
Mortality Trends by Causes of Death and Healthcare during a Period of Global Uncertainty (1990–2017)

Abstract
:1. Introduction
2. Literature Review
- -
- “the expansion of morbidity hypothesis” (the American epidemiologist Gruenberg (1977) pointed out that medical progress at that time was remarkable and that antibiotics were the most innovative invention in saving lives but nevertheless medical care should not only focus on saving lives, but also on improving the health and disability of the chronically ill because, as a consequence, increasing life expectancy will only lead to an extension of illness and disability, with profound implications for increased public spending on health care; and American mental health biostatistician Morton Kramer has made similar arguments);
- -
- “the compression of morbidity hypothesis” (a model proposed by epidemiologist and rheumatologist Fries (1980), who considered it important to compress mortality around the age of 85, despite the constant improvement in life expectancy, because senility will eventually lead to “natural death”, after which it will be difficult for the body to recover from even the slightest suffering; encouraging the development of preventive medicine);
- -
- “the dynamic equilibrium hypothesis”, (a model proposed by the American demographer Kenneth Manton, as a mediation between the two models mentioned above; based on four distinct principles:
- “an individual consists of many organs and each of them senesce in their own rate. Thus, the occurrence of deaths depends on the organ that first reaches insufficient levels of capacity”;
- “these states of component failure might be identified with major chronic degenerative diseases”;
- “effective prevention or treatment of an individual component failure can postpone death of the organism. Since many diseases share the same risk factors, reduction in disease progression rate within one component might also slow down disease progression within another component”;
Proposed Working Hypotheses
3. Materials and Methods
3.1. Data Collection
- -
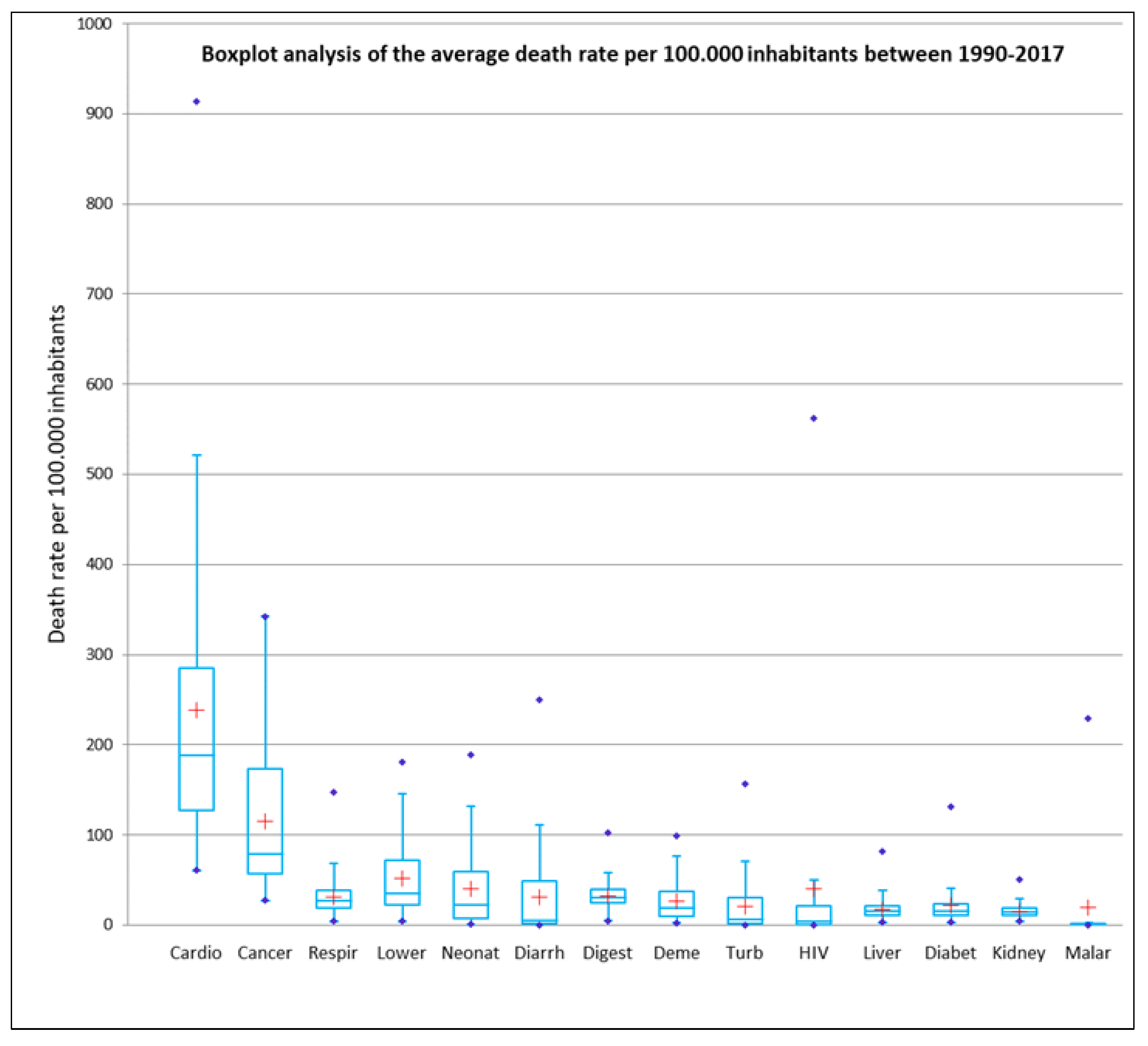
- IHME (Institute for Health Metrics and Evaluation) [26], the Global Burden of Disease Collaborative Network, is an independent population health research institute at UW Medicine, part of the University of Washington, that provides health-related statistics, but also with expertise in other related areas, such as the causation of violent deaths (suicide, terrorism, road traffic accidents etc.) The Global Burden of Disease is a major global study on the causes of death and disease published in the medical journal The Lancet [27]. The resource has been the primary source for disseminating global data on deaths by cause. We considered data from 1990–2017 (27 years), and the top 14 global killer disease types (threshold of 500,000 deaths in 2017), with malaria being the last condition considered (Table 1). In order to obtain the most accurate database possible, the variables were standardised by group maximum. The study was based on data from 194 countries, reported per 100,000 inhabitants, averaged over 27 years of study.
- -
- OWID (Our World in Data), an institute, but also an online scientific publication, which generally focuses on the study of global social issues. The institute does not generate its own statistical data but mention of this institute is necessary because the initial data was obtained through this “portal” [28].
- -
- World Bank, the most important institution in the collection of statistical data worldwide [29]. The data on social and economic aspects of society (the exploratory variables) were obtained from this institution. The organisation collects statistical data from all spheres of society and beyond. The purpose of the proposed variables is to highlight socio-economic impact, health care and to help outline typical territorial structures with a relatively uniform distribution (Table 2).
3.2. Data Analysis Methods
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bergeron-Boucher, M.P.; Aburto, J.M.; Van Raalte, A. Diversification in causes of death in low-mortality countries: Emerging patterns and implications. BMJ Global Health 2020, 5, e002414. [Google Scholar] [CrossRef] [PubMed]
- Deaton, A. Marea evadare. In Sănătatea, Bogăția și Originile Inegalității; Editura Litera București: Bucharest, Romania, 2017. [Google Scholar]
- Abdel-Rahmin, O. The epidemiologic transition: A theory of the epidemiology of population change. Milbank Q. 2005, 83, 731–757. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Rahmin, O. The epidemiologic transition: A theory of the epidemiology of population change/Abdel R. Omran. Bull. World Health Organ. Int. J. Public Health 2001, 79, 161–170. Available online: https://apps.who.int/iris/handle/10665/58102 (accessed on 17 June 2021).
- Mc Keown, R.E. The Epidemiologic Transition: Changing Patterns of Mortality and Population Dynamics. Am. J. Lifestyle Med. 2009, 3 (Suppl. 1), 19S–26S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caselli, G.; Meslé, F.; Vallin, J. Epidemiologic Transition Theory Exceptions. Genus JSTOR 2002, 58, 9–51. Available online: www.jstor.org/stable/29788712 (accessed on 15 April 2021).
- Weisz, G.; Olszynko-Gryn, J. The theory of epidemiologic transition: The origins of a citation classic. J. Hist. Med. Allied. Sci. 2010, 65, 287–326. [Google Scholar] [CrossRef] [PubMed]
- Moe, J.O.; Hagen, T. Trends and variation in mild disability and functional limitations among older adults in Norway, 1986–2008. Eur. J. Ageing 2011, 8, 49–61. [Google Scholar] [CrossRef] [Green Version]
- Vallin, J.; Meslé, F. Convergences and divergences in mortality. A new approach to health transition. Demogr. Res. Spec. Collect. 2004, 2, 11–44. Available online: www.demographic-research.org/special/2/2/ (accessed on 17 June 2021). [CrossRef]
- Armelagos, G.J.; Brown, P.J.; Turner, B. Evolutionary, historical and political economic perspectives on health and disease. Soc. Sci. Med. 2005, 61, 755–765. [Google Scholar] [CrossRef]
- Mackenbach, J.P. The rise and fall of diseases: Reflections on the history of population health in Europe since ca. Eur. J. Epidemiol. 2021. [Google Scholar] [CrossRef]
- Mackenbach, J.P. Chapter 3 Understanding Trends in Population Health. In A History of Population Health; Brill|Rodopi: Leiden, The Netherlands, 2020. [Google Scholar] [CrossRef]
- Fries, J.F. Aging, natural death, and the compression of morbidity. N. Engl. J. Med. 1980, 303, 130–135. [Google Scholar] [CrossRef] [Green Version]
- Olshansky, S.J.; Wilkins, R. Introduction. J. Aging Health 1998, 10, 123–135. [Google Scholar] [CrossRef]
- Lussier, M.; Bourbeau, R.; Choinière, R. Does the recent evolution of Canadian mortality agree with the epidemiologic transition theory. Demogr. Res. 2008, 18, 531–568. [Google Scholar] [CrossRef] [Green Version]
- Meslé, F.; Vallin, J. La Transition Sanitaire: Tendances et Perspectives. In Démographie: Analyse et Synthèse, III. Les Déterminants de la Mortalité; Caselli, G., Vallin, J., Wunsch, G., Eds.; Med Sci: Paris, France, 2002; pp. 439–461. [Google Scholar]
- Meslé, F. Ecart d’espérance de vie entre les sexes: Les raisons du recul de l’avantage féminin. Rev. d’Epidémiologie St. Publique. 2004, 52, 333–352. [Google Scholar] [CrossRef]
- Vallin, J.; Jasilionis, D.; Meslé, F. La transition sanitaire à l’épreuve d’une histoire tourmentée: Le cas des pays baltes. Popul. Sociétés. 2008, 555, 1–4. Available online: http://www.ined.fr/fr/publications/population-et-societes/transition-sanitaire-histoire-tourmentee-pays-baltes/ (accessed on 17 June 2021). [CrossRef] [Green Version]
- Vallin, J.; Meslé, F. De la Transition Épidémiologique à la Transition Sanitaire: L’improbable Convergence générale. In Ralentissements, Résistances et Ruptures dans les Transitions Démographiques, Actes de la Chaire Quetelet; Tabutin, D., Masquelier, B., Eds.; Presses Universitaires de Louvain: Louvain-la-Neuve, France, 2010; pp. 257–290. [Google Scholar]
- Caldwell, J.C. Health transition: The cultural, social and behavioural determinants of health in the Third World. Soc. Sci. Med. 1993, 36, 125–135. [Google Scholar] [CrossRef]
- Picheral, H. La transition sanitaire dans le monde (World health transition). Bull. l’Association Géogr. Fr. 1996, 73, 75–85. [Google Scholar] [CrossRef]
- Caselli, G. Transition sanitaire et structure par cause de la mortalité: Anciennes et nouvelles causes. Ann. Démo. Hist. 1989, 55–77. [Google Scholar] [CrossRef]
- Meslé, F.; Vallin, J. Transition sanitaire: Tendances et perspectives. M S Med. Sci. 2000, 16, 1161–1171. [Google Scholar] [CrossRef]
- Gaudillière, J.P. Un nouvel ordre sanitaire international? Performance, néolibéralisme et outils du gouvernement médico-économique. Écol. Polit. 2016, 52, 107–124. Available online: https://www.cairn.info/revue-ecologie-et-politique-2016-1-page-107.htm (accessed on 17 June 2021). [CrossRef]
- Buse, K.; Harmer, A. Seven Habits of Highly Effective Global Public-Private Health Partnerships. Pract. Potential Soc. Sci. Med. 2007, 64, 259–271. [Google Scholar] [CrossRef] [PubMed]
- The Institute for Health Metrics and Evaluation. Available online: http://www.healthdata.org/ (accessed on 17 June 2021).
- Ritchie, H.; Roser, M. Causes of Death. Published online at Our World in Data.org. 2018. Available online: https://ourworldindata.org/causes-of-death (accessed on 10 January 2021).
- Our World in Data. Available online: https://ourworldindata.org/ (accessed on 17 June 2021).
- World Bank. Available online: https://www.worldbank.org/en/home (accessed on 17 June 2021).
- XLSTAT Version 2014.5.03 Copyright Addinsoft 1995–2014 (2014) XLSTAT and Addinsoft are Registered Trademarks of Addinsoft. Available online: https://www.xlstat.com (accessed on 17 June 2021).
- Groza, O. SIG între structurile spaţiale generale şi specificul local, Analele Ştiinţifice ale Universităţii “Al. I. Cuza” din Iaşi, (serie nouă), tomul XLVII, s. II c. Geogr. Supl. Lucr. Simp. SIG 2002, 7, 51–66. [Google Scholar]
- Bonilla, C. Defining Communities with ESRI’s Grouping Analysis Tool, Azavea (blog). 2016. Available online: https://www.azavea.com/blog/2016/10/12/defining-communities-grouping-analysis-tool/ (accessed on 17 June 2021).
- Jolliffe, I.T.; Cadima, J. Principal component analysis: A review and recent developments. Phil. Trans. R. Soc. A 2016. [Google Scholar] [CrossRef]
- Tukey, J.W. Tukey, Exploratory Data Analysis; Addison-Wesley: Hoboken, NJ, USA, 1977. [Google Scholar]
- Mackenbach, J.P. Chapter 2 Long-term Trends in Population Health. In A History of Population Health; Brill|Rodopi: Leiden, The Netherlands, 2020. [Google Scholar] [CrossRef]
- Hashim, D.; Boffetta, P.; La Vecchia, C.; Rota, M.; Bertuccio, P.; Malvezzi, M.; Negri, E. The global decrease in cancer mortality: Trends and disparities. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 926–933. [Google Scholar] [CrossRef]
- Wang, L.; Kong, L.; Wu, F.; Bai, Y.; Burton, R. Preventing chronic diseases in China. Lancet 2005, 366, 1821–1824. [Google Scholar] [CrossRef]
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M.; et al. Rapid health transition in China, 1990-2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- Martín Cervantes, P.A.; Rueda López, N.; Cruz Rambaud, S. The Effect of Globalization on Economic Development Indicators: An Inter-Regional Approach. Sustainability 2020, 12, 1942. [Google Scholar] [CrossRef] [Green Version]
- Frenk, J.; Frejka, T.; Bobadilla, J.L.; Stern, C.; Lozano, R.; Sepúlveda, J.; José, M. The epidemiologic transition in Latin America. Bol. Oficina Sanit Panam. 1991, 111, 485–496. [Google Scholar] [PubMed]
- Santosa, A.; Wall, S.; Fottrell, E.; Högberg, U.; Byass, P. The development and experience of epidemiological transition theory over four decades: A systematic review. Glob. Health Action 2014, 7, 23574. [Google Scholar] [CrossRef]
- Tyrovolas, S. The burden of disease in Saudi Arabia 1990–2017: Results from the Global Burden of Disease Study 2017. Lancet Planet. Health 2020, 4, 195–208. [Google Scholar] [CrossRef]
- El Bcheraoui, C.; Mimche, H.; Miangotar, Y.; Varsha, S.K.; Ziegeweid, F.; Krohn, J.K.; Ekat, M.H.; Nansseu, J.R.; Dimbuene, Z.T.; Mokdad, A.H.; et al. Burden of disease in francophone Africa, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Glob. Health 2020, 8, e341–e351. [Google Scholar] [CrossRef] [Green Version]
- Robert, W. La mortinatalité: Éclairage historique sur des problèmes persistants d’estimation et d’interprétation. Population 2008, 63, 591–614. Available online: https://www.cairn-int.info/journal-population-2008-4-page-591.htm (accessed on 17 June 2021).
- GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Organisation Mondiale de la Santé. Rapport sur la Santé Dans le Monde. OMS Genève. 2004. Available online: https://www.who.int/whr/2004/fr/ (accessed on 17 June 2021).
- Dixon, S.; Mc Donald, S.; Roberts, J. The impact of HIV and AIDS on Africa’s economic development. BMJ 2002, 324, 232–234. [Google Scholar] [CrossRef] [Green Version]
- Boerma, J.T.; Nyamukapa, C.; Urassa, M.; Gregson, S. Understanding the uneven spread of HIV within Africa: A comparative study of biologic, behavioral, and contextual factors in rural populations in Tanzania and Zimbabwe. Sex. Transm. Dis. 2003, 30, 79–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, T.; Gesesew, H.A.; Bambra, C.; Giugliani, E.; Popay, J.; Sanders, D.; Macinko, J.; Musolino, C.; Baum, F. Why do some countries do better or worse in life expectancy relative to income? An analysis of Brazil, Ethiopia, and the Unite States of America. Int. J. Equity Health 2020, 19, 202. [Google Scholar] [CrossRef] [PubMed]
- Shaw, W.J.; Horrace, C.W.; Vogel, J.R. The Determinants of Life Expectancy: An Analysis of the OECD Health Data. South. Econ. J. 2005, 71, 768–783. [Google Scholar] [CrossRef] [Green Version]
- Pająk, A.; Kozela, M. Cardiovascular Disease in Central and East Europe. Public Health Rev. 2011, 33, 416–435. [Google Scholar] [CrossRef] [Green Version]
- Moser, K.; Shkolnikov, V.; Leon, D.A. World mortality 1950-2000: Divergence replaces convergence from the late 1980s. Bull World Health Organ. 2005, 83, 202–209. Available online: https://apps.who.int/iris/handle/10665/72983 (accessed on 10 April 2021). [PubMed]
- Meslé, F.; Vallin, J. The End of East–West Divergence in European Life Expectancies? An Introduction to the Special Issue. Eur. J. Popul. 2017, 33, 615–627. [Google Scholar] [CrossRef] [Green Version]
- Men, T.; Brennan, P.; Boffetta, P.; Zaridze, D. Russian mortality trends for 1991-2001: Analysis by cause and region. BMJ Clin. Res. 2003, 327, 964. [Google Scholar] [CrossRef] [Green Version]
- Doll, R.; Peto, R.; Hall, E.; Wheatley, K.; Gray, R. Mortality in relation to consumption of alcohol: 13 years’ observations on male British doctors. BMJ 1994, 309, 911–918. [Google Scholar] [CrossRef] [Green Version]
- OECD. States of Fragility; OECD Publishing: Paris, France, 2020. [Google Scholar] [CrossRef]
- Muntele, I.; Istrate, M.; Bănică, A.; Horea-Șerban, R.I. Trends in Life Expectancy in Romania between 1990 and 2018. A Territorial Analysis of its Determinants. Sustainability 2020, 12, 3802. [Google Scholar] [CrossRef]
- Nick, J.; Menzies, M.; Radchenko, D. Covid 19 s wawe in Europe and the United States. Chaos 2021, 31, 031105. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Deaths by Cause | (Dependent Variables) | |
|---|---|---|
| Cardio—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from cardiovascular disease. Cancer—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from cancer. Respir—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from respiratory diseases. Lower—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from lower respiratory infections. Neonat—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from neonatal disorders. Diarrh—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from diarrheal diseases. Digest—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from digestive diseases. Deme—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from dementia. Turb—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from tuberculosis. HIV—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from HIV AIDS. Liver—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from liver diseases. Diabet—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from diabetes. Kidney—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from kidney disease. Malar—Average rates per 100.000 inhabitants between 1990 and 2017 for deaths from malaria. | ||
| Socio-Economic Variables (Exploratory Variables) |
|---|
| GDPpC—Average GDP/per capita in the period 1990–2017. LifeExpe—Average life expectancy in the 1990–2017. HDI—Average Human Development Index (HDI) 1990–2017. Litera—The average share (%) of the literate population in the period 1990–2015. FSI—The average of the state fragility index in the period 2007–2017. Unempl—Total unemployment (%-of total labour force), average in the period 1990–2017 Med_age—Median age (average in the period 1990–2015). Obesity—Share (%) of the obese population, average in the period 1990–2016. Medic_exp—Average medical expenses per person in the period 1995–2017. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ursache, S.-A.; Gabor, V.-R.; Muntele, I.; Maftei, M. Mortality Trends by Causes of Death and Healthcare during a Period of Global Uncertainty (1990–2017). Healthcare 2021, 9, 748. https://doi.org/10.3390/healthcare9060748
Ursache S-A, Gabor V-R, Muntele I, Maftei M. Mortality Trends by Causes of Death and Healthcare during a Period of Global Uncertainty (1990–2017). Healthcare. 2021; 9(6):748. https://doi.org/10.3390/healthcare9060748
Chicago/Turabian StyleUrsache, Simona-Andreea, Vicentiu-Robert Gabor, Ionel Muntele, and Mihai Maftei. 2021. "Mortality Trends by Causes of Death and Healthcare during a Period of Global Uncertainty (1990–2017)" Healthcare 9, no. 6: 748. https://doi.org/10.3390/healthcare9060748
APA StyleUrsache, S. -A., Gabor, V. -R., Muntele, I., & Maftei, M. (2021). Mortality Trends by Causes of Death and Healthcare during a Period of Global Uncertainty (1990–2017). Healthcare, 9(6), 748. https://doi.org/10.3390/healthcare9060748