
Stroke-Prone SHR as Experimental Models for Cardiovascular Disease Risk Reduction in Humans

Abstract
:1. Introduction
2. Materials and Methods
3. Results
- (1)
- Experimental Prevention of Stroke in SHRSP.
- (2)
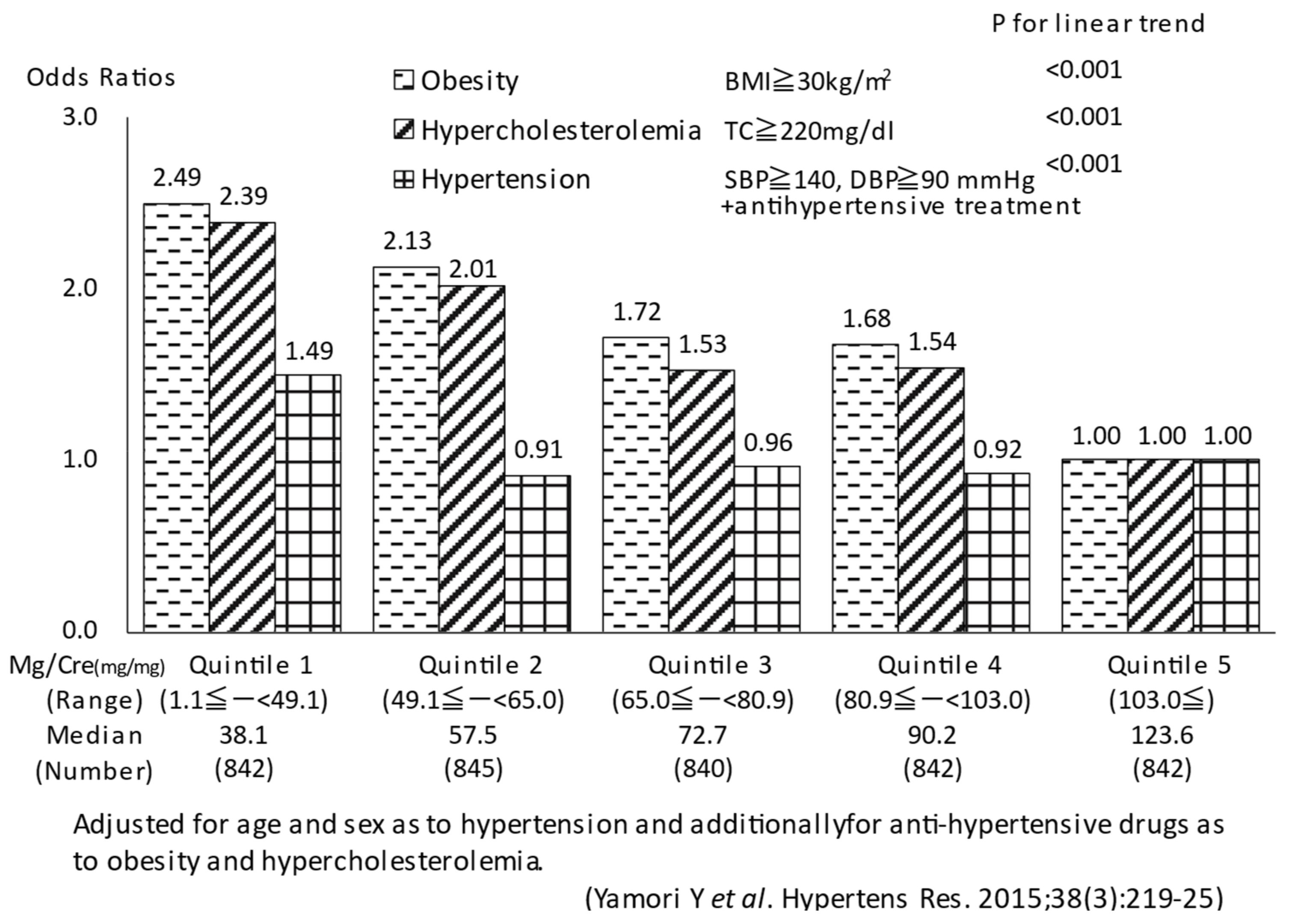
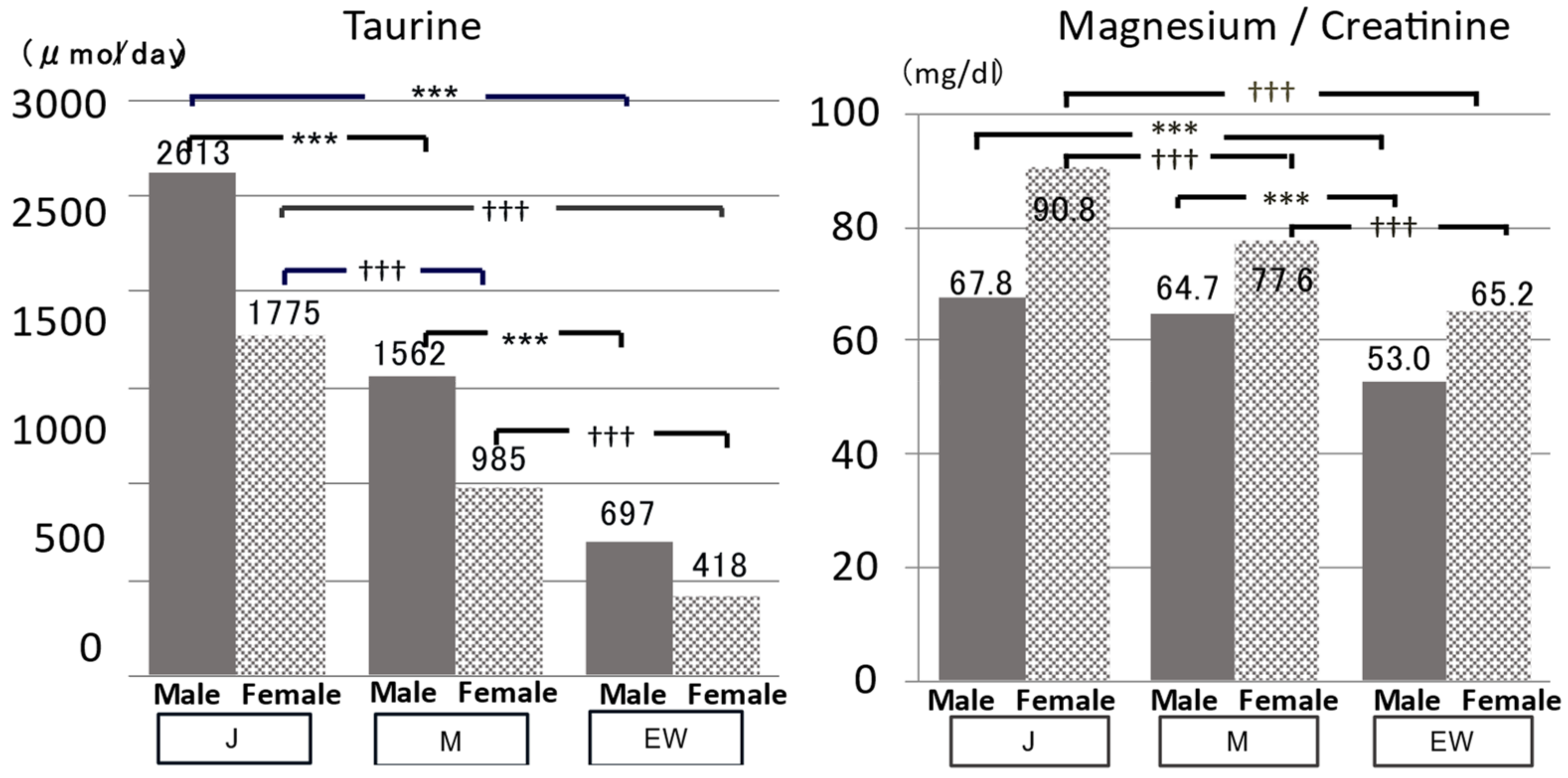
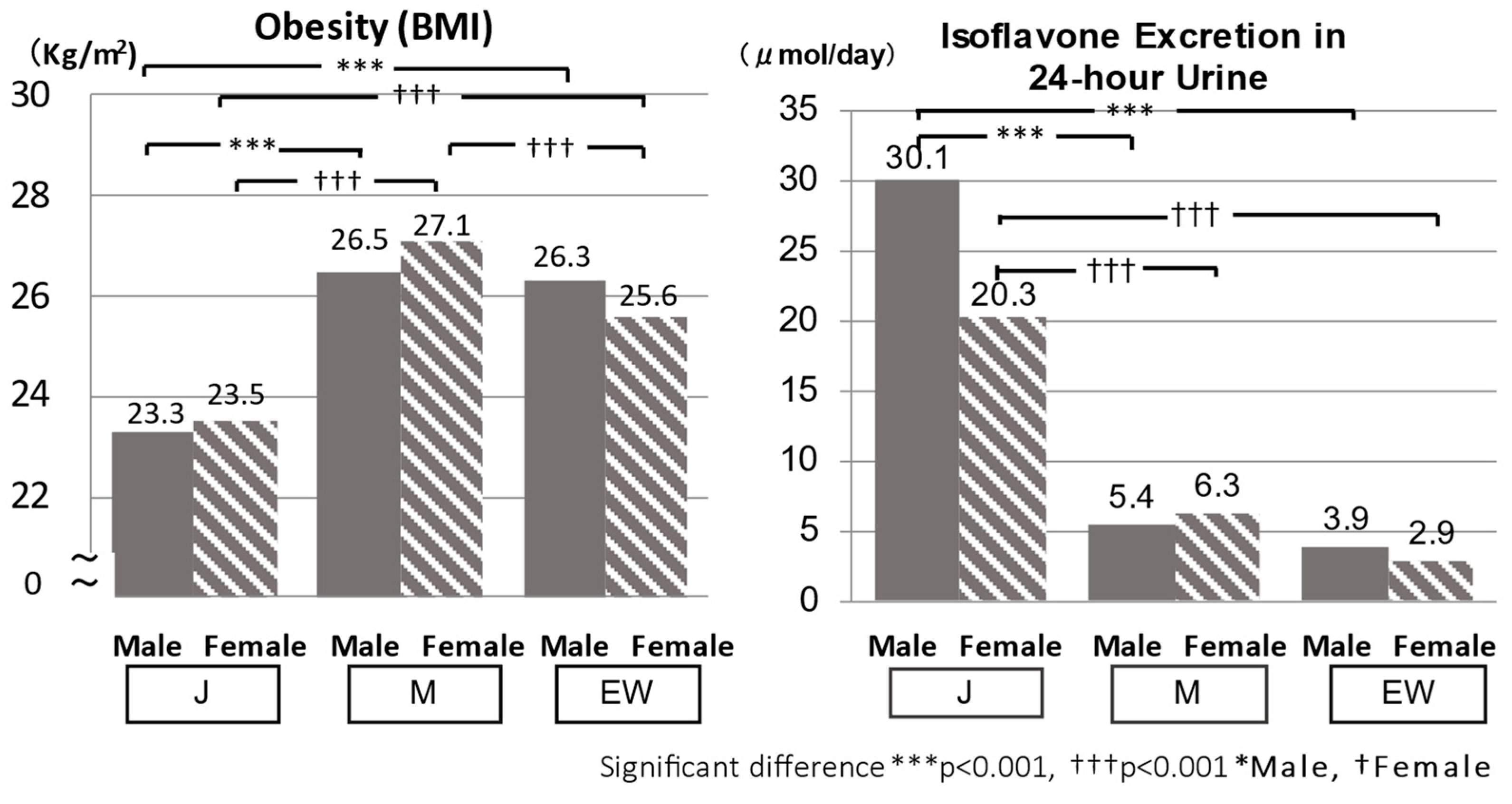
- The Association of Urinary Biomarkers with Cardiovascular Risks in the WHO-CARDIAC Study
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Okamoto, K.; Yamori, Y.; Nagaoka, A. Establishment of the stroke-prone spontaneously hypertensive rat (SHR). Circ. Res. 1974, 34 (Suppl. I), 143–153. [Google Scholar]
- Okamoto, K.; Aoki, K. Development of a Strain of Spontaneously Hypertensive Rats. Jpn. Circ. J. 1963, 27, 282–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamori, Y. The stroke-prone spontaneously hypertensive rat: Contribution to risk factor analysis and prevention of hypertensive diseases. In Handbook of Hypertension; De Jong, W., Ed.; Elsevier: Amsterdam, The Netherlands, 1984; pp. 240–255. [Google Scholar]
- Fredriksson, K.; Nordborg, C.; Kalimo, H.; Olsson, Y.; Johansson, B.B. Cerebral microangiopathy in stroke-prone spontaneously hypertensive rats. An immunohistochemical and ultrastructural study. Acta Neuropathol. Vol. 1988, 75, 241–252. [Google Scholar] [CrossRef]
- Bailey, E.L.; McCulloch, J.; Sudlow, C.; Wardlaw, J.M. Potential animal models of lacunar stroke: A systematic review. Stroke 2009, 40, e451–e458. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, J.M.; Smith, C.; Dichgans, M. Mechanisms underlying sporadic cerebral small vessel disease: Insights from neuroimaging. Lancet Neuurol 2013, 12, 483–497. [Google Scholar] [CrossRef] [Green Version]
- Rajani, R.M.; Quick, S.; Ruigrok, S.R.; Graham, D.; Harris, S.E.; Verhaaren, B.F.J.; Fornage, M.; Seshadri, S.; Atanur, S.S.; Dominiczak, A.F.; et al. Reversal of endothelial dysfunction reduces white matter vulnerability in cerebral small vessel disease in rats. Sci. Transl. Med. 2018, 10, eaam9507. [Google Scholar] [CrossRef] [Green Version]
- Bailey, E.L.; Smith, C.; Sudlow, C.L.M.; Wardlaw, J.M. Is the spontaneously hypertensive stroke prone rat a pertinent model of sub cortical ischemic stroke? A systematic review. Int. J. Stroke 2011, 6, 434–444. [Google Scholar] [CrossRef]
- Nagaoka, A.; Kakihana, M.; Fujiwara, K. Effects of idebenone on neurological deficits following cerebrovascular lesions in stroke-prone spontaneously hypertensive rats. Arch. Gerontol. Geriatr. 1989, 8, 203–212. [Google Scholar] [CrossRef]
- Yoshida, H.; Itoh, S.; Ferdousi, F.; Isoda, H. Post-stroke treatment with K-134, a phosphodiesterase 3 inhibitor, improves stroke outcomes in the stroke-prone spontaneously hypertensive rat model–A comparative evaluation of antiplatelet drugs. J. Pharmacol. Sci. 2022, 148, 229–237. [Google Scholar] [CrossRef]
- Rubattu, S.; Volpe, M.; Kreutz, R.; Ganten, U.; Ganten, D.; Lindpaintner, K. Chromosomal mapping of quantitative trait loci contributing to stroke in a rat model of complex human disease. Nat. Genet. 1996, 13, 429–434. [Google Scholar] [CrossRef]
- Jeffs, B.; Clark, J.S.; Anderson, N.H.; Gratton, J.; Brosnan, M.J.; Gauguier, D.; Reid, J.L.; Macrae, I.M.; Dominiczak, A.F. Sensitivity to cerebral ischaemic insult in a rat model of stroke is determined by a single genetic locus. Nat. Genet. 1997, 16, 364–367. [Google Scholar] [CrossRef]
- Rubattu, S.D.; Hubner, N.; Ganten, U.; Evangelista, A.; Stanzione, R.; Di Angelantonio, E.; Plehm, R.; Langanki, R.; Gianazza, E.; Sironi, L.; et al. Reciprocal congenic lines for a major stroke QTL on rat chromosome 1. Physiol. Genom. 2006, 27, 108–113. [Google Scholar] [CrossRef] [Green Version]
- Nabika, T.; Ohara, H.; Kato, N.; Isomura, M. The stroke-prone spontaneously hypertensive rat: Still a useful model for post-GWAS genetic studies? Hypertens. Res. 2012, 35, 477–484. [Google Scholar] [CrossRef]
- Ferdaus, M.Z.; Xiao, B.; Ohara, H.; Nemoto, K.; Harada, Y.; Saar, K.; Hübner, N.; Isomura, M.; Nabika, T. Identification of Stim1 as a candidate gene for exaggerated sympathetic response to stress in the stroke-prone spontaneously hypertensive rat. PLoS ONE 2014, 9, e95091. [Google Scholar] [CrossRef] [Green Version]
- Gandolgor, T.A.; Ohara, H.; Zong, H.C.; Hirashima, T.; Ogawa, T.; Saar, K.; Hübner, N.; Watanabe, T.; Isomura, M.; Nabika, T. Two genomic regions of crhromosomes 1 and 18 rexplain most of the stroke susceptibility under salt loading in stroke-prone spontaneously hypertensive rat/izm. Hypertension 2013, 62, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Takeuchi, F.; Liang, Y.-Q.; Isono, M.; Tajima, M.; Cui, Z.H.; Iizuka, Y.; Gotoda, T.; Nabika, T.; Kato, N. Integrative genomic analysis of blood pressure and related phenotypes in rats. Dis. Model. Mech. 2021, 14, dmm048090. [Google Scholar] [CrossRef]
- Yamori, Y.; Nara, Y.; Kihara, M.; Mano, M.; Horie, R. Simple method for sampling consecutive 24-h urine for epidemiological and clinical studies. Clin. Exp. Hypertens. 1984, 6, 1161–1167. [Google Scholar] [CrossRef]
- Yamori, Y. Predictive and preventive pathology of cardiovascular diseases. Acta Patho. Jpn. 1989, 39, 683–705. [Google Scholar] [CrossRef]
- CARDIAC Study Group (Ed.) Cardiovascular Diseases and Alimentary Comparison Study Protocol and Manual of Operations. WHO-Collaborating Center for Research on Primary Prevention of Cardiovascular Diseases, and Cardiovascular Diseases Unit; WHO: Shimane, Japan; Geneva, Switzerland, July 1986.
- CARDIAC Study Group. Excerpts from the WHO CARDIAC Study Protocol. J. Cardiovasc. Pharm. 1990, (Suppl. 8), S75–S77. [Google Scholar]
- Yamori, Y. Chapter 2, History of CARDIAC Study and food culture. Chapter 3, Nutrition for healthier ageing-Two decades of world-wide surveys on diet and human life. In Proceedings of the International Symposium, Food Culture: Development and Education 20-Year CARDIAC Study Symposium Supported by UNESCO; Paris, France, 4 October 2005, Nonprofit Organization World Health Frontier Institute: Nishinomiya, Japan, 2008; pp. 11–18, 23–41. [Google Scholar]
- Pounis, G.; Costanzo, S.; Bonaccio, M.; Di Castelnuovo, A.; de Curtis, A.; Ruggiero, E.; Persichillo, M.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; et al. Reduced mortality risk by a polyphenol-rich diet: An analysis from the Moli-sani study. Nutrition 2018, 48, 87–95. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Cesari, F.; Dinu, M.; Pagliai, G.; Rogolino, A.; Giusti, B.; Gori, A.; Casini, A.; Marcucci, R.; Sofi, F. Mediterranean, but not lacto-ovo-vegetarian, diet positively influence circulating progenitor cells for cardiovascular prevention: The CARDIVEG study. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Keenan, T.D.; Agrón, E.; Mares, J.A.; Clemons, T.E.; van Asten, F.; Swaroop, A.; Chew, E.Y. For the AREDS and AREDS2 Research Groups Adherence to a Mediterranean diet and cognitive function in the Age-Related Eye Disease Studies 1 & 2. Alzheimer’s Dement. 2020, 16, 831–842. [Google Scholar]
- Yamori, Y.; Nara, Y.; Tsubouchi, T.; Sogawa, Y.; Ikeda, K.; Horie, R. Dietary prevention of stroke and its mechanisms in stroke-prone spontaneously hypertensive rats—Preventive effect of dietary fibre and palmitoleic acid. J. Hypertens. 1986; 4, (Suppl. 3), S449–S452. [Google Scholar]
- Nara, Y.; Yamori, Y.; Lovenberg, W. Effect of dietary taurine on blood pressure in spontaneously hypertensive rats. Biochem. Pharm. 1978, 27, 2689–2692. [Google Scholar] [PubMed]
- Yamori, Y.; Liu, L.; Mizushima, S.; Ikeda, K.; Nara, Y. Male cardiovascular mortality and dietary markers in 25 population samples of 16 countries. J. Hypertens. 2006, 24, 1499–1505. [Google Scholar] [CrossRef]
- Yamori, Y. Food factors for atherosclerosis prevention: Asian perspective derived from analyses of worldwide dietary biomarkers. Exp. Clin. Cardiol. 2006, 11, 94–98. [Google Scholar]
- Adachi, M.; Nara, Y.; Mano, M.; Yamori, Y. Effect of dietary magnesium supplementation on intralymphocytic free calcium and magnesium in stroke-prone spontaneously hypertensive rats. Clin. Exp. Hypertens. 1994, 16, 317–326. [Google Scholar] [CrossRef]
- Sagara, M.; Murakami, S.; Mizushima, S.; Liu, L.; Mori, M.; Ikeda, K.; Nara, Y.; Yamori, Y. Taurine in 24-h urine samples is inversely related to cardiovascular risks of middle aged subjects in 50 populations of the world. Med. Biol. 2015, 803, 623–635. [Google Scholar]
- Yamori, Y.; Sagara, M.; Mizushima, S.; Liu, L.; Ikeda, K.; Nara, Y. An inverse association between magnesium in 24-h urine and cardiovascular risk factors in middle-aged subjects in 50 CARDIAC Study populations. Hypertens Res. 2015, 38, 219–225. [Google Scholar] [CrossRef]
- Yamori, Y. Worldwide epidemic of obesity: Hope for Japanese diets. Clin. Exp. Pharm. Physiol. 2004, 31 (Suppl. 2), 2–4. [Google Scholar] [CrossRef]
- Villa-Etchegoyen, C.; Lombarte, M.; Matamoros, N.; Belizán, J.M.; Cormick, G. Mechanisms involved in the relationship between low calcium intake and high blood pressure. Nutrients 2019, 11, 1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghazali, S.; Barratt, T.M. Urinary excretion of calcium and magnesium in children. Arch. Dis. Child. 1974, 49, 97–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stapleton, F.B.; Noe, H.N.; Jerkins, G.; Roy, S., III. Urinary excretion of calcium following an oral calcium loading test in healthy children. Pediatrics 1982, 69, 594–597. [Google Scholar] [CrossRef] [PubMed]
- Knapp, E.L. Factors influencing the urinary excretion of calcium. I. In normal persons. J. Clin. Invest. 1947, 26, 182–202. [Google Scholar] [CrossRef] [PubMed]
- Sontia, B.; Touyz, R.M. Role of magnesium in hypertension. Arch. Biochem. Biophys. 2007, 458, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Hatzistavri, L.S.; Sarafidis, P.A.; Georgianos, P.I.; Tziolas, I.M.; Aroditis, C.P.; Zebekakis, P.E.; Pikilidou, M.I.; Lasaridis, A.N. Oral magnesium supplementation reduces ambulatory blood pressure in patients with mild hypertension. Am. J. Hypertens. 2009, 22, 1070–1075. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Sawamura, M.; Nara, Y.; Ikeda, K.; Yamori, Y. Direct inhibitory effects of taurine on norepinephrine-induced contraction in mesenteric artery of stroke-prone spontaneously hypertensive rats. Adv. Exp. Med. Biol. 1996, 403, 257–262. [Google Scholar]
- Mizushima, S.; Nara, Y.; Sawamura, M.; Yamori, Y. Effects of oral taurine supplementation on lipids and sympathetic nerve tone. Amino. Acids 1996, 46, 73–80. [Google Scholar]
- Nielsen, F.H. Magnesium, inflammation, and obesity in chronic disease. Nutr. Rev. 2010, 68, 333–340. [Google Scholar] [CrossRef]
- He, K.; Liu, K.; Daviglus, M.L.; Morris, S.J.; Loria, C.M.; Van Horn, L.; Jacobs, D.R.; Savage, P.J. Magnesium intake and incidence of metabolic syndrome among young adults. Circulation 2006, 113, 1675–1682. [Google Scholar] [CrossRef] [Green Version]
- Fujihira, E.; Takahashi, H.; Nakazawa, M. Effect of long-term feeding of taurine in hereditary hyperglycemic obese mice. Chem. Pharm. Bull. 1970, 18, 1636–1642. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Bi, L.F.; Fang, J.H.; Su, X.L.; Da, G.L.; Kuwamori, T.; Kagamimori, S. Beneficial effects of taurine on serum lipids in overweight or obese non-diabetic subjects. Amino Acids 2003, 26, 267–271. [Google Scholar] [CrossRef]
- Truswell, A.S. Dietary fibre and blood lipids. Curr. Opin. Lipidol. 1995, 6, 14–19. [Google Scholar] [CrossRef]
- Brown, L.; Rosner, B.; Willett, W.W.; Sacks, F.M. Cholesterol-lowering effects of dietary fiber: A meta-analysis. Am. J. Clin. Nutr. 1999, 69, 30–42. [Google Scholar] [CrossRef] [Green Version]
- Murakami, S.; Kondo, Y.; Toda, Y.; Kitajima, H.; Kameo, K.; Sakono, M.; Fukuda, N. Effect of taurine on cholesterol metabolism in hamsters: Up-regulation of low density lipoprotein (LDL) receptor by taurine. Life Sci. 2002, 70, 2355–2366. [Google Scholar] [CrossRef]
- Murakami, S.; Sakurai, T.; Tomoike, H.; Sakono, M.; Nasu, T.; Fukuda, N. Prevention of hypercholesterolemia and atherosclerosis in the hyperlipidemia- and atherosclerosis-prone Japanese (LAP) quail by taurine supplementation. Amino Acids 2010, 38, 271–278. [Google Scholar] [CrossRef]
- Richards, M. A brief review of the archaeological evidence for Palaeolithic and Neolithic subsistence. Eur. J. Clin. Nutr. 2002, 56, 1270–1278. [Google Scholar] [CrossRef]
- TSMD, Torihama Shell Midden Research Group. The Torihama shell midden—A preliminary report of the excavation in 1984. Fukui Prefecture Education Board and Wakasa History Art Folklore Museum Fukui, Japan, 1985. 2-104, Onyu, Obama, Fukui 917-0241, Japan. Available online: https://wakahaku.pref.fukui.lg.jp/ (accessed on 30 August 2016).
- World Health Statistics 2016: Monitoring Health for the SDGs. Available online: https://www.who.int/publications/i/item/9789241565264 (accessed on 30 August 2016).
- Mori, M.; Sagara, M.; Mori, H.; Yamori, Y. Grading of Japanese diet intakes by 24-h urine analysis of taurine and soy isoflavones in relation to cardiovascular risks. Adv. Exp. Med. Biol. 2022, 1370, 173–184. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | N | Dietary Contents | Ca, Mg Contents |
|---|---|---|---|
| Control Diet (CD) | 10 | Control Diet (Crude Protein: 24.6%) | Ca 0.7%, Mg 0.2% |
| CD + Ca | 15 | CD (Ca 0.7%, Mg 0.2%) + Ca (0.9%) | Ca 1.6%, Mg 0.2% |
| CD + Mg | 15 | CD (Ca 0.7%, Mg 0.2%) + Mg (0.6%) | Ca 0.7%, Mg 0.8% |
| Soy Protein Diet (SD) | 15 | Soy Protein Diet (Soy Protein: 24.6%) | Ca 0.7%, Mg 0.2% |
| SD + Ca | 15 | SD (Ca 0.7%, Mg 0.2%) + Ca (0.9%) | Ca 1.6%, Mg 0.2% |
| SD + Ca + Mg | 15 | SD (Ca0.7%, Mg 0.2%) + Ca (0.9%) + Mg (0.6%) | Ca 1.6%, Mg 0.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamori, Y.; Sagara, M.; Mori, H.; Mori, M., on behalf of the CARDIAC Study Group. Stroke-Prone SHR as Experimental Models for Cardiovascular Disease Risk Reduction in Humans. Biomedicines 2022, 10, 2974. https://doi.org/10.3390/biomedicines10112974
Yamori Y, Sagara M, Mori H, Mori M on behalf of the CARDIAC Study Group. Stroke-Prone SHR as Experimental Models for Cardiovascular Disease Risk Reduction in Humans. Biomedicines. 2022; 10(11):2974. https://doi.org/10.3390/biomedicines10112974
Chicago/Turabian StyleYamori, Yukio, Miki Sagara, Hideki Mori, and Mari Mori on behalf of the CARDIAC Study Group. 2022. "Stroke-Prone SHR as Experimental Models for Cardiovascular Disease Risk Reduction in Humans" Biomedicines 10, no. 11: 2974. https://doi.org/10.3390/biomedicines10112974
APA StyleYamori, Y., Sagara, M., Mori, H., & Mori, M., on behalf of the CARDIAC Study Group. (2022). Stroke-Prone SHR as Experimental Models for Cardiovascular Disease Risk Reduction in Humans. Biomedicines, 10(11), 2974. https://doi.org/10.3390/biomedicines10112974