
Forecast of Outpatient Visits to a Tertiary Eyecare Network in India Using the EyeSmart Electronic Medical Record System

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Data Preparation
3. Results
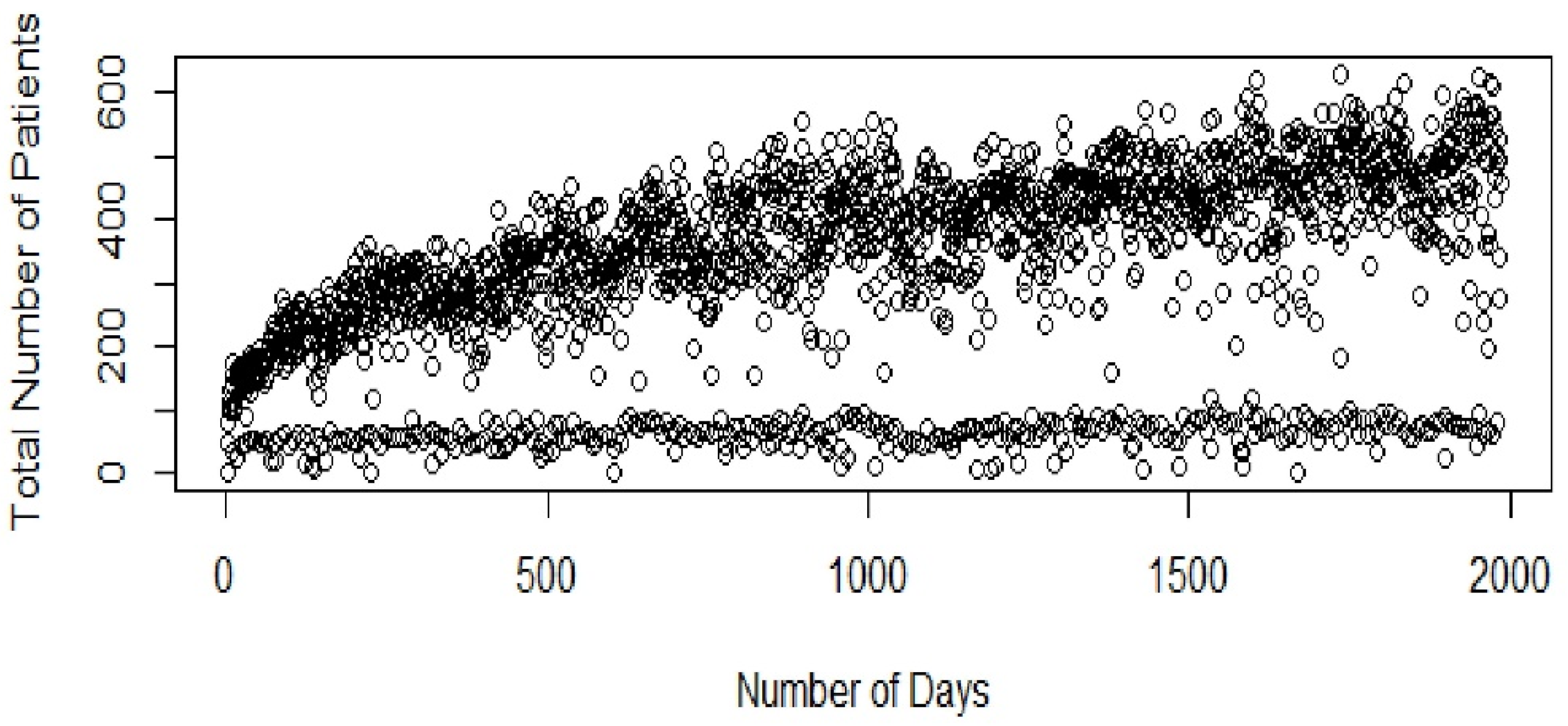
3.1. Exploratory Data Analysis and Data Preprocessing
3.1.1. Data Visualization
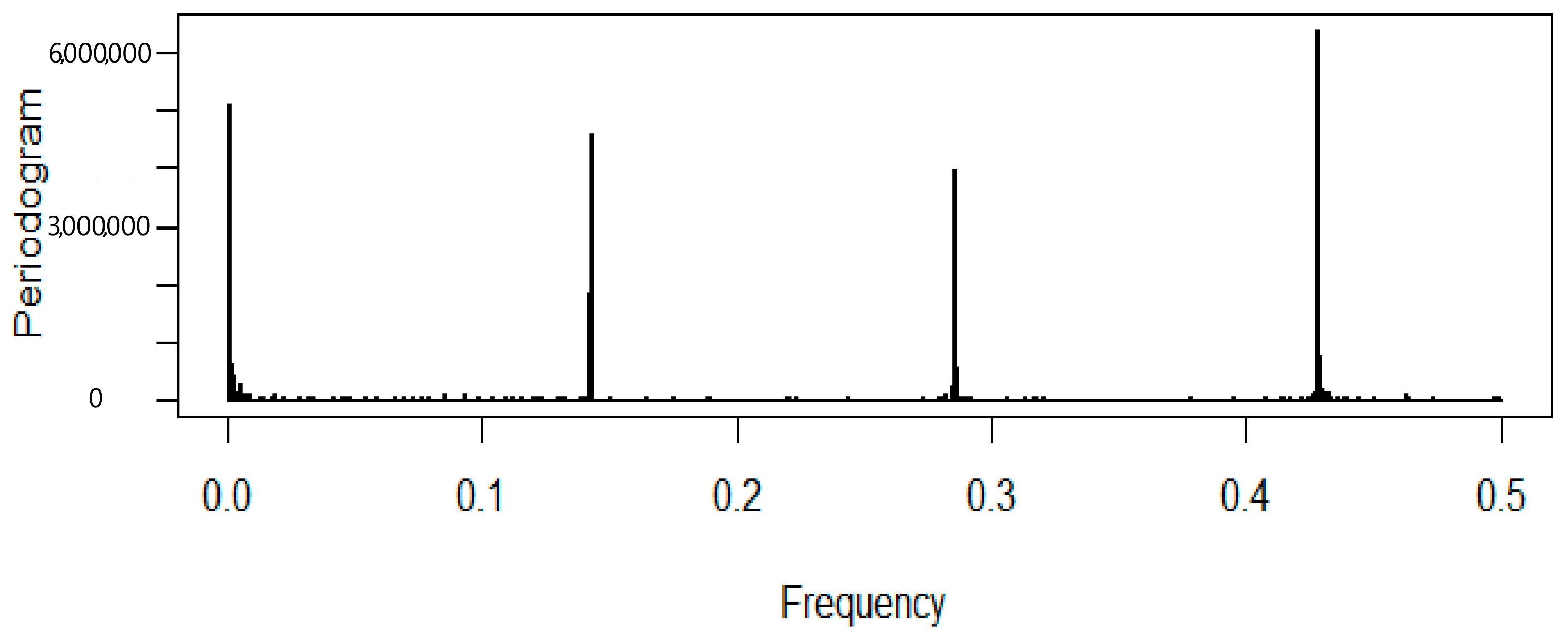
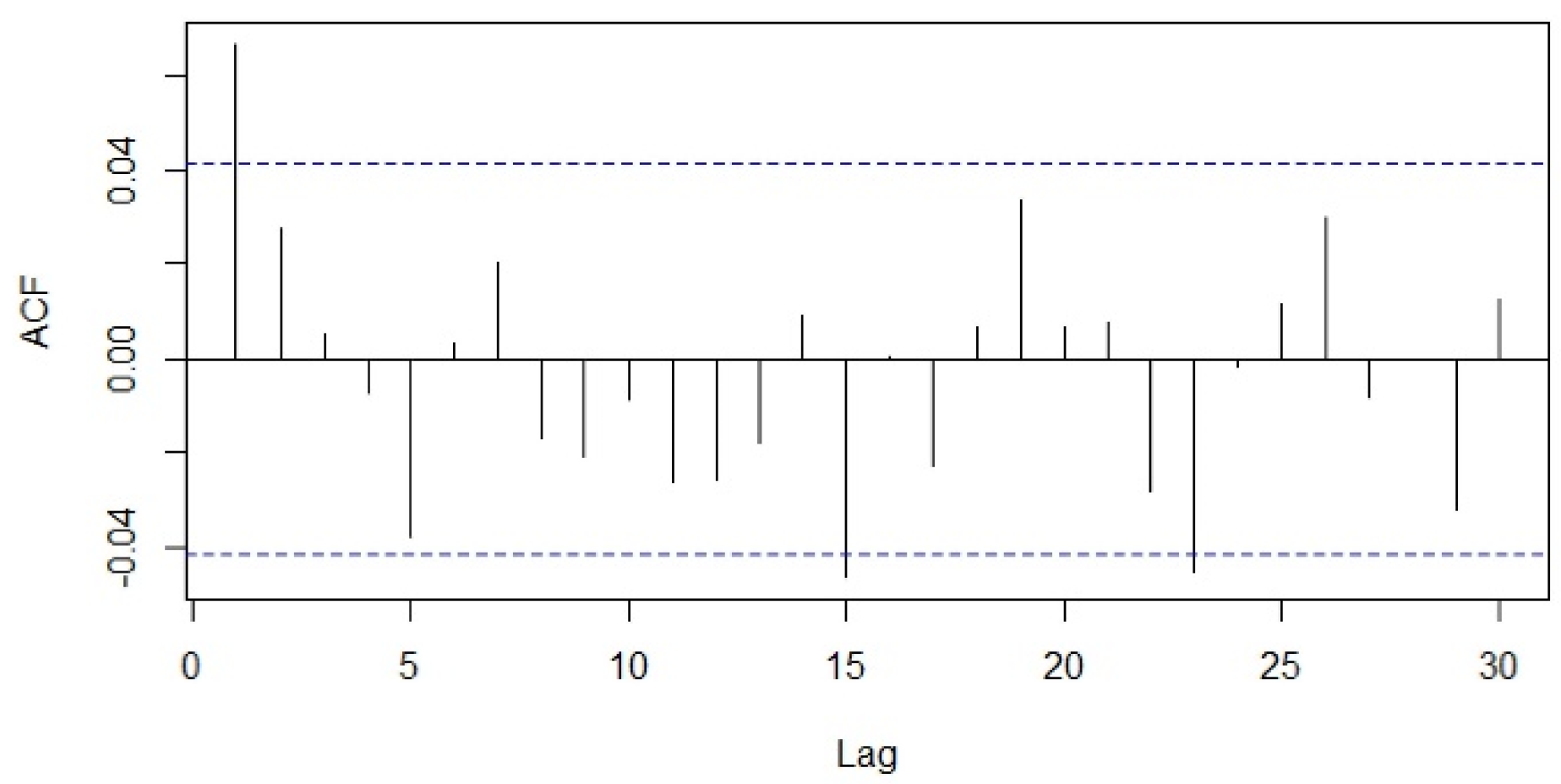
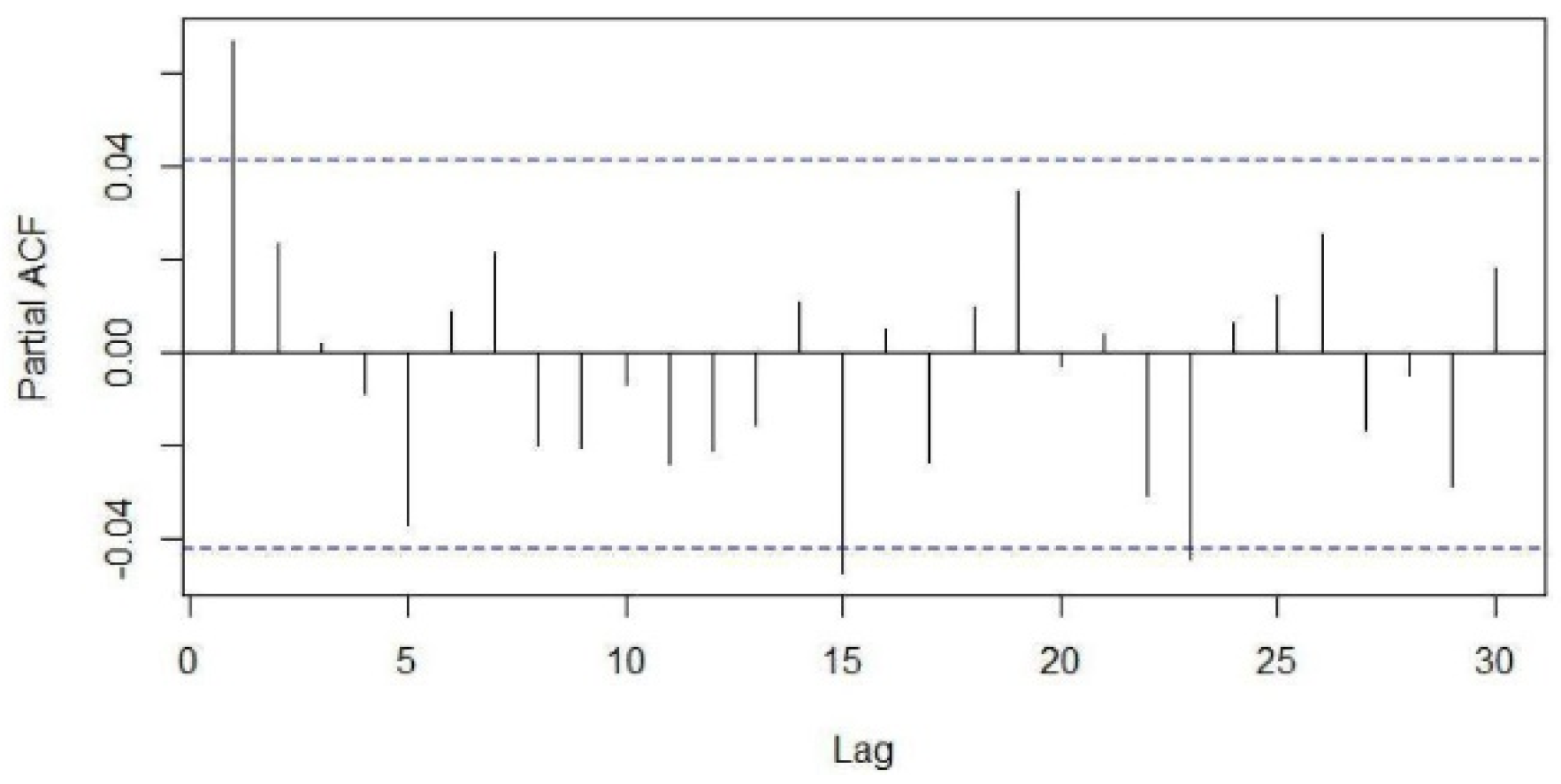
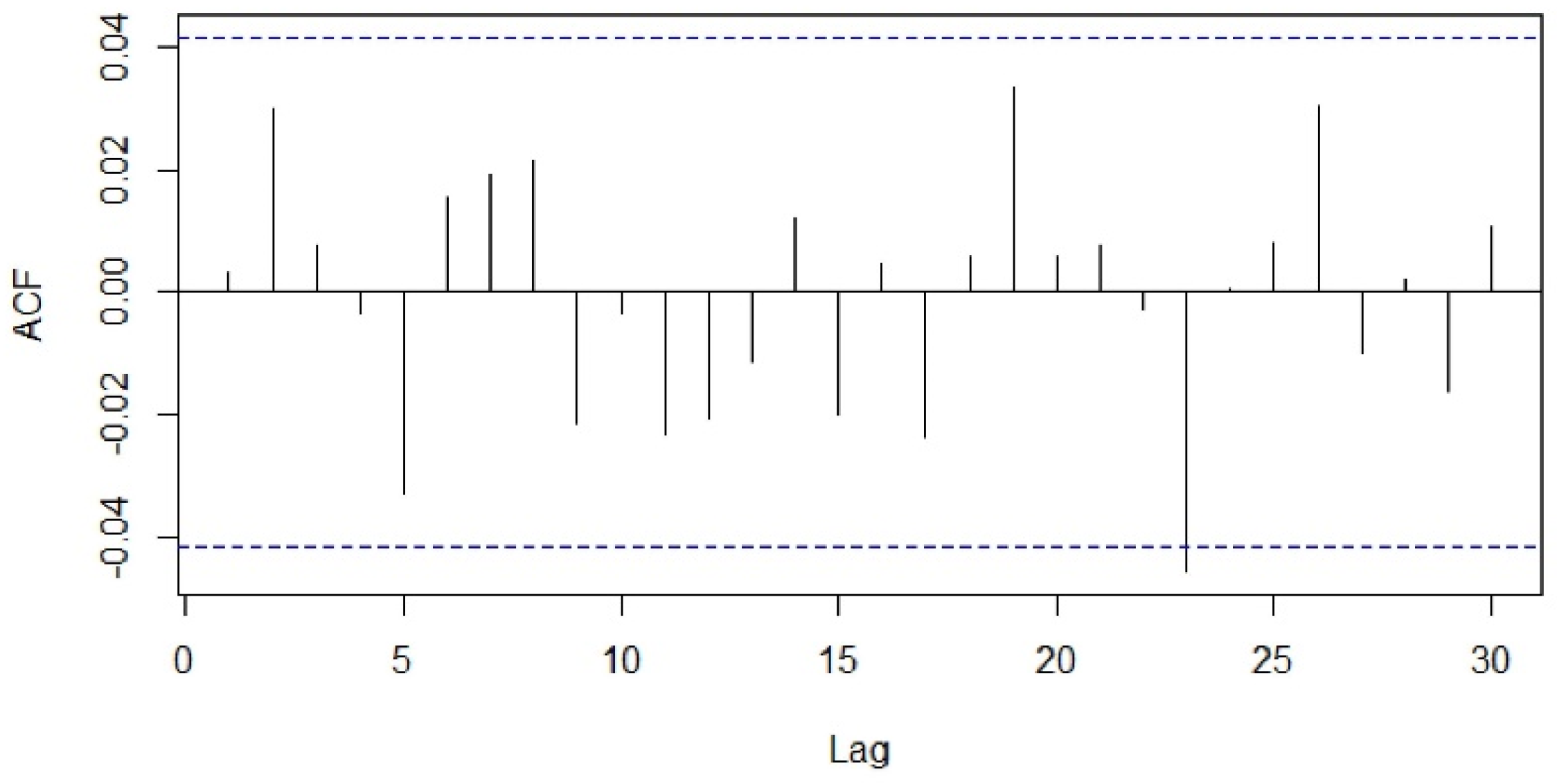
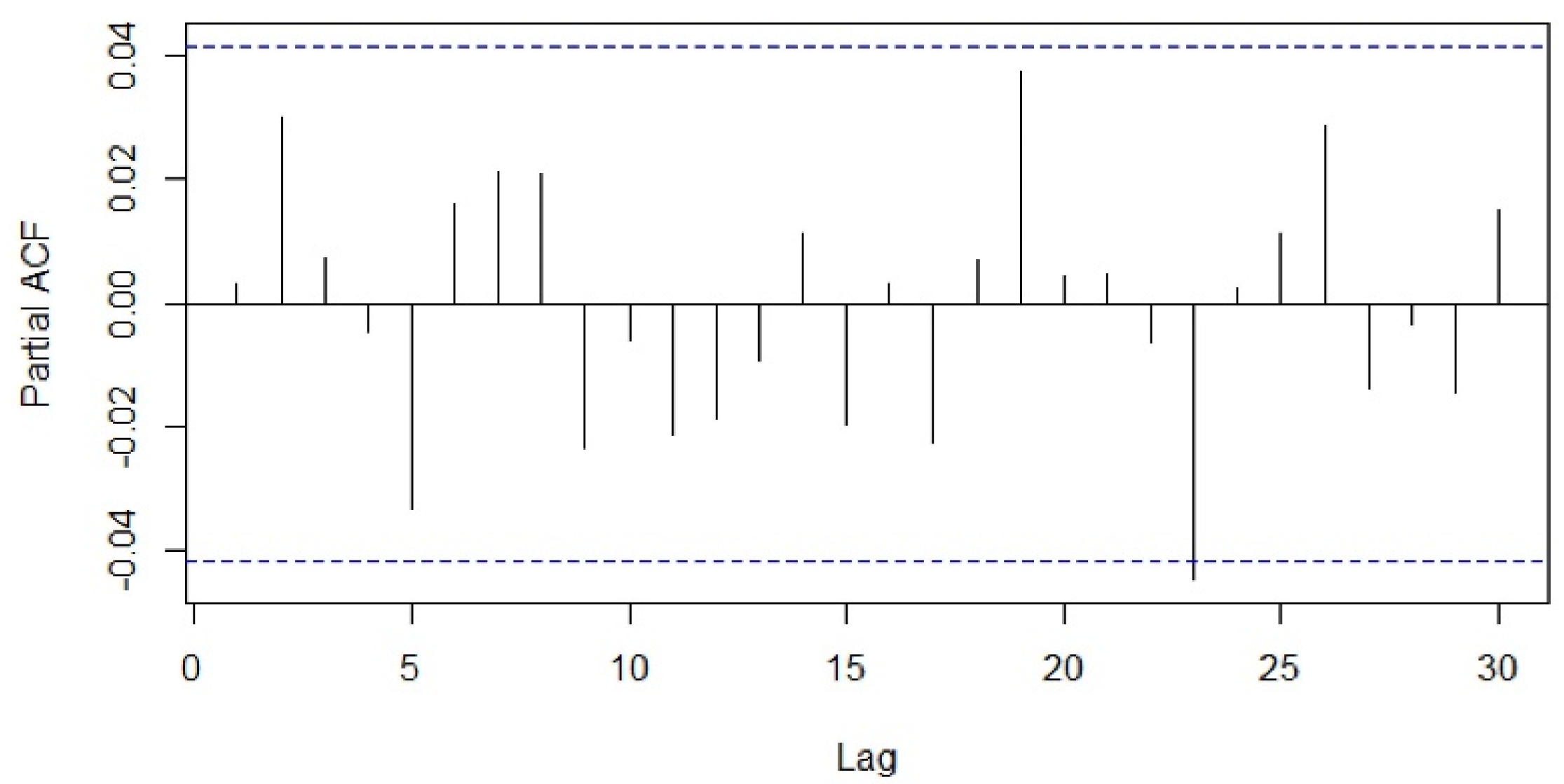
3.1.2. Stationarity Check
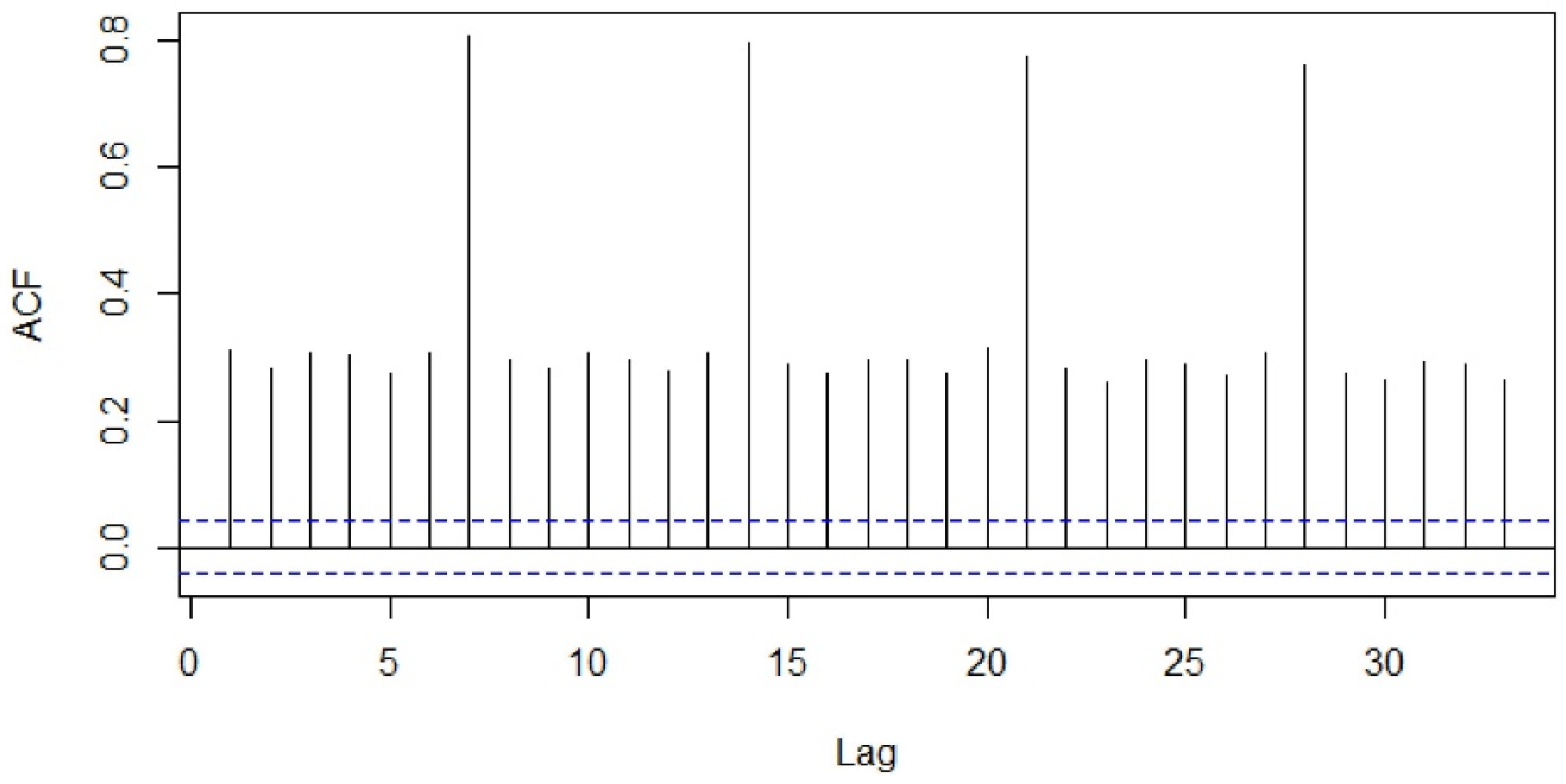
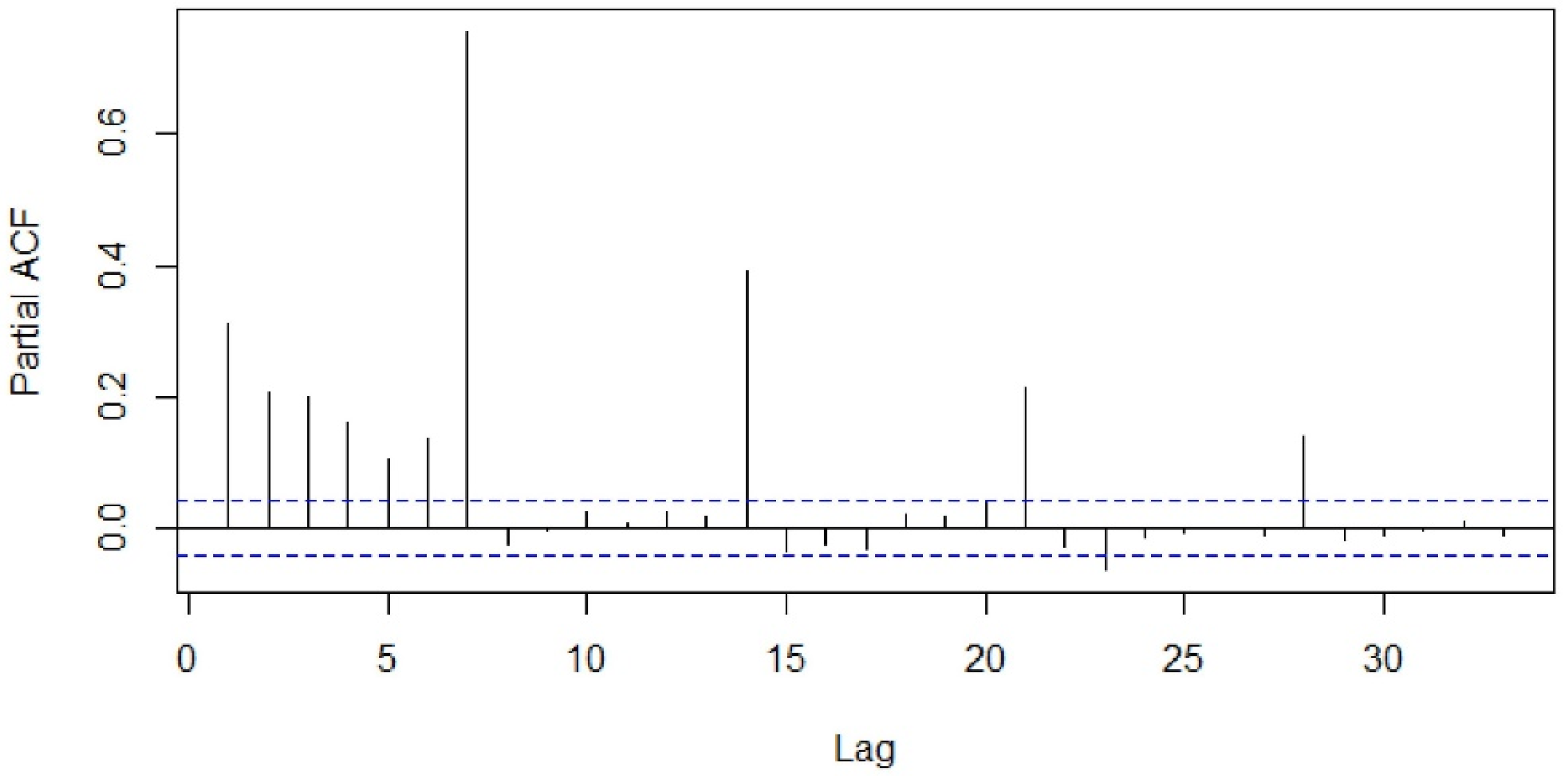
3.2. Model Identification and Diagnostic Checking
3.3. Evaluation Protocol
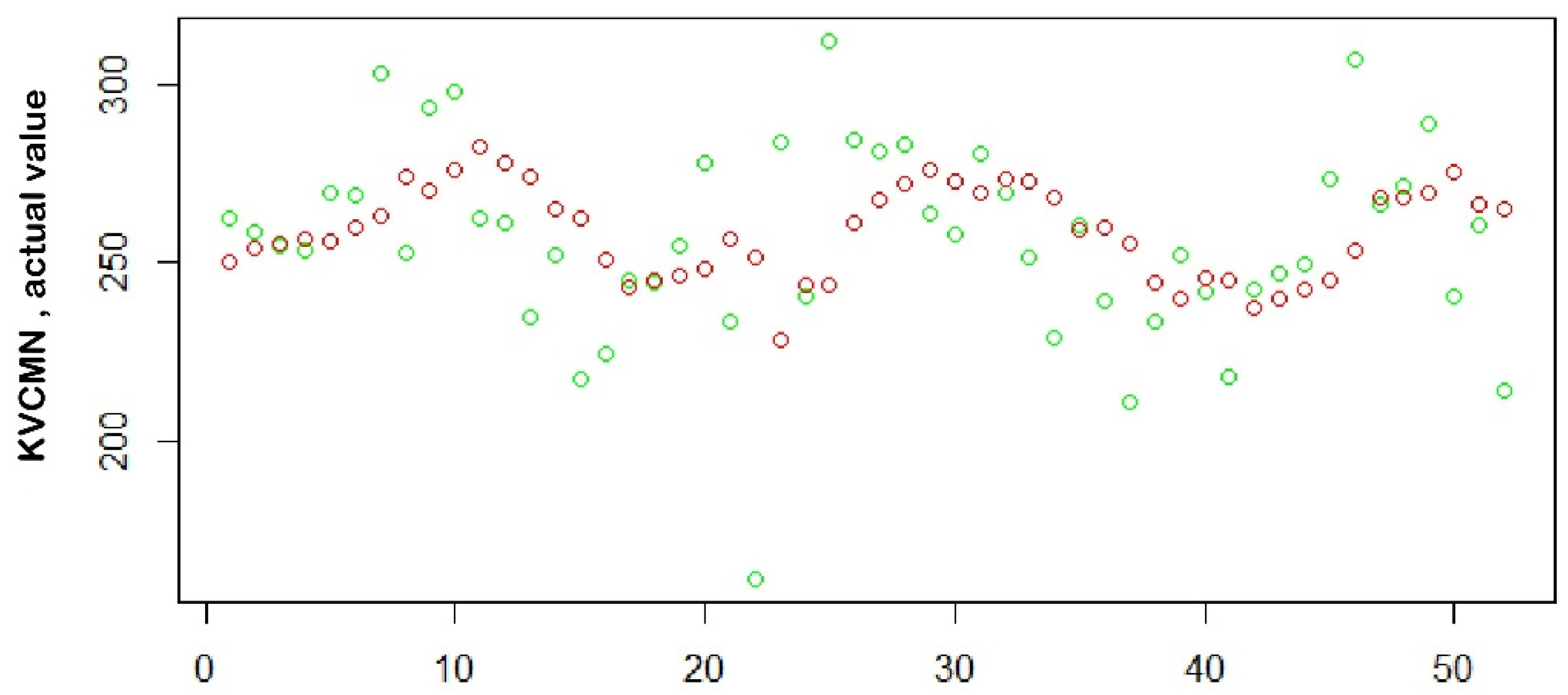
3.4. Measuring Forecast Performance
4. Discussion
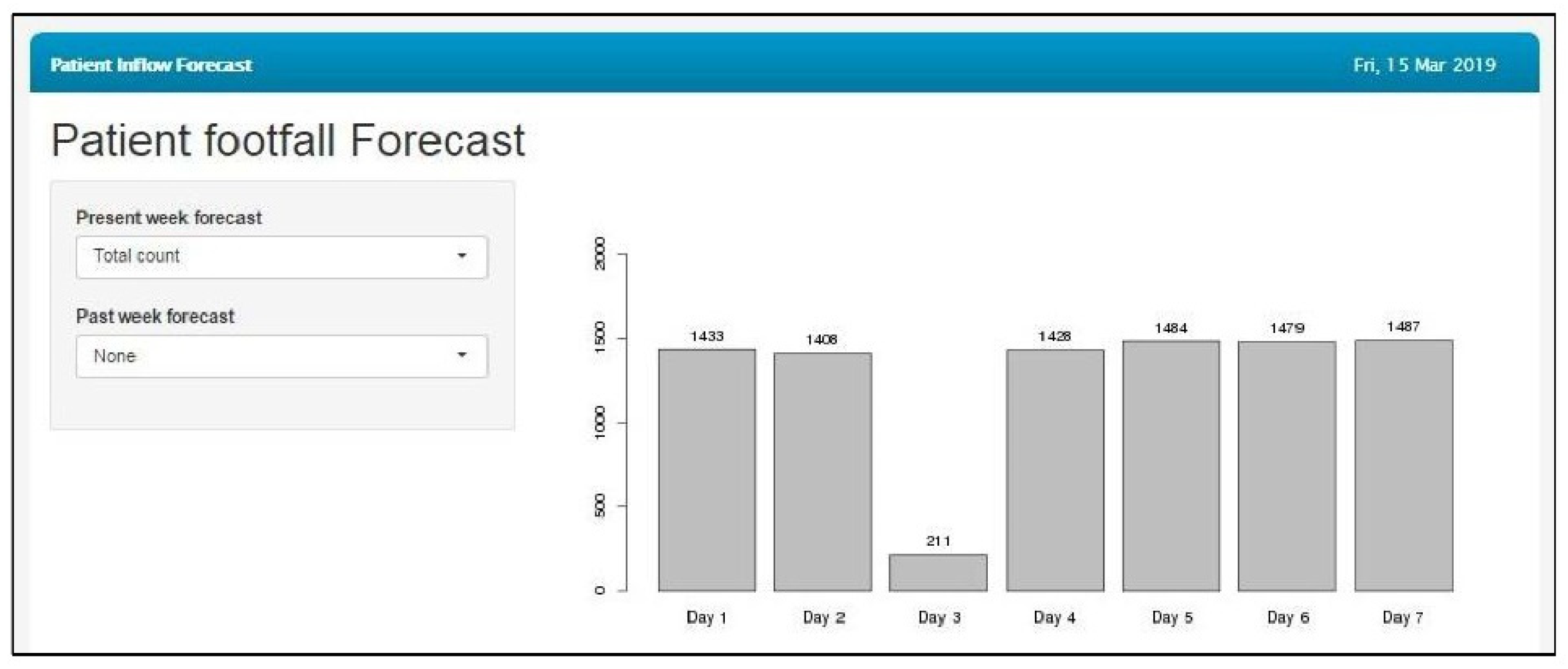
4.1. Principal Results
4.2. Comparison with Prior Works
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramos, I.; Cubillas, J.J.; Feito, F.R.; Ureña, T. Spatial analysis and prediction of the flow of patients to public health centres in a middle-sized Spanish city. Geospat. Health 2016, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, S.; Hamrock, E.; Toerper, M.; Siddiqui, S.; Levin, S. Real-time prediction of inpatient length of stay for discharge prioritization. JAMA 2016, 23, e2–e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaren, D.P.; Jones, R.; Plotnik, R.; Zareba, W.; McIntosh, S.; Alexis, J.; Chen, L.; Block, R.; Lowenstein, C.J.; Kutyifa, V. Prior hospital admission predicts thirty-day hospital readmission for heart failure patients. Cardiol. J. 2016, 23, 155–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, R.; Su, H.; Khalilia, M.; Lin, S.; Peng, Y.; Davis, T.; Hirsh, D.A.; Searles, E.; Tejedor-Sojo, J.; Thompson, M.; et al. Cloud-based Predictive Modeling System and its Application to Asthma Readmission Prediction. AMIA Annu. Symp. Proc. 2015, 5, 406–415. [Google Scholar]
- Zhao, J.; Henriksson, A.; Asker, L.; Boström, H. Predictive modeling of structured electronic health records for adverse drug event detection. BMC Med. Inform. Decis. Mak. 2015, 4, 1472–6947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vahdat, S.F.; Sarraf, A.; Shamsnia, A.; Shahidi, N. Prediction of monthly mean Inflow to Dez Dam reservoir using time series models (Box-jenkins). In Proceedings of the International Conference on Environment and Industrial Innovation, Sinagpore, 4–5 June 2011; Volume 12, pp. 162–166. [Google Scholar]
- Box, G.E.; Jenkins, G.M.; Reinsel, G.C.; Ljung, G.M. Time Series Analysis, Forecasting and Control, 4th ed.; Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Luo, L.; Luo, L.; Zhang, X.; He, X. Hospital daily outpatient visits forecasting using a combinatorial model based on ARIMA and SES models. BMC Health Serv. Res. 2017, 17, 469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calegari, R.; Fogliatto, F.S.; Lucini, F.R.; Neyeloff, J.; Kuchenbecker, R.S.; Schaan, B.D. Forecasting Daily Volume and Acuity of Patients in the Emergency Department. Comput. Math. Methods Med. 2016, 2016, 3863268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.; Xu, C.; Ji, M.; Xiang, W.; He, D. Medical service demand forecasting using a hybrid model based on ARIMA and self-adaptive filtering method. BMC Med. Inf. Decis. Mak. 2020, 20, 237. [Google Scholar] [CrossRef] [PubMed]
- Juang, W.C.; Huang, S.J.; Huang, F.D.; Cheng, P.W.; Wann, S.R. Application of time series analysis in modelling and forecasting emergency department visits in a medical centre in Southern Taiwan. BMJ Open 2017, 7, e018628. [Google Scholar] [CrossRef] [Green Version]
- Yuan, M.; Chen, W.; Wang, T.; Song, Y.; Zhu, Y.; Chen, C.; Yang, Y.; Liu, Y.; Li, Y.; Lin, H. Exploring the growth patterns of medical demand for eye care: A longitudinal hospital-level study over 10 years in China. Ann. Transl. Med. 2020, 8, 1374. [Google Scholar] [CrossRef]
- Huang, D.; Wu, Z. Forecasting outpatient visits using empirical mode decomposition coupled with back-propagation artificial neural networks optimized by particle swarm optimization. PLoS ONE 2017, 12, e0172539. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-R.; Park, J.-E.; Jang, I.-T. Outpatient forecasting model in spine hospital using ARIMA and SARIMA methods. J. Hosp. Manag. Health Policy 2020, 2020, 4. [Google Scholar] [CrossRef]
- Sumitra, I.D.; Basri, I. Forecasting the Number of Outpatient Patient Visits Using the ARIMA, SES And Holt-Winters Methods at XYZ Community Health Center. IOP Conf. Ser. Mater. Sci. Eng. 2020, 879, 012060. [Google Scholar] [CrossRef]
- Zhang, X.; Yu, Y.; Xiong, F.; Luo, L. Prediction of Daily Blood Sampling Room Visits Based on ARIMA and SES Model. Comput. Math. Methods Med. 2020, 2020, 1720134. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Zhao, P.; Wu, D.; Cheng, C.; Huang, H. Time series model for forecasting the number of new admission inpatients. BMC Med. Inf. Decis. Mak. 2018, 18, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | (0,0,0)(0,1,7)7 | (0,0,1)(0,1,7)7 | (1,0,0)(0,1,7)7 | (1,0,1)(0,1,7)7 |
|---|---|---|---|---|
| Male | 20,507.11 | 20,506.7 | 20,506.8 | 20,508.45 |
| Female | 20,002.47 | 19,996.45 | 19,996.72 | 19,998.37 |
| Pediatric | 16,727.46 | 16,729.34 | 16,729.33 | 16,726.48 |
| Adult | 20,513.51 | 20,515.45 | 20,515.46 | 20,517.45 |
| Elderly | 19,066.63 | 19,051.54 | 19,049.88 | 19,049.98 |
| Before time | 21,557.36 | 21,556.42 | 21,556.58 | 21,558.15 |
| Delayed | 19,089.98 | 19,083.4 | 19,083.14 | 19,084.94 |
| Total | 23,117.58 | 23,114.46 | 23,114.66 | 23,116.3 |
| Parameter | Mean Absolute Error | Root-Mean-Square Error | Mean Absolute Percentage Error |
|---|---|---|---|
| Male | 22.98 | 28.36 | 22.99% |
| Female | 17.53 | 24.58 | 17.03% |
| Pediatric | 11.84 | 15.07 | 62.75% |
| Adult | 19.97 | 26.62 | 18.36% |
| Elderly | 16.97 | 21.91 | 23.79% |
| Before time | 30.16 | 36.72 | 44.17% |
| Delayed | 22.36 | 27.10 | 18.56% |
| Total | 37.56 | 48.01 | 16.82% |
| Parameter | No. of Weeks (Error < 20%) |
|---|---|
| Male | 51 (98.07%) |
| Female | 50 (96.15%) |
| Delayed | 51 (98.07%) |
| Before time | 44 (84.61%) |
| Pediatric | 37 (71.15%) |
| Adult | 51 (98.07%) |
| Elderly | 51 (98.07%) |
| Total | 51 (98.07%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sai Prashanthi, G.; Molugu, N.; Kammari, P.; Vadapalli, R.; Das, A.V. Forecast of Outpatient Visits to a Tertiary Eyecare Network in India Using the EyeSmart Electronic Medical Record System. Healthcare 2021, 9, 749. https://doi.org/10.3390/healthcare9060749
Sai Prashanthi G, Molugu N, Kammari P, Vadapalli R, Das AV. Forecast of Outpatient Visits to a Tertiary Eyecare Network in India Using the EyeSmart Electronic Medical Record System. Healthcare. 2021; 9(6):749. https://doi.org/10.3390/healthcare9060749
Chicago/Turabian StyleSai Prashanthi, Gumpili, Nareen Molugu, Priyanka Kammari, Ranganath Vadapalli, and Anthony Vipin Das. 2021. "Forecast of Outpatient Visits to a Tertiary Eyecare Network in India Using the EyeSmart Electronic Medical Record System" Healthcare 9, no. 6: 749. https://doi.org/10.3390/healthcare9060749
APA StyleSai Prashanthi, G., Molugu, N., Kammari, P., Vadapalli, R., & Das, A. V. (2021). Forecast of Outpatient Visits to a Tertiary Eyecare Network in India Using the EyeSmart Electronic Medical Record System. Healthcare, 9(6), 749. https://doi.org/10.3390/healthcare9060749