
Mobile Health to Improve Adherence and Patient Experience in Heart Transplantation Recipients: The mHeart Trial

 , , and
, , and
Abstract: Background
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Design
2.3. Measures
2.3.1. Adherence to Medication Measures
2.3.2. Patients’ Experience with Their Medication Regimen
2.3.3. Type of Pharmaceutical Care Follow-Up at the End of the Study and Beyond
2.3.4. Sociodemographic and Clinical Data
2.4. Study Reporting Guidelines
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BAASIS | Basel Assessment of Adherence to Immunosuppressive Medications Scale |
| CG | control group |
| eHealth | use of information and communication technologies for health |
| EHR | electronic health records |
| HTx | heart transplant |
| IG | intervention group |
| IMTS | Immunosuppressive Medication Timing Scale |
| ISHLT | International Society of Heart and Lung Transplantation |
| mHealth | mobile health |
| mHeart | a mobile health system for the heart transplant population |
| MNA | medication non-adherence |
| RCT | randomized controlled trial |
| SMAQ | Spanish version of the Simplified Medication Adherence Questionnaire |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Adherence Evaluation | Total HTx Patients (N = 134) | CG (N = 63) | IG (N = 71) | Statistics OR (IC 95%) | P-Value |
|---|---|---|---|---|---|
| Adherence to IS treatment | |||||
| SMAQ Global (Adh.), N (%) | |||||
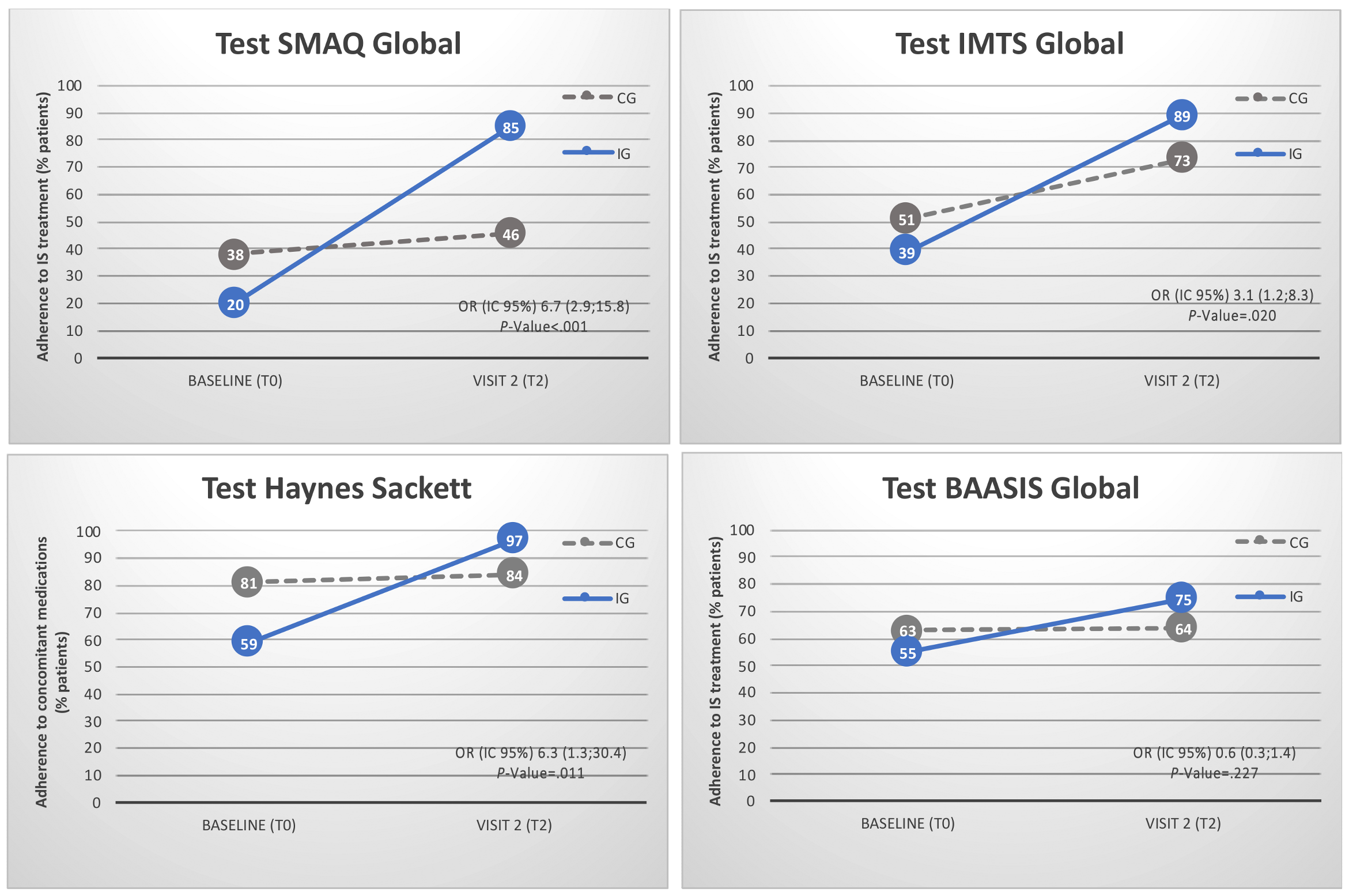
| • T0 | 38 (29) | 24 (38) | 14 (20) | 0.4 (0.2;0.9) | 0.028 * |
| • T2 | 81 (67) | 25 (46) | 56 (85) | 6.7 (2.9;15.8) | <0.001 * |
| • Statistics OR (IC 95%) | 2.2 (0.7; 6.7) | 2.3 (0.3;19.7) | |||
| • P-value McNemar test | 0.286 | <0.001 | |||
| IMTS Global (Adh.), N (%) | |||||
| • T0 | 59 (44) | 32 (51) | 27 (39) | 0.6 (0.3;1.2) | 0.157 * |
| • T2 | 98 (82) | 40 (73) | 58 (89) | 3.1 (1.2;8.3) | 0.020 * |
| • (IC 95%) | 3.7 (1.0;13.7) | 4.2 (0.5;37.5) | |||
| • P-value McNemar test | 0.007 | <.0001 | |||
| BAASIS Global (Adh.), N (%) | |||||
| • T0 | 64 (59) | 34 (63) | 30 (55) | 1.4 (0.7;3.1) | 0.372 * |
| • T2 | 89 (69) | 30 (64) | 39 (75) | 0.6 (0.3;1.4) | 0.227 * |
| • Statistics OR (IC 95%) | 12 (2.6;54.2) | 6.2 (1.4;27.9) | |||
| • P-value McNemar test | 1.0 | 0.057 | |||
| BAASIS (5). VAS Scale, M ± SD | |||||
| • T0 | 93 ± 14 | 93 ± 13 | 93 ± 16 | - | 0.672 ** |
| • T2 | 95 ± 8 | 95 ± 7 | 96 ± 9 | - | 0.225 ** |
| • P-value Friedman test | 0.739 | 0.033 | |||
| Adherence to other medications | |||||
| Haynes Sackett (Adh), N (%) | |||||
| • T0 | 93 (69) | 52 (81) | 41 (59) | 0.3 (0.2;0.7) | 0.004 * |
| • T2 | 110 (92) | 46 (84) | 64 (97) | 6.3 (1.3;30.4) | 0.011 * |
| • Statistics OR (IC 95%) | 1.1 (0.2; 6.6) | 1.5 (0.1;24.4) | |||
| • P-value McNemar test | 0.804 | <0.001 | |||
| Adherence to visits, N (%) | |||||
| T0 | 133 (99) | 64 (100) | 69 (99) | _ | 0.337 * |
| T2 | 121 (90) | 55 (86) | 66 (94) | 0.37 (0.1;1.3) | 0.103 * |
| P-value McNemar test | - | 0.375 | |||
| IS drugs levels | |||||
| CV%, M ± SD) | 33 ± 18 | 34 ± 22 | 29 ± 15 | - | 0.392 ** |
| CV% > 30%, N (%) | 87 (49) | 30 (47) | 29 (41) | - | 0.526 *** |
| Subtherapeutic blood levels, N (M ± SD) | 126 (3 ± 3) | 48 (4 ± 4) | 49 (3 ± 2) | - | 0.251 ** |
| Supratherapeutic blood levels, N (M ± SD) | 83 (4 ± 4) | 23 (4 ± 4) | 20 (2 ± 4) | - | 0.050 ** |
| Therapeutic blood levels, N (%) | 25 (14) | 11 (17) | 13 (19) | - | <0.001 *** |
| Composite adherence score 1, N (%) | |||||
| T0 | 27 (15) | 13 (20) | 6 (9) | - | 0.052 *** |
| T2 | 60 (34) | 15 (23) | 36 (51) | 0.3 (0.1;0.6) | 0.001 *** |
| P-value McNemar test | 0.791 | <0.001 |
Appendix B
| Variables | Total HTx Patients (N = 134) | CG (N = 63) | IG (N = 71) | Statistics OR (IC 95%) | P-Value |
|---|---|---|---|---|---|
| Number of patients feeling that they take excessive medication (Yes), N (%) | |||||
| • T0 | 82 (63) | 35 (56) | 47 (69) | 1.79 (0.9;3.7) | 0.109 * |
| • T2 | 47 (39) | 23 (42) | 24 (36) | 0.80 (0.4;1.7) | 0.540 * |
| • Statistics OR (IC 95%) | - | 3.9 (1.2;12.6) | 4.5 (1.2;17.7) | ||
| • P-value McNemar test | - | 0.167 | <0.001 | ||
| Degree of inconvenience perceived by the patient related to taking medication as prescribed every day (scored 0-10), M ± SD | |||||
| • T0 | 2 ± 3 | 2 ± 2 | 3 ± 3 | - | 0.661 * |
| • T2 | 1 ± 2 | 2 ± 3 | 0.5 ± 2 | - | 0.002 * |
| • Statistics OR (IC 95%) | - | - | - | ||
| • P-value T-test | - | 0.029 | 1.94 | ||
| Patients’ awareness of the importance of immunosuppressive therapy and consequences of not taking it, N (%) | |||||
| 1. “If you discontinued taking your immunosuppressants completely, what do you think would happen to you? (answer 3: rejection)” | |||||
| • T0 | 95 (72) | 47 (75) | 48 (70) | - | 0.762 * |
| • T2 | 119 (98) | 53 (96) | 66 (100) | - | 0.361 |
| • Statistics OR (IC 95%) | - | ||||
| • P-value Friedman test | - | 0.001 | <0.001 | ||
| 2. “If you sometimes forgot to take your immunosuppressants, what do you think would happen to you?” (answer 3: rejection) | |||||
| • T0 | 77 (59) | 41 (66) | 36 (52) | - | 0.114 * |
| • T2 | 107 (88) | 47 (86) | 60 (91) | - | 0.201 * |
| • Statistics OR (95% CI) | - | ||||
| • P-value Friedman test | - | 0.012 | <0.001 | ||
| Knowledge of the medication regimen (% of medications of total prescribed), M ± SD | |||||
| Proportion of medication names remembered | |||||
| • T0 | 76 ± 29 | 73 ± 33 | 79 ± 25 | - | 0.528 ** |
| • T2 | 84 ± 27 | 77 ± 32 | 91 ± 20 | - | 0.006 ** |
| • P-value Wilcoxon test | - | 0.750 | 0.197 | ||
| Proportion of medication doses remembered | |||||
| • T0 | 51 ± 29 | 51 ± 32 | 50 ± 26 | - | 0.864 ** |
| • T2 | 63 ± 29 | 56 ± 32 | 69 ± 25 | - | 0.030 ** |
| • P-value Wilcoxon test | - | 0.842 | 0.072 | ||
| Proportion of medication timing intakes remembered | |||||
| • T0 | 79 ± 25 | 81 ± 26 | 79 ± 25 | - | 0.533 ** |
| • T2 | 91 ± 21 | 87 ± 24 | 93 ± 18 | - | 0.019 ** |
| • P-value Wilcoxon test | - | 0.792 | 0.058 | ||
| Proportion of medication indications remembered (the use of that drug for treating) | |||||
| • T0 | 62 ± 34 | 58 ± 35 | 65 ± 34 | - | 0.213 ** |
| • T2 | 83 ± 24 | 77 ± 26 | 88 ± 22 | - | 0.003 ** |
| • P-value Wilcoxon test | - | 0.284 | 0.014 | ||
| Number of medication side effects reported by patients, M ± SD, IQR | |||||
| • T0 | 6 ± 3, 4;7;8 | 6 ± 3 | 7 ± 3 | - | 0.294 ** |
| • T2 | 3 ± 2, 2;3;5 | 3 ± 2 | 3 ± 2 | - | 0.799 ** |
| • P-value T-test | - | <0.001 | <0.001 |
References
- Brocks, Y.; Zittermann, A.; Grisse, D.; Schmid-Ott, G.; Stock-Gießendanner, S.; Schulz, U.; Brakhage, J.; Benkler, A.; Gummert, J.; Tigges-Limmer, K. Adherence of Heart Transplant Recipients to Prescribed Medication and Recommended Lifestyle Habits. Prog. Transpl. 2017, 27, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Korb-Savoldelli, V.; Sabatier, B.; Gillaizeau, F.; Guillemain, R.; Prognon, P.; Bégué, D.; Durieux, P. Non-adherence with drug treatment after heart or lung transplantation in adults: A systematic review. Patient Educ. Couns. 2010, 81, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Dew, M.A.; DiMartini, A.F.; Dabbs, A.D.V.; Myaskovsky, L.; Steel, J.; Unruh, M.; Switzer, G.E.; Zomak, R.; Kormos, R.L.; Greenhouse, J.B. Rates and Risk Factors for Nonadherence to the Medical Regimen After Adult Solid Organ Transplantation. Transplantation 2007, 83, 858–873. [Google Scholar] [CrossRef] [PubMed]
- Hansen, R.; Seifeldin, R.; Noe, L. Medication Adherence in Chronic Disease: Issues in Posttransplant Immunosuppression. Transpl. Proc. 2007, 39, 1287–1300. [Google Scholar] [CrossRef]
- Dobbels, F.; De Geest, S.; Van Cleemput, J.; Droogne, W.; Vanhaecke, J. Effect of late medication non-compliance on outcome after heart transplantation: A 5-year follow-up. J. Heart Lung Transpl. 2004, 23, 1245–1251. [Google Scholar] [CrossRef]
- De Geest, S.; Dobbels, F.; Fluri, C.; Paris, W.; Troosters, T. Adherence to the therapeutic regimen in heart, lung, and heart-lung transplant recipients. J. Cardiovasc. Nurs. 2005, 20 (Suppl. 5), S88–S98. [Google Scholar] [CrossRef]
- De Geest, S.; Abraham, I.; Moons, P.; Vandeputte, M.; Van Cleemput, J.; Evers, G.; Daenen, W.; Vanhaecke, J. Late acute rejection and subclinical noncompliance with cyclosporine therapy in heart transplant recipients. J. Heart Lung Transpl. 1998, 17, 854–863. [Google Scholar]
- Fine, R.N.; Becker, Y.; De Geest, S.; Eisen, H.; Ettenger, R.; Evans, R.; Rudow, D.L.; McKay, D.; Neu, A.; Nevins, T.; et al. Nonadherence Consensus Conference Summary Report. Arab. Archaeol. Epigr. 2008, 9, 35–41. [Google Scholar] [CrossRef]
- Nieuwlaat, R.; Wilczynski, N.; Navarro, T.; Hobson, N.; Jeffery, R.; Keepanasseril, A.; Agoritsas, T.; Mistry, N.; Iorio, A.; Jack, S.; et al. Interventions for enhancing medication adherence. Cochrane Database Syst. Rev. 2014, 11, CD000011. [Google Scholar] [CrossRef]
- Kini, V.; Ho, P.M. Interventions to Improve Medication Adherence A Review. JAMA 2018, 320, 2461–2473. [Google Scholar] [CrossRef]
- Gustavsen, M.T.; Midtvedt, K.; Lønning, K.; Jacobsen, T.; Reisæter, A.V.; De Geest, S.; Andersen, M.H.; Hartmann, A.; Åsberg, A. Evaluation of tools for annual capture of adherence to immunosuppressive medications after renal transplantation—A single-centre open prospective trial. Transpl. Int. 2019, 32, 614–625. [Google Scholar] [CrossRef] [Green Version]
- Sabaté, E.; World Health Organization (WHO). Adherence to Long-Term Therapies: Evidence for Action. WHO Library Cataloguing-in-Publication Data. 2003. Available online: https://www.who.int/chp/knowledge/publications/adherence_full_report.pdf?ua=1 (accessed on 10 October 2020).
- Denhaerynck, K.; Berben, L.; Dobbels, F.; Russell, C.L.; Crespo-Leiro, M.G.; Poncelet, A.J.; De Geest, S.; Cupples, S.; De Simone, P.; Groenewoud, A.; et al. Multilevel factors are associated with immunosuppressant nonadherence in heart transplant recipients: The international BRIGHT study. Am. J. Transpl. 2018, 18, 1447–1460. [Google Scholar] [CrossRef] [Green Version]
- De Bleser, L.; Matteson, M.; Dobbels, F.; Russell, C.; De Geest, S. Interventions to improve medication-adherence after transplantation: A systematic review. Transpl. Int. 2009, 22, 780–797. [Google Scholar] [CrossRef]
- Senft, Y.; Kirsch, M.; Denhaerynck, K.; Dobbels, F.; Helmy, R.; Russell, C.L.; Berben, L.; De Geest, S.; Crespo-Leiro, M.G.; Cupples, S.; et al. Practice patterns to improve pre and post-transplant medication adherence in heart transplant centres: A secondary data analysis of the international BRIGHT study. Eur. J. Cardiovasc. Nurs. 2018, 17, 356–367. [Google Scholar] [CrossRef]
- Lu, C.Y.; Ross-Degnan, D.; Soumerai, S.B.; Pearson, S.-A. Interventions designed to improve the quality and efficiency of medication use in managed care: A critical review of the literature—2001–2007. BMC Health Serv. Res. 2008, 8, 75. [Google Scholar] [CrossRef] [Green Version]
- Damery, S.; Flanagan, S.; Combes, G. The effectiveness of interventions to achieve co-ordinated multidisciplinary care and reduce hospital use for people with chronic diseases: Study protocol for a systematic review of reviews. Syst. Rev. 2015, 4, 64. [Google Scholar] [CrossRef] [Green Version]
- Damery, S.; Flanagan, S.; Combes, G. Does integrated care reduce hospital activity for patients with chronic diseases? An umbrella review of systematic reviews. BMJ Open 2016, 6, e011952. [Google Scholar] [CrossRef] [Green Version]
- Vallespin, B.; Cornet, J.; Kotzeva, A. Ensuring Evidence-Based Safe and Effective mHealth Applications. Stud. Health Technol. Inform. 2016, 222, 248–261. [Google Scholar] [CrossRef]
- Basch, E.; Deal, A.M.; Kris, M.G.; Scher, H.I.; Hudis, C.A.; Sabbatini, P.; Rogak, L.; Bennett, A.V.; Dueck, A.C.; Atkinson, T.M.; et al. Symptom Monitoring with Patient-Reported Outcomes During Routine Cancer Treatment: A Randomized Controlled Trial. J. Clin. Oncol. 2016, 34, 557–565. [Google Scholar] [CrossRef]
- Park, L.G.; Howie-Esquivel, J.; Dracup, K. A quantitative systematic review of the efficacy of mobile phone interventions to improve medication adherence. J. Adv. Nurs. 2014, 70, 1932–1953. [Google Scholar] [CrossRef]
- Piette, J.D.; List, J.; Rana, G.K.; Townsend, W.; Striplin, D.; Heisler, M. Mobile health devices as tools for worldwide cardiovascular risk reduction and disease management. Circulation 2015, 132, 2012–2027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Pérez, B.; De La Torre-Díez, I.; López-Coronado, M.; Herreros-González, J. Mobile Apps in Cardiology: Review. J. Med. Internet 2013, 15, 15–151. [Google Scholar] [CrossRef] [PubMed]
- Fleming, J.N.; Taber, D.J.; McElligott, J.; McGillicuddy, J.W.; Treiber, F. Mobile Health in Solid Organ Transplant: The Time Is Now. Am. J. Transplant. 2017, 17, 2263–2276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; E Wood, C.; Johnston, M.; Abraham, C.; Francis, J.J.; Hardeman, W. Behaviour change techniques: The development and evaluation of a taxonomic method for reporting and describing behaviour change interventions (a suite of five studies involving consensus methods, randomised controlled trials and analysis of qualitative data). Health Technol. Assess. 2015, 19, 1–187. [Google Scholar] [CrossRef] [Green Version]
- Webb, T.L.; Joseph, J.; Yardley, L.; Michie, S. Using the Internet to Promote Health Behavior Change: A Systematic Review and Meta-analysis of the Impact of Theoretical Basis, Use of Behavior Change Techniques, and Mode of Delivery on Efficacy. J. Med. Internet Res. 2010, 12, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Ritterband, L.M.; Andersson, G.; Christensen, H.M.; Carlbring, P.; Cuijpers, P.; Potts, H.; Van Der Slikke, J.H. Directions for the International Society for Research on Internet Interventions (ISRII). J. Med. Internet Res. 2006, 8, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G.; CONSORT-EHEALTH Group. CONSORT-EHEALTH: Improving and standardizing evaluation reports of Web-based and mobile health interventions. J. Med. Internet Res. 2011, 13, e126. [Google Scholar] [CrossRef] [PubMed]
- Dew, M.A. Behavioral Factors in Heart Transplantation: Quality of Life and Medical Compliance. J. Appl. Biobehav. Res. 1994, 2, 28–54. [Google Scholar] [CrossRef]
- Harper, R.G.; Chacko, R.C.; Kotik-Harper, D.; Young, J.; Gotto, J. Self-Report Evaluation of Health Behavior, Stress Vulnerability, and Medical Outcome of Heart Transplant Recipients. Psychosom. Med. 1998, 60, 563–569. [Google Scholar] [CrossRef]
- Vitinius, F.; Ziemke, M.; Albert, W. Adherence with immunosuppression in heart transplant recipients. Curr. Opin. Organ. Transpl. 2015, 20, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Gomis-Pastor, M.; Mangues, M.A.; Pellicer, V. mHeart—mHealthCare Platform Adapted to the Heart Transplant Population—Technical Specifications and Software Source Code Internet. Mendeley Data 2019. Available online: https://data.mendeley.com/datasets/yf2dgcfmmh/4 (accessed on 10 October 2020). [CrossRef]
- Gomis-Pastor, M.; Mirabet, S.; Roig, E.; Lopez, L.; Brossa, V.; Galvez-Tugas, E.; Rodriguez-Murphy, E.; Feliu, A.; Ontiveros, G.; Garcia-Cuyàs, F.; et al. Interdisciplinary Mobile Health Model to Improve Clinical Care after Heart Transplantation: Implementation Strategy Study. JMIR Cardio. 2020, 4, e19065. [Google Scholar] [CrossRef]
- Gomis-Pastor, M.; Roig, E.; Mirabet, S.; De Pourcq, J.T.; Conejo, I.; Feliu, A.; Brossa, V.; Lopez, L.; Ferrero-Gregori, A.; Barata, A.; et al. A Mobile App (mHeart) to Detect Medication Nonadherence in the Heart Transplant Population: Validation Study. JMIR mHealth uHealth 2020, 8, e15957. [Google Scholar] [CrossRef]
- Conn, V.S.; Enriquez, M.; Ruppar, T.M.; Chan, K.C. Meta-analyses of Theory Use in Medication Adherence Intervention Research. Am. J. Health Behav. 2016, 40, 155–171. [Google Scholar] [CrossRef] [Green Version]
- Salvo, M.C.; Cannon-Breland, M.L. Motivational interviewing for medication adherence. J. Am. Pharm. Assoc. 2015, 55, e354–e363. [Google Scholar] [CrossRef]
- Miller, W.R.; Rose, G.S. Toward a Theory of Motivational Interviewing MI was not founded on theory. Am. Psychol. 2009, 64, 527–537. [Google Scholar] [CrossRef]
- Clinapsis: Clinical Epidemiology and Healthcare Services Internet. Available online: http://www.clinapsis.com/index.php/auth/login/?l=en (accessed on 5 July 2019).
- Dobbels, F.; De Bleser, L.; Berben, L.; Kristanto, P.; Dupont, L.; Nevens, F.; Vanhaecke, J.; Verleden, G.; De Geest, S. Efficacy of a medication adherence enhancing intervention in transplantation: The MAESTRO-Tx trial. J. Hearth Lung Transpl. 2017, 36, 499–508. [Google Scholar] [CrossRef] [Green Version]
- De Geest, S.; Zullig, L.L.; Dunbar-Jacob, J.; Helmy, R.; Hughes, D.A.; Wilson, I.B.; Vrijens, B. ESPACOMP medication adherence reporting guideline (EMERGE). Ann. Internet Med. 2018, 169, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Suárez, F.O.; Plumed, J.S.; Valentín, M.P.; Palomo, P.P.; Cepeda, M.M.; Aguiar, D.L.; Grupo de Estudio Vatren. Validation on the simplified medication adherence questionnaire (SMAQ) in renal transplant patients on tacrolimus. Nefrologia 2011, 31, 690–696. [Google Scholar]
- de Oliveira Marsicano, E.; da Silva Fernandes, N.; Colugnati, F.; dos Santos Grincenkov, F.R.; da Silva Fernandes, N.M.; De Geest, S.; Sanders-Pinheiro, H. Transcultural adaptation and initial validation of Brazilian-Portuguese version of the Basel assessment of adherence to immunosuppressive medications scale (BAASIS) in kidney transplants. BMC Nephrol. 2013, 14, 108. [Google Scholar]
- Orozco-Beltrán, D.; Gil-Guillén, C.C.V. Mejorar la adherencia: Una de las acciones más eficientes para aumentar la supervivencia de los pacientes en prevención secundaria. Revista Española Cardiología Suplementos 2018, 15, 12–18. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Dipchand, A.; Starling, R.; Anderson, A.; Chan, M.; Desai, S.; Fedson, S.; Fisher, P.; Gonzales-Stawinski, G.; Martinelli, L.; et al. The International Society of Heart and Lung Transplantation Guidelines for the care of heart transplant recipients. J. Hearth Lung Transpl. 2010, 29, 914–956. [Google Scholar] [CrossRef]
- McGillicuddy, J.W.; Weiland, A.K.; Frenzel, R.M.; Mueller, M.; Brunner-Jackson, B.M.; Taber, D.J.; Baliga, P.K.; Treiber, F.A. Patient Attitudes Toward Mobile Phone-Based Health Monitoring: Questionnaire Study Among Kidney Transplant Recipients. J. Med. Internet Res. 2013, 15, e6. [Google Scholar] [CrossRef]
- Michie, S.; Prestwich, A. Are interventions theory-based? Development of a theory coding scheme. Health Psychol. 2010, 29, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Pérez, A.B.M.; Suárez, A.L.; Rodríguez, J.R.; Márquez, J.S.; Gallé, E.L. Medication adherence in patients who undergo cardiac transplantation. Transplant. Proc. 2013, 45, 3662–3664. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychol. Rev. 2015, 9, 323–344. [Google Scholar] [CrossRef] [PubMed]
- Lancaster, K.; Abuzour, A.; Khaira, M.; Mathers, A.; Chan, A.; Bui, V.; Lok, A.; Thabane, L.; Dolovich, L. The Use and Effects of Electronic Health Tools for Patient Self-Monitoring and Reporting of Outcomes Following Medication Use: Systematic Review. J. Med. Internet Res. 2018, 20, e294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lycett, H.J.; Raebel, E.M.; Wildman, E.K.; Guitart, J.; Kenny, T.; Sherlock, J.-P.; Cooper, V. Theory-Based Digital Interventions to Improve Asthma Self-Management Outcomes: Systematic Review. J. Med. Internet Res. 2018, 20, e293. [Google Scholar] [CrossRef] [Green Version]
- The CAHPS Ambulatory Care Improvement Guide: Practical Strategies for Improving Patient Experience. Content Last Reviewed February 2020. Agency for Healthcare Research and Quality, Rockville, MD. Available online: https://www.ahrq.gov/cahps/quality-improvement/improvement-guide/improvement-guide.html (accessed on 12 April 2021).
- Youngson, R.; Blennerhassett, M. Humanising healthcare. BMJ 2016, 355, 1–2. [Google Scholar] [CrossRef]
- Gomis-Pastor, M.; Mingell, E.R.; Perez, S.M.; Loidi, V.B.; Lopez, L.L.; Bassons, A.D.; Pousa, A.A.; Ribera, A.F.; Ferrero-Gregori, A.; Perich, L.G.; et al. Multimorbidity and medication complexity: New challenges in heart transplantation. Clin. Transpl.. 2019, 33, e13682. [Google Scholar] [CrossRef]
- Pantuzza, L.L.; Ceccato, M.D.G.B.; Silveira, M.R.; Junqueira, L.M.R.; Reis, A.M.M. Association between medication regimen complexity and pharmacotherapy adherence: A systematic review. Eur. J. Clin. Pharmacol. 2017, 73, 1475–1489. [Google Scholar] [CrossRef]
- Kuo, S.Z.; Haftek, M.; Lai, J.C. Factors Associated with Medication Non-adherence in Patients with End-Stage Liver Disease. Dig. Dis. Sci. 2017, 62, 543–549. [Google Scholar] [CrossRef] [Green Version]
- Ghimire, S.; Peterson, G.M.; Castelino, R.L.; Jose, M.D.; Zaidi, S.T.R. Medication Regimen Complexity and Adherence in Haemodialysis Patients: An Exploratory Study. Am. J. Nephrol. 2016, 43, 318–324. [Google Scholar] [CrossRef]
- Kelders, S.M.; Kok, R.N.; Ossebaard, H.C.; Van Gemert-Pijnen, J.E. Persuasive System Design Does Matter: A Systematic Review of Adherence to Web-based Interventions. J. Med. Internet Res. 2012, 14, 1–24. [Google Scholar] [CrossRef]
- Morton, K.; Beauchamp, M.; Prothero, A.; Joyce, L.; Saunders, L.; Spencer-Bowdage, S.; Dancy, B.; Pedlar, C. The effectiveness of motivational interviewing for health behaviour change in primary care settings: A systematic review. Health Psychol. Rev. 2014, 9, 205–223. [Google Scholar] [CrossRef]
- Alexander, E.; Butler, C.D.; Darr, A.; Jenkins, M.T.; Long, R.D.; Shipman, C.J.; Stratton, T.P. ASHP Statement on Telepharmacy. Am. J. Health Pharm. 2017, 74, e236–e241. [Google Scholar] [CrossRef]
- Strand, M.A.; Tellers, J.; Patterson, A.; Ross, A.; Palombi, L. The achievement of public health services in pharmacy practice: A literature review. Res. Soc. Adm. Pharm. 2016, 12, 247–256. [Google Scholar] [CrossRef]
- De Bleser, L.; Dobbels, F.; Berben, L.; Vanhaecke, J.; Verleden, G.; Nevens, F.; De Geest, S. The spectrum of nonadherence with medication in heart, liver, and lung tranplant patients assessed in various ways. Transpl. Int. 2011, 24, 882–891. [Google Scholar] [CrossRef]
- Dobbels, F.; Berben, L.; De Geest, S.; Drent, G.; Lennerling, A.; Whittaker, C.; Kugler, C. The Psychometric Properties and Practicability of Self-Report Instruments to Identify Medication Nonadherence in Adult Transplant Patients: A Systematic Review. Transplantation 2010, 90, 205–219. [Google Scholar] [CrossRef]
- Schäfer-Keller, P.; Steiger, J.; Bock, A.; Denhaerynck, K.; De Geest, S. Diagnostic Accuracy of Measurement Methods to Assess Non-Adherence to Immunosuppressive Drugs in Kidney Transplant Recipients. Am. J. Transplant. 2008, 8, 616–626. [Google Scholar] [CrossRef]





| Variables | Total HTx Patients (N = 134) | |
|---|---|---|
| Demographic information | ||
| Recipient gender (male), N (%) | 92 (69) | |
| Body mass index (kg/m2), M ± SD | 27 ± 5 | |
| Recipient age at the time of the study (years), M ± SD | 57 ± 14 | |
| Patients > 75 years old, N (%) | 5 (4) | |
| Educational attainment, N (%) | No schooling | 15 (11) |
| Middle school graduate | 58 (43) | |
| High school graduate | 25 (19) | |
| University graduate | 36 (27) | |
| Employment status, N (%) 1 | Disability | 74 (55) |
| Currently employed | 34 (25) | |
| Retired | 19 (14) | |
| No previous employment activity | 7 (5) | |
| Clinical variables, transplant-related (continue inSupplementary File S3) | ||
| Recipient age at HTx (years), M ± SD | 45 ± 16 | |
| Time from HTx (years), M ± SD | 11 ± 7 | |
| Urgent HTx, N (%) | 33 (25) | |
| Heart failure etiology, N (%) | Coronary/ischemic | 35 (26) |
| Cardiomyopathy | 60 (45) | |
| Other | 84 (47) | |
| Re-transplant | 8 (6) | |
| Multimorbidity and use of care resources among HTxR included in the study | ||
| Number of comorbidities Post-HTx, M ± SD 2 | 6 ± 3 | |
| Need or requirement for caregiver, N (%) | 27 (20) | |
| Lives with someone else, N (%) | 114 (88) | |
| Treatment measures | ||
| Immunosuppressive treatment, N (%) | Cyclosporine | 33 (25) |
| Tacrolimus | 98 (73) | |
| Everolimus | 20 (15) | |
| Sirolimus | 3 (2) | |
| Azathioprine | 4 (3) | |
| Mycophenolate mofetil | 71 (53) | |
| Mycophenolate sodium | 29 (22) | |
| Corticosteroids | 114 (85) | |
| Total drugs count, M ± SD | 10 ± 3 | |
| Patients with polypharmacy), N (%) | ≥8 drugs | 100 (75) |
| ≥15 drugs | 9 (7) | |
| Drugs to treat comorbidities, M ± SD | 4 ± 2 | |
| OTC medicines, M ± SD | 2 ± 1 | |
| Complementary therapies, M ± SD | 2 ± 1 | |
| Variables, N (%) | Total HTx Patients (N = 134) | |||
|---|---|---|---|---|
| CG (N = 63) | IG (N = 71) | P-Value | ||
| No need for regular face-to-face in-clinic appointments | Total | 22 (35) | 46 (65) | <0.001 * |
| Discharge from in-clinic visits | 22 (35) | 19 (27) | - | |
| Discharge with intensive mHeart reminders to track medication adherence | 0 (0) | 18 (25) | - | |
| Discharge with mHeart reminders to follow lifestyle habits affecting medication regimens | 0 (0) | 9 (13) | - | |
| Need for regular face-to-face in-clinic appointments | Total | 41 (65) | 25 (35) | <0.001 * |
| Intensive in-clinic follow-up every 6 months | 7 (11) | 3 (4) | - | |
| Annual in-clinic follow-up to reinforce medication adherence | 28 (44) | 14 (20) | - | |
| Annual in-clinic follow-up for other medication-related issues | 6 (10) | 8 (11) | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomis-Pastor, M.; Mirabet Perez, S.; Roig Minguell, E.; Brossa Loidi, V.; Lopez Lopez, L.; Ros Abarca, S.; Galvez Tugas, E.; Mas-Malagarriga, N.; Mangues Bafalluy, M.A. Mobile Health to Improve Adherence and Patient Experience in Heart Transplantation Recipients: The mHeart Trial. Healthcare 2021, 9, 463. https://doi.org/10.3390/healthcare9040463
Gomis-Pastor M, Mirabet Perez S, Roig Minguell E, Brossa Loidi V, Lopez Lopez L, Ros Abarca S, Galvez Tugas E, Mas-Malagarriga N, Mangues Bafalluy MA. Mobile Health to Improve Adherence and Patient Experience in Heart Transplantation Recipients: The mHeart Trial. Healthcare. 2021; 9(4):463. https://doi.org/10.3390/healthcare9040463
Chicago/Turabian StyleGomis-Pastor, Mar, Sonia Mirabet Perez, Eulalia Roig Minguell, Vicenç Brossa Loidi, Laura Lopez Lopez, Sandra Ros Abarca, Elisabeth Galvez Tugas, Núria Mas-Malagarriga, and Mª Antonia Mangues Bafalluy. 2021. "Mobile Health to Improve Adherence and Patient Experience in Heart Transplantation Recipients: The mHeart Trial" Healthcare 9, no. 4: 463. https://doi.org/10.3390/healthcare9040463
APA StyleGomis-Pastor, M., Mirabet Perez, S., Roig Minguell, E., Brossa Loidi, V., Lopez Lopez, L., Ros Abarca, S., Galvez Tugas, E., Mas-Malagarriga, N., & Mangues Bafalluy, M. A. (2021). Mobile Health to Improve Adherence and Patient Experience in Heart Transplantation Recipients: The mHeart Trial. Healthcare, 9(4), 463. https://doi.org/10.3390/healthcare9040463