
Masticatory Force in Relation with Age in Subjects with Full Permanent Dentition: A Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Methodology
2.2. Sample Size and Inclusion Criteria
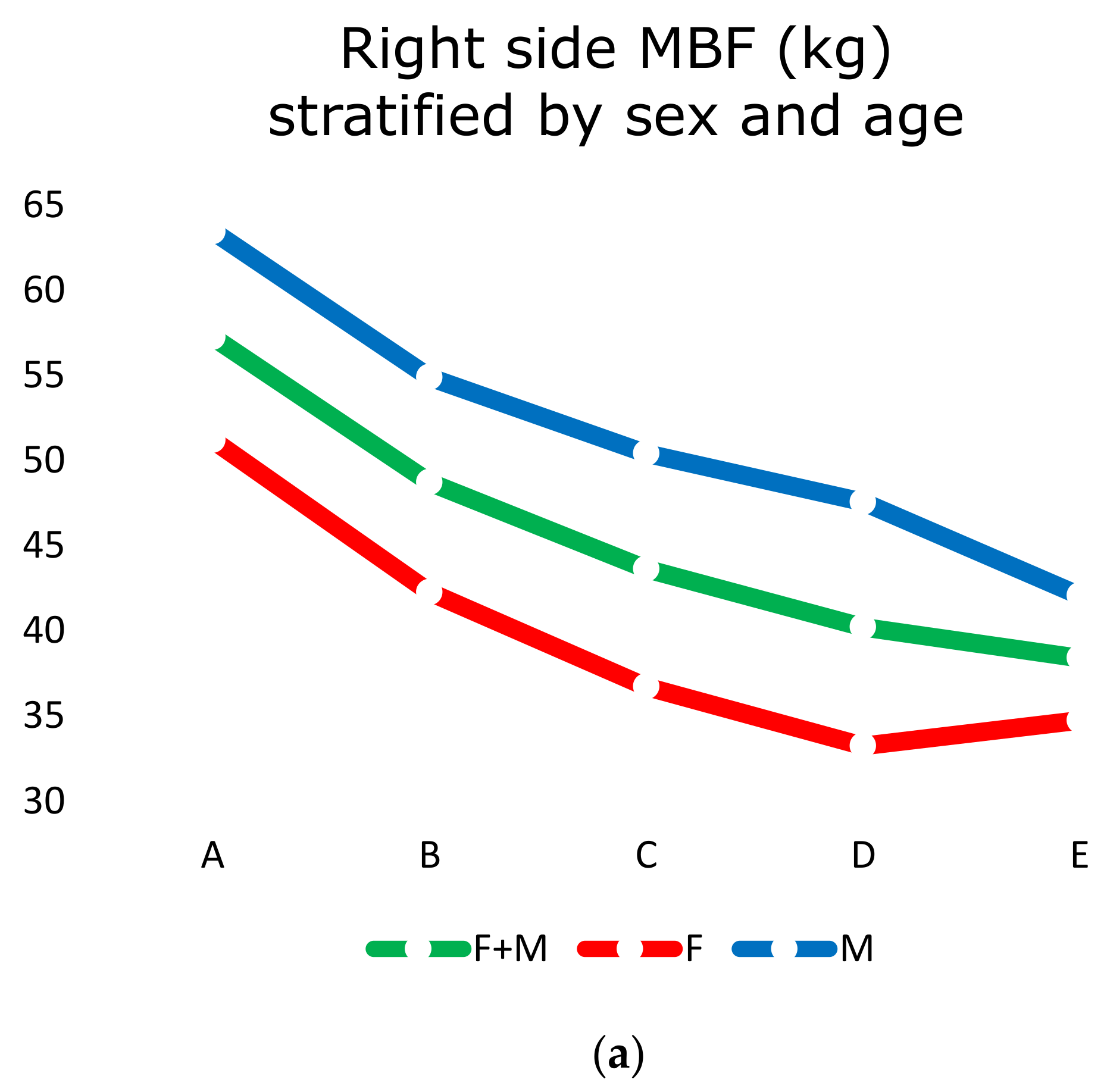
- Group “A” = aging from 20 to 35 years.
- Group “B” = aging from 45 to 59 years.
- Group “C” = aging from 60 to 69 years.
- Group “D” = aging from 70 to 79 years.
- Group “E” = aging more than 79 years.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van der Bilt, A. Assessment of mastication with implications for oral rehabilitation: A review. J. Oral Rehabil. 2011, 38, 754–780. [Google Scholar] [CrossRef]
- Sumonsiri, P.; Thongudomporn, U.; Paphangkorakit, J. Correlation between the median particle size of chewed frankfurter sausage and almonds during masticatory performance test. J. Oral Rehabil. 2018, 45, 512–517. [Google Scholar] [CrossRef]
- Macura-Karbownik, A.; Chladek, G.; Żmudzki, J.; Kasperski, J. Chewing efficiency and occlusal forces in PMMA, acetal and polyamide removable partial denture wearers. Acta Bioeng. Biomech. 2016, 18, 137–144. [Google Scholar] [PubMed]
- Bakke, M.; Holm, B.; Jensen, B.L.; Michler, L.; Möller, E. Unilateral, isometric bite force in 8–68-year-old women and men related to occlusal factors. Eur. J. Oral Sci. 1990, 98, 149–158. [Google Scholar] [CrossRef]
- Kosaka, T.; Kida, M.; Kikui, M.; Hashimoto, S.; Fujii, K.; Yamamoto, M.; Nokubi, T.; Maeda, Y.; Hasegawa, Y.; Kokubo, Y.; et al. Factors Influencing the Changes in Masticatory Performance: The Suita Study. JDR Clin. Transl. Res. 2018, 3, 405–412. [Google Scholar] [CrossRef]
- De Angelis, F.; Basili, S.; Giovanni, F.; Trifan, P.D.; Di Carlo, S.; Manzon, L. Influence of the oral status on cardiovascular diseases in an older Italian population. Int. J. Immunopathol. Pharmacol. 2018, 31, 0394632017751786. [Google Scholar] [CrossRef]
- Schimmel, M.; Katsoulis, J.; Genton, L.; Müller, F. Masticatory function and nutrition in old age. Swiss Dent. J. 2015, 125, 449–454. [Google Scholar]
- Sheiham, A.; Steele, J.G.; Marcenes, W.; Finch, S.; Walls, A.W.G. The relationship between oral health status and Body Mass Index among older people: A national survey of older people in Great Britain. Br. Dent. J. 2002, 192, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.-F.; Chen, C.-C.; Hsu, M.-J.; Huang, N.-J.; Huang, Y.-Z.; Chan, H.-L.; Chang, Y.-J. Age related changes of the motor excitabilities and central and peripheral muscle strength. J. Electromyogr. Kinesiol. 2019, 44, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Motegi, E.; Nomura, M.; Tachiki, C.; Miyazaki, H.; Takeuchi, F.; Takaku, S.; Abe, Y.; Miyatani, M.; Ogai, T.; Fuma, A.; et al. Occlusal force in people in their sixties attending college for elderly. Bull. Tokyo Dent. Coll. 2009, 50, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, P.M. Complete-denture therapy for the geriatric patient. Dent. Clin. N. Am. 1996, 40, 239–254. [Google Scholar]
- Newton, J.; Yemm, R.; Abel, R.; Menhinick, S. Changes in human jaw muscles with age and dental state. Gerodontology 1993, 10, 16–22. [Google Scholar] [CrossRef]
- Kamdem, B.; Seematter-Bagnoud, L.; Botrugno, F.; Santos-Eggimann, B. Relationship between oral health and Fried’s frailty criteria in community-dwelling older persons. BMC Geriatr. 2017, 17, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Sumonsiri, P.; Thongudomporn, U.; Paphangkorakit, J.; Premprabha, T. Assessment of the relationship between masticatory performance, occlusal contact area, chewing time and cycles, and gastric emptying scintigraphy in dentate subjects. J. Oral Rehabil. 2019, 46, 787–791. [Google Scholar] [CrossRef]
- Manzon, L.; Fratto, G.; Poli, O.; Infusino, E. Patient and Clinical Evaluation of Traditional Metal and Polyamide Removable Partial Dentures in an Elderly Cohort. J. Prosthodont. 2019, 28, 868–875. [Google Scholar] [CrossRef]
- Paphangkorakit, J.; Kanpittaya, K.; Pawanja, N.; Pitiphat, W. Effect of chewing rate on meal intake. Eur. J. Oral Sci. 2019, 127, 40–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Y.; Hollis, J.H. Relationship between chewing behavior and body weight status in fully dentate healthy adults. Int. J. Food Sci. Nutr. 2015, 66, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Furuya, J.; Hara, A.; Nomura, T.; Kondo, H. Volitional chewing with a conscious effort alters and facilitates swallowing during feeding sequence. J. Oral Rehabil. 2014, 41, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Hollis, J.H. The effect of mastication on food intake, satiety and body weight. Physiol. Behav. 2018, 193, 242–245. [Google Scholar] [CrossRef]
- Morley, J.E. Decreased Food Intake with Aging. J. Gerontol. Ser. A Boil. Sci. Med Sci. 2001, 56, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Zoltick, E.S.; Sahni, S.; McLean, R.R.; Quach, L.; Casey, V.; Hannan, M. Dietary protein intake and subsequent falls in older men and women: The Framingham study. J. Nutr. Health Aging 2011, 15, 147–152. [Google Scholar] [CrossRef]
- Houston, D.K.; Nicklas, B.J.; Ding, J.; Harris, T.B.; Tylavsky, F.A.; Newman, A.B.; Lee, J.S.; Sahyoun, N.R.; Visser, M.; Kritchevsky, S.B.; et al. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: The Health, Aging, and Body Composition (Health ABC) Study. Am. J. Clin. Nutr. 2008, 87, 150–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volkert, D.; Sieber, C.C. Protein Requirements in the Elderly. Int. J. Vitam. Nutr. Res. 2011, 81, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Rassool, G. Expert report on diet, nutrition and prevention of chronic diseases. J. Adv. Nurs. 2003, 43, 544. [Google Scholar] [CrossRef] [PubMed]
- Hamidi, M.; Boucher, B.A.; Cheung, A.M.; Beyene, J.; Shah, P.S. Fruit and vegetable intake and bone health in women aged 45 years and over: A systematic review. Osteoporos. Int. 2010, 22, 1681–1693. [Google Scholar] [CrossRef]
- Martin, A.; Cherubini, A.; Andres-Lacueva, C.; Paniagua, M.; Joseph, J. Effects of fruits and vegetables on levels of vitamins E and C in the brain and their association with cognitive performance. J. Nutr. Health Aging 2002, 6, 392–404. [Google Scholar] [PubMed]
- Vikstedt, T.; Suominen, M.H.; Joki, A.; Muurinen, S.; Soini, H.; Pitkälä, K.H. Nutritional Status, Energy, Protein, and Micronutrient Intake of Older Service House Residents. J. Am. Med. Dir. Assoc. 2011, 12, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Raynaud-Simon, A.; Aussel, C. Fruit and vegetable intake in older hospitalized patients. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 42–46. [Google Scholar] [CrossRef]
- Donini, L.M.; Poggiogalle, E.; Piredda, M.; Pinto, A.; Barbagallo, M.; Cucinotta, D.; Sergi, G. Anorexia and Eating Patterns in the Elderly. PLoS ONE 2013, 8, e63539. [Google Scholar] [CrossRef] [Green Version]
- Hildebrandt, G.H.; Dominguez, B.; Schork, M.; Loesche, W.J. Functional units, chewing, swallowing, and food avoidance among the elderly. J. Prosthet. Dent. 1997, 77, 588–595. [Google Scholar] [CrossRef]
- Kagawa, R.; Ikebe, K.; Inomata, C.; Okada, T.; Takeshita, H.; Kurushima, Y.; Kibi, M.; Maeda, Y. Effect of dental status and masticatory ability on decreased frequency of fruit and vegetable intake in elderly Japanese subjects. Int. J. Prosthodont. 2012, 25, 68–75. [Google Scholar]
- Kwon, S.H.; Park, H.R.; Lee, Y.M.; Kwon, S.Y.; Kim, O.S.; Kim, H.Y.; Lim, Y.S. Difference in food and nutrient intakes in Korean elderly people according to chewing difficulty: Using data from the Korea National Health and Nutrition Examination Survey 2013 (6th). Nutr. Res. Pract. 2017, 11, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Saberi, B.V.; Nemati, S.; Malekzadeh, M.; Javanmard, A. Assessment of digital panoramic radiography’s diagnostic value in angular bony lesions with 5 mm or deeper pocket depth in mandibular molars. Dent. Res. J. 2017, 14, 32–36. [Google Scholar]
- Müller, H.-P.; Ulbrich, M.; Heinecke, A. Alveolar bone loss in adults as assessed on panoramic radiographs. (II) Multilevel models. Clin. Oral Investig. 2005, 9, 105–110. [Google Scholar] [CrossRef]
- Shinogaya, T.; Sodeyama, A.; Matsumoto, M. Bite force and occlusal load distribution in normal complete dentitions of young adults. Eur. J. Prosthodont. Restor. Dent. 2000, 7, 65–70. [Google Scholar]
- Tatematsu, M.; Mori, T.; Kawaguchi, T.; Takeuchi, K.; Hattori, M.; Morita, I.; Nakagaki, H.; Kato, K.; Murakami, T.; Tuboi, S.; et al. Masticatory performance in 80-year-old individuals. Gerodontology 2004, 21, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Waltimo, A.; Könönen, M. A novel bite force recorder and maximal isometric bite force values for healthy young adults. Eur. J. Oral Sci. 1993, 101, 171–175. [Google Scholar] [CrossRef]
- Eriksson, P.-O.; Thornell, L.-E. Histochemical and morphological muscle-fibre characteristics of the human masseter, the medial pterygoid and the temporal muscles. Arch. Oral Biol. 1983, 28, 781–795. [Google Scholar] [CrossRef]
- Ikebe, K.; Nokubi, T.; Morii, K.; Kashiwagi, J.; Furuya, M. Association of bite force with ageing and occlusal support in older adults. J. Dent. 2005, 33, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, C.H.; Anusavice, K.J.; Young, H.M.; Jones, J.S.; Esquivel-Upshaw, J.F. Maximum clenching force of patients with moderate loss of posterior tooth support: A pilot study. J. Prosthet. Dent. 2002, 88, 498–502. [Google Scholar] [CrossRef]
- Tzankoff, S.P.; Norris, A.H. Effect of muscle mass decrease on age-related BMR changes. J. Appl. Physiol. 1977, 43, 1001–1006. [Google Scholar] [CrossRef]
- Sarkar, A. Oral processing in elderly: Understanding eating capability to drive future food texture modifications. Proc. Nutr. Soc. 2019, 78, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Kohyama, K.; Mioche, L.; Bourdiol, P. Influence of age and dental status on chewing behaviour studied by EMG recordings during consumption of various food samples. Gerodontology 2003, 20, 15–23. [Google Scholar] [CrossRef]
- Eerikäinen, E.; Könönen, M. Forces required by complete dentures for penetrating food in simulated function. J. Oral Rehabil. 1987, 14, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, C.H.; Mahan, P.E.; Lundeen, H.C.; Brehnan, K.; Walsh, E.K.; Sinkewiz, S.L.; Ginsberg, S.B. Occlusal forces during chewing—Influences of biting strength and food consistency. J. Prosthet. Dent. 1981, 46, 561–567. [Google Scholar] [CrossRef]
- Manzon, L.; Vozza, I.; Poli, O. Bite Force in Elderly with Full Natural Dentition and Different Rehabilitation Prosthesis. Int. J. Environ. Res. Public Health 2021, 18, 1424. [Google Scholar] [CrossRef] [PubMed]
- Fontijn-Tekamp, F.A.; Slagter, A.P.; Van Der Bilt, A.; Van’T Hof, M.A.; Witter, D.J.; Kalk, W.; Jansen, J.A. Biting and chewing in overdentures, full dentures, and natural dentitions. J. Dent. Res. 2000, 79, 1519–1524. [Google Scholar] [CrossRef]
- Ringqvist, M. A histochemical study of temporal muscle fibers in denture wearers and subjects with natural dentition. Eur. J. Oral Sci. 1974, 82, 28–39. [Google Scholar] [CrossRef]
- AL-Omiri, M.K.; Sghaireen, M.G.; Alhijawi, M.M.; Alzoubi, I.A.; Lynch, C.D.; Lynch, E. Maximum bite force following unilateral implant-supported prosthetic treatment: Within-subject comparison to opposite dentate side. J. Oral Rehabil. 2014, 41, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.; Hnat, W.P.; Freudenthaler, J.W.; Marcotte, M.R.; Hönigle, K.; Johnson, B.E. A study of maximum bite force during growth and development. Angle Orthod. 1996, 66, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Castelo, P.M.; Bonjardim, L.R.; Pereira, L.J.; Gavião, M.B.D. Facial dimensions, bite force and masticatory muscle thickness in preschool children with functional posterior crossbite. Braz. Oral Res. 2008, 22, 48–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiliaridis, S.; Kjellberg, H.; Wenneberg, B.; Engström, C. The relationship between maximal bite force, bite force endurance, and facial morphology during growth: A cross-sectional study. Acta Odontol. Scand. 1993, 51, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Abu Alhaija, E.S.; Al Zo’ubi, I.A.; Al Rousan, M.E.; Hammad, M.M. Maximal occlusal bite forces in Jordanian individuals with different dentofacial vertical skeletal patterns. Eur. J. Orthod. 2010, 32, 71–77. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age Group | “A” 20~35 Years Old | “B” 45~59 Years Old | “C” 60~69 Years Old | “D” 70~79 Years Old | “E” 80~99 Years Old | |
|---|---|---|---|---|---|---|
| Sex | 40 F + 39 M | 43 F + 45 M | 48 F + 49 M | 42 F + 40 M | 40 F + 40 M | |
| Mean Age (years ± SD) | 25 ± 5 | 52 ± 5 | 64 ± 3 | 75 ± 3 | 86 ± 3 | p < 0.0001 |
| F—Height (cm) | 167 ± 6 | 163 ± 6 | 163 ± 6 | 160 ± 5 | 159 ± 5 | p < 0.0001 |
| M—Height (cm) | 175 ± 8 | 173 ± 8 | 171 ± 7 | 169 ± 7 | 169 ± 6 | |
| F—Weight (kg) | 59 ± 10 | 66 ± 10 | 66 ± 8 | 64 ± 8 | 60 ± 9 | p < 0.0001 |
| M—Weight (kg) | 73 ± 10 | 77 ± 15 | 75 ± 11 | 74 ± 10 | 70 ± 7 | |
| F—BMI | 21 ± 3 * | 25 ± 3 | 25 ± 3 | 25 ± 3 | 24 ± 3 | p < 0.001 * |
| M—BMI | 24 ± 2 * | 25 ± 3 | 26 ± 3 | 26 ± 3 | 24 ± 2 |
| (a) | ||||||
| Age Group | Sex | Mean | D.S. | Median | Mode | |
| “A” | 40 F | 51 | ±16 | 55 | 70 | p < 0.01 |
| 39 M | 63 | ±20 | 65 | 29 | ||
| “B” | 43 F | 42 | ±13 | 40 | 52 | p < 0.01 |
| 45 M | 55 | ±23 | 52 | 40 | ||
| “C” | 48 F | 37 | ±12 | 34 | 30 | p < 0.001 |
| 49 M | 50 | ±19 | 48 | 39 | ||
| “D” | 42 F | 33 | ±11 | 33 | 35 | p < 0.01 |
| 40 M | 48 | ±20 | 49 | 55 | ||
| “E” | 40 F | 35 | ±12 | 34 | 44 | p < 0.05 |
| 40 M | 42 | ±13 | 40 | 26 | ||
| (b) | ||||||
| Age Group | Sex | Mean | D.S. | Median | Mode | |
| “A” | 40 F | 50 | ±17 | 51 | 60 | p < 0.05 |
| 39 M | 61 | ±20 | 61 | 75 | ||
| “B” | 43 F | 40 | ±13 | 40 | 35 | p < 0.05 |
| 45 M | 53 | ±23 | 49 | 49 | ||
| “C” | 48 F | 35 | ±14 | 35 | 35 | p < 0.0001 |
| 49 M | 52 | ±20 | 49 | 45 | ||
| “D” | 42 F | 32 | ±11 | 31 | 30 | p < 0.01 |
| 40 M | 46 | ±20 | 48 | 50 | ||
| “E” | 40 F | 35 | ±12 | 32 | 25 | p < 0.05 |
| 40 M | 40 | ±14 | 40 | 30 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poli, O.; Manzon, L.; Niglio, T.; Ettorre, E.; Vozza, I. Masticatory Force in Relation with Age in Subjects with Full Permanent Dentition: A Cross-Sectional Study. Healthcare 2021, 9, 700. https://doi.org/10.3390/healthcare9060700
Poli O, Manzon L, Niglio T, Ettorre E, Vozza I. Masticatory Force in Relation with Age in Subjects with Full Permanent Dentition: A Cross-Sectional Study. Healthcare. 2021; 9(6):700. https://doi.org/10.3390/healthcare9060700
Chicago/Turabian StylePoli, Ottavia, Licia Manzon, Tarcisio Niglio, Evaristo Ettorre, and Iole Vozza. 2021. "Masticatory Force in Relation with Age in Subjects with Full Permanent Dentition: A Cross-Sectional Study" Healthcare 9, no. 6: 700. https://doi.org/10.3390/healthcare9060700
APA StylePoli, O., Manzon, L., Niglio, T., Ettorre, E., & Vozza, I. (2021). Masticatory Force in Relation with Age in Subjects with Full Permanent Dentition: A Cross-Sectional Study. Healthcare, 9(6), 700. https://doi.org/10.3390/healthcare9060700