
Who Is the Most Vulnerable to Anxiety at the Beginning of the COVID-19 Outbreak in China? A Cross-Sectional Nationwide Survey

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measures
2.2.1. Socio-Demographic Variables
2.2.2. Anxiety Reaction towards COVID-19
2.2.3. Subjective Health Status
2.2.4. Cognitive Risk
2.2.5. Confidence
2.3. Data Management and Statistical Analysis
2.4. Quality Control
2.5. Ethical Approval
3. Results
3.1. Participants and Characteristics
3.2. The Association between Age and Anxiety Score
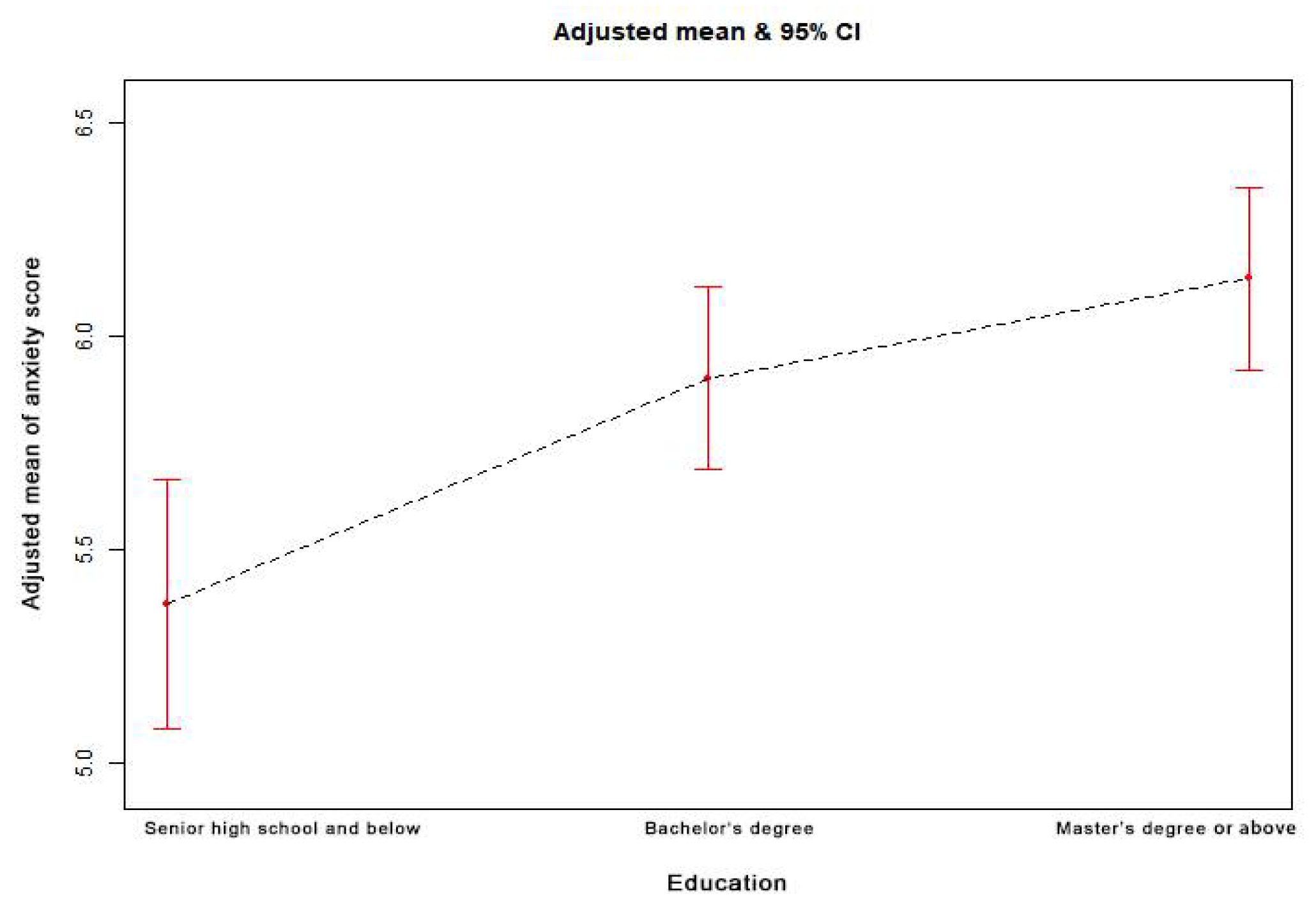
3.3. The Association between Education and Anxiety Score
3.4. The Association between Health and Anxiety Score
3.5. The Association between Cognitive Risk and Anxiety Score
3.6. The Association between Confidence and Anxiety Score
3.7. The Dose–Response Relationship of Age, Education, and Anxiety Score
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Category | n | Non-Adjusted Model | Model I a | Model II b | |||
|---|---|---|---|---|---|---|---|
| (95% CI LL, UL) | p Value | (95% CI LL, UL) | p Value | (95% CI LL, UL) | p Value | ||
| Male | 3680 | ||||||
| <30 years | 1053 | 0 | 0 | 0 | |||
| 30–40 years | 1040 | −0.16 (−0.50, 0.18) | 0.3588 | −0.44 (−0.90, 0.03) | 0.0655 | −0.52 (−0.98, −0.05) | 0.0296 |
| 40–50 years | 874 | −0.55 (−0.91, −0.19) | 0.0028 | −0.88 (−1.41, −0.36) | 0.0010 | −0.98 (−1.50, −0.46) | 0.0002 |
| ≥50 years | 713 | −1.45 (−1.83, −1.07) | <0.0001 | −1.79 (−2.33, −1.24) | <0.0001 | −1.84 (−2.39, −1.28) | <0.0001 |
| Female | 7266 | ||||||
| <30 years | 2416 | 0 | 0 | 0 | |||
| 30–40 years | 2092 | −0.13 (−0.37, 0.10) | 0.2769 | −0.28 (−0.60, 0.03) | 0.0780 | −0.57 (−0.88, −0.25) | 0.0004 |
| 40–50 years | 1618 | −1.27 (−1.52, −1.01) | <0.0001 | −1.43 (−1.79, −1.08) | <0.0001 | −1.73 (−2.08, −1.38) | <0.0001 |
| ≥50 years | 1140 | −2.28 (−2.56, −2.00) | <0.0001 | −2.44 (−2.82, −2.05) | <0.0001 | −2.77 (−3.18, −2.36) | <0.0001 |
| p interaction | <0.0001 | ||||||

References
- Gates, B. Responding to Covid-19—A Once-in-a-Century Pandemic? N. Engl. J. Med. 2020, 382, 1677–1679. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- USA Today. The World Surpasses 20 Million COVID-19 Cases: A Look at the Milestones and Setbacks. Available online: https://www.usatoday.com/story/news/nation/2020/07/23/united-states-coronavirus-cases-deaths-timeline/5485674002/ (accessed on 23 July 2020).
- Blakey, S.M.; Abramowitz, J.S. Psychological Predictors of Health Anxiety in Response to the Zika Virus. J. Clin. Psychol. Med. Set. 2017, 24, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Liao, Q.; Cowling, B.J.; Lam, W.W.T.; Ng, D.M.W.; Fielding, R. Anxiety, worry and cognitive risk estimate in relation to protective behaviors during the 2009 influenza A/H1N1 pandemic in Hong Kong: Ten cross-sectional surveys. BMC Infect. Dis. 2014, 14, 169. [Google Scholar] [CrossRef] [Green Version]
- Abdulkareem, S.A.; Augustijn, E.-W.; Filatova, T.; Musial, K.; Mustafa, Y.T. Risk perception and behavioral change during epidemics: Comparing models of individual and collective learning. PLoS ONE 2020, 15, e0226483. [Google Scholar] [CrossRef]
- Lau, J.T.F.; Yang, X.; Tsui, H.; Kim, J.H. Monitoring community responses to the SARS epidemic in Hong Kong: From day 10 to day 62. J. Epidemiol. Commun. Health 2003, 57, 864–870. [Google Scholar] [CrossRef]
- Brug, J.; Aro, A.R.; Oenema, A.; De Zwart, O.; Richardus, J.H.; Bishop, G.D. SARS Risk Perception, Knowledge, Precautions, and Information Sources, the Netherlands. Emerg. Infect. Dis. 2004, 10, 1486–1489. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The Psychological Impact of the SARS Epidemic on Hospital Employees in China: Exposure, Risk Perception, and Altruistic Acceptance of Risk. Can. J. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.J.; Amlôt, R.; Page, L.; Wessely, S. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: Cross sectional telephone survey. BMJ 2009, 339, b2651. [Google Scholar] [CrossRef] [Green Version]
- Bayham, J.; Kuminoff, N.V.; Gunn, Q.; Fenichel, E. Measured voluntary avoidance behaviour during the 2009 A/H1N1 epidemic. Proc. R. Soc. B Biol. Sci. 2015, 282, 20150814. [Google Scholar] [CrossRef] [Green Version]
- Lau, J.T.F.; Griffiths, S.; Choi, K.C.; Tsui, H.Y. Avoidance behaviors and negative psychological responses in the general population in the initial stage of the H1N1 pandemic in Hong Kong. BMC Infect. Dis. 2010, 10, 139. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Cowling, B.; Wu, P.; Yu, J.; Li, F.; Zeng, L.; Wu, J.T.; Li, Z.; Leung, G.; Yu, H. Human Exposure to Live Poultry and Psychological and Behavioral Responses to Influenza A(H7N9), China. Emerg. Infect. Dis. 2014, 20, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Wu, P.; Wang, L.; Cowling, B.J.; Yu, J.; Fang, V.J.; Li, F.; Zeng, L.; Wu, J.T.; Li, Z.; et al. Live poultry exposure and public response to influenza A(H7N9) in urban and rural China during two epidemic waves in 2013–2014. PLoS ONE 2015, 10, e0137831. [Google Scholar] [CrossRef]
- Cheng, C.; Tang, C.S.-K. The psychology behind the masks: Psychological responses to the severe acute respiratory syndrome outbreak in different regions. Asian J. Soc. Psychol. 2004, 7, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Vartti, A.-M.; Oenema, A.; Schreck, M.; Uutela, A.; De Zwart, O.; Brug, J.; Aro, A.R. SARS Knowledge, Perceptions, and Behaviors: A Comparison between Finns and the Dutch during the SARS Outbreak in 2003. Int. J. Behav. Med. 2009, 16, 41–48. [Google Scholar] [CrossRef] [Green Version]
- De Zwart, O.; Veldhuijzen, I.K.; Elam, G.; Aro, A.R.; Abraham, T.; Bishop, G.D.; Voeten, H.A.C.M.; Richardus, J.H.; Brug, J. Perceived Threat, Risk Perception, and Efficacy Beliefs Related to SARS and Other (Emerging) Infectious Diseases: Results of an International Survey. Int. J. Behav. Med. 2009, 16, 30–40. [Google Scholar] [CrossRef] [Green Version]
- Bults, M.; Beaujean, D.J.M.A.; de Zwart, O.; Kok, G.; van Empelen, P.; van Steenbergen, J.E.; Richardus, J.H.; Voeten, H.A.C.M. Perceived risk, anxiety and behavioural responses of the general public during the early phase of the Influenza A (H1N1) pandemic in the Netherlands. Psychol. Health 2010, 25, 121–122. [Google Scholar]
- Wallace, C.L.; Wladkowski, S.; Gibson, A.; White, P. Grief During the COVID-19 Pandemic: Considerations for Palliative Care Providers. J. Pain Symptom Manag. 2020, 60, e70–e76. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Wang, Y.; Fu, H.; Dai, J. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef]
- Leung, G.; Quah, S.R.; Ho, L.-M.; Ho, S.-Y.; Hedley, A.J.; Lee, H.-P.; Lam, T.-H. A Tale of Two Cities: Community Psychobehavioral Surveillance and Related Impact on Outbreak Control in Hong Kong and Singapore During the Severe Acute Respiratory Syndrome Epidemic. Infect. Control Hosp. Epidemiol. 2004, 25, 1033–1041. [Google Scholar] [CrossRef] [Green Version]
- Takebayashi, Y.; Lyamzina, Y.; Suzuki, Y.; Murakami, M. Risk Perception and Anxiety Regarding Radiation after the 2011 Fukushima Nuclear Power Plant Accident: A Systematic Qualitative Review. Int. J. Environ. Res. Public Health 2017, 14, 1306. [Google Scholar] [CrossRef] [Green Version]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef]
- Lu, W.-H.; Ko, N.-Y.; Chang, Y.-P.; Yen, C.-F.; Wang, P.-W. The Coronavirus Disease 2019 Pandemic in Taiwan: An Online Survey on Worry and Anxiety and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 7974. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef] [PubMed]
- Zsido, A.N.; Teleki, S.A.; Csokasi, K.; Rozsa, S.; Bandi, S. Development of the short version of the spielberger state—Trait anxiety inventory. Psychiatry Res. 2020, 291, 113223. [Google Scholar] [CrossRef]
- Prati, G.; Pietrantoni, L.; Zani, B. A Social-Cognitive Model of Pandemic Influenza H1N1 Risk Perception and Recommended Behaviors in Italy. Risk Anal. 2010, 31, 645–656. [Google Scholar] [CrossRef]
- Moghanibashi-Mansourieh, A. Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian J. Psychiatry 2020, 51, 102076. [Google Scholar] [CrossRef]
- Roy, D.; Tripathy, S.; Kar, S.K.; Sharma, N.; Verma, S.K.; Kaushal, V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J. Psychiatry 2020, 51, 102083. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Wu, J.; Wang, J.; Nicholas, S.; Maitland, E.; Fan, Q. Application of Big Data Technology for COVID-19 Prevention and Control in China: Lessons and Recommendations. J. Med. Internet Res. 2020, 22, e21980. [Google Scholar] [CrossRef] [PubMed]
- Mehra, A.; Rani, S.; Sahoo, S.; Parveen, S.; Singh, A.P.; Chakrabarti, S.; Grover, S. A crisis for elderly with mental disorders: Relapse of symptoms due to heightened anxiety due to COVID-19. Asian J. Psychiatry 2020, 51, 102114. [Google Scholar] [CrossRef]
- Lau, J.T.; Yang, X.; Pang, E.; Tsui, H.; Wong, E.; Wing, Y.K. SARS-related perceptions in Hong Kong. Emerg. Infect. Dis. 2005, 11, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Stefanac, N.; Hetrick, S.; Hulbert, C.; Spittal, M.J.; Witt, K.; Robinson, J. Are young female suicides increasing? A comparison of sex-specific rates and characteristics of youth suicides in Australia over 2004–2014. BMC Public Health 2019, 19, 1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, B.W.; Kay, V.S.; Hoyt, T.V.; Bernard, M.L. Predicting the anticipated emotional and behavioral responses to an avian flu outbreak. Am. J. Infect. Control. 2009, 37, 371–380. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on College Students’ Mental Health in the United States: Interview Survey Study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- Araújo, F.J.D.O.; De Lima, L.S.A.; Cidade, P.I.M.; Nobre, C.B.; Neto, M.L.R. Impact Of Sars-Cov-2 And Its Reverberation In Global Higher Education And Mental Health. Psychiatry Res. 2020, 288, 112977. [Google Scholar] [CrossRef]
- Shook, E.; Curtis, A.; Curtis, J.; Gibson, G.; Horst, A.V.; Little, V.; Woolverton, C. Assessing the Geographic Context of Risk Perception and Behavioral Response to Potential Ebola Exposure. Int. J. Environ. Res. Public Health 2019, 16, 831. [Google Scholar] [CrossRef] [Green Version]
- Kashiwazaki, Y.; Takebayashi, Y.; Murakami, M. Relationships between radiation risk perception and health anxiety, and contribution of mindfulness to alleviating psychological distress after the Fukushima accident: Cross-sectional study using a path model. PLoS ONE 2020, 15, e0235517. [Google Scholar] [CrossRef] [PubMed]
- Germani, A.; Buratta, L.; Del Vecchio, E.; Mazzeschi, C. Emerging Adults and COVID-19: The Role of Individualism-Collectivism on Perceived Risks and Psychological Maladjustment. Int. J. Environ. Res. Public Health 2020, 17, 3497. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.; Guo, Z.; Zhou, L.; Xue, S.; Zhu, Q.; Zhu, H. Combined and Relative Effect Levels of Perceived Risk, Knowledge, Optimism, Pessimism, and Social Trust on Anxiety among Inhabitants Concerning Living on Heavy Metal Contaminated Soil. Int. J. Environ. Res. Public Health 2016, 13, 1076. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.S.C.; Ansari, D.; Knowland, V.C.P. Annual Research Review: Educational neuroscience: Progress and prospects. J. Child Psychol. Psychiatry 2019, 60, 477–492. [Google Scholar] [CrossRef] [Green Version]
- Bagroy, S.; Kumaraguru, P.; De Choudhury, M. A Social Media Based Index of Mental Well-Being in College Campuses. In Proceedings of the CHI Conference on Human Factors in Computing Systems, Denver, CO, USA, 6–11 May 2017; Association for Computing Machinery (ACM): New York, NY, USA, 2017; Volume 2017, pp. 1634–1646. [Google Scholar]
- Weible, C.M.; Nohrstedt, D.; Cairney, P.; Carter, D.; Crow, D.A.; Durnová, A.P.; Heikkila, T.; Ingold, K.; McConnell, A.; Stone, D. COVID-19 and the policy sciences: Initial reactions and perspectives. Policy Sci. 2020, 53, 225–241. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Mishima, N. Province-level estimation of waste mobile phones in China and location planning of recycling centers. Waste Manag. Res. 2019, 37, 898–905. [Google Scholar] [CrossRef]
- Lippke, S.; Dahmen, A.; Gao, L.; Guza, E.; Nigg, C.R. To What Extent is Internet Activity Predictive of Psychological Well-Being? Psychol. Res. Behav. Manag. 2021, 14, 207–219. [Google Scholar] [CrossRef]
- Tang, C.S.-K.; Wong, C.-Y. Factors influencing the wearing of facemasks to prevent the severe acute respiratory syndrome among adult Chinese in Hong Kong. Prev. Med. 2004, 39, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Groß, S.; Jahn, C.; Cushman, S.; Bär, C.; Thum, T. SARS-CoV-2 receptor ACE2-dependent implications on the cardiovascular system: From basic science to clinical implications. J. Mol. Cell. Cardiol. 2020, 144, 47–53. [Google Scholar] [CrossRef]
- Xu, G.; Yang, Y.; Du, Y.; Peng, F.; Hu, P.; Wang, R.; Yin, M.; Li, T.; Tu, L.; Sun, J.; et al. Clinical Pathway for Early Diagnosis of COVID-19: Updates from Experience to Evidence-Based Practice. Clin. Rev. Allergy Immunol. 2020, 59, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Guo, M.; Duan, L.; Wu, F.; Hu, G.; Wang, Z.; Huang, Q.; Liao, T.; Xu, J.; Ma, Y.; et al. Development and validation of a risk factor-based system to predict short-term survival in adult hospitalized patients with COVID-19: A multicenter, retrospective, cohort study. Crit. Care 2020, 24, 1–13. [Google Scholar] [CrossRef]
- Asmundson, G.J.; Taylor, S. Coronaphobia: Fear and the 2019-nCoV outbreak. J. Anxiety Disord. 2020, 70, 102196. [Google Scholar] [CrossRef]
- Ni, M.Y.; Yang, L.; Leung, C.M.C.; Li, N.; Yao, X.I.; Wang, Y.; Leung, G.M.; Cowling, B.J.; Liao, Q. Mental Health, Risk Factors, and Social Media Use During the COVID-19 Epidemic and Cordon Sanitaire Among the Community and Health Professionals in Wuhan, China: Cross-Sectional Survey. JMIR Ment. Health 2020, 7, e19009. [Google Scholar] [CrossRef]
- Chen, S.; Westman, M.; Hobfoll, S.E. The Commerce and Crossover of Resources: Resource Conservation in the Service of Resilience. Stress Health 2015, 31, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, Y.; Okada, T.; Morikawa, M.; Yamauchi, A.; Sato, M.; Ando, M.; Ozaki, N. Perinatal depression and anxiety of primipara is higher than that of multipara in Japanese women. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]



| Normal | Mild Anxiety | Moderate Anxiety | Severe Anxiety | p Value | |
|---|---|---|---|---|---|
| (n = 5490) | (n = 2391) | (n = 2608) | (n = 457) | ||
| Anxiety score | 2.95 ± 2.09 | 7.98 ± 0.81 | 11.04 ± 1.08 | 14.47 ± 0.50 | <0.001 |
| Age(years) | 38.79 ± 12.61 | 36.23 ± 12.25 | 34.57 ± 10.64 | 32.85 ± 9.90 | <0.001 |
| Sex | <0.001 | ||||
| Male | 2146 (39.09%) | 735 (30.74%) | 701 (26.88%) | 98 (21.44%) | |
| Female | 3344 (60.91%) | 1656 (69.26%) | 1907 (73.12%) | 359 (78.56%) | |
| Marriage | <0.001 | ||||
| Unmarried | 1601 (29.16%) | 813 (34.00%) | 917 (35.16%) | 187 (40.92%) | |
| Married | 3664 (66.74%) | 1510 (63.15%) | 1610 (61.73%) | 257 (56.24%) | |
| Divorced | 161 (2.93%) | 45 (1.88%) | 62 (2.38%) | 11 (2.41%) | |
| Widowed | 41 (0.75%) | 14 (0.59%) | 7 (0.27%) | 1 (0.22%) | |
| Other | 23 (0.42%) | 9 (0.38%) | 12 (0.46%) | 1 (0.22%) | |
| Education | <0.001 | ||||
| Senior high school and below | 1165 (21.22%) | 409 (17.11%) | 305 (11.69%) | 52 (11.38%) | |
| Bachelor’s degree | 3035 (55.28%) | 1395 (58.34%) | 1563 (59.93%) | 258 (56.46%) | |
| Master’s degree or above | 1290 (23.50%) | 587 (24.55%) | 740 (28.37%) | 147 (32.17%) | |
| Occupation | <0.001 | ||||
| Medical professional | 924 (16.83%) | 431 (18.03%) | 515 (19.75%) | 96 (21.01%) | |
| Laborers | 462 (8.42%) | 134 (5.60%) | 133 (5.10%) | 26 (5.69%) | |
| Teachers and researchers | 1129 (20.56%) | 437 (18.28%) | 452 (17.33%) | 61 (13.35%) | |
| Government staff | 195 (3.55%) | 88 (3.68%) | 129 (4.95%) | 18 (3.94%) | |
| Commercial and service personnel | 1093 (19.91%) | 488 (20.41%) | 509 (19.52%) | 77 (16.85%) | |
| Students | 723 (13.17%) | 412 (17.23%) | 467 (17.91%) | 102 (22.32%) | |
| Retired staff | 305 (5.56%) | 126 (5.27%) | 52 (1.99%) | 11 (2.41%) | |
| Other | 659 (12.00%) | 275 (11.50%) | 351 (13.46%) | 66 (14.44%) | |
| Residence | 0.002 | ||||
| Urban | 4351 (79.25%) | 1893 (79.17%) | 2145 (82.25%) | 382 (83.59%) | |
| Rural | 1139 (20.75%) | 498 (20.83%) | 463 (17.75%) | 75 (16.41%) | |
| Area | 0.009 | ||||
| From Hubei province | 69 (1.26%) | 42 (1.76%) | 59 (2.26%) | 6 (1.31%) | |
| From other provinces | 5324 (96.98%) | 2299 (96.15%) | 2485 (95.28%) | 444 (97.16%) | |
| From abroad | 97 (1.77%) | 50 (2.09%) | 64 (2.45%) | 7 (1.53%) | |
| Family members | 0.270 | ||||
| < 3 family members | 566 (10.31%) | 210 (8.78%) | 263 (10.08%) | 43 (9.41%) | |
| 3–5 family members | 3085 (56.19%) | 1323 (55.33%) | 1462 (56.06%) | 263 (57.55%) | |
| ≥ 5 family members | 1839 (33.50%) | 858 (35.88%) | 883 (33.86%) | 151 (33.04%) | |
| Contact history | <0.001 | ||||
| No | 5170 (94.17%) | 2203 (92.14%) | 2312 (88.65%) | 3902 (85.34%) | |
| Yes | 320 (5.83%) | 188 (7.86%) | 296 (11.35%) | 67 (14.66%) |
| Variables | n (%) | Non-Adjusted Model | Model I b | Model II c | |||
|---|---|---|---|---|---|---|---|
| (95% CI LL, UL) a | p Value | (95% CI LL, UL) | p Value | (95% CI LL, UL) | p Value | ||
| Age category | |||||||
| <30 years | 3469 (31.69) | 0 | 0 | 0 | |||
| 30–40 years | 3132 (28.61) | −0.18 (−0.38, 0.02) | 0.0704 | −0.46 (−0.72, −0.20) | 0.0006 | −0.40 (−0.68, −0.12) | 0.0053 |
| 40–50 years | 2492 (22.77) | −1.08 (−1.29, −0.87) | <0.0001 | −1.28 (−1.57, −0.98) | <0.0001 | −1.29 (−1.60, −0.98) | <0.0001 |
| ≥50 years | 1853 (16.93) | −2.07 (−2.30, −1.85) | <0.0001 | −2.15 (−2.46, −1.84) | <0.0001 | −2.12 (−2.47, −1.78) | <0.0001 |
| p Value for Trend | <0.001 | ||||||
| Education category | |||||||
| Senior high school and below | 1931 (17.64) | 0 | 0 | 0 | |||
| Bachelor’s degree | 6251 (57.11) | 1.21 (1.00, 1.42) | <0.0001 | 0.89 (0.67, 1.12) | <0.0001 | 0.84 (0.62, 1.06) | <0.0001 |
| Master’s degree or above | 2764 (25.25) | 1.55 (1.31, 1.79) | <0.0001 | 1.19 (0.92, 1.46) | <0.0001 | 1.15 (0.88, 1.41) | <0.0001 |
| p Value for Trend | <0.001 | ||||||
| Health category | |||||||
| Very healthy | 6332 (57.85) | 0 | 0 | 0 | |||
| Healthy | 3497 (31.95) | 1.57 (1.40, 1.73) | <0.0001 | 1.76 (1.60, 1.92) | <0.0001 | 1.76 (1.59, 1.92) | <0.0001 |
| Ordinary or unhealthy | 1117 (10.20) | 2.18 (1.92, 2.43) | <0.0001 | 2.78 (2.52, 3.03) | <0.0001 | 2.83 (2.58, 3.09) | <0.0001 |
| p Value for Trend | <0.001 | ||||||
| Variables | n (%) | Non-Adjusted Model | Model I b | Model II c | |||
|---|---|---|---|---|---|---|---|
| (95% CI LL, UL) a | p Value | (95% CI LL, UL) | p Value | (95% CI LL, UL) | p Value | ||
| Cognitive risk | |||||||
| No risk | 1755 (16.01) | 0 | 0 | 0 | |||
| Low risk | 6440 (58.80) | 2.52 (2.32, 2.72) | <0.0001 | 2.43 (2.33, 2.63) | <0.0001 | 2.21 (2.02, 2.41) | <0.0001 |
| Medium risk | 1982 (18.17) | 4.95 (4.70, 5.19) | <0.0001 | 4.79 (4.55, 5.03) | <0.0001 | 4.36 (4.12, 4.60) | <0.0001 |
| High risk | 591 (5.40) | 4.99 (4.63, 5.34) | <0.0001 | 4.87 (4.52, 5.22) | <0.0001 | 4.52 (4.18, 4.87) | <0.0001 |
| Extremely high risk | 178 (1.62) | 5.27 (4.68, 5.85) | <0.0001 | 5.15 (4.57, 5.73) | <0.0001 | 4.89 (4.33, 5.46) | <0.0001 |
| p Value for Trend | <0.001 | ||||||
| Confidence | |||||||
| Unconfident | 1235 (11.28) | 0 | 0 | 0 | |||
| Somewhat confident | 5322 (48.62) | −0.41 (−0.66, −0.16) | 0.0012 | −0.56 (−0.80, −0.32) | <0.0001 | −0.54 (−0.77, −0.31) | <0.0001 |
| Confident | 3535 (32.29) | −1.94 (−2.20, −1.68) | <0.0001 | −2.00 (−2.26, −1.75) | <0.0001 | −1.72 (−1.95, −1.48) | <0.0001 |
| Very confident | 854 (7.80) | −2.94 (−3.29, −2.59) | <0.0001 | −2.92 (−3.26, −2.58) | <0.0001 | −2.45 (−2.77, −2.13) | <0.0001 |
| p Value for Trend | <0.001 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, B.; Han, B.; Zheng, H.; Liu, H.; Zhao, T.; Wan, Y.; Cui, F. Who Is the Most Vulnerable to Anxiety at the Beginning of the COVID-19 Outbreak in China? A Cross-Sectional Nationwide Survey. Healthcare 2021, 9, 970. https://doi.org/10.3390/healthcare9080970
Liu B, Han B, Zheng H, Liu H, Zhao T, Wan Y, Cui F. Who Is the Most Vulnerable to Anxiety at the Beginning of the COVID-19 Outbreak in China? A Cross-Sectional Nationwide Survey. Healthcare. 2021; 9(8):970. https://doi.org/10.3390/healthcare9080970
Chicago/Turabian StyleLiu, Bei, Bingfeng Han, Hui Zheng, Hanyu Liu, Tianshuo Zhao, Yongmei Wan, and Fuqiang Cui. 2021. "Who Is the Most Vulnerable to Anxiety at the Beginning of the COVID-19 Outbreak in China? A Cross-Sectional Nationwide Survey" Healthcare 9, no. 8: 970. https://doi.org/10.3390/healthcare9080970
APA StyleLiu, B., Han, B., Zheng, H., Liu, H., Zhao, T., Wan, Y., & Cui, F. (2021). Who Is the Most Vulnerable to Anxiety at the Beginning of the COVID-19 Outbreak in China? A Cross-Sectional Nationwide Survey. Healthcare, 9(8), 970. https://doi.org/10.3390/healthcare9080970