
Medication Handling and Storage among Pilgrims during the Hajj Mass Gathering


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting, Design and Population
2.2. Data Collection Tool and Scoring System
2.3. Statistical Analysis
2.4. Ethics and Confidentiality
3. Results
3.1. Characteristics of the Study Population
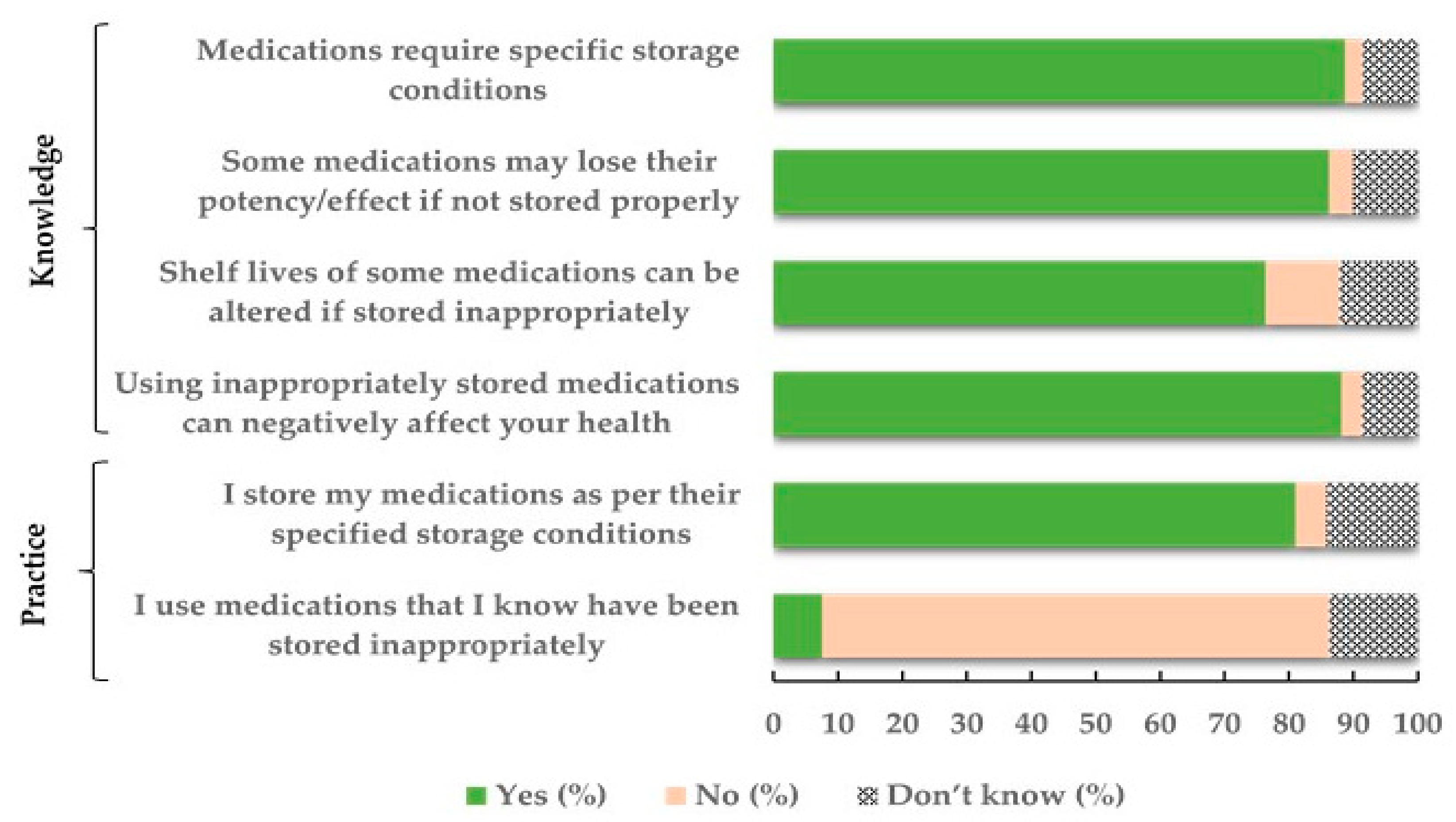
3.2. Medication Storage Knowledge and Practice among Hajj Pilgrims
3.3. Medication Sources and Handling during the Hajj
3.4. Medication Storage during Hajj
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stanisz, B.; Regulska, K. Kinetics of degradation of imidapril hydrochloride in finished dosage formulations. Acta Pol. Pharm. Drug Res. 2013, 70, 737–742. [Google Scholar]
- De Winter, S.; Vanbrabant, P.; Vi, N.T.T.; Deng, X.; Spriet, I.; Van Schepdael, A.; Gillet, J.-B. Impact of temperature exposure on stability of drugs in a real-world out-of-hospital setting. Ann. Emerg. Med. 2013, 62, 380–387.e1. [Google Scholar] [CrossRef]
- Kupper, T.E.; Schraut, B.; Rieke, B.; Hemmerling, A.V.; Schoffl, V.; Steffgen, J. Drugs and drug administration in extreme environments. J. Travel Med. 2006, 13, 35–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armenian, P.; Campagne, D.; Stroh, G.; Tallman, C.I.; Zeng, W.Z.D.; Lin, T.; Gerona, R.R. Hot and cold drugs: National park service medication stability at the extremes of temperature. Prehospital Emerg. Care 2017, 21, 378–438. [Google Scholar] [CrossRef] [PubMed]
- Yezli, S.; Mushi, A.; Almuzaini, Y.; Balkhi, B.; Yassin, Y.; Khan, A. Prevalence of diabetes and hypertension among Hajj pilgrims: A systematic review. Int. J. Env. Res. Public Health 2021, 18, 1155. [Google Scholar] [CrossRef]
- Alqahtani, A.S.; Althimiri, N.A.; BinDhim, N.F. Saudi Hajj pilgrims’ preparation and uptake of health preventive measures during Hajj 2017. J. Infect. Public Heal. 2019, 12, 772–776. [Google Scholar] [CrossRef] [PubMed]
- Yezli, S.; Yassin, Y.; Mushi, A.; Maashi, F.; Aljabri, N.; Mohamed, G.; Bieh, K.; Awam, A.; Alotaibi, B. Knowledge, attitude and practice (KAP) survey regarding antibiotic use among pilgrims attending the 2015 Hajj mass gathering. Travel Med. Infect. Dis. 2019, 28, 52–58. [Google Scholar] [CrossRef]
- Khan, S.; Alghafari, Y. Temperature, precipitation and relative humidity fluctuation of Makkah Al Mukarramah, kingdom of Saudi Arabia (1985–2016). Trans. Mach. Learn. Artif. Intell. 2018, 6, 42. [Google Scholar]
- Khan, E.A.; Shambour, M.K.Y. An analytical study of mobile applications for Hajj and Umrah services. Appl. Comput. Inform. 2018, 14, 37–47. [Google Scholar] [CrossRef]
- Hailat, M.; Al-Shdefat, R.I.; Muflih, S.M.; Ahmed, N.; Attarabeen, O.; Alkhateeb, F.M.; Al Meanazel, O.; Gassar, E.S. Public knowledge about dosage forms, routes of drug administration and medication proper storage conditions in Riyadh District, Saudi Arabia. J. Pharm. Heal. Serv. Res. 2020, 11, 205–213. [Google Scholar] [CrossRef]
- Martins, R.R.; Farias, A.D.; Oliveira, Y.M.D.C.; Diniz, R.D.S.; Oliveira, A.G. Prevalence and risk factors of inadequate medicine home storage: A community-based study. Rev. Saúde Pública 2017, 51, 95. [Google Scholar] [CrossRef]
- Wieczorkiewicz, S.M.; Kassamali, Z.; Danziger, L.H. Behind Closed Doors: Medication Storage and Disposal in the Home. Ann. Pharm. 2013, 47, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Foroutan, B.; Foroutan, R. Household storage of medicines and self-medication practices in south-east Islamic Republic of Iran. East Mediterr. Heal. J. 2014, 20, 547–553. [Google Scholar] [CrossRef]
- Haseeb, A.; Faidah, H.S.; Elrajjal, M.E. Pilgrims attitude and believes towards medications use during Hajj 2013. In Proceedings of the 18th Scientific Forum for the Research of Hajj, Umrah and Madinah Visit—Scientific Bulletin for 1439AH (2018), Mecca, Saudi Arabia, 1–2 May 2018. [Google Scholar]
- Daughton, C.G.; Ruhoy, I.S. Green pharmacy and pharmEcovigilance: Prescribing and the planet. Expert Rev. Clin. Pharmacol. 2011, 4, 211–232. [Google Scholar]
- Matalová, P.; Poruba, M.; Wawruch, M.; Ondra, P.; Urbánek, K. Acute Medication Poisoning Causing Hospital Admissions in Childhood: A 3-Year Prospective Observational Single-Center Study. Physiol. Res. 2019, 68, S31–S38. [Google Scholar] [CrossRef] [PubMed]
- Alotaibi, B.; Yassin, Y.; Mushi, A.; Maashi, F.; Thomas, A.; Mohamed, G.; Hassan, A.; Yezli, S. Tuberculosis knowledge, attitude and practice among healthcare workers during the 2016 Hajj. PLoS ONE 2019, 14, e0210913. [Google Scholar] [CrossRef] [PubMed]
- Mimesh, S.A.; Al-Khenaizan, S.; Memish, Z.A. Dermatologic challenges of pilgrimage. Clin. Dermatol. 2008, 26, 52–61. [Google Scholar] [CrossRef]
- Hatchett, R. The medicines refrigerator and the importance of the cold chain in the safe storage of medicines. Nurs. Stand. 2017, 32, 53–63. [Google Scholar] [CrossRef]
- Frimpter, G.W.; Timpanelli, A.E.; Eisenmenger Wj Stein, H.S.; Ehrlich, L.I. Reversible "Faconi syndrome" caused by degraded tetracycline. JAMA 1963, 184, 111–113. [Google Scholar] [CrossRef]
- BaDawood, A.O.; Bossei, A.A.; AlSabhani, M.F.; AlAhmari, S.M.; Shata, M.T.; Hamam, A.F. The burden on EDs during Hajj due to pilgrim noncompliance with treatment for chronic conditions. SJEMed 2020, 1, 103–109. [Google Scholar] [CrossRef]
- Azeem, M.; Tashani, M.; Barasheed, O.; Heron, L.; A Hill-Cawthorne, G.; Haworth, E.; E Dwyer, D.; Rashid, H.; Booy, R. Knowledge, Attitude and Practice (KAP) Survey Concerning Antimicrobial Use among Australian Hajj Pilgrims. Infect. Disord. Drug Targets 2014, 14, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Netere, A.K.; Ashete, E.; Gebreyohannes, E.A.; Belachew, S.A. Evaluations of knowledge, skills and practices of insulin storage and injection handling techniques of diabetic patients in Ethiopian primary hospitals. BMC Public Health 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Das Choudhury, S.; Das, S.K.; Hazra, A. Survey of knowledge-attitude-practice concerning insulin use in adult diabetic patients in eastern India. Indian J. Pharm. 2014, 46, 425–429. [Google Scholar]
- Marks, J.R.; Schectman, J.M.; Groninger, H.; Plews-Ogan, M.L. The association of health literacy and socio-demographic factors with medication knowledge. Patient Educ. Couns. 2010, 78, 372–376. [Google Scholar] [CrossRef]
- Rolls, C.A.; Obamiro, K.O.; Chalmers, L.; Bereznicki, L.R.E. The relationship between knowledge, health literacy, and adherence among patients taking oral anticoagulants for stroke thromboprophylaxis in atrial fibrillation. Cardiovasc. Ther. 2017, 35, e12304. [Google Scholar] [CrossRef]
- Agarwal, M.; Williams, J.; Tavoulareas, D.; Studnek, J.R. A Brief Educational Intervention Improves Medication Safety Knowledge in Grandparents of Young Children. AIMS Public Health 2015, 2, 44–55. [Google Scholar] [CrossRef]
- de la Cruz, M.; Reddy, A.; Balankari, V.; Epner, M.; Frisbee-Hume, S.; Wu, J.; Liu, D.; Yennuraialingam, S.; Cantu, H.; Williams, J.; et al. The impact of an educational program on patient practices for safe use, storage, and disposal of opioids at a comprehensive cancer center. Oncologist 2017, 22, 115–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alomi, Y.A.; Khayat, N.A.Y.; Baljoon, M.J.; Bamagaus, Y.A.; Jumah, H.M.A. National Survey of Hospital Medication Safety Practice during Mass Gathering (Hajj-2016) in Makkah, Saudi Arabia: Medication Preparation and Dispensing. J. Pharm. Pr. Community Med. 2017, 3, s36–s42. [Google Scholar] [CrossRef]
- A Bawazir, S.; Abou-Auda, H.S.; A Gubara, O.; I Al-Khamis, K.; Al-Yamani, M.J. Public Attitude toward Drug Technical Package Inserts in Saudi Arabia. J. Pharm. Technol. 2003, 19, 209–218. [Google Scholar] [CrossRef]
- Davis, T.C.; Wolf, M.S.; Bass, P.F., 3rd; Thompson, J.A.; Tilson, H.H.; Neuberger, M.; Parker, R.M. Literacy and misunderstanding prescription drug labels. Ann. Intern. Med. 2006, 145, 887–894. [Google Scholar] [CrossRef]
- Wolf, M.S.; Davis, T.C.; Tilson, H.H.; Bass, P.F., 3rd; Parker, R.M. Misunderstanding of prescription drug warning labels among patients with low literacy. Am. J. Health Syst. Pharm. 2006, 63, 1048–1055. [Google Scholar] [CrossRef] [PubMed]
- Mullen, R.J.; Duhig, J.; Russell, A.; Scarazzini, L.; Lievano, F.; Wolf, M.S. Best-practices for the design and development of prescription medication information: A systematic review. Patient Educ. Couns. 2018, 101, 1351–1367. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.E.; Leong, D. What Should I Know About Medication Storage and Disposal? JAMA Intern. Med. 2020, 180, 1560. [Google Scholar] [CrossRef] [PubMed]
- Gidey, M.T.; Birhanu, A.H.; Tsadik, A.G.; Welie, A.G.; Assefa, B.T. Knowledge, Attitude, and Practice of Unused and Expired Medication Disposal among Patients Visiting Ayder Comprehensive Specialized Hospital. BioMed Res. Int. 2020, 2020, 1–7. [Google Scholar] [CrossRef]
- Biçer, E.K. An Important Environmental Risk from Patients with Diabetes using Insulin: Disposal of Medical Waste. Curr. Res. Diabetes Obes. J. 2018, 7, 1–2. [Google Scholar] [CrossRef]
- Manjunath, K.; Moray, K.V.; Shalini, A.M.; Pricilla, S.R.A.; John, S.M.; Prasad, J.H. The insulin sharps disposal study: Evaluation of a structured patient education initiative in an urban community health centre in India. J. Fam. Med. Prim. Care 2020, 9, 6164–6170. [Google Scholar] [CrossRef]
- Bahendeka, S.; Kaushik, R.; Swai, A.B.; Otieno, F.; Bajaj, S.; Kalra, S.; Bavuma, C.M.; Karigire, C. EADSG Guidelines: Insulin Storage and Optimisation of Injection Technique in Diabetes Management. Diabetes Ther. 2019, 10, 341–366. [Google Scholar] [CrossRef] [Green Version]
- Alkatheri, A.M.; Albekairy, A.M. Does the patients′ educational level and previous counseling affect their medication knowledge? Ann. Thorac. Med. 2013, 8, 105–108. [Google Scholar] [CrossRef]
- Lee, S.; Khare, M.M.; Olson, H.R.; Chen, A.M.; Law, A.V. The TEACH trial: Tailored education to assist label comprehension and health literacy. Res. Soc. Adm. Pharm. 2018, 14, 839–845. [Google Scholar] [CrossRef]


{kind=link}
| Variable | N | % |
|---|---|---|
| Total participants | 1221 | |
| Gender | ||
| Male | 768 | 63.3 |
| Female | 445 | 36.7 |
| Age (Years) | ||
| Mean, SD (range) | 50.8, 12.5 (18–98) | |
| <40 | 221 | 8.3 |
| 40–59 | 666 | 55.2 |
| ≥60 | 320 | 26.5 |
| Nationality | ||
| Middle East and North Africa * | 431 | 35.8 |
| South Asia | 316 | 26.2 |
| Sub-Saharan Africa | 230 | 19.2 |
| Southeast Asia | 211 | 17.5 |
| Other ** | 16 | 1.3 |
| Literacy | ||
| Yes | 987 | 90.2 |
| No | 107 | 9.8 |
| Educational level | ||
| Universe/higher education | 538 | 50.4 |
| Secondary education | 330 | 28.5 |
| Primary education | 138 | 11.9 |
| No formal education | 105 | 9.1 |
| Underlying Health conditions | ||
| No | 715 | 62.4 |
| Yes | 430 | 37.6 |
| Diabetes mellitus | 277 | 24.2 |
| Hypertension | 239 | 20.9 |
| Cardiovascular disease | 34 | 3.0 |
| Chronic kidney disease | 5 | 0.4 |
| Chronic lung disease | 14 | 1.2 |
| Chronic liver disease | 4 | 0.3 |
| Immunosuppressive illness | 4 | 0.3 |
| Cancer | 5 | 0.4 |
| Variable | N | OR | 95% CI | p-Value | aOR | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|
| Gender | |||||||
| Female | 445 | 1 | |||||
| Male | 768 | 1.00 | 0.77–1.28 | 0.99 | |||
| Age (years) | |||||||
| <40 | 221 | 1 | 1 | ||||
| 40–59 | 666 | 0.99 | 0.70–1.39 | 0.96 | 1.22 | 0.50–2.95 | 0.65 |
| ≥60 | 320 | 0.54 | 0.37–0.78 | 0.001 | 0.78 | 0.30–2.02 | 0.61 |
| Nationality | |||||||
| Sub-Saharan Africa | 230 | 1 | |||||
| Middle East and North Africa * | 431 | 1.05 | 0.74–1.51 | 0.73 | |||
| Other ** | 16 | 1.15 | 0.36–3.71 | 0.80 | |||
| South Asia | 316 | 0.47 | 0.33–1.03 | 0.08 | |||
| Southeast Asia | 211 | 1.01 | 0.67–1.54 | 0.93 | |||
| Literacy | |||||||
| No | 107 | 1 | |||||
| Yes | 987 | 0.98 | 0.64–1.51 | 0.96 | |||
| Educational level | |||||||
| No formal education | 105 | 1 | 1 | ||||
| Primary education | 138 | 6.13 | 3.45–10.97 | <0.0001 | 7.65 | 3.17–18.47 | <0.0001 |
| Secondary education | 330 | 6.14 | 3.69–10.21 | <0.0001 | 5.11 | 2.25–11.59 | <0.0001 |
| Universe/higher education | 583 | 14.03 | 8.51–23.13 | <0.0001 | 24.43 | 10.12–58.98 | <0.0001 |
| Underlying health conditions | |||||||
| No | 715 | 1 | 1 | ||||
| Yes | 430 | 0.75 | 0.58–0.97 | 0.03 | 2.72 | 1.47–5.03 | 0.001 |
| Education on medication storage | |||||||
| No | 112 | 1 | 1 | ||||
| Yes | 383 | 1.94 | 1.26–2.98 | 0.002 | 2.37 | 1.38–4.05 | 0.002 |
| Variable | Category | N | % |
|---|---|---|---|
| Pilgrims using medication during Hajj | 534 | 44.4 | |
| Where did you acquire your medication? | Outside KSA | 457 | 86.4 |
| Inside KSA | 309 | 60.2 | |
| Source of medication in KSA | Pharmacist | 117 | 36.6 |
| Physician | 252 | 78.8 | |
| Family/friend | 8 | 2.5 | |
| Who handles your medication during Hajj? | Myself | 424 | 81.2 |
| Family member | 43 | 8.3 | |
| Medical mission | 94 | 18.0 | |
| Number of medications pilgrims currently using | 1–4 | 472 | 91.6 |
| 5–9 | 37 | 7.2 | |
| ≥10 | 6 | 1.2 | |
| Handling of remaining medication post-Hajj | Take it home | 444 | 83.9 |
| Throw it away | 81 | 15.3 | |
| Other | 6 | 1.1 |
| Medication Storage | Makkah n (%) | Madinah n (%) | Mina n (%) | Arafat n (%) |
|---|---|---|---|---|
| With self | 448 (85.5) | 409 (85.0) | 413 (80.2) | 415 (80.7) |
| With medical mission | 82 (15.6) | 72 (15.0) | 109 (21.2) | 106 (20.6) |
| In shared storage | 12 (2.3) | 8 (1.7) | 5 (1.0) | 4 (0.8) |
| Other | 10 (1.9) | 9 (1.9) | 8 (1.6) | 8 (1.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yezli, S.; Yassin, Y.; Mushi, A.; Balkhi, B.; Stergachis, A.; Khan, A. Medication Handling and Storage among Pilgrims during the Hajj Mass Gathering. Healthcare 2021, 9, 626. https://doi.org/10.3390/healthcare9060626
Yezli S, Yassin Y, Mushi A, Balkhi B, Stergachis A, Khan A. Medication Handling and Storage among Pilgrims during the Hajj Mass Gathering. Healthcare. 2021; 9(6):626. https://doi.org/10.3390/healthcare9060626
Chicago/Turabian StyleYezli, Saber, Yara Yassin, Abdulaziz Mushi, Bander Balkhi, Andy Stergachis, and Anas Khan. 2021. "Medication Handling and Storage among Pilgrims during the Hajj Mass Gathering" Healthcare 9, no. 6: 626. https://doi.org/10.3390/healthcare9060626
APA StyleYezli, S., Yassin, Y., Mushi, A., Balkhi, B., Stergachis, A., & Khan, A. (2021). Medication Handling and Storage among Pilgrims during the Hajj Mass Gathering. Healthcare, 9(6), 626. https://doi.org/10.3390/healthcare9060626