
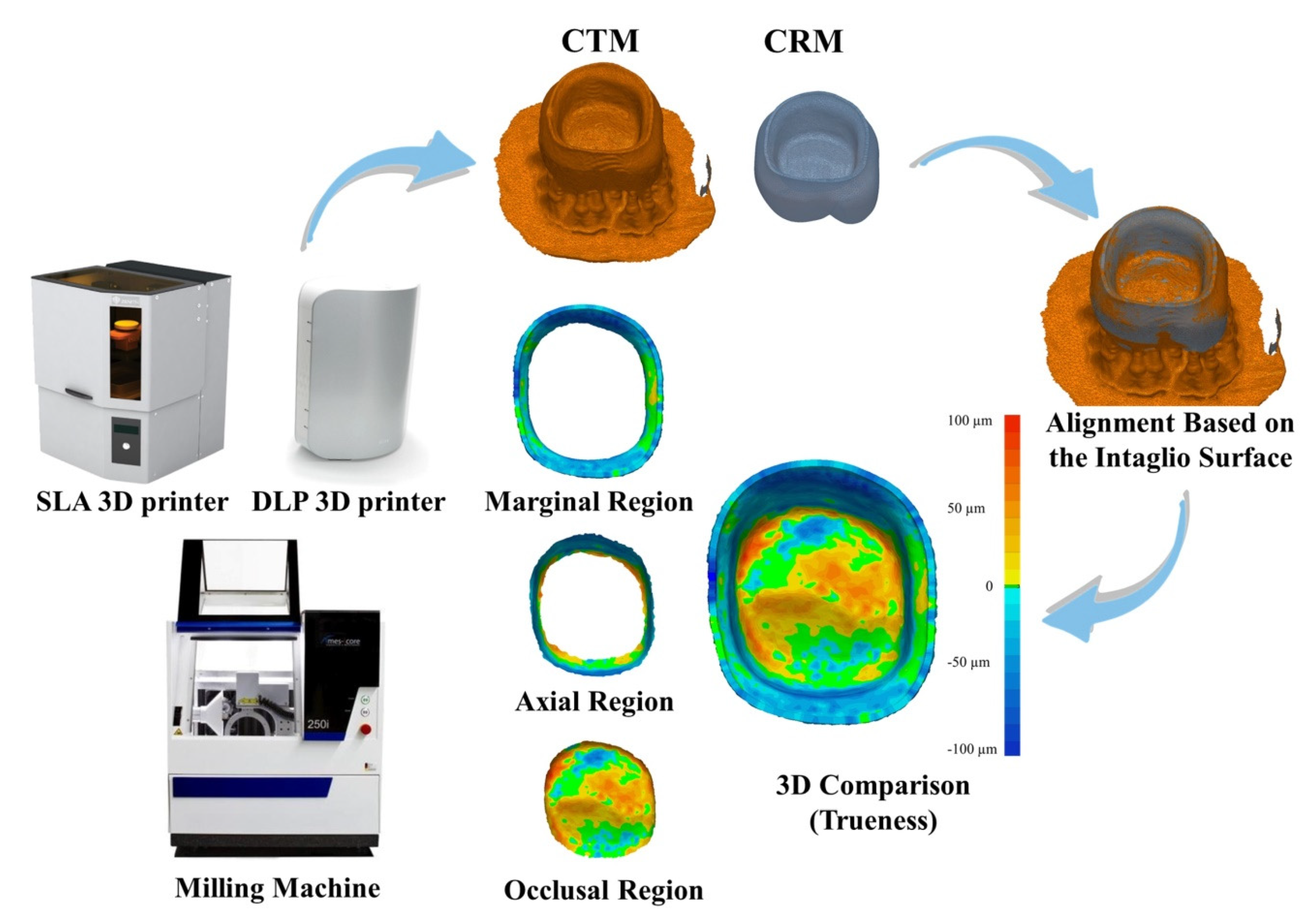
Comparison of Intaglio Surface Trueness of Interim Dental Crowns Fabricated with SLA 3D Printing, DLP 3D Printing, and Milling Technologies




Abstract
:1. Introduction
2. Materials and Methods
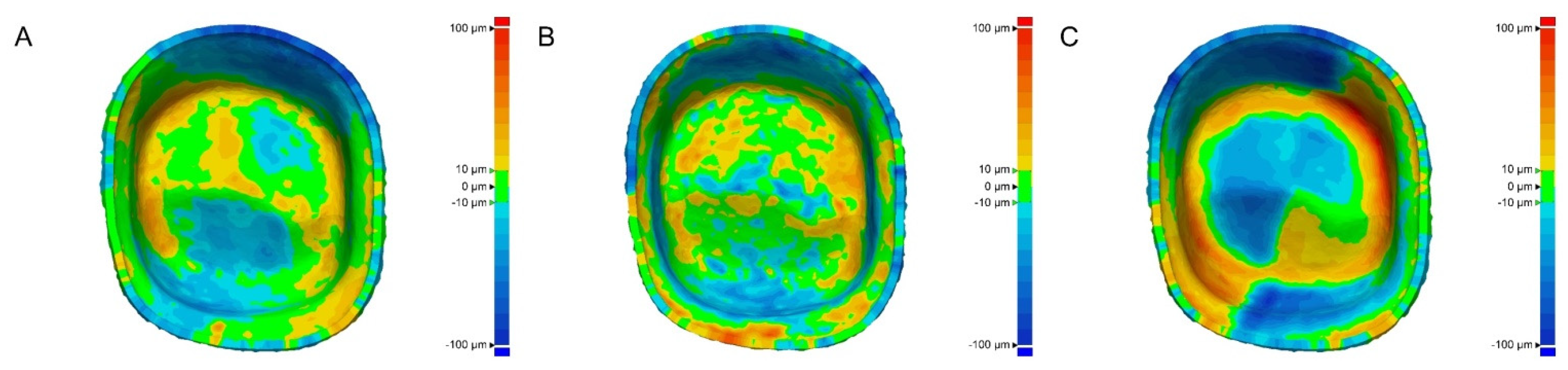
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kale, E.; Cilli, M.; Özçelik, T.B.; Yilmaz, B. Marginal fit of CAD-CAM monolithic zirconia crowns fabricated by using cone beam computed tomography scans. J. Prosthet. Dent. 2020, 123, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Son, K.; Lee, K.B. Effect of finish line locations of tooth preparation on the accuracy of intraoral scanners. Int. J. Comput. Dent. 2021, 24, 29–40. [Google Scholar]
- Angwarawong, T.; Reeponmaha, T.; Angwaravong, O. Influence of thermomechanical aging on marginal gap of CAD-CAM and conventional interim restorations. J. Prosthet. Dent. 2020, 124, 566.e1–566.e6. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.J.; Bae, E.B.; Lee, J.J.; Choi, J.W.; Jeon, Y.C.; Jeong, C.M.; Huh, J.B. Clinical evaluation of the fit of lithium disilicate crowns fabricated with three different CAD-CAM systems. J. Prosthet. Dent. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Baba, N.Z.; Goodacre, B.J.; Goodacre, C.J.; Müller, F.; Wagner, S. CAD/CAM complete denture systems and physical properties: A review of the literature. J. Prosthodont. 2021, 30, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, C.; Ender, A.; Attin, T.; Mehl, A. Trueness of four different milling procedures used in dental CAD/CAM systems. Clin. Oral Investig. 2017, 21, 551–558. [Google Scholar] [CrossRef]
- Son, K.; Yu, B.Y.; Yoon, T.H.; Lee, K.B. Comparative study of the trueness of the inner surface of crowns fabricated from three types of lithium disilicate blocks. Appl. Sci. 2019, 9, 1798. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.J.; Son, K.; Bae, E.B.; Choi, J.W.; Lee, K.B.; Huh, J.B. Comparison of the trueness of lithium disilicate crowns fabricated from all-in-one and combination CAD/CAM systems. Int. J. Prosthodont. 2019, 32, 352–354. [Google Scholar] [CrossRef]
- Taha, D.; Nour, M.; Zohdy, M.; El-Etreby, A.; Hamdy, A.; Salah, T. The effect of different wax pattern fabrication techniques on the marginal fit of customized lithium disilicate implant abutments. J. Prosthodont. 2019, 28, 1018–1023. [Google Scholar] [CrossRef]
- Kim, M.K.; Son, K.; Yu, B.Y.; Lee, K.B. Effect of the volumetric dimensions of a complete arch on the accuracy of scanners. J. Adv. Prosthodont. 2020, 12, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Martínez, S.; Cuesta, E.; Barreiro, J.; Álvarez, B. Analysis of laser scanning and strategies for dimensional and geometrical control. J. Adv. Manuf. Technol. 2010, 46, 621–629. [Google Scholar] [CrossRef]
- Choi, Y.K.; Banerjee, A. Tool path generation and tolerance analysis for free-form surfaces. Int. J. Mach. Tools Manuf. 2007, 47, 689–696. [Google Scholar] [CrossRef]
- Xiao, Z.; Yang, Y.; Xiao, R.; Bai, Y.; Song, C.; Wang, D. Evaluation of topology-optimized lattice structures manufactured via selective laser melting. Mater. Des. 2018, 143, 27–37. [Google Scholar] [CrossRef]
- Bosch, G.; Ender, A.; Mehl, A. A 3-dimensional accuracy analysis of chairside CAD/CAM milling processes. J. Prosthet. Dent. 2014, 112, 1425–1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, Y.G.; Lee, W.S.; Lee, K.B. Accuracy evaluation of dental models manufactured by CAD/CAM milling method and 3D printing method. J. Adv. Prosthodont. 2018, 10, 245–251. [Google Scholar] [CrossRef] [Green Version]
- Park, H.N.; Lim, Y.J.; Yi, W.J.; Han, J.S.; Lee, S.P. A comparison of the accuracy of intraoral scanners using an intraoral environment simulator. J. Adv. Prosthodont. 2018, 10, 58–64. [Google Scholar] [CrossRef]
- Tan, F.B.; Wang, C.; Dai, H.W.; Fan, Y.B.; Song, J.L. Accuracy and reproducibility of 3D digital tooth preparations made by gypsum materials of various colors. J. Adv. Prosthodont. 2018, 10, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.Y.; Esguerra, R.J.; Chia, V.A.P.; Tan, Y.H.; Tan, K.B.C. Three-dimensional accuracy of digital static interocclusal registration by three intraoral scanner systems. J. Prosthodont. 2018, 27, 120–128. [Google Scholar] [CrossRef]
- Motel, C.; Kirchner, E.; Adler, W.; Wichmann, M.; Matta, R.E. Impact of different scan bodies and scan strategies on the accuracy of digital implant impressions assessed with an intraoral scanner: An in vitro study. J. Prosthodont. 2020, 29, 309–314. [Google Scholar] [CrossRef] [Green Version]
- Fluegge, T.; Att, W.; Metzger, M.; Nelson, K. A novel method to evaluate precision of optical implant impressions with commercial scan bodies—An experimental approach. J. Prosthodont. 2017, 26, 34–41. [Google Scholar] [CrossRef]
- Zarone, F.; Ruggiero, G.; Ferrari, M.; Mangano, F.; Joda, T.; Sorrentino, R. Accuracy of a chairside intraoral scanner compared with a laboratory scanner for the completely edentulous maxilla: An in vitro 3-dimensional comparative analysis. J. Prosthet. Dent. 2020, 124, 761.e1–761.e7. [Google Scholar] [CrossRef] [PubMed]
- Mejía, J.B.C.; Wakabayashi, K.; Nakamura, T.; Yatani, H. Influence of abutment tooth geometry on the accuracy of conventional and digital methods of obtaining dental impressions. J. Prosthet. Dent. 2017, 118, 392–399. [Google Scholar] [CrossRef]
- Jeong, I.D.; Kim, W.C.; Park, J.; Kim, C.M.; Kim, J.H. Ceramic molar crown reproducibility by digital workflow manufacturing: An in vitro study. J. Adv. Prosthodont. 2017, 9, 252–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revilla-León, M.; Subramanian, S.G.; Özcan, M.; Krishnamurthy, V.R. Clinical study of the influence of ambient light scanning conditions on the accuracy (trueness and precision) of an intraoral scanner. J. Prosthodont. 2020, 29, 107–113. [Google Scholar] [CrossRef]
- Wang, W.; Yu, H.; Liu, Y.; Jiang, X.; Gao, B. Trueness analysis of zirconia crowns fabricated with 3-dimensional printing. J. Prosthet. Dent. 2019, 121, 285–291. [Google Scholar] [CrossRef]
- Li, R.; Chen, H.; Wang, Y.; Zhou, Y.; Shen, Z.; Sun, Y. Three-dimensional trueness and margin quality of monolithic zirconia restorations fabricated by additive 3D gel deposition. J. Prosthodont. Res. 2020, 64, 478–484. [Google Scholar] [CrossRef]
- Yu, B.Y.; Son, K.; Lee, K.B. Evaluation of intaglio surface trueness and margin quality of interim crowns in accordance with the build angle of stereolithography apparatus 3-dimensional printing. J. Prosthet. Dent. 2020, in press. [Google Scholar] [CrossRef]
- Lee, B.I.; You, S.G.; You, S.M.; Kang, S.Y.; Kim, J.H. Effect of rinsing time on the accuracy of interim crowns fabricated by digital light processing: An in vitro study. J. Adv. Prosthodont. 2021, 13, 24–35. [Google Scholar] [CrossRef]
- Srinivasan, M.; Cantin, Y.; Mehl, A.; Gjengedal, H.; Müller, F.; Schimmel, M. CAD/CAM milled removable complete dentures: An in vitro evaluation of trueness. Clin. Oral Investig. 2017, 21, 2007–2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalberer, N.; Mehl, A.; Schimmel, M.; Müller, F.; Srinivasan, M. CAD-CAM milled versus rapidly prototyped (3D-printed) complete dentures: An in vitro evaluation of trueness. J. Prosthet. Dent. 2019, 121, 637–643. [Google Scholar] [CrossRef]
- Jang, D.; Son, K.; Lee, K.B. A Comparative study of the fitness and trueness of a three-unit fixed dental prosthesis fabricated using two digital workflows. Appl. Sci. 2019, 9, 2778. [Google Scholar] [CrossRef] [Green Version]
- Ender, A.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef] [Green Version]
- Fukazawa, S.; Odaira, C.; Kondo, H. Investigation of accuracy and reproducibility of abutment position by intraoral scanners. J. Prosthodont. Res. 2017, 61, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Methani, M.M.; Revilla-León, M.; Zandinejad, A. The potential of additive manufacturing technologies and their processing parameters for the fabrication of all-ceramic crowns: A review. J. Esthet. Dent. 2020, 32, 182–192. [Google Scholar] [CrossRef]
- Quan, H.; Zhang, T.; Xu, H.; Luo, S.; Nie, J.; Zhu, X. Photo-curing 3D printing technique and its challenges. Bioact. Mater. 2020, 5, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Goyanes, A.; Gaisford, S.; Basit, A.W. Stereolithographic (SLA) 3D printing of oral modified-release dosage forms. Int. J. Pharm. 2016, 503, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Zhao, L.; Jian, M.; Mao, Y.; Yu, M.; Guo, X. EHMP-DLP: Multi-projector DLP with energy homogenization for large-size 3D printing. Rapid Prototyp. J. 2018, 24, 1500–1510. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Evaluated Region | Manufacturing | Mean | SD | 95% Confidence Interval (CI) | Minimum | Maximum | F | p | |
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Whole region | SLA | 25.7 A | 5.1 | 22.8 | 28.6 | 18 | 34.2 | 66.684 | <0.001 * |
| DLP | 29.5 A | 3.3 | 27.6 | 31.3 | 24.4 | 36.8 | |||
| Milling | 44.8 B | 5.5 | 41.7 | 47.9 | 33 | 53.2 | |||
| Marginal region | SLA | 26.7 A | 4.4 | 24.2 | 29.2 | 20.2 | 34 | 45.267 | <0.001 * |
| DLP | 27.0 A | 4.7 | 24.3 | 29.6 | 20.4 | 37.3 | |||
| Milling | 45.2 B | 8.2 | 40.6 | 49.8 | 35.8 | 59.4 | |||
| Axial region | SLA | 27.6 A | 6.5 | 24 | 31.3 | 17.6 | 40.9 | 47.674 | <0.001 * |
| DLP | 30.9 A | 5.6 | 27.8 | 34 | 23.6 | 40.6 | |||
| Milling | 50.5 B | 8.3 | 45.9 | 55.2 | 34 | 63.1 | |||
| Occlusal region | SLA | 23.6 A | 5.3 | 20.6 | 26.5 | 17 | 33.4 | 32.288 | <0.001 * |
| DLP | 29.0 B | 3.6 | 26.9 | 31 | 24.3 | 35.5 | |||
| Milling | 36.9 C | 4.4 | 34.4 | 39.3 | 29.1 | 45.5 | |||
| Evaluated Region | SLA | DLP | Milling |
|---|---|---|---|
| Whole region | 25.7 ± 5.1 | 29.5 ± 3.3 | 44.8 ± 5.5 A |
| Marginal region | 26.7 ± 4.4 | 27.0 ± 4.4 | 45.2 ± 8.2 A |
| Axial region | 27.6 ± 6.5 | 30.9 ± 5.6 | 50.5 ± 8.3 A |
| Occlusal region | 23.6 ± 5.3 | 29.0 ± 3.6 | 36.9 ± 4.4 B |
| F | 1.52 | 2.016 | 10.025 |
| p | 0.219 | 0.122 | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, K.; Lee, J.-H.; Lee, K.-B. Comparison of Intaglio Surface Trueness of Interim Dental Crowns Fabricated with SLA 3D Printing, DLP 3D Printing, and Milling Technologies. Healthcare 2021, 9, 983. https://doi.org/10.3390/healthcare9080983
Son K, Lee J-H, Lee K-B. Comparison of Intaglio Surface Trueness of Interim Dental Crowns Fabricated with SLA 3D Printing, DLP 3D Printing, and Milling Technologies. Healthcare. 2021; 9(8):983. https://doi.org/10.3390/healthcare9080983
Chicago/Turabian StyleSon, Keunbada, Jung-Ho Lee, and Kyu-Bok Lee. 2021. "Comparison of Intaglio Surface Trueness of Interim Dental Crowns Fabricated with SLA 3D Printing, DLP 3D Printing, and Milling Technologies" Healthcare 9, no. 8: 983. https://doi.org/10.3390/healthcare9080983
APA StyleSon, K., Lee, J. -H., & Lee, K. -B. (2021). Comparison of Intaglio Surface Trueness of Interim Dental Crowns Fabricated with SLA 3D Printing, DLP 3D Printing, and Milling Technologies. Healthcare, 9(8), 983. https://doi.org/10.3390/healthcare9080983