
BiodentineTM Full Pulpotomy in Mature Permanent Teeth with Irreversible Pulpitis and Apical Periodontitis


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
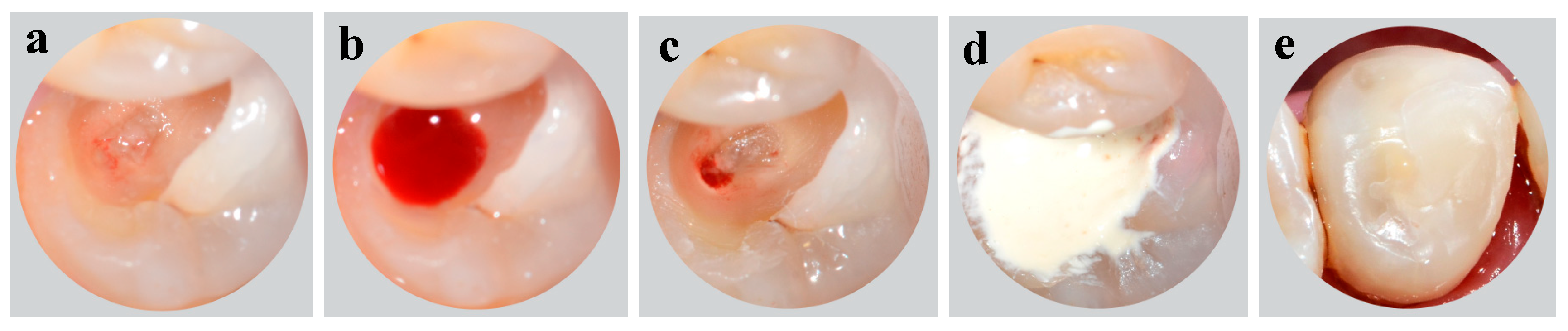
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Smith, A.J.; Cassidy, N.; Perry, H.; Begue-Kirn, C.; Ruch, J.-V.; Lesot, H. Reactionary dentinogenesis. Int. J. Dev. Biol. 2003, 39, 273–280. [Google Scholar]
- Bleicher, F. Odontoblast physiology. Exp. Cell Res. 2014, 325, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.R.; Takahashi, Y.; Graham, L.W.; Simon, S.; Imazato, S.; Smith, A.J. Inflammation–regeneration interplay in the dentine–pulp complex. J. Dent. 2010, 38, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Bjørndal, L. Indirect pulp therapy and stepwise excavation. Pediatric Dent. 2008, 30, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Farges, J.-C.; Alliot-Licht, B.; Renard, E.; Ducret, M.; Gaudin, A.; Smith, A.J.; Cooper, P.R. Dental pulp defence and repair mechanisms in dental caries. Mediat. Inflamm. 2015, 2015, 230251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, J.; Thomas, M.; Locke, M.; Dummer, P. A survey of dental practitioners in Wales to evaluate the management of deep carious lesions with vital pulp therapy in permanent teeth. Br. Dent. J. 2016, 221, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Stolpe, M. Direct pulp capping after a carious exposure versus root canal treatment: A cost-effectiveness analysis. J. Endod. 2014, 40, 1764–1770. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry. Guideline on pulp therapy for primary and immature permanent teeth. Pediatr. Dent. 2009, 31, 179–186. [Google Scholar]
- American Association of Endodontists. Endodontic Diagnosis. Endodontics: Colleagues for Excellence; MediVisuals, Inc.: Richmond, VA, USA, 2013. [Google Scholar]
- Al-Omiri, M.K.; Mahmoud, A.A.; Rayyan, M.R.; Abu-Hammad, O. Fracture resistance of teeth restored with post-retained restorations: An overview. J. Endod. 2010, 36, 1439–1449. [Google Scholar] [CrossRef]
- Bjørndal, L.; Reit, C. Endodontic malpractice claims in Denmark 1995–2004. Int. Endod. J. 2008, 41, 1059–1065. [Google Scholar] [CrossRef]
- Tavares, P.B.; Bonte, E.; Boukpessi, T.; Siqueira, J.F., Jr.; Lasfargues, J.-J. Prevalence of apical periodontitis in root canal–treated teeth from an urban French population: Influence of the quality of root canal fillings and coronal restorations. J. Endod. 2009, 35, 810–813. [Google Scholar] [CrossRef]
- Boucher, Y.; Matossian, L.; Rilliard, F.; Machtou, P. Radiographic evaluation of the prevalence and technical quality of root canal treatment in a French subpopulation. Int. Endod. J. 2002, 35, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Figdor, D. Apical periodontitis: A very prevalent problem. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 651–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuo, T.; Nakanishi, T.; Shimizu, H.; Ebisu, S. A clinical study of direct pulp capping applied to carious-exposed pulps. J. Endod. 1996, 22, 551–556. [Google Scholar] [CrossRef]
- Aguilar, P.; Linsuwanont, P. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: A systematic review. J. Endod. 2011, 37, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Asgary, S.; Eghbal, M.J.; Fazlyab, M.; Baghban, A.A.; Ghoddusi, J. Five-year results of vital pulp therapy in permanent molars with irreversible pulpitis: A non-inferiority multicenter randomized clinical trial. Clin. Oral Investig. 2015, 19, 335–341. [Google Scholar] [CrossRef]
- Taha, N.A.; Ahmad, M.B.; Ghanim, A. Assessment of mineral trioxide aggregate pulpotomy in mature permanent teeth with carious exposures. Int. Endod. J. 2017, 50, 117–125. [Google Scholar] [CrossRef]
- Witherspoon, D.E. Vital pulp therapy with new materials: New directions and treatment perspectives—Permanent teeth. Pediatric Dent. 2008, 30, 220–224. [Google Scholar] [CrossRef]
- Taha, N.A.; Khazali, M.A. Partial pulpotomy in mature permanent teeth with clinical signs indicative of irreversible pulpitis: A randomized clinical trial. J. Endod. 2017, 43, 1417–1421. [Google Scholar] [CrossRef]
- Kundzina, R.; Stangvaltaite, L.; Eriksen, H.; Kerosuo, E. Capping carious exposures in adults: A randomized controlled trial investigating mineral trioxide aggregate versus calcium hydroxide. Int. Endod. J. 2017, 50, 924–932. [Google Scholar] [CrossRef]
- Schmitt, D.; Lee, J.; Bogen, G. Multifaceted use of ProRootTM MTA root canal repair material. Pediatr. Dent. 2001, 23, 326–330. [Google Scholar]
- Tran, X.V.; Gorin, C.; Willig, C.; Baroukh, B.; Pellat, B.; Decup, F.; Opsahl Vital, S.; Chaussain, C.; Boukpessi, T. Effect of a calcium-silicate-based restorative cement on pulp repair. J. Dent. Res. 2012, 91, 1166–1171. [Google Scholar] [CrossRef]
- Simon, S.R.J.; Berdal, A.; Cooper, P.R.; Lumley, P.J.; Tomson, P.L.; Smith, A.J. Dentin-pulp complex regeneration: From lab to clinic. Adv. Dent. Res. 2011, 23, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, J. Staining potential of Neo MTA Plus, MTA Plus, and Biodentine used for pulpotomy procedures. J. Endod. 2015, 41, 1139–1145. [Google Scholar] [CrossRef] [PubMed]
- Dawood, A.E.; Parashos, P.; Wong, R.H.; Reynolds, E.C.; Manton, D.J. Calcium silicate-based cements: Composition, properties, and clinical applications. J. Investig. Clin. Dent. 2017, 8, e12195. [Google Scholar] [CrossRef]
- Quintana, R.M.; Jardine, A.P.; Grechi, T.R.; Grazziotin-Soares, R.; Ardenghi, D.M.; Scarparo, R.K.; Grecca, F.S.; Kopper, P.M.P. Bone tissue reaction, setting time, solubility, and pH of root repair materials. Clin. Oral Investig. 2019, 23, 1359–1366. [Google Scholar] [CrossRef]
- Vallés, M.; Roig, M.; Duran-Sindreu, F.; Martínez, S.; Mercadé, M. Color stability of teeth restored with Biodentine: A 6-month in vitro study. J. Endod. 2015, 41, 1157–1160. [Google Scholar] [CrossRef]
- Donfrancesco, O.; Del Giudice, A.; Zanza, A.; Relucenti, M.; Petracchiola, S.; Gambarini, G.; Testarelli, L.; Seracchiani, M. SEM Evaluation of Endosequence BC Sealer Hiflow in Different Environmental Conditions. J. Compos. Sci. 2021, 5, 99. [Google Scholar] [CrossRef]
- Marconyak Jr, L.J.; Kirkpatrick, T.C.; Roberts, H.W.; Roberts, M.D.; Aparicio, A.; Himel, V.T.; Sabey, K.A. A comparison of coronal tooth discoloration elicited by various endodontic reparative materials. J. Endod. 2016, 42, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Wolters, W.; Duncan, H.; Tomson, P.; Karim, I.; McKenna, G.; Dorri, M.; Stangvaltaite, L.; Van Der Sluis, L. Minimally invasive endodontics: A new diagnostic system for assessing pulpitis and subsequent treatment needs. Int. Endod. J. 2017, 50, 825–829. [Google Scholar] [CrossRef]
- Taha, N.A.; Abdelkhader, S.Z. Outcome of full pulpotomy using Biodentine in adult patients with symptoms indicative of irreversible pulpitis. Int. Endod. J. 2018, 51, 819–828. [Google Scholar] [CrossRef] [PubMed]
- Cushley, S.; Duncan, H.F.; Lappin, M.J.; Tomson, P.L.; Lundy, F.T.; Cooper, P.; Clarke, M.; El Karim, I.A. Pulpotomy for mature carious teeth with symptoms of irreversible pulpitis: A systematic review. J. Dent. 2019, 88, 103158. [Google Scholar] [CrossRef] [PubMed]
- Bergenholtz, G.; Spångberg, L. Controversies in endodontics. Crit. Rev. Oral Biol. Med. 2004, 15, 99–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stashenko, P.; Teles, R.; d’Souza, R. Periapical inflammatory responses and their modulation. Crit. Rev. Oral Biol. Med. 1998, 9, 498–521. [Google Scholar] [CrossRef] [PubMed]
- Asgary, S.; Parhizkar, A. The Role of Vital Pulp Therapy in the Management of Periapical Lesions. Eur. Endod. J. 2021, 6, 130. [Google Scholar]
- Bowles, W.R.; Withrow, J.C.; Lepinski, A.M.; Hargreaves, K.M. Tissue levels of immunoreactive substance P are increased in patients with irreversible pulpitis. J. Endod. 2003, 29, 265–267. [Google Scholar] [CrossRef]
- Chapman, M.N.; Nadgir, R.N.; Akman, A.S.; Saito, N.; Sekiya, K.; Kaneda, T.; Sakai, O. Periapical lucency around the tooth: Radiologic evaluation and differential diagnosis. Radiographics 2013, 33, E15–E32. [Google Scholar] [CrossRef] [PubMed]
- Dayal, P.; Subhash, M.; Bhat, A. Pulpo-periapical periodontitis: A radiographic study. Endodontology 1999, 11, 60–64. [Google Scholar]
- Lin, L.M.; Ricucci, D.; Saoud, T.M.; Sigurdsson, A.; Kahler, B. Vital pulp therapy of mature permanent teeth with irreversible pulpitis from the perspective of pulp biology. Aust. Endod. J. 2020, 46, 154–166. [Google Scholar] [CrossRef]
- Ricucci, D.; Loghin, S.; Siqueira Jr, J.F. Correlation between clinical and histologic pulp diagnoses. J. Endod. 2014, 40, 1932–1939. [Google Scholar] [CrossRef]
- Stanley, H.R. Pulp capping: Conserving the dental pulp—Can it be done? Is it worth it? Oral Surg. Oral Med. Oral Pathol. 1989, 68, 628–639. [Google Scholar] [CrossRef]
- Tran, X.V.; Salehi, H.; Truong, M.T.; Sandra, M.; Sadoine, J.; Jacquot, B.; Cuisinier, F.; Chaussain, C.; Boukpessi, T. Reparative mineralized tissue characterization after direct pulp capping with calcium-silicate-based cements. Materials 2019, 12, 2102. [Google Scholar] [CrossRef] [Green Version]
- Giraud, T.; Jeanneau, C.; Bergmann, M.; Laurent, P.; About, I. Tricalcium silicate capping materials modulate pulp healing and inflammatory activity in vitro. J. Endod. 2018, 44, 1686–1691. [Google Scholar] [CrossRef] [Green Version]
- Massler, M. Preserving the exposed pulp: A review. J. Pedod. 1978, 2, 217–227. [Google Scholar] [PubMed]
- Atmeh, A.; Chong, E.; Richard, G.; Festy, F.; Watson, T. Dentin-cement interfacial interaction: Calcium silicates and polyalkenoates. J. Dent. Res. 2012, 91, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Ha, H.-T. The effect of the maturation time of calcium silicate-based cement (Biodentine™) on resin bonding: An in vitro study. Appl. Adhes. Sci. 2019, 7, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Pradelle-Plasse, N.; Tran, X.V.; Colon, P.; Laurent, P.; Aubut, V.; About, I.; Goldberg, M. Emerging trends in (bio) material research. In Biocompatibility or Cytotoxic Effects of Dental Composites, 1st ed.; Coxmoor Publishing Company: Oxford, UK, 2009; pp. 181–203. [Google Scholar]
- Koubi, G.; Colon, P.; Franquin, J.-C.; Hartmann, A.; Richard, G.; Faure, M.-O.; Lambert, G. Clinical evaluation of the performance and safety of a new dentine substitute, Biodentine, in the restoration of posterior teeth—A prospective study. Clin. Oral Investig. 2012, 17, 243–249. [Google Scholar] [CrossRef] [Green Version]
- Duncan, H.; Galler, K.; Tomson, P.; Simon, S.; El-Karim, I.; Kundzina, R.; Krastl, G.; Dammaschke, T.; Fransson, H. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int. Endod. J. 2019, 52, 923–934. [Google Scholar]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, X.V.; Ngo, L.T.Q.; Boukpessi, T. BiodentineTM Full Pulpotomy in Mature Permanent Teeth with Irreversible Pulpitis and Apical Periodontitis. Healthcare 2021, 9, 720. https://doi.org/10.3390/healthcare9060720
Tran XV, Ngo LTQ, Boukpessi T. BiodentineTM Full Pulpotomy in Mature Permanent Teeth with Irreversible Pulpitis and Apical Periodontitis. Healthcare. 2021; 9(6):720. https://doi.org/10.3390/healthcare9060720
Chicago/Turabian StyleTran, Xuan Vinh, Lan Thi Quynh Ngo, and Tchilalo Boukpessi. 2021. "BiodentineTM Full Pulpotomy in Mature Permanent Teeth with Irreversible Pulpitis and Apical Periodontitis" Healthcare 9, no. 6: 720. https://doi.org/10.3390/healthcare9060720
APA StyleTran, X. V., Ngo, L. T. Q., & Boukpessi, T. (2021). BiodentineTM Full Pulpotomy in Mature Permanent Teeth with Irreversible Pulpitis and Apical Periodontitis. Healthcare, 9(6), 720. https://doi.org/10.3390/healthcare9060720