
Prevalence of Colorectal Polyps Based on Cardiorespiratory Fitness, Muscle Strength, Health Behavior, and Abdominal Obesity in Asymptomatic Elderly



Abstract
:1. Introduction
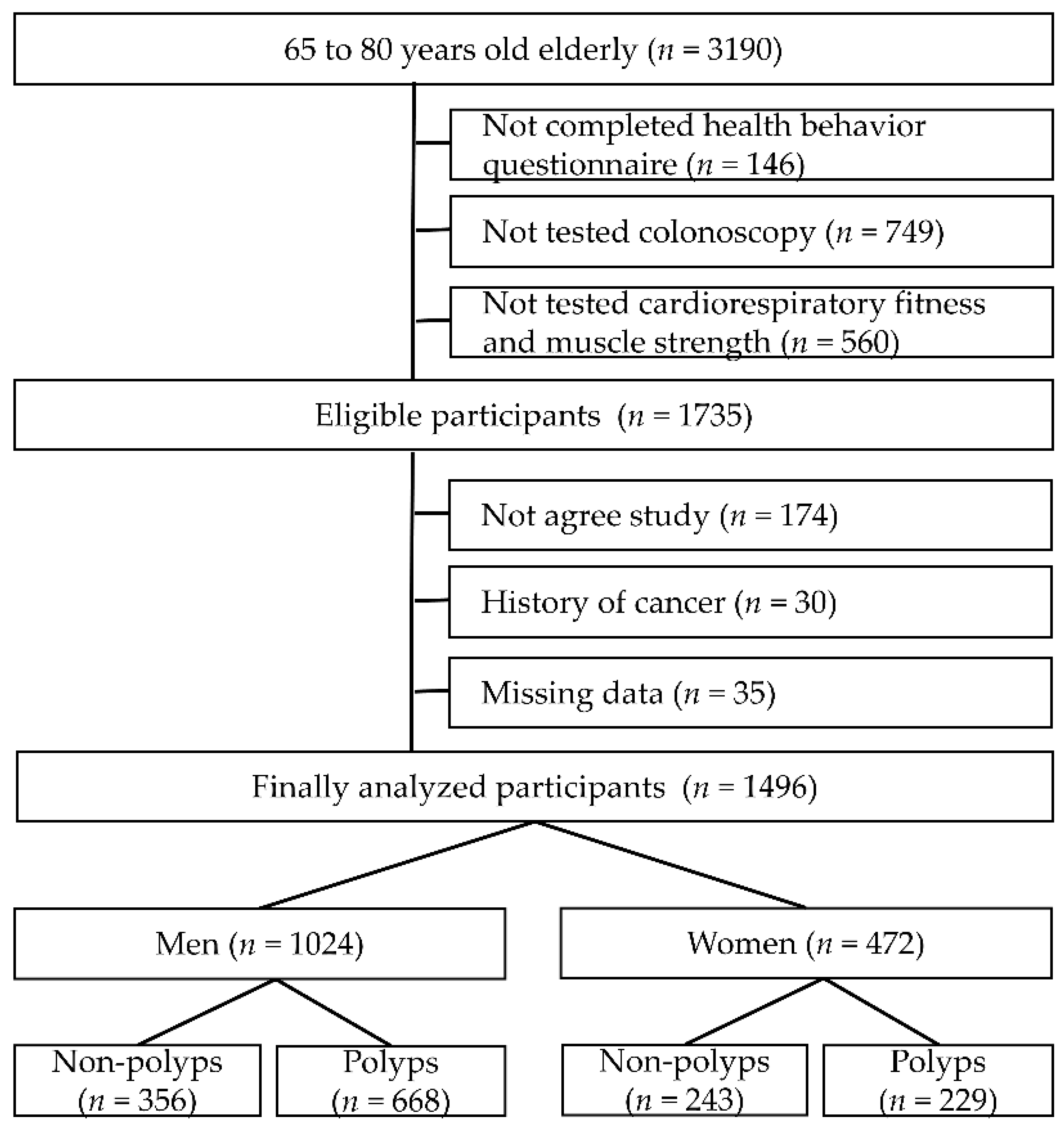
2. Methods
2.1. Health Behavior Questionnaire
2.2. Obesity
2.3. Fitness Test
2.3.1. Cardiorespiratory Fitness
2.3.2. Leg Muscle Strength
2.4. Colonoscopy
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.-W.; Won, Y.-J.; Oh, C.-M.; Kong, H.-J.; Lee, D.H.; Lee, K.H. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2014. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2017, 49, 292–305. [Google Scholar] [CrossRef]
- Rezasoltani, S.; Aghdaei, H.A.; Dabiri, H.; Sepahi, A.A.; Modarressi, M.H.; Mojarad, E.N. The association between fecal microbiota and different types of colorectal polyp as precursors of colorectal cancer. Microb. Pathog. 2018, 124, 244–249. [Google Scholar] [CrossRef]
- Song, M.; Emilsson, L.; Bozorg, S.R.; Nguyen, L.H.; Joshi, A.D.; Staller, K.; Nayor, J.; Chan, A.T.; Ludvigsson, J.F. Risk of colorectal cancer incidence and mortality after polypectomy: A Swedish record-linkage study. Lancet Gastroenterol. Hepatol. 2020, 5, 537–547. [Google Scholar] [CrossRef]
- He, X.; Wu, K.; Ogino, S.; Giovannucci, E.L.; Chan, A.T.; Song, M. Association between risk factors for colorectal cancer and risk of serrated polyps and conventional adenomas. Gastroenterology 2018, 155, 355–373. [Google Scholar] [CrossRef]
- Jayasekara, H.; Reece, J.C.; Buchanan, D.D.; Ahnen, D.J.; Parry, S.; Jenkins, M.A.; Win, A.K. Risk factors for metachronous colorectal cancer or polyp: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2017, 32, 301–326. [Google Scholar] [CrossRef]
- Øines, M.; Helsingen, L.M.; Bretthauer, M.; Emilsson, L. Epidemiology and risk factors of colorectal polyps. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 419–424. [Google Scholar] [CrossRef]
- Bailie, L.; Loughrey, M.B.; Coleman, H.G. Lifestyle risk factors for serrated colorectal polyps: A systematic review and meta-analysis. Gastroenterology 2017, 152, 92–104. [Google Scholar] [CrossRef] [Green Version]
- Nakai, K.; Watari, J.; Tozawa, K.; Tamura, A.; Hara, K.; Yamasaki, T.; Kondo, T.; Kono, T.; Tomita, T.; Ohda, Y. Sex differences in associations among metabolic syndrome, obesity, related biomarkers, and colorectal adenomatous polyp risk in a Japanese population. J. Clin. Biochem. Nutr. 2018, 63, 154–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Kim, J.H.; Lee, H.J.; Park, S.J.; Hong, S.P.; Cheon, J.H.; Kim, W.H.; Park, J.S.; Jeon, J.Y.; Kim, T.I. The effects of physical activity and body fat mass on colorectal polyp recurrence in patients with previous colorectal cancer. Cancer Prev. Res. 2017, 10, 478–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenner, D.R.; Shaw, E.; Yannitsos, D.H.; Warkentin, M.T.; Brockton, N.T.; McGregor, S.E.; Town, S.; Hilsden, R.J. The association between recreational physical activity, sedentary time, and colorectal polyps in a population screened for colorectal cancer. Cancer Epidemiol. 2018, 53, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Song, H.K.; Kim, Y.H. The relationship between exercise, cardiopulmonary fitness, and prevalence of colon polyps according to age group. J. Men’s Health 2019, 15, e35–e45. [Google Scholar]
- Oh, J.Y.; Yang, Y.J.; Kim, B.S.; Kang, J.H. Validity and reliability of Korean version of International Physical Activity Questionnaire (IPAQ) short form. J. Korean Acad. Fam. Med. 2007, 28, 532–541. [Google Scholar]
- Reinert, D.F.; Allen, J.P. The alcohol use disorders identification test: An update of research findings. Alcohol. Clin. Exp. Res. 2007, 31, 185–199. [Google Scholar] [CrossRef]
- WHO. Tobacco Questions for Surveys: A Subset of Key Questions from the Global Adult Tobacco Survey (GATS): Global Tobacco Surveillance System; World Health Organization: Atlanta, GA, USA, 2011. [Google Scholar]
- WHO. World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of the WHO Consultation of Obesity; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Inoue, S.; Zimmet, P.; Caterson, I.; Chunming, C.; Ikeda, Y.; Khalid, A.; Kim, Y. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; World Health Organization: Sydney, Australia, 2000. [Google Scholar]
- ACSM. ACSM’s Guildelines for Exercise Testing and Prescription 10th; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2017. [Google Scholar]
- CSMi. Humac Norm Users Guide; Computer Sports Medicine, Inc.: Stoughton, MA, USA, 2019. [Google Scholar]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, T.; Ishikawa, H.; Sakai, T.; Ayabe, M.; Wakabayashi, K.; Mutoh, M.; Matsuura, N. Effect of physical fitness on colorectal tumor development in patients with familial adenomatous polyposis. Medicine 2019, 98, e17076–e17082. [Google Scholar] [CrossRef]
- Robsahm, T.E.; Falk, R.S.; Heir, T.; Sandvik, L.; Vos, L.; Erikssen, J.; Tretli, S. Cardiorespiratory fitness and risk of site-specific cancers: A long-term prospective cohort study. Cancer Med. 2017, 6, 865–873. [Google Scholar] [CrossRef] [PubMed]
- Takemura, Y.; Kikuchi, S.; Oba, K.; Inaba, Y.; Nakagawa, K. A high level of physical fitness during thirties is a negative risk factor for colonic polyps during fifties. Keio J. Med. 2000, 49, 111–116. [Google Scholar] [CrossRef]
- Hillreiner, A.; Baumeister, S.E.; Sedlmeier, A.M.; Finger, J.D.; Schlitt, H.J.; Leitzmann, M.F. Association between cardiorespiratory fitness and colorectal cancer in the UK Biobank. Eur. J. Epidemiol. 2020, 35, 961–973. [Google Scholar] [CrossRef] [PubMed]
- Vella, C.A.; Van Guilder, G.P.; Dalleck, L.C. Low cardiorespiratory fitness is associated with markers of insulin resistance in young, normal weight, Hispanic women. Metab. Syndr. Relat. Disord. 2016, 14, 272–278. [Google Scholar] [CrossRef] [Green Version]
- Santos, R.d.; Viana, V.A.R.; Boscolo, R.A.; Marques, V.; Santana, M.G.d.; Lira, F.S.d.; Tufik, S.; de Mello, M. Moderate exercise training modulates cytokine profile and sleep in elderly people. Cytokine 2012, 60, 731–735. [Google Scholar] [CrossRef] [Green Version]
- Traustadóttir, T.; Davies, S.S.; Su, Y.; Choi, L.; Brown-Borg, H.M.; Roberts, L.J.; Harman, S.M. Oxidative stress in older adults: Effects of physical fitness. Age 2012, 34, 969–982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.S.; Kim, J.W.; Kim, B.G.; Lee, K.L.; Lee, J.K.; Kim, J.S.; Koh, S.-J. Sarcopenia is associated with an increased risk of advanced colorectal neoplasia. Int. J. Colorectal Dis. 2017, 32, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.H.; Kim, Y.J.; Oh, Y.H.; Kong, M.H.; Kim, H.J. Association between colorectal adenoma and hand grip strength in the elderly. J. Bone Metab. 2019, 26, 161–167. [Google Scholar] [CrossRef]
- Wolin, K.Y.; Yan, Y.; Colditz, G.A. Physical activity and risk of colon adenoma: A meta-analysis. Br. J. Cancer 2011, 104, 882–885. [Google Scholar] [CrossRef]
- Oruç, Z.; Kaplan, M.A. Effect of exercise on colorectal cancer prevention and treatment. World J. Gastrointest. Oncol. 2019, 11, 348–366. [Google Scholar] [CrossRef]
- IJspeert, J.; Bossuyt, P.; Kuipers, E.; Stegeman, I.; de Wijkerslooth, T.; Stoop, E.; van Leerdam, M.; Dekker, E. Smoking status informs about the risk of advanced serrated polyps in a screening population. Endosc. Int. Open 2016, 4, E73–E78. [Google Scholar] [CrossRef] [Green Version]
- Devin, J.L.; Bolam, K.A.; Jenkins, D.G.; Skinner, T.L. The influence of exercise on the insulin-like growth factor axis in oncology: Physiological basis, current, and future perspectives. Cancer Epidemiol. Prev. Biomark. 2016, 25, 239–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fairey, A.S.; Courneya, K.S.; Field, C.J.; Bell, G.J.; Jones, L.W.; Mackey, J.R. Randomized controlled trial of exercise and blood immune function in postmenopausal breast cancer survivors. J. Appl. Physiol. 2005, 98, 1534–1540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehl, K.A.; Davis, J.M.; Clements, J.M.; Berger, F.G.; Pena, M.M.; Carson, J.A. Decreased intestinal polyp multiplicity is related to exercise mode and gender in Apc Min/+ mice. J. Appl. Physiol. 2005, 98, 2219–2225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, B.K. Exercise-induced myokines and their role in chronic diseases. Brain Behav. Immun. 2011, 25, 811–816. [Google Scholar] [CrossRef]
- Kawanishi, N.; Yano, H.; Mizokami, T.; Takahashi, M.; Oyanagi, E.; Suzuki, K. Exercise training attenuates hepatic inflammation, fibrosis and macrophage infiltration during diet induced-obesity in mice. Brain Behav. Immun. 2012, 26, 931–941. [Google Scholar] [CrossRef]
- Rogers, C.J.; Zaharoff, D.A.; Hance, K.W.; Perkins, S.N.; Hursting, S.D.; Schlom, J.; Greiner, J.W. Exercise enhances vaccine-induced antigen-specific T cell responses. Vaccine 2008, 26, 5407–5415. [Google Scholar] [CrossRef] [Green Version]
- Schmid, D.; Leitzmann, M.F. Cardiorespiratory fitness as predictor of cancer mortality: A systematic review and meta-analysis. Ann. Oncol. 2015, 26, 272–278. [Google Scholar] [CrossRef]
- Penn, E.; Garrow, D.; Romagnuolo, J. Influence of race and sex on prevalence and recurrence of colon polyps. Arch. Intern. Med. 2010, 170, 1127–1132. [Google Scholar] [CrossRef] [Green Version]
- Hong, W.; Dong, L.; Stock, S.; Basharat, Z.; Zippi, M.; Zhou, M. Prevalence and characteristics of colonic adenoma in mainland China. Cancer Manag. Res. 2018, 10, 2743–2755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, J.B.; Lagas, J.S.; Broestl, L.; Sponagel, J.; Rockwell, N.; Rhee, G.; Rosen, S.F.; Chen, S.; Klein, R.S.; Imoukhuede, P. Sex differences in cancer mechanisms. Biol. Sex Differ. 2020, 11, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.H.; Zhang, S.M.; Rexrode, K.M.; Manson, J.E.; Chan, A.T.; Wu, K.; Tworoger, S.S.; Hankinson, S.E.; Fuchs, C.; Gaziano, J.M. Association between sex hormones and colorectal cancer risk in men and women. Clin. Gastroenterol. Hepatol. 2013, 11, 419–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.; Kim, Y.H. Colorectal Polyp Prevalence According to Alcohol Consumption, Smoking and Obesity. Int. J. Environ. Res. Public Health 2020, 17, 2387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Um, K.; Park, C.-S.; Yoo, C.; Ahn, Y.-S.; Kim, M.; Jeong, K.S. Risk factors including night shift work of colorectal polyp. Ann. Occup. Environ. Med. 2020, 32, e26–e36. [Google Scholar] [CrossRef] [PubMed]
- Fliss-Isakov, N.; Zelber-Sagi, S.; Webb, M.; Halpern, Z.; Kariv, R. Smoking habits are strongly associated with colorectal polyps in a population-based case-control study. J. Clin. Gastroenterol. 2018, 52, 805–811. [Google Scholar] [CrossRef]
- Shrubsole, M.J.; Wu, H.; Ness, R.M.; Shyr, Y.; Smalley, W.E.; Zheng, W. Alcohol drinking, cigarette smoking, and risk of colorectal adenomatous and hyperplastic polyps. Am. J. Epidemiol. 2008, 167, 1050–1058. [Google Scholar] [CrossRef]
- Pan, J.; Cen, L.; Xu, L.; Miao, M.; Li, Y.; Yu, C.; Shen, Z. Prevalence and risk factors for colorectal polyps in a Chinese population: A retrospective study. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Song, Y.K.; Park, Y.S.; Seon, C.S.; Lim, H.J.; Son, B.K.; Ahn, S.B.; Jo, Y.K.; Kim, S.H.; Jo, Y.J.; Lee, J.H. Alcohol drinking increased the risk of advanced colorectal adenomas. Intest. Res. 2015, 13, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Rossi, M.; Jahanzaib Anwar, M.; Usman, A.; Keshavarzian, A.; Bishehsari, F. Colorectal cancer and alcohol consumption—Populations to molecules. Cancers 2018, 10, 38. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Kim, Y.; Lee, S. An association between colonic adenoma and abdominal obesity: A cross-sectional study. BMC Gastroenterol. 2009, 9, 4. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.H.; Jung, Y.S.; Park, J.H.; Park, D.I.; Sohn, C.I. Abdominal Obesity is More Predictive of Advanced Colorectal Neoplasia Risk Than Overall Obesity in Men. J. Clin. Gastroenterol. 2019, 53, e284–e290. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F.; Charles, K.A.; Mantovani, A. Smoldering and polarized inflammation in the initiation and promotion of malignant disease. Cancer Cell 2005, 7, 211–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frayn, K.N. Visceral fat and insulin resistance—Causative or correlative? Br. J. Nutr. 2000, 83, S71–S77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parian, A.M.; Lazarev, M.G. Serrated colorectal lesions in patients with inflammatory bowel disease. Gastroenterol. Hepatol. 2018, 14, 19–25. [Google Scholar]
- Doubeni, C.A.; Laiyemo, A.O.; Major, J.M.; Schootman, M.; Lian, M.; Park, Y.; Graubard, B.I.; Hollenbeck, A.R.; Sinha, R. Socioeconomic status and the risk of colorectal cancer: An analysis of more than a half million adults in the National Institutes of Health-AARP Diet and Health Study. Cancer 2012, 118, 3636–3644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorey, K.M.; Luginaah, I.N.; Bartfay, E.; Fung, K.Y.; Holowaty, E.J.; Wright, F.C.; Hamm, C.; Kanjeekal, S.M. Effects of socioeconomic status on colon cancer treatment accessibility and survival in Toronto, Ontario, and San Francisco, California, 1996–2006. Am. J. Public Health 2011, 101, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Soltani, G.; Poursheikhani, A.; Yassi, M.; Hayatbakhsh, A.; Kerachian, M.; Kerachian, M.A. Obesity, diabetes and the risk of colorectal adenoma and cancer. BMC Endocr. Disord. 2019, 19, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, G.S.; Kou, T.D.; Barnholtz Sloan, J.S.; Koroukian, S.M.; Schluchter, M.D. Use of colonoscopy for polyp surveillance in Medicare beneficiaries. Cancer 2013, 119, 1800–1807. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Men (n = 1024) | Women (n = 472) | p-Value |
|---|---|---|---|
| Age, years | 68.0 (0.295) | 68.3 (0.414) | 0.522 |
| Height, cm | 168.0 (0.568) | 153.0 (0.540) | <0.001 * |
| Weight, kg | 70.4 (0.839) | 58.7 (0.839) | <0.001 * |
| BMI, kg/m2 | 25.3 (0.849) | 24.5 (0.319) | 0.009 * |
| Waist circumference, cm | 86.0 (0.705) | 79.0 (0.985) | <0.001 * |
| Cardiorespiratory fitness, mL/kg −1/min−1 | 29.7 (0.492) | 25.3 (0.518) | <0.001 * |
| Muscle strength, N·m/kg·m−1 | 2.90 (0.08) | 1.92 (0.07) | <0.001 * |
| Smoking status, n (%) | |||
| Never | 182 (18.3%) | 498 (88.3%) | <0.001 * |
| Former | 462 (46.4%) | 34 (6.0%) | |
| Current | 352 (35.3%) | 32 (5.7%) | |
| Alcohol frequency, n (%) | |||
| 0–1 day week | 426 (42.8%) | 498 (88.3%) | <0.001 * |
| 2–3 days/week | 274 (27.5%) | 52 (9.2%) | |
| 4–7 days/week | 296 (29.7%) | 14 (2.5%) | |
| Physical activity, n (%) | |||
| Every day | 143 (14.4%) | 80 (14.2%) | <0.001 * |
| 3–5 days/week | 316 (31.7%) | 170 (30.1%) | |
| 1–2 days/week | 337 (33.8%) | 150 (26.6%) | |
| None | 200 (20.1%) | 164 (29.1%) | |
| Education, n (%) | |||
| Graduate | 180 (18.1%) | 33 (5.9%) | <0.001 * |
| College or university | 379 (38.1%) | 150 (26.6%) | |
| High school | 437 (43.9%) | 381 (67.6%) | |
| Income (USD), n (%) | |||
| >9000 USD | 187 (18.8%) | 95 (16.8%) | <0.001 * |
| 3000 to 9000 USD | 536 (53.8%) | 207 (36.7%) | |
| <3000 USD | 273 (27.4%) | 262 (46.5%) | |
| Colorectal polyp, n (%) | 668 (65.2%) | 229 (48.5%) | <0.001 * |
| Variables | Men | p-Value | Women | p-Value | ||
|---|---|---|---|---|---|---|
| Non–Polyp | Polyp | Non–Polyp | Polyp | |||
| Waist circumference | ||||||
| Normal | 257 (74.1%) | 425 (65.5%) | 0.006 * | 207 (71.4%) | 173 (63.1%) | <0.001 * |
| Obesity | 90 (25.9%) | 224 (34.5%) | 83 (28.6%) | 101 (36.9%) | ||
| Cardiorespiratory fitness | ||||||
| High | 153 (44.1%) | 188 (29.0%) | <0.001 * | 121 (41.7%) | 73 (26.6%) | <0.001 * |
| Middle | 118 (34.0%) | 212 (32.7%) | 106 (36.6%) | 80 (29.2%) | ||
| Low | 76 (21.9%) | 249 (38.3%) | 63 (21.7%) | 121 (44.2%) | ||
| Muscle strength | ||||||
| High | 135 (38.9%) | 195 (30.0%) | 0.004 * | 113 (39.0%) | 79 (28.8%) | 0.038 * |
| Middle | 116 (33.4%) | 216 (33.3%) | 90 (31.0%) | 96 (35.1%) | ||
| Low | 96 (27.7%) | 238 (36.7%) | 87 (30.0%) | 99 (36.1%) | ||
| Smoking status | ||||||
| None | 75 (21.6%) | 107 (16.5%) | <0.001 * | 268 (92.5%) | 230 (84.0%) | 0.107 |
| Former | 179 (51.6%) | 283 (43.6%) | 12 (4.1%) | 22 (8.0%) | ||
| Current | 93 (26.8%) | 259 (39.9%) | 10 (3.4%) | 22 (8.0%) | ||
| Alcohol frequency | ||||||
| 0–1 day/week | 156 (45.0%) | 270 (41.6%) | 0.046 * | 256 (88.3%) | 242 (88.4%) | 0.154 |
| 2–3 days/week | 109 (31.4%) | 165 (25.4%) | 30 (10.3%) | 22 (8.0%) | ||
| 4–7 days/week | 82 (23.6%) | 214 (33.0%) | 4 (1.4%) | 10 (3.6%) | ||
| Physical activity | ||||||
| 6–7 days/week | 56 (16.1%) | 87 (13.5%) | 0.021 * | 43 (14.8%) | 37 (13.5%) | 0.044 * |
| 3–5 days/week | 121 (34.9%) | 195 (30.0%) | 95 (32.8%) | 75 (27.4%) | ||
| 1–2 days/week | 118 (34.0%) | 219 (33.7%) | 73 (25.2%) | 77 (28.1%) | ||
| None | 52 (15.0%) | 148 (22.8%) | 79 (27.2%) | 85 (31.0%) | ||
| Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Waist circumference | ||||
| Normal | Reference | – | Reference | – |
| Obesity | 1.254 (1.017–1.861) | 0.023 * | 1.151 (1.010–2.291) | 0.014 * |
| Smoking status | ||||
| None | Reference | – | Reference | – |
| Former | 1.100 (0.847–1.598) | 0.410 | 1.098 (0.857–1.597) | 0.460 |
| Current | 1.781 (1.349–2.856) | <0.001 * | 1.884 (1.298–2.749) | <0.001 * |
| Alcohol frequency | ||||
| 0–1 day/week | Reference | – | Reference | – |
| 2–3 days/week | 1.044 (0.664–1.267) | 0.413 | 1.019 (0.660–1.161) | 0.271 |
| 4–7 days/week | 1.541 (0.545–2.219) | 0.084 | 1.121 (1.061–2.113) | 0.034 * |
| Physical activity | ||||
| Every day | Reference | – | Reference | – |
| 3–5 days/week | 1.074 (0.686–1.721) | 0.687 | 1.039 (0.709–1.569) | 0.581 |
| 1–2 days/week | 1.114 (0.741–1.796) | 0.749 | 1.241 (0.798–1.880) | 0.145 |
| None | 1.397 (1.018–2.340) | 0.019 * | 1.693 (1.087–2.913) | 0.022 * |
| Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Waist circumference | ||||
| Normal | Reference | – | Reference | – |
| Obesity | 1.231 (1.014–2.019) | 0.021 * | 1.178 (1.015–2.612) | 0.019 * |
| Smoking status | ||||
| None | Reference | – | Reference | – |
| Former | 1.358 (0.584–2.513) | 0.126 | 1.040 (0.653–3.746) | 0.294 |
| Present | 2.769 (0.735–5.570) | 0.108 | 2.591 (0.747–4.710) | 0.200 |
| Alcohol frequency | ||||
| 0–1 day/week | Reference | – | Reference | – |
| 2–3 days/week | 0.889 (0.534–1.840) | 0.667 | 0.879 (0.348–1.640) | 0.613 |
| 4–7 days/week | 3.145 (0.646–7.687) | 0.124 | 2.491 (0.640–5.749) | 0.314 |
| Physical activity | ||||
| Every day | Reference | – | Reference | – |
| 3–5 days/week | 0.851 (0.547–1.904) | 0.850 | 1.671 (0.870–2.501) | 0.349 |
| 1–2 days/week | 1.119 (0.639–1.841) | 0.521 | 1.519 (0.744–3.697) | 0.870 |
| None | 1.150 (0.841–2.409) | 0.221 | 1.861 (1.068–3.451) | 0.018 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, S.; Zhang, J.; Kim, Y.; Zhang, W. Prevalence of Colorectal Polyps Based on Cardiorespiratory Fitness, Muscle Strength, Health Behavior, and Abdominal Obesity in Asymptomatic Elderly. Healthcare 2021, 9, 1400. https://doi.org/10.3390/healthcare9101400
Zhang S, Zhang J, Kim Y, Zhang W. Prevalence of Colorectal Polyps Based on Cardiorespiratory Fitness, Muscle Strength, Health Behavior, and Abdominal Obesity in Asymptomatic Elderly. Healthcare. 2021; 9(10):1400. https://doi.org/10.3390/healthcare9101400
Chicago/Turabian StyleZhang, Shiyu, Junyong Zhang, Yonghwan Kim, and Wangyang Zhang. 2021. "Prevalence of Colorectal Polyps Based on Cardiorespiratory Fitness, Muscle Strength, Health Behavior, and Abdominal Obesity in Asymptomatic Elderly" Healthcare 9, no. 10: 1400. https://doi.org/10.3390/healthcare9101400
APA StyleZhang, S., Zhang, J., Kim, Y., & Zhang, W. (2021). Prevalence of Colorectal Polyps Based on Cardiorespiratory Fitness, Muscle Strength, Health Behavior, and Abdominal Obesity in Asymptomatic Elderly. Healthcare, 9(10), 1400. https://doi.org/10.3390/healthcare9101400