

Vertigo in Acute Stroke Is a Predictor of Brain Location but Is Not Related to Early Outcome: The Experience of Sagrat Cor Hospital of Barcelona Stroke Registry



Abstract
:1. Introduction
2. Materials and Methods
3. Results
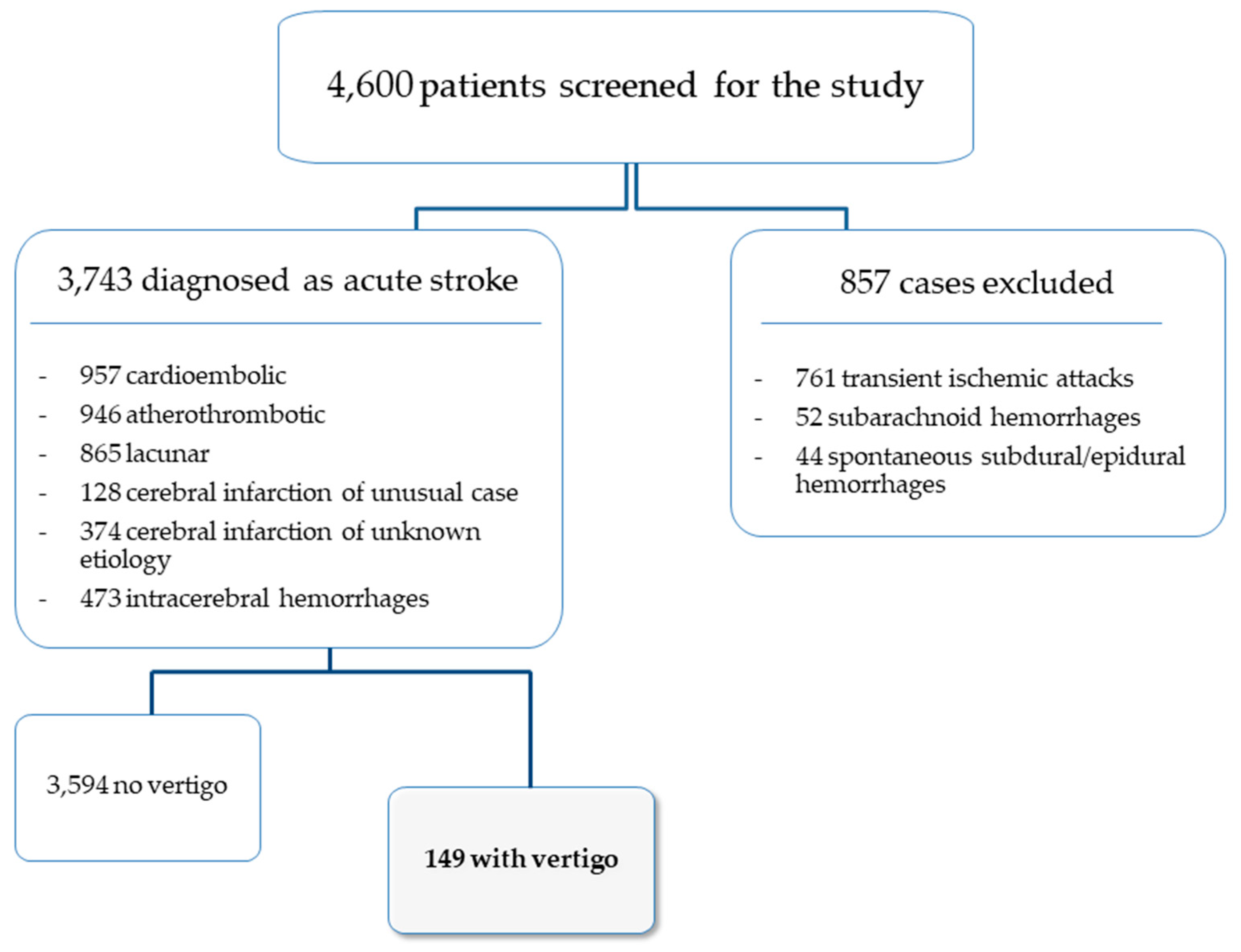
3.1. General Data
3.2. Differences between the Vertigo and the Non-Vertigo Acute Stroke Groups
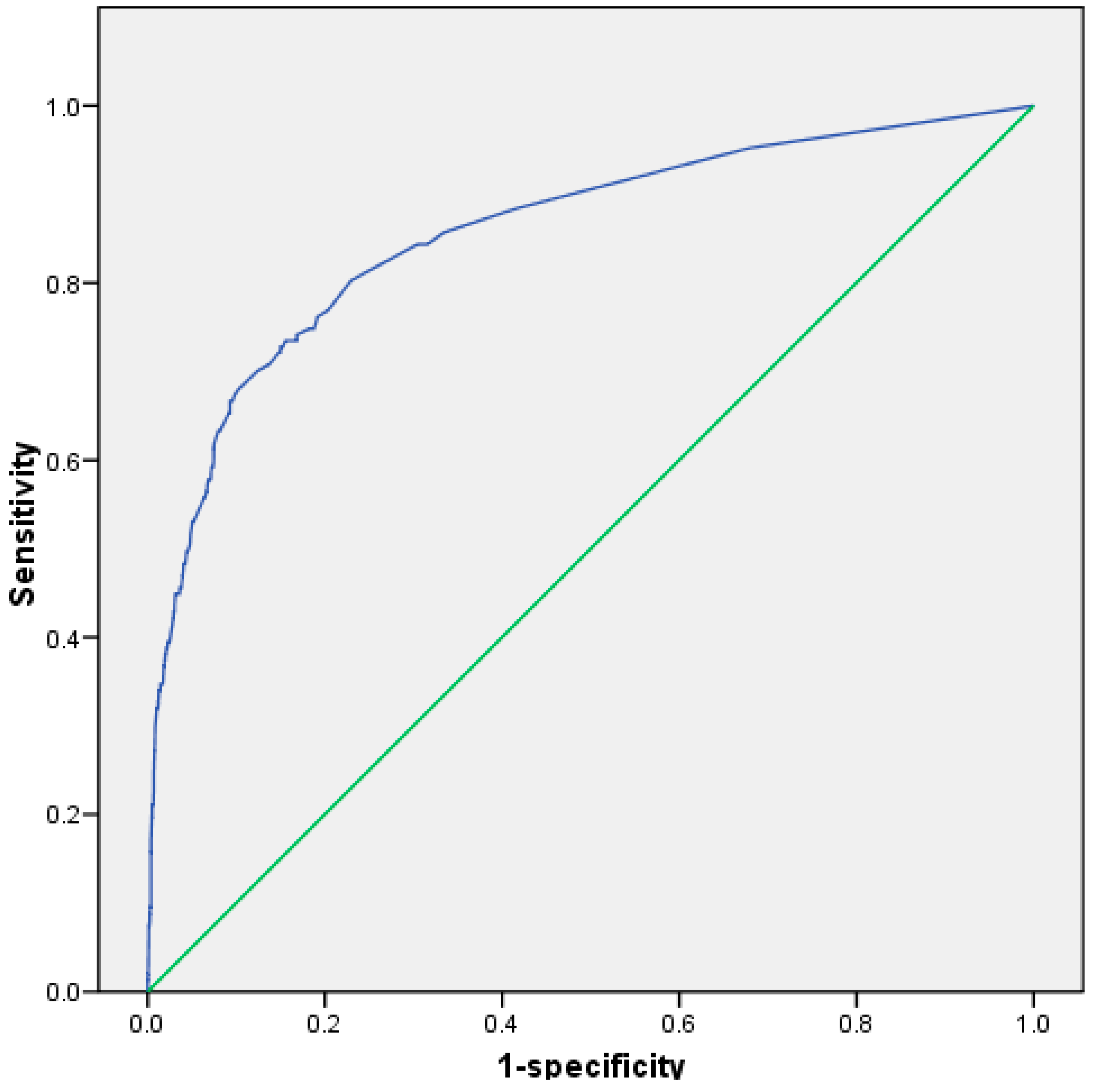
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Mao, R.; Zong, N.; Hu, Y.; Chen, Y.; Xu, Y. Neuronal Death Mechanisms and Therapeutic Strategy in Ischemic Stroke. Neurosci. Bull. 2022, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Mencl, S.; Garz, C.; Niklass, S.; Braun, H.; Göb, E.; Homola, G.; Heinze, H.J.; Reymann, K.G.; Kleinschnitz, C.; Schreiber, S. Early Microvascular Dysfunction in Cerebral Small Vessel Disease Is Not Detectable on 3.0 Tesla Magnetic Resonance Imaging: A Longitudinal Study in Spontaneously Hypertensive Stroke-Prone Rats. Exp. Transl. Stroke Med. 2013, 5, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruchoux, M.M.; Domenga, V.; Brulin, P.; Maciazek, J.; Limol, S.; Tournier-Lasserve, E.; Joutel, A. Transgenic Mice Expressing Mutant Notch3 Develop Vascular Alterations Characteristic of Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy. Am. J. Pathol. 2003, 162, 329–342. [Google Scholar] [CrossRef] [Green Version]
- Duering, M.; Csanadi, E.; Gesierich, B.; Jouvent, E.; Hervé, D.; Seiler, S.; Belaroussi, B.; Ropele, S.; Schmidt, R.; Chabriat, H.; et al. Incident Lacunes Preferentially Localize to the Edge of White Matter Hyperintensities: Insights into the Pathophysiology of Cerebral Small Vessel Disease. Brain 2013, 136, 2717–2726. [Google Scholar] [CrossRef] [Green Version]
- Zonneveld, T.P.; Richard, E.; Vergouwen, M.D.I.; Nederkoorn, P.J.; de Haan, R.; Roos, Y.B.; Kruyt, N.D. Blood Pressure-Lowering Treatment for Preventing Recurrent Stroke, Major Vascular Events, and Dementia in Patients with a History of Stroke or Transient Ischaemic Attack. Cochrane Database Syst. Rev. 2018, 7, CD007858. [Google Scholar] [CrossRef] [Green Version]
- Gasull, T.; Arboix, A. Molecular mechanisms and pathophysiology of acute stroke: Emphasis on biomarkers in the different stroke subtypes. Int. J. Mol. Sci. 2022, 23, 9476. [Google Scholar] [CrossRef]
- Kim, K.Y.; Shin, K.Y.; Chang, K.A. Potential Biomarkers for Post-Stroke Cognitive Impairment: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2022, 23, 602. [Google Scholar] [CrossRef]
- Cullell, N.; Gallego-Fábrega, C.; Cárcel-Márquez, J.; Muiño, E.; Llucià-Carol, L.; Lledós, M.; Martín-Campos, J.M.; Molina, J.; Casas, L.; Almería, M.; et al. ICA1L is associated with small vessel disease: A proteome-wide association study in small vessel stroke and intracerebral haemorrhage. Int. J. Mol. Sci. 2022, 23, 3161. [Google Scholar] [CrossRef]
- Wang, W.X.; Springer, J.E.; Hatton, K.W. MicroRNAs as Biomarkers for Predicting Complications Following Aneurysmal Subarachnoid Hemorrhage. Int. J. Mol. Sci. 2021, 22, 9492. [Google Scholar] [CrossRef]
- Giralt-Steinhauer, E.; Jiménez-Baladó, J.; Fernández-Pérez, I.; Rey, L.A.; Rodríguez-Campello, A.; Ois, A.; Cuadrado-Godia, E.; Jiménez-Conde, J.; Roquer, J. Genetics and epigenetics of spontaneous intracerebral hemorrhage. Int. J. Mol. Sci. 2022, 23, 6479. [Google Scholar] [CrossRef]
- Kumar, S.; Selim, M.; Caplan, L. Medical complications after stroke. Lancet Neurol. 2010, 9, 105–118. [Google Scholar] [CrossRef]
- Carrera, E.; Maeder-Ingvar, M.; Rossetti, A.O.; Devuyst, G.; Bogousslavsky, J. Trends in risk factors, paterns and causes in hospitalized strokes over 25 years: The Lausanne Stroke Registry. Cerebrovasc. Dis. 2007, 24, 97–103. [Google Scholar] [CrossRef] [PubMed]
- WHO. The Top 10 Causes of Death 9 December 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 30 March 2022).
- Chung, J.; Marini, S.; Pera, J.; Norrving, B.; Jimenez-Conde, J.; Roquer, J.; Fernandez-Cadenas, I.; Tirschwell, D.L.; Selim, M.; Brown, D.L.; et al. Genome-Wide Association Study of Cerebral Small Vessel Disease Reveals Established and Novel Loci. Brain 2019, 142, 3176–3189. [Google Scholar] [CrossRef] [PubMed]
- Luy, M.; Gast, K. Do women live longer or do men die earlier? Reflections on the causes of sex differences in life expectancy. Gerontology 2014, 60, 143–153. [Google Scholar] [CrossRef]
- Kobayashi, L.C.; Beeken, R.J.; Meisel, S.F. Biopsychosocial predictors of perceived life expectancy in a national sample of older men and women. Plos One 2017, 12, e0189245. [Google Scholar]
- Olindo, S.; Cabre, P.; Deschamps, R.; Chatot-Henry, C.; Rene-Corail, P.; Fournerie, P.; Saint-Vil, M.; May, F.; Smadja, D. Acute stroke in the very elderly. Epidemiological features, stroke subtypes, management, and outcome in Martinique, French West Indies. Stroke 2003, 34, 1593–1597. [Google Scholar] [CrossRef] [Green Version]
- Montaner, J.; Perea-Gainza, M.; Delgado, P.; Ribó, M.; Chacón, P.; Rosell, A.; Quintana, M.; Palacios, M.E.; Molina, C.A.; Alvarez-Sabín, J. Etiologic Diagnosis of Ischemic Stroke Subtypes with Plasma Biomarkers. Stroke 2008, 39, 2280–2288. [Google Scholar] [CrossRef] [Green Version]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients with Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e99. [Google Scholar] [CrossRef]
- Palomeras Soler, E.; Fossas Felip, P.; Casado Ruiz, V.; Cano Orgaz, A.; Sanz Cartagena, P.; Muriana Batiste, D. The Mataró Stroke Registry: A 10-year registry in a community hospital. Neurologia 2015, 30, 283–289. [Google Scholar] [CrossRef]
- Newman-Toker, D.E.; Della Santina, C.C.; Blitz, A. Vertigo and hearing loss. Handb. Clin. Neurol. 2016, 136, 905–921. [Google Scholar] [CrossRef]
- Choi, K.D.; Kim, J.S. Vascular vertigo: Updates. J. Neurol. 2019, 266, 1835–1843. [Google Scholar] [CrossRef] [PubMed]
- Phalgune, D.; Sankalia, D.; Kothari, S. Diagnosing Stroke in Acute Vertigo: Sensitivity and Specificity of HINTS Battery in Indian Population. Neurol. India. 2021, 69, 97–101. [Google Scholar] [CrossRef]
- Tehrani, A.S.S.; Kattah, J.C.; Kerber, K.A.; Gold, D.R.; Zee, D.S.; Urrutia, V.C.; Newman-Toker, D.E. Diagnosing stroke in acute dizziness and vertigo. Pitfalls and pearls. Stroke 2018, 49, 788–795. [Google Scholar] [CrossRef]
- Choi, J.; Lee, S.; Kim, J. Central vertigo. Curr. Opin. Neurol. 2018, 31, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Camps-Renom, P.; Delgado-Mederos, R.; Martínez-Domeño, A.; Prats-Sánchez, L.; Cortés-Vicente, E.; Simón-Talero, M.; Arboix, A.; Ois, Á.; Purroy, F.; Martí-Fàbregas, J. Clinical Characteristics and Outcome of the Capsular Warning Syndrome: A Multicenter Study. Int. J. Stroke 2015, 10, 571–575. [Google Scholar]
- Dieterich, M.; Brandt, T.H. Vestibular syndromes and vertigo. In Stroke Syndromes; Bogousslavsky, J., Caplan, L., Eds.; Cambridge University Press: Cambridge, UK, 1995; pp. 80–90. [Google Scholar]
- Jacova, C.; Pearce, L.A.; Costello, R.; McClure, L.A.; Holliday, S.L.; Hart, R.G.; Benavente, O.R. Cognitive impairment in lacunar strokes: The SPS3 trial. Ann. Neurol. 2012, 72, 351–362. [Google Scholar]
- Liu, W.; Liu, R.; Sun, W.; Peng, Q.; Zhang, W.; Xu, E.; Cheng, Y.; Ding, M.; Li, Y.; Hong, Z.; et al. Different impacts of blood pressure variability on the progression of cerebral microbleeds and white matter lesions. Stroke 2012, 43, 2916–2922. [Google Scholar]
- Arboix, A.; Roig, H.; Rossich, R.; Martínez, E.M.; García-Eroles, L. Differences between hypertensive and non-hypertensive ischemic stroke. Eur. J. Neurol. 2004, 11, 687–692. [Google Scholar]
- Bejot, Y.; Catteau, A.; Caillier, M.; Rouaud, O.; Durier, J.; Marie, C.; Di Carlo, A.; Osseby, G.V.; Moreau, T.; Giroud, M. Trends in incidence, risk factors, and survival in symptomatic lacunar stroke in Dijon, France, from 1989 to 2006. A population-based study. Stroke 2008, 39, 1945–1951. [Google Scholar]
- Hopf, H.C. Vertigo and masseter paresis. A new local brainstem syndrome probably of vascular origin. J. Neurol. 1987, 235, 42–45. [Google Scholar]
- Brickman, A.M.; Reit, C.Z.; Luchsinger, J.A.; Manly, J.J.; Schupf, N.; Muraskin, J.; DeCarli, C.; Brown, T.R.; Mayeux, R. Long-term blood pressure fluctuation and cerebrovascular disease in an elderly cohort. Arch. Neurol. 2010, 67, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A.; Rennie, M. Clinical study of 28 patients with cerebellar hemorrhage. Med. Clin. (Barc.) 2009, 132, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A. Cardiovascular risk factors for acute stroke: Risk profiles in the different subtypes of ischemic stroke. World. J. Clin. Cases. 2015, 3, 418–429. [Google Scholar] [CrossRef]
- Arboix, A.; Massons, J.; Oliveres, M.; García, L.; Titus, F. An analysis of 1000 consecutive patients with acute cerebrovascular disease. The registry of cerebrovascular disease of La Alianza-Hospital Central of Barcelona. Med. Clin. (Barc.) 1993, 101, 281–285. [Google Scholar] [PubMed]
- Arboix, A.; Alvarez-Sabin, J.; Soler, L. Stroke. Classification and diagnostic criteria. Ad hoc Editorial Committee of the Task Force on Cerebrovascular Diseases of SEN. Neurologia 1998, 13 (Suppl. S3), S3–S10. [Google Scholar]
- Special Report from the National Institute of Neurological Disorders and Stroke: Classification of cerebrovascular diseases III. Stroke 1990, 21, 637–676. [CrossRef] [Green Version]
- Bisdorff, A.; Von Brevern, M.; Lempert, T.; Newmn-Toker, D.E. Classification of vestibular symptoms: Towards an International classification of vestibular disorders. J. Vestib. Res. 2009, 19, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bamford, J.M.; Sandercock, P.A.; Warlow, C.P.; Slattery, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1989, 20, 828. [Google Scholar] [CrossRef]
- Choi, J.; Lee, S.; Kim, J. Ischemic syndromes causing dizziness and vertigo. Handb. Clin. Neurol. 2016, 137, 317–340. [Google Scholar] [CrossRef]
- Von Brevern, M.; Süßmilch, S.; Zeise, D. Acute vertigo due to hemispheric stroke. J. Neurol. Sci. 2014, 339, 153–156. [Google Scholar] [CrossRef]
- Khansa, A.; Cahyani, A.; Amalia, L. Clinical profile of stroke patients with vertigo in Hasan Sadikin General Hospital Bandung Neurology Ward. J. Med. Health. 2019, 2, 856–866. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Lee, H. Vertigo Due to Posterior Circulation Stroke. Semin. Neurol. 2013, 33, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Sohn, S.I.; Cho, Y.W.; Lee, S.R.; Ahn, B.H.; Park, B.R.; Baloh, R.W. Cerebellar infarction presenting isolated vertigo: Frequency and vascular topographical patterns. Neurology 2006, 67, 1178–1183. [Google Scholar] [CrossRef]
- Jiang, S.; Yan, Y.; Yang, T.; Zhu, Q.; Wang, C.; Bai, X.; Hao, Z.; Zhang, S.; Yang, Q.; Fan, Z.; et al. Plaque Distribution Correlates with Morphology of Lenticulostriate Arteries in Single Subcortical Infarctions. Stroke 2020, 51, 2801–2809. [Google Scholar] [CrossRef]
- Boehme, A.K.; McClure, L.A.; Zhang, Y.; Luna, J.M.; Del Brutto, O.H.; Benavente, O.R.; Elkind, M.S.V. Inflammatory Markers and Outcomes after Lacunar Stroke: Levels of Inflammatory Markers in Treatment of Stroke Study. Stroke 2016, 47, 659–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavallée, P.C.; Labreuche, J.; Faille, D.; Huisse, M.G.; Nicaise-Roland, P.; Dehoux, M.; Gongora-Rivera, F.; Jaramillo, A.; Brenner, D.; Deplanque, D.; et al. Circulating Markers of Endothelial Dysfunction and Platelet Activation in Patients with Severe Symptomatic Cerebral Small Vessel Disease on Behalf of the Lacunar-B.I.C.H.A.T. Investigators. Cerebrovasc. Dis. 2013, 36, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Fan, Z.; Kong, Q.; Xiao, J.; Wu, F.; An, J.; Yang, Q.; Li, D.; Zhuo, Y. Visualization of the Lenticulostriate Arteries at 3T Using Black-Blood T1-Weighted Intracranial Vessel Wall Imaging: Comparison with 7T TOF-MRA. Eur. Radiol. 2019, 29, 1452–1459. [Google Scholar] [CrossRef] [PubMed]
- Iadecola, C.; Parikh, N.S. Blood pressure ups and downs foreshadow cerebral microangiopathy. J. Am. Coll. Cardiol. 2020, 75, 2400–2402. [Google Scholar] [CrossRef]
- Elhfnawy, A.M.; El-Raouf, M.A.; Volkmann, J.; Fluri, F.; Elsalamawy, D. Relation of infarction location and volume to vertigo in vertebrobasilar stroke. Brain Behav. 2020, 10, e01564. [Google Scholar] [CrossRef]
- Maida, C.D.; Norrito, R.L.; Daidone, M.; Tuttolomondo, A.; Pinto, A. Neuroinflammatory mechanisms in ischemic stroke: Focus on cardioembolic stroke, background, and therapeutic approaches. Int. J. Mol. Sci. 2020, 21, 6454. [Google Scholar] [CrossRef]
- Chen, Y.; Pu, J.; Liu, Y.; Tian, L.; Chen, X.; Gui, S.; Xu, S.; Song, X.; Xie, P. Pro-inflammatory cytokines are associated with the development of post-stroke depression in the acute stage of stroke: A meta-analysis. Top Stroke Rehabil. 2020, 27, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Mustanoja, S.; Putaala, J.; Koivunen, R.J.; Surakka, I.; Tatlisumak, T. Blood pressure levels in the acute phase after intracerebral hemorrhage are associated with mortality in young adults. Eur. J. Neurol. 2018, 8, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A.; García-Plata, C.; García-Eroles, L.; Massons, J.; Comes, E. Clinical study of 99 patients with pure sensory stroke. J. Neurol. 2005, 252, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Rudilosso, S.; Rodríguez-Vázquez, A.; Urra, X.; Arboix, A. The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke. Int. J. Mol. Sci. 2022, 23, 1497. [Google Scholar] [CrossRef]
- Purroy, F.; Montaner, J.; Molina, C.A.; Delgado, P.; Ribo, M.; Alvarez-Sabín, J. Patterns and predictors of early risk of recurrence after transient ischemic attack with respect to etiologic subtypes. Stroke 2007, 38, 3225–3229. [Google Scholar] [CrossRef] [Green Version]
- Tao, W.D.; Liu, M.; Fisher, M.; Wang, D.R.; Li, J.; Furie, K.L.; Wu, B.O. Posterior versus anterior circulation infarction: How different are the neurological deficits? Stroke 2012, 43, 2060–2065. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Kim, H.J.; Kim, J.S. Isolated vestibular syndrome due to brainstem and cerebellar lesions. J. Neurol. 2017, 264, 63–69. [Google Scholar] [CrossRef]
- Doijiri, R.; Uno, H.; Miyashita, K.; Ihara, M.; Nagatsuka, K. How commonly is stroke found in patients with isolated vertigo or dizziness attack? J. Stroke Cerebrovasc. Dis. 2016, 25, 2549–2552. [Google Scholar] [CrossRef]
- Lee, J.O.; Park, S.H.; Kim, H.J.; Kim, M.S.; Park, B.R.; Kim, J.S. Vulnerability of the vestibular organs to transient ischemia: Implications for isolated vascular vertigo. Neurosci. Lett. 2014, 558, 180–185. [Google Scholar] [CrossRef]
- Choi, K.D.; Lee, H.; Kim, J.S. Vertigo in brainstem and cerebellar strokes. Curr. Opin. Neurol. 2013, 28, 90–95. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.P.; Li, H.R.; Ma, Q.K.; Yin, S.; Peng, Y.F.; Zhang, H.L.; Zhao, M.; Zhang, S.L. Prevalence of stroke and hypoperfusion in patients with isolated vertigo and vascular risk factors. Front. Neurol. 2018, 9, 974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Kim, J.S. Acute diagnosis and management of stroke presenting dizziness or vertigo. Neurol. Clin. 2015, 33, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Zhang, L.; Zhang, R.; Duan, J.; Huang, J.; Qiu, D. Clinical features differ between patients with vertigo attack only and weakness attack accompanying vertigo before vertebrobasilar stroke: A retrospective study. Front. Neurol. 2022, 13, 928902. [Google Scholar] [CrossRef] [PubMed]
- Smirnov, M.; Destrieux, C.; Maldonado, I.L. Cerebral White Matter Vasculature: Still Uncharted? Brain 2021, 144, 3561–3575. [Google Scholar] [CrossRef] [PubMed]
- Muiño, E.; Fernández-Cadenas, I.; Arboix, A. Contribution of “Omic” Studies to the Understanding of CADASIL. A Systematic Review. Int. J. Mol. Sci. 2021, 22, 7357. [Google Scholar] [CrossRef] [PubMed]
- Meissner, A. Hypertension and the brain: A risk factor for more than heart disease. Cerebrovasc. Dis. 2016, 42, 255–262. [Google Scholar] [CrossRef]
- Harriott, A.M.; Karakaya, F.; Ayata, C. Headache after ischemic stroke: A systematic review and meta-analysis. Neurology 2020, 94, e75–e86. [Google Scholar] [CrossRef]
- Lebedeva, E.R.; Ushenin, A.V.; Gurary, N.M.; Tsypushkina, T.S.; Gilev, D.V.; Kislyak, N.V.; Olesen, J. Headache at onset of first-ever ischemic stroke: Clinical characteristics and predictors. Eur. J. Neurol. 2021, 28, 852–860. [Google Scholar] [CrossRef]
- Qiu, D.; Zhang, L.; Deng, J.; Xia, Z.; Duan, J.; Wang, J.; Zhang, R. New Insights Into Vertigo Attack Frequency as a Predictor of Ischemic Stroke. Front. Neurol. 2020, 11, 593524. [Google Scholar] [CrossRef]
- Di Stefano, V.; De Angelis, M.V.; Montemitro, C.; Russo, M.; Carrini, C.; di Giannantonio, M.; Brighina, F.; Onofrj, M.; Werring, D.J.; Simister, R. Clinical presentation of strokes confined to the insula: A systematic review of literature. Neurol. Sci. 2021, 42, 1697–1704. [Google Scholar] [CrossRef]
- Yokokawa, H.; Goto, A.; Terui, K.; Funami, Y.; Watanabe, K.; Yasumura, S. Prevalence of Metabolic Syndrome and Serum Marker Levels in Patients with Four Subtypes of Cerebral Infarction in Japan. J. Clin. Neurosci. 2008, 15, 769–773. [Google Scholar] [CrossRef]
- Gąsecki, D.; Kwarciany, M.; Nyka, W.; Narkiewicz, K. Hypertension, brain damage and cognitive decline. Curr. Hypertens. Rep. 2013, 15, 547–558. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Acute Stroke with Vertigo n = 149 | Acute Stroke without Vertigo n = 3594 | p Value |
|---|---|---|---|
| Age, years, mean (SD) | 71.8 (12.9) | 75.9 (11.6) | 0.0001 |
| Age ≥ 85 years old | 21 (14.3) | 827 (23) | 0.013 |
| Sex | 0.676 | ||
| Males | 79 (52.6) | 1757 (49.0) | |
| Females | 70 (47.6) | 1837 (51.1) | |
| Variable | Acute Stroke with Vertigo n = 149 | Acute Stroke without Vertigo n = 3594 | p Value |
|---|---|---|---|
| Risk factors | |||
| Hypertension | 96 (65.3) | 2094 (58.3) | 0.089 |
| Atrial fibrillation | 30 (20.4) | 1024 (28.5) | 0.033 |
| Hyperlipidemia | 38 (25.9) | 664 (18.5) | 0.025 |
| Diabetes mellitus | 34 (23.1) | 826 (23.0) | 0.517 |
| Ischemic heart disease | 22 (15.0) | 537 (14.0) | 0.534 |
| Heavy smoking (>20 cigarettes/day) | 22 (15.0) | 372 (10.4) | 0.074 |
| Chronic obstructive pulmonary disease | 7 (4.8) | 320 (8.9) | 0.081 |
| Nephropathy | 0 (0.0) | 137 (3.8) | 0.016 |
| Clinical findings | |||
| Headache | 58 (39.5) | 442 (12.3) | 0.0001 |
| Nausea, vomiting | 68 (46.3) | 260 (7.2) | 0.0001 |
| Limb weakness | 71 (48.3) | 2728 (75.9) | 0.0001 |
| Speech disturbances (dysarthria, aphasia) | 48 (32.7) | 1821 (50.7) | 0.0001 |
| Ataxia | 54 (36.7) | 204 (5.7) | 0.0001 |
| Cranial nerve palsy | 25 (17.0) | 174 (4.8) | 0.0001 |
| Neuroimaging findings topography | |||
| Frontal lobe | 9 (6.1) | 505 (14.1) | 0.006 |
| Parietal lobe | 14 (9.5) | 873 (24.3) | 0.0001 |
| Temporal lobe | 15 (10.2) | 884 (24.6) | 0.0001 |
| Internal capsule | 11 (7.5) | 648 (18.0) | 0.001 |
| Basal ganglia | 10 (6.8) | 503 (14) | 0.013 |
| Midbrain | 6 (4.1) | 45 (1.3) | 0.011 |
| Pons | 27 (18.4) | 185 (5.1) | 0.0001 |
| Medulla | 14 (9.5) | 35 (1.0) | 0.000 |
| Cerebellum | 46 (31.3) | 83 (2.3) | 0.0001 |
| Middle cerebral artery | 26 (17.7) | 1921 (53.5) | 0.0001 |
| Vertebral artery | 21 (14.3) | 101 (2.8) | 0.0001 |
| Basilar artery | 36 (24.5) | 226 (6.3) | 0.0001 |
| Posteroinferior cerebellar artery | 16 (10.9) | 20 (0.6) | 0.0001 |
| Anteroinferior cerebellar artery | 6 (4.1) | 11 (0.3) | 0.0001 |
| Superior cerebellar artery | 18 (12.2) | 32 (0.9) | 0.0001 |
| Stroke subtypes | 0.0001 | ||
| Atherothrombotic infarct | 51 (34.7) | 894 (24.9) | |
| Cardioembolic infarct | 27 (18.4) | 930 (25.9) | |
| Infarction of unknown cause | 22 (15) | 352 (9.8) | |
| Lacunar stroke | 14 (9.5) | 850 (23.7) | |
| Infarctions of unusual cause | 4 (2.7) | 124 (3.5) | |
| Intracerebral hemorrhage | 29 (19.7) | 444 (12.4) | |
| Outcome | |||
| Symptom-free at discharge | 21 (14.3) | 352 (15.4) | 0.723 |
| In-hospital death | 17 (11.6) | 523 (14.6) | 0.312 |
| Length of stay, days, median (interquartile range) | 12 (8–20) | 12 (8–20) | 0.977 |
| Prolonged hospital stay > 12 days | 65 (44.2) | 1695 (47.2) | 0.269 |
| Regression Model | Coefficient (β) | Standard Error | Odds Ratio (95% Confidence Interval) | p Value |
|---|---|---|---|---|
| Model based on demographics, risk factors, clinical characteristics, and cerebral and vascular topography | ||||
| Cerebellum | 1.721 | 0.278 | 5.59 (3.24–9.64) | 0.0001 |
| Nausea, vomiting | 1.500 | 0.214 | 4.48 (2.95–6.82) | 0.0001 |
| Medulla involvement | 1.055 | 0.401 | 2.87 (1.35–6.30) | 0.009 |
| Pons involvement | 0.870 | 0.325 | 2.39 (1.26–4.51) | 0.007 |
| Basilar artery involvement | 0.858 | 0.291 | 2.36 (1.33–4.17) | 0.003 |
| Ataxia | 0.846 | 0.256 | 2.33 (1.41–3.85) | 0.001 |
| Headache | 0.836 | 0.211 | 2.31 (1.53–3.49) | 0.0001 |
| Speech disturbances | −0.457 | 0.203 | 0.63 (0.42–0.94) | 0.025 |
| Limb weakness | −0.755 | 0.196 | 0.47 (0.32–0.69) | 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
d’Annunzio, A.; Arboix, A.; García-Eroles, L.; Sánchez-López, M.-J. Vertigo in Acute Stroke Is a Predictor of Brain Location but Is Not Related to Early Outcome: The Experience of Sagrat Cor Hospital of Barcelona Stroke Registry. Biomedicines 2022, 10, 2830. https://doi.org/10.3390/biomedicines10112830
d’Annunzio A, Arboix A, García-Eroles L, Sánchez-López M-J. Vertigo in Acute Stroke Is a Predictor of Brain Location but Is Not Related to Early Outcome: The Experience of Sagrat Cor Hospital of Barcelona Stroke Registry. Biomedicines. 2022; 10(11):2830. https://doi.org/10.3390/biomedicines10112830
Chicago/Turabian Styled’Annunzio, Angela, Adrià Arboix, Luís García-Eroles, and María-José Sánchez-López. 2022. "Vertigo in Acute Stroke Is a Predictor of Brain Location but Is Not Related to Early Outcome: The Experience of Sagrat Cor Hospital of Barcelona Stroke Registry" Biomedicines 10, no. 11: 2830. https://doi.org/10.3390/biomedicines10112830
APA Styled’Annunzio, A., Arboix, A., García-Eroles, L., & Sánchez-López, M. -J. (2022). Vertigo in Acute Stroke Is a Predictor of Brain Location but Is Not Related to Early Outcome: The Experience of Sagrat Cor Hospital of Barcelona Stroke Registry. Biomedicines, 10(11), 2830. https://doi.org/10.3390/biomedicines10112830