.A.; Cao, M. Effects of resistance training on exercise ability in chronic obstructive pulmonary disease subjects: A systematic review and meta-analysis. Int. J. Clin. Pract. 2021, 75, e14373. [Google Scholar] [CrossRef] [PubMed]
- Strasser, B.; Siebert, U.; Schobersberger, W. Effects of resistance training on respiratory function in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. Sleep Breath. 2013, 17, 217–226. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, S.D.; Taylor, N.F.; Paratz, J.D. Progressive resistance exercise improves muscle strength and may improve elements of performance of daily activities for people with copd: A systematic review. Chest 2009, 136, 1269–1283. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.-h.; Chen, J.w.; Chen, X.; Lin, L.; Yan, H.y.; Zhou, Y.-q.; Chen, R. Impact of resistance training in subjects with copd: A systematic review and meta-analysis. Respir. Care 2015, 60, 1130–1145. [Google Scholar] [CrossRef] [PubMed]
- De Brandt, J.; Spruit, M.A.; Hansen, D.; Franssen, F.M.; Derave, W.; Sillen, M.J.; Burtin, C. Changes in lower limb muscle function and muscle mass following exercise-based interventions in patients with chronic obstructive pulmonary disease: A review of the English-language literature. Chron. Respir. Dis. 2018, 15, 182–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global strategy for the diagnosis, management and prevention of chronic obstructive lung disease 2017 report: Gold executive summary. Respirology 2017, 22, 575–601. [Google Scholar] [CrossRef] [PubMed]
- De Morton, N.A. The PEDro Scale Is a Valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Foley, N.C.; Bhogal, S.K.; Teasell, R.W.; Bureau, Y.; Speechley, M.R. Estimates of quality and reliability with the Physiotherapy Evidence-Based Database scale to assess the methodology of randomized controlled trials of pharmacological and nonpharmacological interventions. Phys. Ther. 2006, 86, 817–824. [Google Scholar] [CrossRef]
- Clark, C.J.; Cochrane, L.M.; Mackay, E.; Paton, B. Skeletal muscle strength and endurance in patients with mild COPD and the effects of weight training. Eur. Respir. J. 2000, 15, 92–97. [Google Scholar] [CrossRef] [Green Version]
- Dourado, V.Z.; Tanni, S.E.; Antunes, L.C.O.; Paiva, S.a.R.; Campana, A.O.; Renno, A.C.M.; Godoy, I. Effect of three exercise programs on patients with chronic obstructive pulmonary disease. Braz. J. Med. Biol. Res. 2009, 42, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Kongsgaard, M.; Backer, V.; Jørgensen, K.; Kjær, M.; Beyer, N. Heavy resistance training increases muscle size, strength and physical function in elderly male COPD-patients--a pilot study. Respir. Med. 2004, 98, 1000–1007. [Google Scholar] [CrossRef] [Green Version]
- Ortega, F.; Toral, J.; Cejudo, P.; Villagomez, R.; Sánchez, H.; Castillo, J.; Montemayor, T. Comparison of effects of strength and endurance training in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2002, 166, 669–674. [Google Scholar] [CrossRef]
- De Silva, B.S.A.; Gobbo, L.A.; Freire, A.P.C.F.; Trevisan, I.B.; Silva, I.G.; Ramos, E.M.C. Effects of a resistance training with elastic tubing in strength, quality of life and dypsnea in patients with chronic obstructive pulmonary disease. J. Phys. Educ. 2016, 27, e-2722. [Google Scholar] [CrossRef] [Green Version]
- De Silva, B.S.A.; Lira, F.S.; Rossi, F.E.; Ramos, D.; Uzeloto, J.S.; Freire, A.P.C.F.; de Lima, F.F.; Gobbo, L.A.; Ramos, E.M.C. Inflammatory and metabolic responses to different resistance training on chronic obstructive pulmonary disease: A randomized control trial. Front. Physiol. 2018, 9, 262. [Google Scholar] [CrossRef]
- Vonbank, K.; Strasser, B.; Mondrzyk, J.; Marzluf, B.A.; Richter, B.; Losch, S.; Nell, H.; Petkov, V.; Haber, P. Strength training increases maximum working capacity in patients with copd—randomized clinical trial comparing three training modalities. Respir. Med. 2012, 106, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Hoff, J.; Tjønna, A.; Steinshamn, S.; Høydal, M.; Richardson, R.; Helgerud, J. Maximal strength training of the legs in COPD: A therapy for mechanical inefficiency. Med. Sci. Sports Exerc. 2007, 39, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Nyberg, A.; Lindström, B.; Rickenlund, A.; Wadell, K. Low-load/high-repetition elastic band resistance training in patients with COPD: A randomized, controlled, multicenter trial. Clin. Respir. J. 2015, 9, 278–288. [Google Scholar] [CrossRef]
- Ramos, E.M.C.; de Toledo-Arruda, A.C.; Fosco, L.C.; Bonfim, R.; Bertolini, G.N.; Guarnier, F.A.; Cecchini, R.; Pastre, C.M.; Langer, D.; Gosselink, R.; et al. The effects of elastic tubing-based resistance training compared with conventional resistance training in patients with moderate chronic obstructive pulmonary disease: A randomized clinical trial. Clin. Rehabil. 2014, 28, 1096–1106. [Google Scholar] [CrossRef] [PubMed]
- Simpson, K.; Killian, K.; McCartney, N.; Stubbing, D.G.; Jones, N.L. Randomised controlled trial of weightlifting exercise in patients with chronic airflow limitation. Thorax 1992, 47, 70–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spruit, M.A.; Gosselink, R.; Troosters, T.; Paepe, K.D.; Decramer, M. Resistance versus endurance training in patients with COPD and peripheral muscle weakness. Eur. Respir. J. 2002, 19, 1072–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zambom-Ferraresi, F.; Cebollero, P.; Gorostiaga, E.; Hernández, M.; Hueto, J.; Cascante, J.; Rezusta, L.; Val, L.; Anton, M. Effects of combined resistance and endurance training versus resistance training alone on strength, exercise capacity, and quality of life in patients with COPD. J. Cardiopulm. Rehabil. Prev. 2015, 35, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Freire, A.P.C.F.; Camillo, C.A.M.; de Alencar Silva, B.S.; Uzeloto, J.S.; de Lima, F.F.; Gobbo, L.A.; Ramos, D.; Ramos, E.M.C. Resistance training using different elastic components offers similar gains on muscle strength to weight machine equipment in individuals with COPD: A randomized controlled trial. Physiother. Theory Pract. 2020 24, 1–14. [CrossRef]
- Nyberg, A.; Martin, M.; Saey, D.; Milad, N.; Patoine, D.; Morissette, M.C.; Auger, D.; Stål, P.; Maltais, F. Effects of low-load/high-repetition resistance training on exercise capacity, health status, and limb muscle adaptation in patients with severe COPD: A randomized controlled trial. Chest 2021, 159, 1821–1832. [Google Scholar] [CrossRef]
- Nakamura, Y.; Tanaka, K.; Yabushita, N.; Sakai, T.; Shigematsu, R. Effects of exercise frequency on functional fitness in older adult women. Arch. Gerontol. Geriatr. 2007, 44, 163–173. [Google Scholar] [CrossRef]
- Burtin, C.; Saey, D.; Saglam, M.; Langer, D.; Gosselink, R.; Janssens, W.; Decramer, M.; Maltais, F.; Troosters, T. Effectiveness of exercise training in patients with COPD: The role of muscle fatigue. Eur. Respir. J. 2012, 40, 338–344. [Google Scholar] [CrossRef]
- Robles, P.G.; Mathur, S.; Janaudis-Fereira, T.; Dolmage, T.E.; Goldstein, R.S.; Brooks, D. Measurement of peripheral muscle strength in individuals with chronic obstructive pulmonary disease: A systematic review. J. Cardiopulm. Rehabil. Prev. 2011, 31, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.A.; Kaplovitch, E.; Beauchamp, M.K.; Dolmage, T.E.; Goldstein, R.S.; Gillies, C.L.; Brooks, D.; Mathur, S. Is quadriceps endurance reduced in COPD? A systematic review. Chest 2015, 147, 673–684. [Google Scholar] [CrossRef] [Green Version]
- Iepsen, U.W.; Jørgensen, K.J.; Ringbaek, T.; Hansen, H.; Skrubbeltrang, C.; Lange, P. A systematic review of resistance training versus endurance training in COPD. J. Cardiopulm. Rehabil. Prev. 2015, 35, 163–172. [Google Scholar] [CrossRef]
- Probst, V.S.; Troosters, T.; Pitta, F.; Decramer, M.; Gosselink, R. Cardiopulmonary stress during exercise training in patients with COPD. Eur. Respir. J. 2006, 27, 1110–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro-Cruz, R.; Alcazar, J.; Rodriguez-Lopez, C.; Losa-Reyna, J.; Alfaro-Acha, A.; Ara, I.; García-García, F.J.; Alegre, L.M. The effect of the stretch-shortening cycle in the force–velocity relationship and its association with physical function in older adults with COPD. Front. Physiol. 2019, 10. [Google Scholar] [CrossRef] [Green Version]
- Hernández, M.; Zambom-Ferraresi, F.; Cebollero, P.; Hueto, J.; Cascante, J.A.; Antón, M.M. The relationships between muscle power and physical activity in older men with chronic obstructive pulmonary disease. J. Aging Phys. Act. 2017, 25, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Considerations and practical options for measuring muscle strength: A narrative review. BioMed Res. Int. 2019, 2019, 8194537. [Google Scholar] [CrossRef] [PubMed]
- Marquis, K.; Debigaré, R.; Lacasse, Y.; LeBlanc, P.; Jobin, J.; Carrier, G.; Maltais, F. Midthigh muscle cross-sectional area is a better predictor of mortality than body mass index in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2002, 166, 809–813. [Google Scholar] [CrossRef]
- Rutten, E.P.A.; Spruit, M.A.; Wouters, E.F.M. Critical view on diagnosing muscle wasting by single-frequency bio-electrical impedance in COPD. Respir. Med. 2010, 104, 91–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steiner, M.C.; Barton, R.L.; Singh, S.J.; Morgan, M.D.L. Bedside methods versus dual energy x--ray absorptiometry for body composition measurement in COPD. Eur. Respir. J. 2002, 19, 626–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Study | Randomization | Concealed Allocation | Baseline Comparability | Blind Subjects | Blind Therapists | Blind Assessor | FU | ITT | Between-Group Comparison | Point Estimates and Variability | PEDro Score | Attrition Rate (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Clark [28] | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5/10 | 0 |
| Dourado [29] | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4/10 | 28 |
| Freire [41] | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 7/10 | 27 |
| Hoff [35] | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6/10 | 0 |
| Kongsgaard [30] | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4/10 | 28 |
| Nyberg [36] | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8/10 | 9 |
| Nyberg [42] | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 7/10 | 30 |
| Ortega [31] | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5/10 | 13 |
| Ramos [37] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 6/10 | 24 |
| Silva [32] | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 5/10 | 32 |
| Silva [33] | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 5/10 | 27 |
| Simpson [38] | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 6/10 | 18 |
| Spruit [39] | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 6/10 | 38 |
| Vonbank [34] | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 3/10 | 16 |
| Zambom-Ferraresi [40] | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 7/10 | 10 |
| Study | Study Groups | Study Intervention | Study Duration | Training Protocol |
|---|---|---|---|---|
| Clark [28] | Conventional resistance training (CO): 26; Control (CG): 17 | CO: 8 exercises (chest press, body squat, squat calf, lat machine, arm curls, leg press, knee extension, knee flexion) with weights. CG: No intervention. | 12 weeks | Frequency: 2 d/w Reps: 3 × 10 Phase velocity: NA Rest: NA Load: 70% of 1RM Progression: Every 6 weeks (repeating 1RM test) |
| Dourado [29] | Conventional resistance training (CO): 11; Low-intensity training (LIT): 13; Combined training (CT): 11 | CO: 7 exercises (leg press, leg extension, lat pull down, chest press, seated rowing, triceps pulley, and biceps curl) with weight machines. LIT: 30 min of walking and 30 min of low-intensity CO with free weights, on exercise mats and on parallel bars. CT: 30 min of CO group and 30 min as LIT group. | 12 weeks | Frequency: 3 d/w Reps: 3 × 12 (CO); 2 × 8 (CT) Phase velocity: NA Rest: 2 min Load: 50–80% of 1RM Progression: Every 3 weeks (repeating 1RM test) |
| Freire [41] | Conventional resistance training (CO): 16; Elastic tubing resistance (ER): 18; Elastic bands resistance (EB): 14 | CO: 5 exercises (shoulder abduction, elbow flexion, shoulder flexion; knee extension and knee flexion) with weight machines. ER and EB: The same exercise program of CO was carried out with elastic tubing or bands. | 12 weeks | Frequency: 3 d/w Reps: 2 × 15 (weeks 1–2); 3 × 15 (weeks 3–6); 3 × 10 (weeks 7–9); 3 × 15 (weeks 10–12) Phase velocity: 2 s Rest: 2 min Load: established with nRM Progression: Each session with the nRM test |
| Hoff [35] | Conventional resistance training (CO): 6; Control (CG): 6 | CO: 1 exercise (leg press). CG: No intervention. | 8 weeks | Frequency: 3 d/w Reps: 4 × 5 Phase velocity: Explosive concentric, slow eccentric Rest: 2 min Load: 85–90% of 1RM Progression: 2.5 kg increment when 5 reps were exceeded |
| Kongsgaard [30] | Conventional resistance training (CO): 6; Control (CG): 7 | CO: 3 exercises (leg press, knee extension, knee flexion) with weight machines. CG: Breathing exercise. | 12 weeks | Frequency: 2 d/w Reps: 4 × 8 Phase velocity: Explosive concentric Rest: 2–3 min Load: 80% of 1RM Progression: Every week |
| Nyberg [36] | Elastic bands resistance (EB): 22; Control (CG): 22 | EB: 8 exercises (latissimus row, chest press, leg extension, straight arm shoulder flex, leg curl, elbow flexion, leg heel raise, leg step-up). CG: 4 days of education. | 8 weeks | Frequency: 3 d/w Reps: 2 × 25 Phase velocity: 1 s Rest: 1 min Load: Established nRM Progression: Every 2 sessions (if Borg scale < 4) |
| Nyberg [42] | Elastic band single-limb resistance (SEB): 16; Elastic band two-limb resistance (TEB):17 | SEB: 7 exercises (knee extension, leg curl, latissimus row, chest press, elbow flexion, shoulder flexion, calf) with a single limb at a time. TEB: As SEB but using both limbs at a time. | 8 weeks | Frequency: 3 d/w Reps: 3 × 25–30 Phase velocity: 1 s Rest: 1 min Load: Established nRM Progression: Increased every two sessions by 10% if patients exceeded 30 reps |
| Ortega [31] | Conventional resistance training (CO): 17; Endurance training (ET): 16; Combined training (CT): 14 | CO: 5 exercises (lat pull, butterfly, neck press, leg flexion, leg extension) with gymnastic apparatus. ET: 40 min of cycling at 70% of peak work capacity. CT: 20 min of cycling plus CO. | 12 weeks | Frequency: 3 d/w Reps: 4 × 6–8 (CO); 2 × 6–8 (CT) Phase velocity: NA Rest: NA Load: 70–85% of 1RM Progression: Every 2 weeks (repeating 1RM test) |
| Ramos [37] | Conventional resistance training (CO): 17; Elastic tubing resistance (ER): 17 | CO: 5 exercises (knee extension, knee flexion, shoulder abduction, shoulder flexion, elbow flexion) with weight machines. ER: Same exercises as CO group, performed with elastic tubing. | 8 weeks | Frequency: 3 d/w Reps: 3 × 10 (CO); 2–7 × maximum in 20 s (ER) Phase velocity: NA Rest: 2 min Load: 60% (week 1) to 80% (week 8) of 1RM Progression: Increased by 4% every four sessions (CO); increased by one set every two sessions (ER) |
| Silva [32] | Conventional resistance training (CO): 10; Elastic tubing resistance (ER): 9 | CO: 5 exercises (knee flexion, knee extension, shoulder flexion, shoulder abduction, elbow flexion) with weight machines. ER: Same exercises as CO group, performed with elastic tubing. | 12 weeks | Frequency: 3 d/w Reps: 2 × 15 (weeks 1–3); 3 × 15 (weeks 4–6); 3 × 10 (weeks 7–9); 4 × 6 (weeks 10–12) Phase velocity: 1.8 s Rest: 2 min Load: 15RM Progression: Increased when patients exceeded the nRM |
| Silva [33] | Conventional resistance training (CO): 11; Elastic resistance (ER): 24 | CO: 5 exercises (knee flexion, knee extension, shoulder flexion, shoulder abduction, elbow flexion) with weight machines. ER: Same exercises as CO group, performed with elastics. | 12 weeks | Frequency: 3 d/w Reps: 2 × 15 (weeks 1–3); 3 × 15 (weeks 4–6); 3 × 10 (weeks 7–9); 3 × 15 (weeks 10–12) Phase velocity: NA Rest: NA Load: Established nRM Progression: Increased when patients exceeded the nRM |
| Simpson [38] | Conventional resistance training (CO): 14; Control (CG): 14 | CO: 3 exercises with weights using a single limb at a time (arm curl, leg extension, leg press). CG: No intervention. | 8 weeks | Frequency: 3 d/w Reps: 3 × 10 Phase velocity: Slow concentric Rest: NA Load: 50% (week 1) to 85% (week 8) of 1RM Progression: Every 6 sessions (repeating 1RM test) |
| Spruit [39] | Conventional resistance training (CO): 14; Endurance training (ET): 16 | CO: 6 exercises (quadriceps, pectorals, triceps brachia, deltoids, biceps brachia, hamstrings) with weight machines. ET: Cycling or walking for 25 min at 75% of peak work or 60% of 6-min walk speed) plus arm cranking (4–9 min). | 12 weeks | Frequency: 3 d/w Reps: 3 × 8 Phase velocity: NA Rest: NA Load: 70% of 1RM Progression: Increased by 5% of 1RM every week |
| Vonbank [34] | Conventional resistance training (CO): 12; Endurance training (ET): 12; Combined training (CT): 12 | CO: 8 exercises (chest press, chest cross, shoulder press, pull downs, biceps curl, triceps extensions, sit-ups, leg press). ET: Cycling for 20 min (increased by 5 min every 4 weeks) at 60% of estimated VO2peak. CT: CO plus ET | 12 weeks | Frequency: 2 d/w Reps: 2 × 8–15 (weeks 1–4); 3 × 8-15 (weeks 5–9); 4 × 8–15 (weeks 10–12) Phase velocity: NA Rest: NA Load: Established nRM Progression: Increased when patients exceeded the nRM |
| Zambom- Ferraresi [40] | Conventional resistance training (CO): 14; Combined training (CT): 14; Control (CG): 8 | CO: 6 exercises (leg press, knee extension, knee flexion, chest press, seated row, shoulder press) with weight machines. CT: one d/w of CO and 1 d/w of cycling for 20–35 min at 65–90% of peak heaCO rate (increased each session). CG: No intervention. | 12 weeks | Frequency: 2 d/w Reps: 3–4 × 6–12 Phase velocity: NA Rest: NA Load: 50–70% of 1RM Progression: Every 6 weeks (repeating 1RM test) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pancera, S.; Lopomo, N.F.; Bianchi, L.N.C.; Pedersini, P.; Villafañe, J.H. Isolated Resistance Training Programs to Improve Peripheral Muscle Function in Outpatients with Chronic Obstructive Pulmonary Diseases: A Systematic Review. Healthcare 2021, 9, 1397. https://doi.org/10.3390/healthcare9101397
Pancera S, Lopomo NF, Bianchi LNC, Pedersini P, Villafañe JH. Isolated Resistance Training Programs to Improve Peripheral Muscle Function in Outpatients with Chronic Obstructive Pulmonary Diseases: A Systematic Review. Healthcare. 2021; 9(10):1397. https://doi.org/10.3390/healthcare9101397
Chicago/Turabian StylePancera, Simone, Nicola F. Lopomo, Luca N. C. Bianchi, Paolo Pedersini, and Jorge H. Villafañe. 2021. "Isolated Resistance Training Programs to Improve Peripheral Muscle Function in Outpatients with Chronic Obstructive Pulmonary Diseases: A Systematic Review" Healthcare 9, no. 10: 1397. https://doi.org/10.3390/healthcare9101397
APA StylePancera, S., Lopomo, N. F., Bianchi, L. N. C., Pedersini, P., & Villafañe, J. H. (2021). Isolated Resistance Training Programs to Improve Peripheral Muscle Function in Outpatients with Chronic Obstructive Pulmonary Diseases: A Systematic Review. Healthcare, 9(10), 1397. https://doi.org/10.3390/healthcare9101397