
Is Misoprostol Vaginal Insert Safe for the Induction of Labor in High-Risk Pregnancy Obese Women?

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
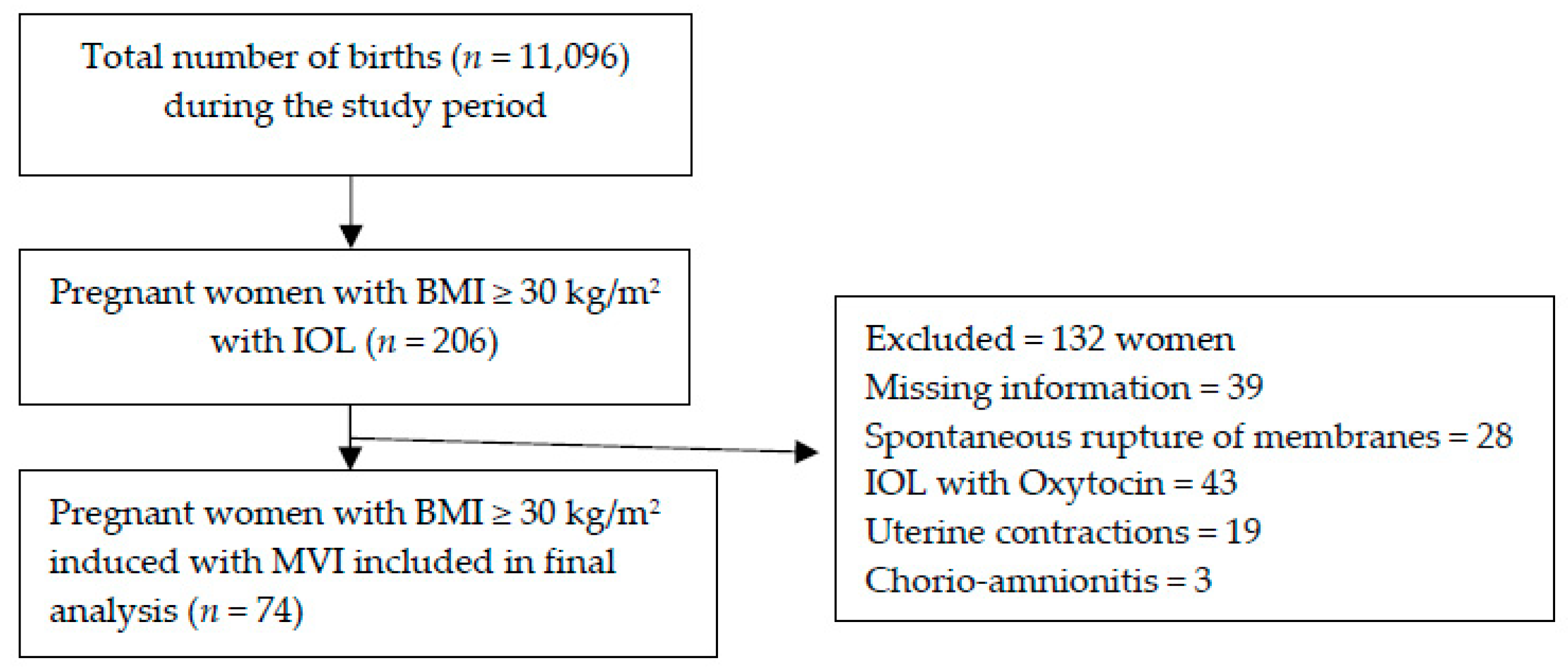
2.1. Study Design
2.2. Clinical Evaluation and Data Collection
2.3. Statistics
3. Results
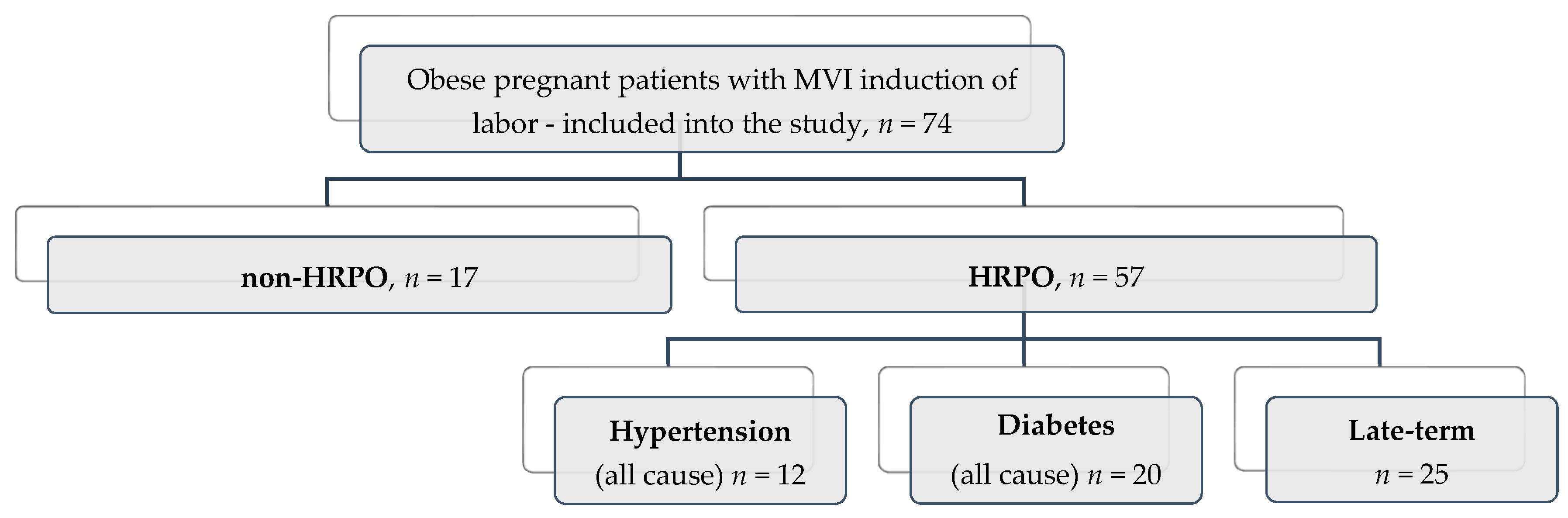
3.1. Description of the Studied Group
3.2. Evaluation of Failure Rate for Induction of Labor (IOL) with Misoprostol Vaginal Insert (MVI). Incidence of Cesarean Section
3.3. Safety Profile
3.4. Correlations between Study Subgroups and Outcomes of the MVI IOL
4. Discussion
4.1. Limitations
4.2. Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| C-section | Cesarean section |
| EU | European Union |
| FDA | Food Drug Administration |
| GPCR | G protein-coupled receptors |
| HELLP | Hemolysis, elevated liver enzymes, low platelet count. |
| HRPO | High risk pregnant obese women |
| IOL | Induction of labor—artificially initiated labor |
| MVI | Misoprostol vaginal insert |
| NICU | Neonatal intensive care unit |
| NSAIDs | Non-steroidal anti-inflammatory drugs |
| PROM | Prelabour rupture of membrane |
| P.G.s | Prostaglandins |
| PGE2 | Prostaglandin E2 |
| WHO | World Health Organization |
| SPSS® | Statistical Package for the Social Sciences, IBM® |
| Tmax | Time to peak plasma levels |
References
- World Health Organization. WHO Recommendations for Induction of Labour; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- WHO. WHO Recommendations for Induction of Labour. Available online: http://www.who.int/reproductivehealth/publications/maternal_perinatal_health/9789241501156/en (accessed on 29 March 2021).
- Gissler, M.; Mohangoo, A.D.; Blondel, B.; Chalmers, J.; Macfarlane, A.; Gaižauskiené, A.; Gatt, M.; Lack, N.; Sakkeus, L.; Zeitlin, J. Perinatal health monitoring in Europe: Results from the EURO-PERISTAT project. Inform. Health Soc. Care 2010, 35, 64–79. [Google Scholar] [CrossRef] [PubMed]
- Levine, L.D. Cervical ripening: Why we do what we do. Semin. Perinatol. 2020, 44, 151216. [Google Scholar] [CrossRef]
- Acharya, T.; Devkota, R.; Bhattarai, B.; Acharya, R. Outcome of misoprostol and oxytocin in induction of labour. SAGE Open Med. 2017, 5. [Google Scholar] [CrossRef]
- Leduc, D.; Biringer, A.; Lee, L.; Dy, J.; Corbett, T.; Duperron, L.; Lange, I.; Muise, S.; Parish, B.; Regush, L.; et al. Induction of Labour. J. Obstet. Gynaecol. Can. 2013, 35, 840–857. [Google Scholar] [CrossRef]
- Pimentel, V.M.; Arabkhazaeli, M.; Moon, J.-Y.; Wang, A.; Kapedani, A.; Bernstein, P.S.; Tropper, P.J. Induction of labor using one dose vs multiple doses of misoprostol: A randomized controlled trial. Am. J. Obstet. Gynecol. 2018, 218, 614.e1–614.e8. [Google Scholar] [CrossRef] [Green Version]
- Bakker, R.; Pierce, S.; Myers, D. The role of prostaglandins E1 and E2, dinoprostone, and misoprostol in cervical ripening and the induction of labor: A mechanistic approach. Arch. Gynecol. Obstet. 2017, 296, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Ande, A.B.; Ezeanochie, C.M.; Olagbuji, N.B. Induction of labor in prolonged pregnancy with unfavorable cervix: Comparison of sequential intracervical Foley catheter–intravaginal misoprostol and intravaginal misoprostol alone. Arch. Gynecol. Obstet. 2011, 285, 967–971. [Google Scholar] [CrossRef]
- Hofmeyr, G.J.; Gülmezoglu, A.M. Vaginal misoprostol for cervical ripening and induction of labour. Cochrane Database Syst. Rev. 2003, CD000941. [Google Scholar] [CrossRef]
- Raj, G.M.; Raveendran, R. Introduction to Basics of Pharmacology and Toxicology; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany, 2021; Volume 2021. [Google Scholar]
- Tang, O.S.; Gemzell-Danielsson, K.; Ho, P.C. Misoprostol: Pharmacokinetic profiles, effects on the uterus and side-effects. Int. J. Gynecol. Obstet. 2007, 99, S160–S167. [Google Scholar] [CrossRef]
- Rossi, R.M.; Warshak, C.R.; Masters, H.R.; Regan, J.K.; Kritzer, S.A.; Magner, K.P. Comparison of prostaglandin and mechanical cervical ripening in the setting of small for gestational age neonates*. J. Matern. Neonatal Med. 2018, 32, 3841–3846. [Google Scholar] [CrossRef]
- Allen, R.; O’Brien, B.M. Uses of Misoprostol in Obstetrics and Gynecology. Rev. Obstet. Gynecol. 2009, 2, 159–168. [Google Scholar]
- Stephenson, M.L.; Hawkins, J.S.; Powers, B.L.; Wing, D.A. Misoprostol Vaginal Insert for Induction of Labor: A Delivery System with Accurate Dosing and Rapid Discontinuation. Women’s Health 2014, 10, 29–36. [Google Scholar] [CrossRef]
- Vallera, C.; Choi, L.O.; Cha, C.M.; Hong, R.W. Uterotonic Medications. Anesthesiol. Clin. 2017, 35, 207–219. [Google Scholar] [CrossRef]
- Misoprostol. Available online: https://go.drugbank.com/drugs/DB00929 (accessed on 28 February 2021).
- Drabo, S. A Pill in the Lifeworld of Women in Burkina Faso: Can Misoprostol Reframe the Meaning of Abortion. Int. J. Environ. Res. Public Health 2019, 16, 4425. [Google Scholar] [CrossRef] [Green Version]
- Aubert, J.; Bejan-Angoulvant, T.; Jonville-Béra, A.-P. Pharmacologie du misoprostol (données pharmacocinétiques, tolérance et effets tératogènes). J. Gynécologie Obs. Biol. Reprod. 2014, 43, 114–122. [Google Scholar] [CrossRef]
- Henriques, A.; Lourenço, A.V.; Ribeirinho, A.; Ferreira, H.; Graça, L.M. Maternal Death Related to Misoprostol Overdose. Obstet. Gynecol. 2007, 109, 489–490. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, V.; O’Kelly, S.; Monaghan, B.; Rowan, A.; Farah, N.; Turner, M.J. Maternal obesity and induction of labor. Acta Obstet. Gynecol. Scand. 2013, 92, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- Deruelle, P.; Patte, C. A critical appraisal of the misoprostol removable, controlled-release vaginal delivery system of labor induction. Int. J. Women’s Health 2015, 7, 889–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayburn, W.F.; Powers, B.L.; Plasse, T.F.; Carr, D.; Di Spirito, M. Pharmacokinetics of a Controlled-Release Misoprostol Vaginal Insert at Term. J. Soc. Gynecol. Investig. 2006, 13, 112–117. [Google Scholar] [CrossRef]
- Handal-Orefice, R.C.; Friedman, A.M.; Chouinard, S.M.; Eke, A.C.; Feinberg, B.; Politch, J.; Iverson, R.E.; Yarrington, C.D. Oral or Vaginal Misoprostol for Labor Induction and Cesarean Delivery Risk. Obstet. Gynecol. 2019, 134, 10–16. [Google Scholar] [CrossRef]
- ACOG Committee on Practice Bulletins. Obstetrics ACOG Practice Bulletin No. 107: Induction of Labor. Obstet. Gynecol. 2009, 114, 386–397. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Practice Bulletin No. 146. Obstet. Gynecol. 2014, 124, 390–396. [Google Scholar] [CrossRef]
- SOGC Clinical Practice Guideline No. 296, 2013: Induction of Labor. Journal of Obstetrics Gynecology, Canada. Available online: https://www.guidelinecentral.com/summaries/induction-of-labour/#section-date (accessed on 29 March 2021).
- Overview|Inducing Labour|Guidance|NICE. Available online: https://www.nice.org.uk/guidance/cg70 (accessed on 29 March 2021).
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paredes, C.; Hsu, R.C.; Tong, A.; Johnson, J.R. Obesity and Pregnancy. NeoReviews 2021, 22, e78–e87. [Google Scholar] [CrossRef]
- Poston, L.; Caleyachetty, R.; Cnattingius, S.; Corvalán, C.; Uauy, R.; Herring, S.; Gillman, M.W. Preconceptional and maternal obesity: Epidemiology and health consequences. Lancet Diabetes Endocrinol. 2016, 4, 1025–1036. [Google Scholar] [CrossRef]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of Gestational Weight Gain With Maternal and Infant Outcomes. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef]
- Glazer, K.B.; Danilack, V.A.; Field, A.E.; Werner, E.F.; Savitz, D.A. Term Labor Induction and Cesarean Delivery Risk among Obese Women with and without Comorbidities. Am. J. Perinatol. 2020. [Google Scholar] [CrossRef]
- Lauth, C.; Huet, J.; Dolley, P.; Thibon, P.; Dreyfus, M. Maternal obesity in prolonged pregnancy: Labor, mode of delivery, maternal and fetal outcomes. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 101909. [Google Scholar] [CrossRef]
- Hersh, A.R.; Skeith, A.E.; Sargent, J.A.; Caughey, A.B. Induction of labor at 39 weeks of gestation versus expectant management for low-risk nulliparous women: A cost-effectiveness analysis. Am. J. Obstet. Gynecol. 2019, 220, 590.e1–590.e10. [Google Scholar] [CrossRef]
- Coates, D.; Homer, C.; Wilson, A.; Deady, L.; Mason, E.; Foureur, M.; Henry, A. Induction of labour indications and timing: A systematic analysis of clinical guidelines. Women Birth 2020, 33, 219–230. [Google Scholar] [CrossRef]
- Hawkins, J.S.; Stephenson, M.; Powers, B.; Wing, D.A. Diabetes mellitus: An independent predictor of duration of prostaglandin labor induction. J. Perinatol. 2017, 37, 488–491. [Google Scholar] [CrossRef]
- Zhang, J.; Bricker, L.; Wray, S.; Quenby, S. Poor uterine contractility in obese women. BJOG Int. J. Obstet. Gynaecol. 2007, 114, 343–348. [Google Scholar] [CrossRef]
- Maged, A.M.; El-Semary, A.M.; Marie, H.M.; Belal, D.S.; Hany, A.; Taymour, M.A.; Omran, E.F.; ElBaradie, S.M.Y.; Mohamed, M.A.K. Effect of maternal obesity on labor induction in postdate pregnancy. Arch. Gynecol. Obstet. 2018, 298, 45–50. [Google Scholar] [CrossRef]
- Rosen, H.; Melamed, N.; Porat, S.; Farine, D.; Maxwell, C.; Ronzoni, S. Maternal Obesity Class as a Predictor of Induction Failure: A Practical Risk Assessment Tool. Am. J. Perinatol. 2015, 32, 1298–1304. [Google Scholar] [CrossRef]
- Maggi, C.; Mazzoni, G.; Gerosa, V.; Fratelli, N.; Prefumo, F.; Sartori, E.; Lojacono, A. Labor induction with misoprostol vaginal insert compared with dinoprostone vaginal insert. Acta Obstet. Gynecol. Scand. 2019, 98, 1268–1273. [Google Scholar] [CrossRef] [PubMed]
- Hansen, W.; Mccord, L.; Manning, M.; O’Brien, J.; Curry, T.; Garabedian, M. Up-Regulation of Oxytocin Receptor Expression at Term Is Related to Maternal Body Mass Index. Am. J. Perinatol. 2013, 30, 491–498. [Google Scholar] [CrossRef]
- Lassiter, J.R.; Holliday, N.; Lewis, D.F.; Mulekar, M.; Abshire, J.; Brocato, B. Induction of labor with an unfavorable cervix: How does BMI affect success? J. Matern. Neonatal Med. 2015, 29, 3000–3002. [Google Scholar] [CrossRef]
- Romanian Society of Obstetrics and Ginecology of Romania. Clinical Guidelines Revised Edition 2019. Available online: https://sogr.ro/ghiduri-clinice-2019-finale (accessed on 12 April 2021).
- Bolla, D.; Weissleder, S.V.; Radan, A.-P.; Gasparri, M.L.; Raio, L.; Müller, M.; Surbek, D. Misoprostol vaginal insert versus misoprostol vaginal tablets for the induction of labour: A cohort study. BMC Pregnancy Childbirth 2018, 18, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckwith, L.; Magner, K.; Kritzer, S.; Warshak, C.R. Prostaglandin versus mechanical dilation and the effect of maternal obesity on failure to achieve active labor: A cohort study. J. Matern. Neonatal Med. 2016, 30, 1621–1626. [Google Scholar] [CrossRef] [PubMed]
- Pevzner, L.; Powers, B.L.; Rayburn, W.F.; Rumney, P.; Wing, D.A. Effects of Maternal Obesity on Duration and Outcomes of Prostaglandin Cervical Ripening and Labor Induction. Obstet. Gynecol. 2009, 114, 1315–1321. [Google Scholar] [CrossRef]
- Rossi, R.M.; Requarth, E.W.; Warshak, C.R.; Dufendach, K.; Hall, E.S.; DeFranco, E.A. Predictive Model for Failed Induction of Labor Among Obese Women. Obstet. Gynecol. 2019, 134, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Wing, D.A.; Stephenson, M.L. A novel misoprostol delivery system for induction of labor: Clinical utility and patient considerations. Drug Des. Dev. Ther. 2015, 9, 2321–2327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, J.; Nugent, R.; Vangaveti, V. Influence of maternal obesity on Bishop Score and failed induction of labour: A retrospective cohort study in a regional tertiary centre. Aust. N. Zealand J. Obstet. Gynaecol. 2019, 59, 243–250. [Google Scholar] [CrossRef]
- Global Obesity Observatory-Romania. Available online: https://data.worldobesity.org/country/romania-178/#data_prevalence (accessed on 29 March 2021).
- Carlhäll, S.; Källén, K.; Blomberg, M. The effect of maternal body mass index on duration of induced labor. Acta Obstet. Gynecol. Scand. 2019, 99, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Benalcazar-Parra, C.; Monfort-Orti, R.; Ye-Lin, Y.; Prats-Boluda, G.; Alberola-Rubio, J.; Perales, A.; Garcia-Casado, J. Comparison of labour induction with misoprostol and dinoprostone and characterization of uterine response based on electrohysterogram. J. Matern. Neonatal Med. 2017, 32, 1586–1594. [Google Scholar] [CrossRef]
- Viteri, O.A.; Tabsh, K.K.; Alrais, M.A.; Salazar, X.C.; Lopez, J.M.; Fok, R.Y.; Chauhan, S.P.; Sibai, B.M. Transcervical Foley Balloon Plus Vaginal Misoprostol versus Vaginal Misoprostol Alone for Cervical Ripening in Nulliparous Obese Women: A Multicenter, Randomized, Comparative-Effectiveness Trial. Am. J. Perinatol. 2020. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| High-Risk Pregnancies | WHO (2018) | ACOG (2014) | SOGC (2013) | NICE (2008) |
|---|---|---|---|---|
| Late-term pregnancy | Yes | No | Yes | Yes |
| Diabetes | Yes | Yes | Yes | Yes |
| Preeclampsia | N/A | Yes | Yes | N/A |
| Demographic Data | Non-High-Risk Pregnant Obese Women (Non HRPO) N = 17 | High Risk Pregnant Obese Women (HRPO) (N = 57) | p-Value * | ||
|---|---|---|---|---|---|
| Late-Term n = 25 | Diabetes n = 20 | Hypertension n = 12 | |||
| Maternal age, mean (SD) | 28.5 ± 6.3 | 29.4 ± 3.1 | 32.2 ± 3.9 | 29.3 ± 5.4 | 0.173 |
| Area of residence | |||||
| Urban (n) | 12 | 20 | 15 | 9 | 0.919 |
| Rural (n) | 5 | 5 | 5 | 3 | |
| BMI class, mean (SD) | |||||
| obese class I | 13 (76.4%) | 18 (31.6%) | 14 (24.6%) | 10 (17.5%) | |
| obese class II | 4 (23.6%) | 7 (12.3%) | 6 (10.5%) | 2 (3.5%) | |
| Mean BMI (SD) | 33.1 ± 2.6 | 34.1 ± 2.8 | 33.7 ± 3.1 | 32.5 ± 1.4 | 0.144 |
| Parity | |||||
| Primiparous (n) | 17 | 23 | 19 | 9 | 0.096 |
| Multiparous (n) | 0 | 2 | 1 | 3 | |
| Induction data | |||||
| GA at delivery (weeks), mean (SD) | 39.3 ± 0.8 | 41 ± 0 | 38.3 ± 0.5 | 38.5 ± 0.7 | <0.001 |
| Bishop score, mean (SD) | 2.2 ± 0.8 | 1.3 ± 1.4 | 1.7 ± 1.2 | 2.6 ± 1.0 | 0.003 |
| Neonatal outcomes | |||||
| Birth weight (grams), mean (SD) | 3205.8 ± 301.3 | 3450 ± 0.8 | 3417.5 ± 478.8 | 3250 ± 342.4 | 0.165 |
| NICU admission, n (%) | 2 (11.7%) | 2 (3.5%) | 3 (5.2%) | 2 (3.5%) | 0.853 |
| HRPO * (n = 57) (n/%) | non-HRPO * (n = 17) (n/%) | p-Value | |
|---|---|---|---|
| Vaginal deliveries | 40 (70.2%) | 13 (72.4%) | 0.39 |
| C-sections | 17 (29.8%) | 4 (23.5%) | 0.46 |
| Non HRPO Women (n = 17, 23.0%) | HRPO Women (n = 57, 77.0%) | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | 95% CI | Late-Term (n = 25) Mean ± SD | Diabetes (n = 20) Mean ± SD | Preeclampsia (n = 12) Mean ± SD | Total (n = 57) Mean ± SD | 95% CI | ||
| Misoprostol action (h) | 12.4 ± 5.7 | 9.5–15.3 | 11.0 ± 5.9 | 10.8 ± 3.9 | 12.3 ± 6.6 | 11.2 ± 5.4 | 9.8–12.6 | 0.435 |
| Time induction to delivery (h) | 18.4 ± 8.5 | 14.1–22.8 | 16.7 ± 5.5 | 16.6 ± 4.7 | 17.3 ± 7.4 | 17.0 ± 5.6 | 15.5–18.5 | 0.041 |
| Initial Bishop score | 2.2 ± 0.8 | 1.8–2.7 | 1.2 ± 1.5 | 1.7 ± 1.2 | 2.7 ± 1.1 | 1.7 ± 1.4 | 1.4–2.1 | 0.147 |
| 1-min Appgar score | 8.5 ± 0.9 | 8.0–9.0 | 8.5 ± 0.7 | 8.4 ± 1.2 | 8.4 ± 0.8 | 8.5 ± 0.9 | 8.2–8.7 | 0.990 |
| 5-min Appgar score | 9.2 ± 0.8 | 8.8–9.6 | 9.1 ± 0.6 | 9 ± 0.6 | 9 ± 0.6 | 9.0 ± 0.6 | 8.7–9.2 | 0.372 |
| Weight (grams) | 3205.9 ± 434.4 | 2982.5–3429.2 | 3450 ± 301.4 | 3417 ± 478.8 | 3417.5 ± 478.8 | 3396.5 ± 381.8 | 3295.1–3497.8 | 0.084 |
| Gestational age (weeks) | 39.8 ± 0.9 | 39.4–40.3 | 41.3 ± 0.2 | 38.9 ± 0.6 | 38.9 ± 0.6 | 39.9 ± 1.3 | 39.5–40.3 | 0.901 |
| HRPO Women | Non HRPO Women | p-Value | |||
|---|---|---|---|---|---|
| Mean ± SD | 95% CI | Mean ± SD | 95% CI | ||
| Cesareans (n = 21) | n = 17, 81.0% | n = 4, 19.0% | |||
| Misoprostol action (h) | 10.9 ± 4.9 | 8.4–13.4 | 10.9 ± 2.3 | 7.2–14.6 | 0.985 |
| Time induction to delivery (h) | 17.3 ± 4.8 | 14.8–19.7 | 15.2 ± 4.6 | 7.9–22.5 | 0.453 |
| Initial Bishop score | 2.1 ± 1.5 | 1.3–2.9 | 2.3 ± 0.5 | 1.5–3.1 | 0.869 |
| 1-min Appgar score | 8.2 ± 1.1 | 7.6–8.7 | 7.8 ± 1.3 | 5.8–9.8 | 0.496 |
| 5-min Appgar score | 9.0 ± 0.7 | 8.6–9.4 | 8.5 ± 0.6 | 7.6–9.4 | 0.207 |
| Weight (grams) | 3252.9 ± 271.8 | 3113.2–3392.7 | 3275.0 ± 450.0 | 2558.9–3991.1 | 0.898 |
| Gestational age (weeks, mean ± SD) | 39.6 ± 1.3 | 38.9–40.3 | 40.0 ± 0.7 | 38.8–41.3 | 0.578 |
| Spontaneous births (n = 42) | n = 33, 78.6% | n = 9, 21.4% | |||
| Misoprostol action (h) | 10.8 ± 5.9 | 8.7–12.9 | 15.7 ± 5.5 | 11.5–20.0 | 0.029 |
| Time induction to delivery (h) | 16.3 ± 6.2 | 14.1–18.5 | 23.7 ± 7.7 | 17.8–29.6 | 0.004 |
| Initial Bishop score | 1.5 ± 1.3 | 1.0–2.0 | 2.6 ± 0.9 | 1.9–3.2 | 0.028 |
| 1-min Appgar score | 8.6 ± 0.7 | 8.4–8.9 | 8.6 ± 0.7 | 8.0–9.1 | 0.851 |
| 5-min Appgar score | 9.0 ± 0.5 | 8.9–9.2 | 9.3 ± 0.9 | 8.7–10.0 | 0.165 |
| Weight (grams) | 3472.7 ± 400.4 | 3330.8–3614.7 | 3316.7 ± 394.5 | 3013.4–3619.9 | 0.305 |
| Gestational age (weeks, mean ± SD) | 40.2 ± 1.2 | 39.7–40.6 | 39.9 ± 0.9 | 39.1–40.6 | 0.500 |
| Instrumental delivery (n = 11) | n = 7, 63.6% | n = 4, 36.4% | p-value * | ||
| Misoprostol action (h) | 13.8 ± 4.0 | 10.1–17.5 | 6.4 ± 1.7 | 3.8–9.0 | 0.007 |
| Time induction to delivery (h) | 17.9 ± 3.7 | 16.5–23.3 | 11.9 ± 2.9 | 5.3–14.4 | 0.001 |
| Initial Bishop score | 1.9 ± 1.1 | 0.9–2.9 | 1.5 ± 0.6 | 0.6–2.4 | 0.557 |
| 1-min Appgar score | 8.6 ± 1.1 | 7.5–9.6 | 9.0 ± 0.8 | 7.7–10.3 | 0.527 |
| 5-min Appgar score | 9.0 ± 0.8 | 8.2–9.8 | 9.5 ± 0.6 | 8.6–10.4 | 0.312 |
| Weight (grams) | 3385.7 ± 467.0 | 2953.8–3817.6 | 2887.5 ± 458.9 | 2157.2–3617.8 | 0.121 |
| Gestational age (weeks, mean ± SD) | 39.2 ± 1.5 | 37.7–40.6 | 39.6 ± 1.1 | 37.8–41.4 | 0.638 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varlas, V.N.; Bostan, G.; Nasui, B.A.; Bacalbasa, N.; Pop, A.L. Is Misoprostol Vaginal Insert Safe for the Induction of Labor in High-Risk Pregnancy Obese Women? Healthcare 2021, 9, 464. https://doi.org/10.3390/healthcare9040464
Varlas VN, Bostan G, Nasui BA, Bacalbasa N, Pop AL. Is Misoprostol Vaginal Insert Safe for the Induction of Labor in High-Risk Pregnancy Obese Women? Healthcare. 2021; 9(4):464. https://doi.org/10.3390/healthcare9040464
Chicago/Turabian StyleVarlas, Valentin Nicolae, Georgiana Bostan, Bogdana Adriana Nasui, Nicolae Bacalbasa, and Anca Lucia Pop. 2021. "Is Misoprostol Vaginal Insert Safe for the Induction of Labor in High-Risk Pregnancy Obese Women?" Healthcare 9, no. 4: 464. https://doi.org/10.3390/healthcare9040464
APA StyleVarlas, V. N., Bostan, G., Nasui, B. A., Bacalbasa, N., & Pop, A. L. (2021). Is Misoprostol Vaginal Insert Safe for the Induction of Labor in High-Risk Pregnancy Obese Women? Healthcare, 9(4), 464. https://doi.org/10.3390/healthcare9040464