
Lung Ultrasound in Pediatrics and Neonatology: An Update




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Principles of LUS
3. Normal and Abnormal Findings at LUS
4. Application of LUS in Pediatric Diseases
4.1. Pleural Effusions
4.2. Pneumothorax
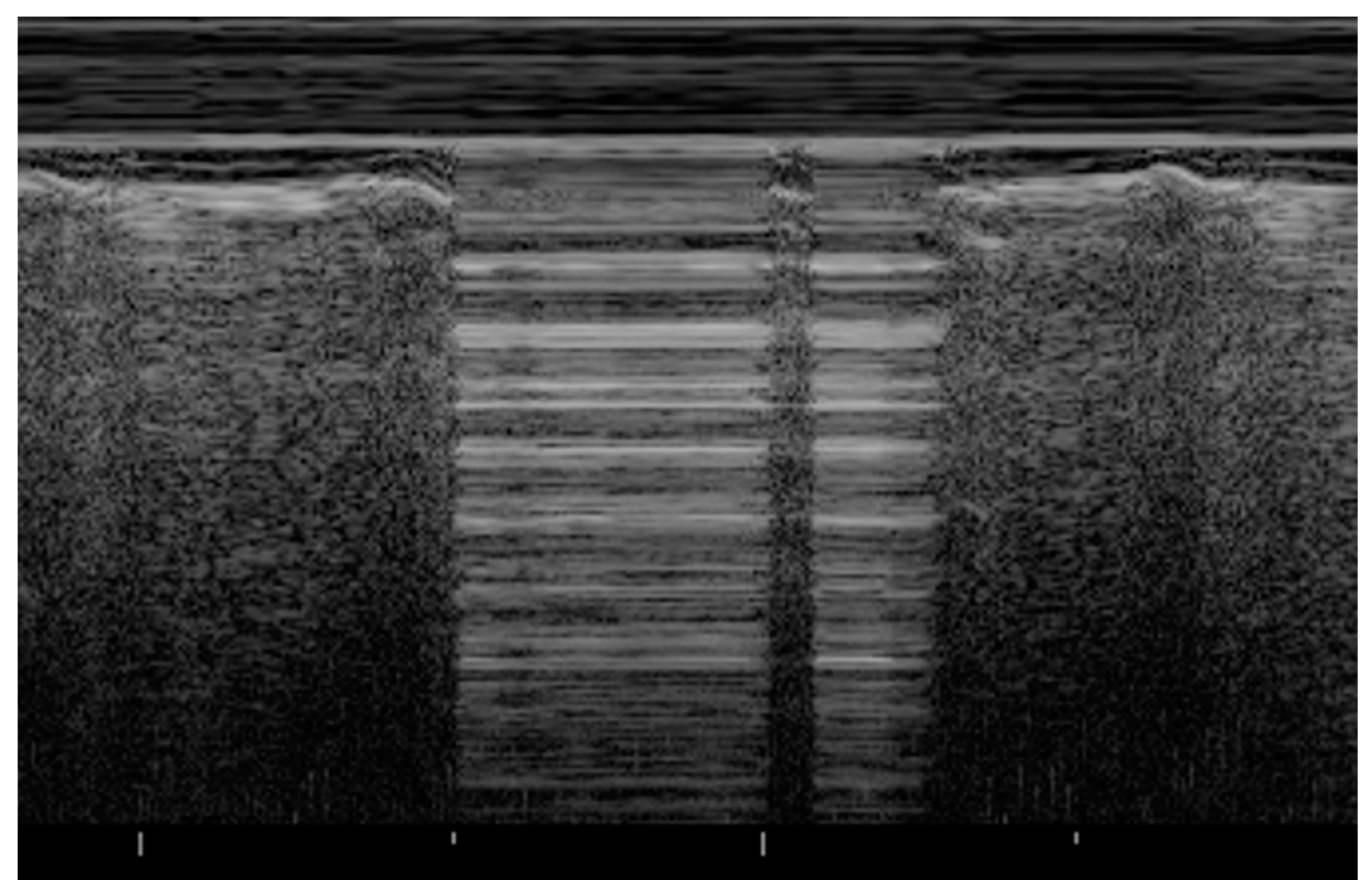
- Seashore sign (lateral): echogenic pleural line divides the image in the motionless part represented by horizontal lines (sea waves) and the part below that appear granular (sand) as the normal to-and-from motion of the lung is reflected over that area (normal lung sliding).
- Barcode sign (central): absence of a dynamic image, substituted by a static posterior acoustic shadowing (horizontal lines).
4.3. Pneumonia
4.4. Atelectasis
4.5. Congenital Lung Malformations
4.6. Congenital Diaphragmatic Hernia
4.7. Neonatal Pathologies
4.8. Bronchiolitis
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coley, B.D. Chest Sonography in Children: Current Indications, Techniques, and Imaging Findings. Radiol. Clin. N. Am. 2011, 49, 825–846. [Google Scholar] [CrossRef]
- Kurepa, D.; Zaghloul, N.; Watkins, L.; Liu, J. Neonatal Lung Ultrasound Exam Guidelines. J. Perinatol. 2018, 38, 11–22. [Google Scholar] [CrossRef]
- Liang, H.-Y.; Liang, X.-W.; Chen, Z.-Y.; Tan, X.-H.; Yang, H.-H.; Liao, J.-Y.; Cai, K.; Yu, J.-S. Ultrasound in Neonatal Lung Disease. Quant. Imaging Med. Surg. 2018, 8, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.-Y.; Sorantin, E. The basic principles of lung ultrasound. In Neonatal Lung Ultrasonography; Liu, J., Sorantin, E., Cao, H.-Y., Eds.; Springer: Dordrecht, The Netherlands, 2018; pp. 1–8. ISBN 978-94-024-1547-6. [Google Scholar]
- Iovine, E.; Nenna, R.; Bloise, S.; La Regina, D.P.; Pepino, D.; Petrarca, L.; Frassanito, A.; Lubrano, R.; Midulla, F. Lung Ultrasound: Its Findings and New Applications in Neonatology and Pediatric Diseases. Diagnostics 2021, 11, 625. [Google Scholar] [CrossRef] [PubMed]
- Moro, F.; Buonsenso, D.; Moruzzi, M.C.; Inchingolo, R.; Smargiassi, A.; Demi, L.; Larici, A.R.; Scambia, G.; Lanzone, A.; Testa, A.C. How to Perform Lung Ultrasound in Pregnant Women with Suspected COVID-19. Ultrasound Obstet. Gynecol. 2020, 55, 593–598. [Google Scholar] [CrossRef] [Green Version]
- Cattarossi, L. Lung Ultrasound: Diagnostic and Therapeutic Issues. Acta Biomed. 2014, 85, 25–29. [Google Scholar] [PubMed]
- Joshi, P.; Vasishta, A.; Gupta, M. Ultrasound of the Pediatric Chest. Br. J. Radiol. 2019, 92, 20190058. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Buda, N.; Ciuca, I.M.; Dong, Y.; Fang, C.; Feldkamp, A.; Jüngert, J.; Kosiak, W.; Mentzel, H.J.; Pienar, C.; et al. Lung Ultrasound in Children, WFUMB Review Paper (Part 2). Med. Ultrason. 2021. [Google Scholar] [CrossRef]
- Koh, D.-M.; Burke, S.; Davies, N.; Padley, S.P.G. Transthoracic US of the Chest: Clinical Uses and Applications. Radiographics 2002, 22, e1. [Google Scholar] [CrossRef]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International Evidence-Based Recommendations for Point-of-Care Lung Ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [Green Version]
- Soldati, G.; Smargiassi, A.; Inchingolo, R.; Buonsenso, D.; Perrone, T.; Briganti, D.F.; Perlini, S.; Torri, E.; Mariani, A.; Mossolani, E.E.; et al. Proposal for International Standardization of the Use of Lung Ultrasound for Patients With COVID-19: A Simple, Quantitative, Reproducible Method. J. Ultrasound Med. 2020, 39, 1413–1419. [Google Scholar] [CrossRef] [Green Version]
- Gargani, L.; Volpicelli, G. How I Do It: Lung Ultrasound. Cardiovasc. Ultrasound 2014, 12, 25. [Google Scholar] [CrossRef] [Green Version]
- Rath, C.; Suryawanshi, P. Point of Care Neonatal Ultrasound—Head, Lung, Gut and Line Localization. Indian Pediatr. 2016, 53, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Soni, N.J.; Franco, R.; Velez, M.I.; Schnobrich, D.; Dancel, R.; Restrepo, M.I.; Mayo, P.H. Ultrasound in the Diagnosis and Management of Pleural Effusions. J. Hosp. Med. 2015, 10, 811–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kocijancic, I.; Vidmar, K.; Ivanovi-Herceg, Z. Chest Sonography versus Lateral Decubitus Radiography in the Diagnosis of Small Pleural Effusions. J. Clin. Ultrasound 2003, 31, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Trinavarat, P.; Riccabona, M. Potential of Ultrasound in the Pediatric Chest. Eur. J. Radiol. 2014, 83, 1507–1518. [Google Scholar] [CrossRef]
- Yang, P.C.; Luh, K.T.; Chang, D.B.; Wu, H.D.; Yu, C.J.; Kuo, S.H. Value of Sonography in Determining the Nature of Pleural Effusion: Analysis of 320 Cases. AJR Am. J. Roentgenol. 1992, 159, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Ramnath, R.R.; Heller, R.M.; Ben-Ami, T.; Miller, M.A.; Campbell, P.; Neblett, W.W.; Holcomb, G.W.; Hernanz-Schulman, M. Implications of Early Sonographic Evaluation of Parapneumonic Effusions in Children with Pneumonia. Pediatrics 1998, 101, 68–71. [Google Scholar] [CrossRef]
- Calder, A.; Owens, C.M. Imaging of Parapneumonic Pleural Effusions and Empyema in Children. Pediatr. Radiol. 2009, 39, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Supakul, N.; Karmazyn, B. Ultrasound of the Pediatric Chest—The Ins and Outs. Semin. Ultrasound CT MR 2013, 34, 274–285. [Google Scholar] [CrossRef]
- Feldman, M.K.; Katyal, S.; Blackwood, M.S. US Artifacts. Radiographics 2009, 29, 1179–1189. [Google Scholar] [CrossRef]
- Cattarossi, L.; Copetti, R.; Brusa, G.; Pintaldi, S. Lung Ultrasound Diagnostic Accuracy in Neonatal Pneumothorax. Can. Respir. J. 2016, 2016, 6515069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahmarde, H.; Parooie, F.; Salarzaei, M. Accuracy of Ultrasound in Diagnosis of Pneumothorax: A Comparison between Neonates and Adults-A Systematic Review and Meta-Analysis. Can. Respir. J. 2019, 2019, 5271982. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D.A.; Menu, Y. A Bedside Ultrasound Sign Ruling out Pneumothorax in the Critically Ill. Lung Sliding. Chest 1995, 108, 1345–1348. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D.; Mezière, G.; Biderman, P.; Gepner, A. The “Lung Point”: An Ultrasound Sign Specific to Pneumothorax. Intensive Care Med. 2000, 26, 1434–1440. [Google Scholar] [CrossRef]
- Duke, T. Neonatal Pneumonia in Developing Countries. Arch. Dis. Child. Fetal Neonatal Ed. 2005, 90, F211–F219. [Google Scholar] [CrossRef] [PubMed]
- Pereda, M.A.; Chavez, M.A.; Hooper-Miele, C.C.; Gilman, R.H.; Steinhoff, M.C.; Ellington, L.E.; Gross, M.; Price, C.; Tielsch, J.M.; Checkley, W. Lung Ultrasound for the Diagnosis of Pneumonia in Children: A Meta-Analysis. Pediatrics 2015, 135, 714–722. [Google Scholar] [CrossRef] [Green Version]
- Jaworska, J.; Komorowska-Piotrowska, A.; Pomiećko, A.; Wiśniewski, J.; Woźniak, M.; Littwin, B.; Kryger, M.; Kwaśniewicz, P.; Szczyrski, J.; Kulińska-Szukalska, K.; et al. Consensus on the Application of Lung Ultrasound in Pneumonia and Bronchiolitis in Children. Diagnostics 2020, 10, 935. [Google Scholar] [CrossRef] [PubMed]
- Nissen, M.D. Congenital and Neonatal Pneumonia. Paediatr. Respir. Rev. 2007, 8, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Balk, D.S.; Lee, C.; Schafer, J.; Welwarth, J.; Hardin, J.; Novack, V.; Yarza, S.; Hoffmann, B. Lung Ultrasound Compared to Chest X-Ray for Diagnosis of Pediatric Pneumonia: A Meta-Analysis. Pediatr. Pulmonol. 2018, 53, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Song, W.; Wang, Y.; Han, J.; Lv, K. Lung Ultrasonography versus Chest Radiography for the Diagnosis of Pediatric Community Acquired Pneumonia in Emergency Department: A Meta-Analysis. J. Thorac. Dis. 2019, 11, 5107–5114. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.P.; Tunik, M.G.; Tsung, J.W. Prospective Evaluation of Point-of-Care Ultrasonography for the Diagnosis of Pneumonia in Children and Young Adults. JAMA Pediatr. 2013, 167, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Chavez, M.A.; Naithani, N.; Gilman, R.H.; Tielsch, J.M.; Khatry, S.; Ellington, L.E.; Miranda, J.J.; Gurung, G.; Rodriguez, S.; Checkley, W. Agreement Between the World Health Organization Algorithm and Lung Consolidation Identified Using Point-of-Care Ultrasound for the Diagnosis of Childhood Pneumonia by General Practitioners. Lung 2015, 193, 531–538. [Google Scholar] [CrossRef]
- Liu, J.; Liu, F.; Liu, Y.; Wang, H.-W.; Feng, Z.-C. Lung Ultrasonography for the Diagnosis of Severe Neonatal Pneumonia. Chest 2014, 146, 383–388. [Google Scholar] [CrossRef]
- Reali, F.; Sferrazza Papa, G.F.; Carlucci, P.; Fracasso, P.; Di Marco, F.; Mandelli, M.; Soldi, S.; Riva, E.; Centanni, S. Can Lung Ultrasound Replace Chest Radiography for the Diagnosis of Pneumonia in Hospitalized Children? Respiration 2014, 88, 112–115. [Google Scholar] [CrossRef]
- Iorio, G.; Capasso, M.; De Luca, G.; Prisco, S.; Mancusi, C.; Laganà, B.; Comune, V. Lung Ultrasound in the Diagnosis of Pneumonia in Children: Proposal for a New Diagnostic Algorithm. PeerJ 2015, 3, e1374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omran, A.; Eesai, S.; Ibrahim, M.; El-Sharkawy, S. Lung Ultrasound in Diagnosis and Follow up of Community Acquired Pneumonia in Infants Younger than 1-Year Old. Clin. Respir. J. 2018, 12, 2204–2211. [Google Scholar] [CrossRef] [PubMed]
- Boursiani, C.; Tsolia, M.; Koumanidou, C.; Malagari, A.; Vakaki, M.; Karapostolakis, G.; Mazioti, A.; Alexopoulou, E. Lung Ultrasound as First-Line Examination for the Diagnosis of Community-Acquired Pneumonia in Children. Pediatr. Emerg. Care 2017, 33, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, H.L.; Özkaya, A.K.; Sarı Gökay, S.; Tolu Kendir, Ö.; Şenol, H. Point-of-Care Lung Ultrasound in Children with Community Acquired Pneumonia. Am. J. Emerg. Med. 2017, 35, 964–969. [Google Scholar] [CrossRef]
- Copetti, R.; Cattarossi, L. Ultrasound Diagnosis of Pneumonia in Children. Radiol. Med. 2008, 113, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Maughan, B.C.; Asselin, N.; Carey, J.L.; Sucov, A.; Valente, J.H. False-Negative Chest Radiographs in Emergency Department Diagnosis of Pneumonia. Rhode Isl. Med. J. 2014, 97, 20–23. [Google Scholar]
- Williams, G.J.; Macaskill, P.; Kerr, M.; Fitzgerald, D.A.; Isaacs, D.; Codarini, M.; McCaskill, M.; Prelog, K.; Craig, J.C. Variability and Accuracy in Interpretation of Consolidation on Chest Radiography for Diagnosing Pneumonia in Children under 5 Years of Age. Pediatr. Pulmonol. 2013, 48, 1195–1200. [Google Scholar] [CrossRef]
- Johnson, J.; Kline, J.A. Intraobserver and Interobserver Agreement of the Interpretation of Pediatric Chest Radiographs. Emerg. Radiol. 2010, 17, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Urbankowska, E.; Krenke, K.; Drobczyński, Ł.; Korczyński, P.; Urbankowski, T.; Krawiec, M.; Kraj, G.; Brzewski, M.; Kulus, M. Lung Ultrasound in the Diagnosis and Monitoring of Community Acquired Pneumonia in Children. Respir. Med. 2015, 109, 1207–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloise, S.; La Regina, D.P.; Pepino, D.; Iovine, E.; Laudisa, M.; Di Mattia, G.; Nicolai, A.; Nenna, R.; Petrarca, L.; Mancino, E.; et al. Lung Ultrasound Compared to Chest X-Ray for the Diagnosis of CAP in Children. Pediatr. Int. 2021, 63, 448–453. [Google Scholar] [CrossRef]
- Lai, S.-H.; Wong, K.-S.; Liao, S.-L. Value of Lung Ultrasonography in the Diagnosis and Outcome Prediction of Pediatric Community-Acquired Pneumonia with Necrotizing Change. PLoS ONE 2015, 10, e0130082. [Google Scholar] [CrossRef] [PubMed]
- Riccabona, M. Ultrasound of the Chest in Children (Mediastinum Excluded). Eur. Radiol. 2008, 18, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Tan Kendrick, A.P.; Ling, H.; Subramaniam, R.; Joseph, V.T. The Value of Early CT in Complicated Childhood Pneumonia. Pediatr. Radiol. 2002, 32, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Kurian, J.; Levin, T.L.; Han, B.K.; Taragin, B.H.; Weinstein, S. Comparison of Ultrasound and CT in the Evaluation of Pneumonia Complicated by Parapneumonic Effusion in Children. AJR Am. J. Roentgenol. 2009, 193, 1648–1654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajalioghli, P.; Nemati, M.; Dinparast Saleh, L.; Fouladi, D.F. Can Chest Computed Tomography Be Replaced by Lung Ultrasonography with or without Plain Chest Radiography in Pediatric Pneumonia? J. Thorac. Imaging 2016, 31, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Kharasch, S.; Duggan, N.M.; Cohen, A.R.; Shokoohi, H. Lung Ultrasound in Children with Respiratory Tract Infections: Viral, Bacterial or COVID-19? A Narrative Review. Open Access Emerg. Med. 2020, 12, 275–285. [Google Scholar] [CrossRef]
- Malla, D.; Rathi, V.; Gomber, S.; Upreti, L. Can Lung Ultrasound Differentiate between Bacterial and Viral Pneumonia in Children? J. Clin. Ultrasound 2020, 49, 91–100. [Google Scholar] [CrossRef]
- Tsung, J.W.; Kessler, D.O.; Shah, V.P. Prospective Application of Clinician-Performed Lung Ultrasonography during the 2009 H1N1 Influenza A Pandemic: Distinguishing Viral from Bacterial Pneumonia. Crit. Ultrasound J. 2012, 4, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hizal, M.; Aykac, K.; Yayla, B.C.C.; Yilmaz, A.; Altun, D.; Akkaya, H.E.; Bayhan, G.I.; Kurt, A.N.C.; Karakaya, J.; Ozsurekci, Y.; et al. Diagnostic Value of Lung Ultrasonography in Children with COVID-19. Pediatr. Pulmonol. 2021, 56, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F. Systematic Review of COVID-19 in Children Shows Milder Cases and a Better Prognosis than Adults. Acta Paediatr. 2020, 109, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Gregorio-Hernández, R.; Escobar-Izquierdo, A.B.; Cobas-Pazos, J.; Martínez-Gimeno, A. Point-of-Care Lung Ultrasound in Three Neonates with COVID-19. Eur. J. Pediatr. 2020, 179, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Guitart, C.; Suárez, R.; Girona, M.; Bobillo-Perez, S.; Hernández, L.; Balaguer, M.; Cambra, F.J.; Jordan, I.; KIDS-Corona Study Group. Kids Corona Platform Lung Ultrasound Findings in Pediatric Patients with COVID-19. Eur. J. Pediatr. 2021, 180, 1117–1123. [Google Scholar] [CrossRef]
- Denina, M.; Scolfaro, C.; Silvestro, E.; Pruccoli, G.; Mignone, F.; Zoppo, M.; Ramenghi, U.; Garazzino, S. Lung Ultrasound in Children With COVID-19. Pediatrics 2020, 146, e20201157. [Google Scholar] [CrossRef] [Green Version]
- Musolino, A.M.; Supino, M.C.; Buonsenso, D.; Ferro, V.; Valentini, P.; Magistrelli, A.; Lombardi, M.H.; Romani, L.; D’Argenio, P.; Campana, A.; et al. Lung Ultrasound in Children with COVID-19: Preliminary Findings. Ultrasound Med. Biol. 2020, 46, 2094–2098. [Google Scholar] [CrossRef]
- Kennedy, T.M.; Malia, L.; Dessie, A.; Kessler, D.O.; Ng, L.; Chiang, E.L.; Rabiner, J.E. Lung Point-of-Care Ultrasound in Pediatric COVID-19: A Case Series. Pediatr. Emerg. Care 2020, 36, 544–548. [Google Scholar] [CrossRef] [PubMed]
- Türe, E.; Korkmaz, M.F.; Aksoy, F.D.; Ceylan Demirtaş, B.; Menekşe, B.; Çiftçi, M.; Korkmaz, M. Point-of-Care Lung Ultrasound Findings in the Pediatric Emergency Clinic during the COVID-19 Pandemic. J. Clin. Ultrasound 2020, 49, 85–90. [Google Scholar] [CrossRef]
- Pare, J.R.; Camelo, I.; Mayo, K.C.; Leo, M.M.; Dugas, J.N.; Nelson, K.P.; Baker, W.E.; Shareef, F.; Mitchell, P.M.; Schechter-Perkins, E.M. Point-of-Care Lung Ultrasound Is More Sensitive than Chest Radiograph for Evaluation of COVID-19. West. J. Emerg. Med. 2020, 21, 771–778. [Google Scholar] [CrossRef]
- Lichtenstein, D.A.; Lascols, N.; Prin, S.; Mezière, G. The “Lung Pulse”: An Early Ultrasound Sign of Complete Atelectasis. Intensive Care Med. 2003, 29, 2187–2192. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Chen, S.-W.; Liu, F.; Li, Q.-P.; Kong, X.-Y.; Feng, Z.-C. The Diagnosis of Neonatal Pulmonary Atelectasis Using Lung Ultrasonography. Chest 2015, 147, 1013–1019. [Google Scholar] [CrossRef]
- Acosta, C.M.; Maidana, G.A.; Jacovitti, D.; Belaunzarán, A.; Cereceda, S.; Rae, E.; Molina, A.; Gonorazky, S.; Bohm, S.H.; Tusman, G. Accuracy of Transthoracic Lung Ultrasound for Diagnosing Anesthesia-Induced Atelectasis in Children. Anesthesiology 2014, 120, 1370–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, B. Congenital Bronchopulmonary Foregut Malformations: Concepts and Controversies. Pediatr. Radiol. 2006, 36, 773–791. [Google Scholar] [CrossRef] [PubMed]
- Quercia, M.; Panza, R.; Calderoni, G.; Di Mauro, A.; Laforgia, N. Lung Ultrasound: A New Tool in the Management of Congenital Lung Malformation. Am. J. Perinatol. 2019, 36, S99–S105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, B. Magnetic Resonance Imaging for Congenital Lung Malformations. Pediatr. Radiol. 2021, 1–11. [Google Scholar] [CrossRef]
- Annunziata, F.; Bush, A.; Borgia, F.; Raimondi, F.; Montella, S.; Poeta, M.; Borrelli, M.; Santamaria, F. Congenital Lung Malformations: Unresolved Issues and Unanswered Questions. Front. Pediatr. 2019, 7, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waelti, S.L.; Garel, L.; Soglio, D.D.; Rypens, F.; Messerli, M.; Dubois, J. Neonatal Congenital Lung Tumors—The Importance of Mid-Second-Trimester Ultrasound as a Diagnostic Clue. Pediatr. Radiol. 2017, 47, 1766–1775. [Google Scholar] [CrossRef] [PubMed]
- David, M.; Lamas-Pinheiro, R.; Henriques-Coelho, T. Prenatal and Postnatal Management of Congenital Pulmonary Airway Malformation. Neonatology 2016, 110, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Merli, L.; Nanni, L.; Curatola, A.; Pellegrino, M.; De Santis, M.; Silvaroli, S.; Paradiso, F.V.; Buonsenso, D. Congenital Lung Malformations: A Novel Application for Lung Ultrasound? J. Ultrasound 2019, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Yousef, N.; Mokhtari, M.; Durand, P.; Raimondi, F.; Migliaro, F.; Letourneau, A.; Tissières, P.; De Luca, D. Lung Ultrasound Findings in Congenital Pulmonary Airway Malformation. Am. J. Perinatol. 2018, 35, 1222–1227. [Google Scholar] [CrossRef]
- Gallot, D.; Coste, K.; Francannet, C.; Laurichesse, H.; Boda, C.; Ughetto, S.; Vanlieferinghen, P.; Scheye, T.; Vendittelli, F.; Labbe, A.; et al. Antenatal Detection and Impact on Outcome of Congenital Diaphragmatic Hernia: A 12-Year Experience in Auvergne, France. Eur. J. Obstet. Gynecol. Reprod. Biol. 2006, 125, 202–205. [Google Scholar] [CrossRef]
- Desjardins, M.P.; Weerdenburg, K.D.; Fischer, J.W. Emergency Point-of-Care Ultrasound Diagnosis of Diaphragmatic Hernia in the Pediatric Emergency Department. Pediatr. Emerg. Care 2016, 32, 685–687. [Google Scholar] [CrossRef] [PubMed]
- Rankin, J.H.; Elkhunovich, M.; Seif, D.; Chilstrom, M. Point-of-Care Ultrasound Diagnosis of Diaphragmatic Hernia in an Infant With Respiratory Distress. Pediatr. Emerg. Care 2016, 32, 731–733. [Google Scholar] [CrossRef]
- Corsini, I.; Parri, N.; Coviello, C.; Leonardi, V.; Dani, C. Lung Ultrasound Findings in Congenital Diaphragmatic Hernia. Eur. J. Pediatr. 2019, 178, 491–495. [Google Scholar] [CrossRef]
- Aichhorn, L.; Küng, E.; Habrina, L.; Werther, T.; Berger, A.; Urlesberger, B.; Schwaberger, B. The Role of Lung Ultrasound in the Management of the Critically Ill Neonate—A Narrative Review and Practical Guide. Children 2021, 8, 628. [Google Scholar] [CrossRef]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; Te Pas, A.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; Simeoni, U.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome—2019 Update. Neonatology 2019, 115, 432–450. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, A.; Gaspar, H.A.; Preto, M.; Ejzenberg, F.E. Point-of-Care Lung Ultrasound in Paediatric Critical and Emergency Care. J. Paediatr. Child Health 2018, 54, 945–952. [Google Scholar] [CrossRef]
- Brat, R.; Yousef, N.; Klifa, R.; Reynaud, S.; Shankar Aguilera, S.; De Luca, D. Lung Ultrasonography Score to Evaluate Oxygenation and Surfactant Need in Neonates Treated with Continuous Positive Airway Pressure. JAMA Pediatr. 2015, 169, e151797. [Google Scholar] [CrossRef] [Green Version]
- Gregorio-Hernández, R.; Arriaga-Redondo, M.; Pérez-Pérez, A.; Ramos-Navarro, C.; Sánchez-Luna, M. Lung Ultrasound in Preterm Infants with Respiratory Distress: Experience in a Neonatal Intensive Care Unit. Eur. J. Pediatr. 2020, 179, 81–89. [Google Scholar] [CrossRef]
- Liu, J.; Wang, Y.; Fu, W.; Yang, C.-S.; Huang, J.-J. Diagnosis of Neonatal Transient Tachypnea and Its Differentiation from Respiratory Distress Syndrome Using Lung Ultrasound. Medicine 2014, 93, e197. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Chen, X.-X.; Li, X.-W.; Chen, S.-W.; Wang, Y.; Fu, W. Lung Ultrasonography to Diagnose Transient Tachypnea of the Newborn. Chest 2016, 149, 1269–1275. [Google Scholar] [CrossRef] [PubMed]
- Vergine, M.; Copetti, R.; Brusa, G.; Cattarossi, L. Lung Ultrasound Accuracy in Respiratory Distress Syndrome and Transient Tachypnea of the Newborn. Neonatology 2014, 106, 87–93. [Google Scholar] [CrossRef]
- Copetti, R.; Cattarossi, L. The “Double Lung Point”: An Ultrasound Sign Diagnostic of Transient Tachypnea of the Newborn. Neonatology 2007, 91, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Piastra, M.; Yousef, N.; Brat, R.; Manzoni, P.; Mokhtari, M.; De Luca, D. Lung Ultrasound Findings in Meconium Aspiration Syndrome. Early Hum. Dev. 2014, 90 (Suppl. 2), S41–S43. [Google Scholar] [CrossRef]
- Mosca, F.; Colnaghi, M.; Fumagalli, M. BPD: Old and New Problems. J. Matern. Fetal Neonatal Med. 2011, 24 (Suppl. 1), 80–82. [Google Scholar] [CrossRef]
- Gao, S.; Xiao, T.; Ju, R.; Ma, R.; Zhang, X.; Dong, W. The Application Value of Lung Ultrasound Findings in Preterm Infants with Bronchopulmonary Dysplasia. Transl. Pediatr. 2020, 9, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Loi, B.; Vigo, G.; Baraldi, E.; Raimondi, F.; Carnielli, V.P.; Mosca, F.; De Luca, D. Lung Ultrasound to Monitor Extremely Preterm Infants and Predict Bronchopulmonary Dysplasia. A Multicenter Longitudinal Cohort Study. Am. J. Respir. Crit. Care Med. 2021, 203, 1398–1409. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.; Mohsen, N.; Diambomba, Y.; Lashin, A.; Louis, D.; Elsayed, Y.; Shah, P.S. Lung Ultrasound for Prediction of Bronchopulmonary Dysplasia in Extreme Preterm Neonates: A Prospective Diagnostic Cohort Study. J. Pediatr. 2021. [Google Scholar] [CrossRef] [PubMed]
- Oulego-Erroz, I.; Alonso-Quintela, P.; Terroba-Seara, S.; Jiménez-González, A.; Rodríguez-Blanco, S. Early Assessment of Lung Aeration Using an Ultrasound Score as a Biomarker of Developing Bronchopulmonary Dysplasia: A Prospective Observational Study. J. Perinatol. 2021, 41, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Ojembarrena, A.; Serna-Guerediaga, I.; Aldecoa-Bilbao, V.; Gregorio-Hernández, R.; Alonso-Quintela, P.; Concheiro-Guisán, A.; Ramos-Rodríguez, A.; Heras-Martín, M.D.L.; Rodeño-Fernández, L.; Oulego-Erroz, I. The Predictive Value of Lung Ultrasound Scores in Developing Bronchopulmonary Dysplasia: A Prospective Multicenter Diagnostic Accuracy Study. Chest 2021. [Google Scholar] [CrossRef]
- Zahr, R.A.; Ashfaq, A.; Marron-Corwin, M. Neonatal Pulmonary Hemorrhage. Neoreviews 2012, 13, e302–e306. [Google Scholar] [CrossRef] [Green Version]
- Lovrenski, J. Lung Ultrasonography of Pulmonary Complications in Preterm Infants with Respiratory Distress Syndrome. Ups. J. Med. Sci. 2012, 117, 10–17. [Google Scholar] [CrossRef]
- Ren, X.-L.; Fu, W.; Liu, J.; Liu, Y.; Xia, R.-M. Lung Ultrasonography to Diagnose Pulmonary Hemorrhage of the Newborn. J. Matern. Fetal Neonatal Med. 2017, 30, 2601–2606. [Google Scholar] [CrossRef]
- Meissner, H.C. Viral Bronchiolitis in Children. N. Engl. J. Med. 2016, 374, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Ralston, S.L.; Lieberthal, A.S.; Meissner, H.C.; Alverson, B.K.; Baley, J.E.; Gadomski, A.M.; Johnson, D.W.; Light, M.J.; Maraqa, N.F.; Mendonca, E.A.; et al. Clinical Practice Guideline: The Diagnosis, Management, and Prevention of Bronchiolitis. Pediatrics 2014, 134, e1474–e1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuh, S.; Lalani, A.; Allen, U.; Manson, D.; Babyn, P.; Stephens, D.; MacPhee, S.; Mokanski, M.; Khaikin, S.; Dick, P. Evaluation of the Utility of Radiography in Acute Bronchiolitis. J. Pediatr. 2007, 150, 429–433. [Google Scholar] [CrossRef]
- Di Mauro, A.; Ammirabile, A.; Quercia, M.; Panza, R.; Capozza, M.; Manzionna, M.M.; Laforgia, N. Acute Bronchiolitis: Is There a Role for Lung Ultrasound? Diagnostics 2019, 9, 172. [Google Scholar] [CrossRef] [Green Version]
- Caiulo, V.A.; Gargani, L.; Caiulo, S.; Fisicaro, A.; Moramarco, F.; Latini, G.; Picano, E. Lung Ultrasound in Bronchiolitis: Comparison with Chest X-Ray. Eur. J. Pediatr. 2011, 170, 1427–1433. [Google Scholar] [CrossRef]
- Jaszczołt, S.; Polewczyk, T.; Dołęga-Kozierowska, M.; Woźniak, M.; Doniec, Z. Comparison of Lung Ultrasound and Chest X-Ray Findings in Children with Bronchiolitis. J. Ultrason. 2018, 18, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Di Mauro, A.; Cappiello, A.R.; Ammirabile, A.; Abbondanza, N.; Bianchi, F.P.; Tafuri, S.; Manzionna, M.M. Lung Ultrasound and Clinical Progression of Acute Bronchiolitis: A Prospective Observational Single-Center Study. Medicina 2020, 56, 314. [Google Scholar] [CrossRef] [PubMed]
- Basile, V.; Di Mauro, A.; Scalini, E.; Comes, P.; Lofù, I.; Mostert, M.; Tafuri, S.; Manzionna, M.M. Lung Ultrasound: A Useful Tool in Diagnosis and Management of Bronchiolitis. BMC Pediatr. 2015, 15, 63. [Google Scholar] [CrossRef] [Green Version]
- Taveira, M.; Yousef, N.; Miatello, J.; Roy, C.; Claude, C.; Boutillier, B.; Dubois, C.; Pierre, A.F.; Tissières, P.; Durand, P. Can a Simple Lung Ultrasound Score Predict Length of Ventilation for Infants with Severe Acute Viral Bronchiolitis? Arch. Pediatr. 2018, 25, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Zoido Garrote, E.; García Aparicio, C.; Camila Torrez Villarroel, C.; Pedro Vega García, A.; Muñiz Fontán, M.; Oulego Erroz, I. Usefulness of Early Lung Ultrasound in Acute Mild–Moderate Acute Bronchiolitis. A Pilot Study. An. Pediatr. 2019, 90, 10–18. [Google Scholar] [CrossRef] [PubMed]
- La Regina, D.P.; Bloise, S.; Pepino, D.; Iovine, E.; Laudisa, M.; Cristiani, L.; Nicolai, A.; Nenna, R.; Mancino, E.; Di Mattia, G.; et al. Lung Ultrasound in Bronchiolitis. Pediatr. Pulmonol. 2021, 56, 234–239. [Google Scholar] [CrossRef]
- Bueno-Campaña, M.; Sainz, T.; Alba, M.; Del Rosal, T.; Mendez-Echevarría, A.; Echevarria, R.; Tagarro, A.; Ruperez-Lucas, M.; Herrreros, M.L.; Latorre, L.; et al. Lung Ultrasound for Prediction of Respiratory Support in Infants with Acute Bronchiolitis: A Cohort Study. Pediatr. Pulmonol. 2019, 54, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Supino, M.C.; Giglioni, E.; Battaglia, M.; Mesturino, A.; Scateni, S.; Scialanga, B.; Reale, A.; Musolino, A.M.C. Point of Care Diaphragm Ultrasound in Infants with Bronchiolitis: A Prospective Study. Pediatr. Pulmonol. 2018, 53, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Biagi, C.; Pierantoni, L.; Baldazzi, M.; Greco, L.; Dormi, A.; Dondi, A.; Faldella, G.; Lanari, M. Lung Ultrasound for the Diagnosis of Pneumonia in Children with Acute Bronchiolitis. BMC Pulm. Med. 2018, 18, 191. [Google Scholar] [CrossRef] [Green Version]
- Avni, E.F.; Braude, P.; Pardou, A.; Matos, C. Hyaline Membrane Disease in the Newborn: Diagnosis by Ultrasound. Pediatr. Radiol. 1990, 20, 143–146. [Google Scholar] [CrossRef]
- Copetti, R.; Cattarossi, L.; Macagno, F.; Violino, M.; Furlan, R. Lung Ultrasound in Respiratory Distress Syndrome: A Useful Tool for Early Diagnosis. Neonatology 2008, 94, 52–59. [Google Scholar] [CrossRef]
- Singh, Y.; Tissot, C.; Fraga, M.V.; Yousef, N.; Cortes, R.G.; Lopez, J.; Sanchez-de-Toledo, J.; Brierley, J.; Colunga, J.M.; Raffaj, D.; et al. International Evidence-Based Guidelines on Point of Care Ultrasound (POCUS) for Critically Ill Neonates and Children Issued by the POCUS Working Group of the European Society of Paediatric and Neonatal Intensive Care (ESPNIC). Crit. Care 2020, 24, 65. [Google Scholar] [CrossRef] [Green Version]
- Girona-Alarcón, M.; Cuaresma-González, A.; Rodríguez-Fanjul, J.; Bobillo-Perez, S.; Inarejos, E.; Sánchez-de-Toledo, J.; Jordan, I.; Balaguer, M. LUCAS (Lung Ultrasonography in Cardiac Surgery) Score to Monitor Pulmonary Edema after Congenital Cardiac Surgery in Children. J. Matern. Fetal Neonatal Med. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Cantinotti, M.; Giordano, R.; Scalese, M.; Marchese, P.; Franchi, E.; Viacava, C.; Molinaro, S.; Assanta, N.; Koestenberger, M.; Kutty, S.; et al. Prognostic Value of a New Lung Ultrasound Score to Predict Intensive Care Unit Stay in Pediatric Cardiac Surgery. Ann. Thorac. Surg. 2020, 109, 178–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razak, A.; Faden, M. Neonatal Lung Ultrasonography to Evaluate Need for Surfactant or Mechanical Ventilation: A Systematic Review and Meta-Analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2020, 105, 164–171. [Google Scholar] [CrossRef]
- Raimondi, F.; Yousef, N.; Migliaro, F.; Capasso, L.; De Luca, D. Point-of-Care Lung Ultrasound in Neonatology: Classification into Descriptive and Functional Applications. Pediatr. Res. 2018, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Buonsenso, D.; Pata, D.; Chiaretti, A. COVID-19 Outbreak: Less Stethoscope, More Ultrasound. Lancet Respir. Med. 2020, 8, e27. [Google Scholar] [CrossRef] [Green Version]
- Monti, J.D.; Younggren, B.; Blankenship, R. Ultrasound Detection of Pneumothorax with Minimally Trained Sonographers: A Preliminary Study. J. Spec. Oper. Med. 2009, 9, 43–46. [Google Scholar]
- Buonsenso, D.; De Rose, C. Implementation of Lung Ultrasound in Low- to Middle-Income Countries: A New Challenge Global Health? Eur. J. Pediatr. 2021, 1–8. [Google Scholar] [CrossRef]
- Catalano, D.; Trovato, G.; Sperandeo, M.; Sacco, M.C. Lung Ultrasound in Pediatric Pneumonia. The Persistent Need of Chest X-Rays. Pediatr. Pulmonol. 2014, 49, 617–618. [Google Scholar] [CrossRef] [PubMed]
- Tsou, P.-Y.; Chen, K.P.; Wang, Y.-H.; Fishe, J.; Gillon, J.; Lee, C.-C.; Deanehan, J.K.; Kuo, P.-L.; Yu, D.T.Y. Diagnostic Accuracy of Lung Ultrasound Performed by Novice Versus Advanced Sonographers for Pneumonia in Children: A Systematic Review and Meta-Analysis. Acad. Emerg. Med. 2019, 26, 1074–1088. [Google Scholar] [CrossRef] [PubMed]
- Tomà, P. Lung Ultrasound in Pediatric Radiology—Cons. Pediatr. Radiol. 2020, 50, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Soldati, G.; Curatola, A.; Morello, R.; De Rose, C.; Vacca, M.E.; Lazzareschi, I.; Musolino, A.M.; Valentini, P. Lung Ultrasound Pattern in Healthy Infants during the First 6 Months of Life. J. Ultrasound Med. 2020, 39, 2379–2388. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ammirabile, A.; Buonsenso, D.; Di Mauro, A. Lung Ultrasound in Pediatrics and Neonatology: An Update. Healthcare 2021, 9, 1015. https://doi.org/10.3390/healthcare9081015
Ammirabile A, Buonsenso D, Di Mauro A. Lung Ultrasound in Pediatrics and Neonatology: An Update. Healthcare. 2021; 9(8):1015. https://doi.org/10.3390/healthcare9081015
Chicago/Turabian StyleAmmirabile, Angela, Danilo Buonsenso, and Antonio Di Mauro. 2021. "Lung Ultrasound in Pediatrics and Neonatology: An Update" Healthcare 9, no. 8: 1015. https://doi.org/10.3390/healthcare9081015
APA StyleAmmirabile, A., Buonsenso, D., & Di Mauro, A. (2021). Lung Ultrasound in Pediatrics and Neonatology: An Update. Healthcare, 9(8), 1015. https://doi.org/10.3390/healthcare9081015