
Medical Faculty’s and Students’ Perceptions toward Pediatric Electronic OSCE during the COVID-19 Pandemic in Saudi Arabia

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Electronic-OSCE Procedures
- Zoom™ breakout rooms were created by the examination committee.
- Students arrived 15 min before the start of the exam and were admitted to waiting virtual breakout rooms.
- The students and the examiners were asked to keep their cameras on throughout the exam.
- The students were admitted to their assigned virtual breakout rooms where their examiners were waiting for them there (e.g., two examiners in each breakout room).
- The examiners then presented students with three different clinical scenarios, which included patient history taking, an emergency case, and a chronic pediatric problem.
- The students were then given eight minutes to answer all post-encounter prompts.
- While one of the examiners was observing and grading the students, the other examiner acted as a standardized patient as needed based on the case scenario.
- At the end of the encounter (24 min in total), a five-minute break was given to allow timely admission of the next group of students.
- A 15-min break between each student and the next was taken to complete the checklist and mark the students by each examiner separately for the three stations.
- The case scenarios were changed for each group with a total of 18 scenarios.
2.3. Faculty’s and Students’ Perceptions of e-OSCE
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
|
|
|
|
|
|
|
|
|
|
|
|
|
|
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
References
- Major, S.; Sawan, L.; Vognsen, J.; Jabre, M. COVID-19 pandemic prompts the development of a Web-OSCE using Zoom teleconferencing to resume medical students’ clinical skills training at Weill Cornell Medicine-Qatar. BMJ Simul. Technol. Enhanc. Learn. 2020, bmjstel-2020-000629. [Google Scholar] [CrossRef]
- Lara, S.; Foster, C.W.; Hawks, M.; Montgomery, M. Remote Assessment of Clinical Skills During COVID-19: A Virtual, High-Stakes, Summative Pediatric Objective Structured Clinical Examination. Acad. Pediatr. 2020, 20, 760–761. [Google Scholar] [CrossRef] [PubMed]
- Pitt, M.B.; Li, S.T.; Klein, M. Novel Educational Responses to COVID-19: What is Here to Stay? Acad. Pediatr. 2020, 20, 733–734. [Google Scholar] [CrossRef] [PubMed]
- Elham, A. Implementing eOSCE During COVID-19 Lockdown. J. Adv. Pharm. Educ. Res. 2020, 10, 174–180. [Google Scholar]
- Alsoufi, A.; Alsuyihili, A.; Msherghi, A.; Elhadi, A.; Atiyah, H.; Ashini, A.; Ashwieb, A.; Ghula, M.; Ben Hasan, H.; Abudabuos, S.; et al. Impact of the COVID-19 pandemic on medical education: Medical students’ knowledge, attitudes, and practices regarding electronic learning. PLoS ONE 2020, 15, e0242905. [Google Scholar] [CrossRef] [PubMed]
- Alea, L.A.; Fabrea, M.F.; Roldan, R.D.A.; Farooqi, A.Z. Teachers’ Covid-19 awareness, distance learning education experiences and perceptions towards institutional readiness and challenges. Int. J. Learn. Teach. Educ. Res. 2020, 19, 127–144. [Google Scholar]
- Walsh, K. Online assessment in medical education-current trends and future directions. Malawi Med. J. 2015, 27, 71–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, R.T.; Biagioli, F.E.; Mujcic, J.; Schneider, B.N.; Spires, L.; Dodson, L.G. The feasibility and acceptability of administering a telemedicine objective structured clinical exam as a solution for providing equivalent education to remote and rural learners. Rural. Remote Health 2015, 15, 3399. [Google Scholar] [PubMed]
- School, H.M. Coronavirus Communications. Available online: https://hms.harvard.edu/coronavirus/coronavirus-communications (accessed on 18 October 2020).
- Stowell, J.R.; Bennett, D. Effects of online testing on student exam performance and test anxiety. J. Educ. Comput. Res. 2010, 42, 161–171. [Google Scholar] [CrossRef]
- Batais, M.A.; Temsah, M.H.; AlGhofili, H.; AlRuwayshid, N.; Alsohime, F.; Almigbal, T.H.; Al-Rabiaah, A.; Al-Eyadhy, A.A.; Mujammami, M.H.; Halwani, R.; et al. The coronavirus disease of 2019 pandemic-associated stress among medical students in middle east respiratory syndrome-CoV endemic area: An observational study. Med. (Baltim.) 2021, 100, e23690. [Google Scholar] [CrossRef] [PubMed]
- Al-Rabiaah, A.; Temsah, M.H.; Al-Eyadhy, A.A.; Hasan, G.M.; Al-Zamil, F.; Al-Subaie, S.; Alsohime, F.; Jamal, A.; Alhaboob, A.; Al-Saadi, B.; et al. Middle East Respiratory Syndrome-Corona Virus (MERS-CoV) associated stress among medical students at a university teaching hospital in Saudi Arabia. J. Infect. Public Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Saddik, B.; Hussein, A.; Sharif-Askari, F.S.; Kheder, W.; Temsah, M.H.; Koutaich, R.A.; Haddad, E.S.; Al-Roub, N.M.; Marhoon, F.A.; Hamid, Q.; et al. Increased Levels of Anxiety Among Medical and Non-Medical University Students During the COVID-19 Pandemic in the United Arab Emirates. Risk Manag. Healthc Policy 2020, 13, 2395–2406. [Google Scholar] [CrossRef] [PubMed]
- Temsah, M.H.; Alhuzaimi, A.N.; Alamro, N.; Alrabiaah, A.; Al-Sohime, F.; Alhasan, K.; Kari, J.A.; Almaghlouth, I.; Aljamaan, F.; Al-Eyadhy, A.; et al. Knowledge, attitudes and practices of healthcare workers during the early COVID-19 pandemic in a main, academic tertiary care centre in Saudi Arabia. Epidemiol. Infect. 2020, 148, e203. [Google Scholar] [CrossRef] [PubMed]
- Graf, J.; Smolka, R.; Simoes, E.; Zipfel, S.; Junne, F.; Holderried, F.; Wosnik, A.; Doherty, A.M.; Menzel, K.; Herrmann-Werner, A. Communication skills of medical students during the OSCE: Gender-specific differences in a longitudinal trend study. BMC Med. Educ. 2017, 17, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.-J.; Lee, Y.J.; Lee, M.J.; Kim, Y.H. E-Learning for Enhancement of Medical Student Performance at the Objective Structured Clinical Examination (OSCE) in the COVID-19 Era. 2020. Available online: https://assets.researchsquare.com/files/rs-126355/v1/6f83ee43-4189-432e-a706-48b6a3bf9376.pdf?c=1609139666 (accessed on 18 October 2020).
- Khalaf, K.; El-Kishawi, M.; Moufti, M.A.; Al Kawas, S. Introducing a comprehensive high-stake online exam to final-year dental students during the COVID-19 pandemic and evaluation of its effectiveness. Med. Educ. Online 2020, 25, 1826861. [Google Scholar] [CrossRef] [PubMed]
- Elledge, R.; Williams, R.; Fowell, C.; Green, J. Maxillofacial education in the time of COVID-19: The West Midlands experience. Br. J. Oral Maxillofac. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Petrisor, M.; Marusteri, M.; Simpalean, D.; Carasca, E.; Ghiga, D. Medical students’ acceptance of online assessment systems. Acta Med. Marisiensis 2016, 62, 30–32. [Google Scholar] [CrossRef] [Green Version]
- Pal, D.; Vanijja, V. Perceived usability evaluation of Microsoft Teams as an online learning platform during COVID-19 using system usability scale and technology acceptance model in India. Child. Youth Serv. Rev. 2020, 119, 105535. [Google Scholar] [CrossRef] [PubMed]

| Characteristic | Frequency | Percentage |
|---|---|---|
| Sex | ||
| Female | 63 | 86.3 |
| Male | 10 | 13.7 |
| Age | ||
| ≤30 years | 50 | 68.5 |
| >30 years | 23 | 31.5 |
| Role | ||
| Academic teacher | 23 | 31.5 |
| Medical student | 50 | 68.5 |
| Previously used teleconference methods | ||
| Face time | 26 | 35.6 |
| Zoom | 72 | 98.6 |
| Webinar | 40 | 54.8 |
| Work-related online meetings | 26 | 35.6 |
| Online learning interfaces | 35 | 47.9 |
| Telephonic conference | 15 | 20.5 |
| Other methods/tools | 1 | 1.4 |
| Question | Frequency | Percentage (%) |
|---|---|---|
| How comfortable did you feel participating in this remote clinical exam (via Zoom or any other similar application)? | ||
| Not at all comfortable | 1 | 1.4 |
| Not so comfortable | 7 | 9.6 |
| Somewhat comfortable | 14 | 19.2 |
| Very comfortable | 35 | 47.9 |
| Extremely comfortable | 16 | 21.9 |
| In regard to your previous experience with “classic face-to-face” clinical OSCE, what is the preferred OSCE style for you during the COVID-19 Pandemic? | ||
| Virtual OSCE (e-OSCE) is preferred | 39 | 53.4 |
| Classic face-to-face is preferred | 23 | 31.5 |
| Both are equally preferred for me | 11 | 15.1 |
| How do you think these remote clinical exams (e-OSCE) affected the quality of the student’s assessment? | ||
| Similar assessment to the face-to-face OSCE | 34 | 46.6 |
| Better assessment than face-to-face OSCE | 11 | 15.1 |
| Worse assessment than face-to-face OSCE | 28 | 38.4 |
| Doing remote video assessment during the COVID-19 pandemic decreased my anxiety-mean (SD) 1–5 Likert agreement. | ||
| Strongly disagree | 6 | 8.2 |
| Disagree | 13 | 17.8 |
| Neither agree or disagree | 18 | 24.7 |
| Agree | 26 | 35.6 |
| Strongly agree | 10 | 13.7 |
| Video conferencing as an assessment tool for the pediatric course should be incorporated in next year’s courses. | ||
| Strongly disagree | 5 | 6.8 |
| Disagree | 20 | 27.4 |
| Neither agree or disagree | 19 | 26 |
| Agree | 24 | 32.9 |
| Strongly agree | 5 | 6.8 |
| Do you suggest continuing on remote student assessments (via Zoom or similar platforms) after the COVID crisis? | ||
| Yes | 19 | 26 |
| No | 54 | 74 |
| Characteristic | Frequency | Percentage (%) |
|---|---|---|
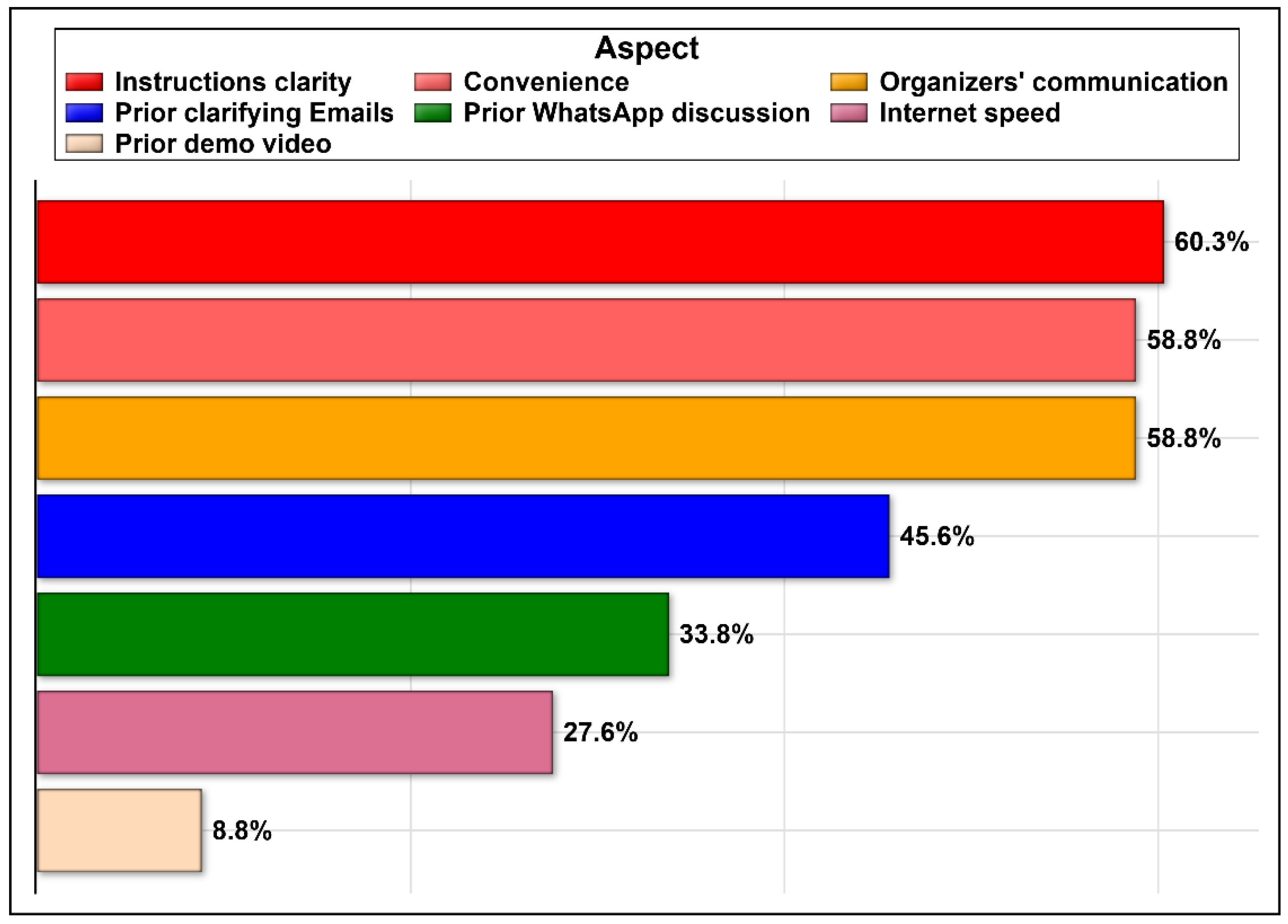
| The participants perceived Positive aspects of the Online OSCE experience | ||
| The clear instructions provided | 41 | 60.3 |
| Organizers’ prompt communications | 40 | 58.8 |
| The free use of the zoom application | 40 | 58.8 |
| Clarifying emails received from the organizers | 31 | 45.6 |
| The WhatsApp group discussion that related specifically to this event | 23 | 33.8 |
| The fast internet speed | 19 | 27.9 |
| The demo of videoconference before connecting | 5 | 7.4 |
| Other | 6 | 8.8 |
| The participants perceived negative aspects of the Online OSCE experience | ||
| Slow internet speed | 30 | 44.1 |
| Unclear demo video | 18 | 26.4 |
| Unclear instructions | 10 | 14.7 |
| Unfamiliarity with the application | 6 | 8.8 |
| Not receiving clarification emails | 2 | 2.9 |
| Other | 23 | 33.8 |
| Variable | How Do You Think These Remote Clinical Exams (e-OSCE) Affected the Quality of the Student’s Assessment? | Test Statistic | p-Value | |
| Similar/Better | Worse | |||
| Sex | ||||
| Female | 40 (88.9) | 23 (82.1) | χ2(1) = 0.22 | 0.642 |
| Male | 5 (11.1) | 5 (17.9) | ||
| Age | ||||
| ≤30 years | 35 (77.8) | 15 (53.6) | χ2(1) = 4.70 | 0.030 |
| >30 years | 10 (22.2) | 13 (46.4) | ||
| Role | ||||
| Academic teacher/coordinator | 10 (22.2) | 13 (46.4) | χ2(1) = 4.670 | 0.030 |
| Medical student | 35 (77.8) | 15 (53.6) | ||
| How likely is it that you would recommend virtual assessment (e-OSCE) to a friend or colleague?-median Likert rating | 8 | 6 | U(73) = 380.5 | 0.003 |
| How comfortable did you feel participating in this remote clinical exam (via Zoom or any other similar application)?—median Likert rating | 4 | 3.4 | U(73) = 418 | 0.010 |
| In regard to your previous experience with “classic face-to-face” clinical OSCE, what is the preferred OSCE style for you during the COVID Pandemic? | ||||
| virtual OSCE (e-OSCE) is preferred | 29 (64.4) | 10 (35.7) | χ2(2) = 7.60 | 0.022 |
| classic face-to-face is preferred | 9 (20) | 14 (50) | ||
| Both are equally preferred for me | 7 (15.6) | 4 (14.3) | ||
| Doing remote video assessment during the COVID-19 pandemic decreased my anxiety-median Likert agreement | 4 | 3 | U(73) = 487 | 0.093 |
| Video conferencing as an assessment tool for the pediatric course should be incorporated in next year’s courses-median value | 4 | 2 | U(73) = 223.5 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaiba, L.A.; Alnamnakani, M.A.; Temsah, M.-H.; Alamro, N.; Alsohime, F.; Alrabiaah, A.; Alanazi, S.N.; Alhasan, K.; Alherbish, A.; Mobaireek, K.F.; et al. Medical Faculty’s and Students’ Perceptions toward Pediatric Electronic OSCE during the COVID-19 Pandemic in Saudi Arabia. Healthcare 2021, 9, 950. https://doi.org/10.3390/healthcare9080950
Shaiba LA, Alnamnakani MA, Temsah M-H, Alamro N, Alsohime F, Alrabiaah A, Alanazi SN, Alhasan K, Alherbish A, Mobaireek KF, et al. Medical Faculty’s and Students’ Perceptions toward Pediatric Electronic OSCE during the COVID-19 Pandemic in Saudi Arabia. Healthcare. 2021; 9(8):950. https://doi.org/10.3390/healthcare9080950
Chicago/Turabian StyleShaiba, Lana A., Mahdi A. Alnamnakani, Mohamad-Hani Temsah, Nurah Alamro, Fahad Alsohime, Abdulkarim Alrabiaah, Shahad N. Alanazi, Khalid Alhasan, Adi Alherbish, Khalid F. Mobaireek, and et al. 2021. "Medical Faculty’s and Students’ Perceptions toward Pediatric Electronic OSCE during the COVID-19 Pandemic in Saudi Arabia" Healthcare 9, no. 8: 950. https://doi.org/10.3390/healthcare9080950
APA StyleShaiba, L. A., Alnamnakani, M. A., Temsah, M.-H., Alamro, N., Alsohime, F., Alrabiaah, A., Alanazi, S. N., Alhasan, K., Alherbish, A., Mobaireek, K. F., Bashiri, F. A., & AlRuthia, Y. (2021). Medical Faculty’s and Students’ Perceptions toward Pediatric Electronic OSCE during the COVID-19 Pandemic in Saudi Arabia. Healthcare, 9(8), 950. https://doi.org/10.3390/healthcare9080950