

Impact of Wound Dressing on Mechanotransduction within Tissues of Chronic Wounds

 , ,
, , 
Abstract
:1. Introduction
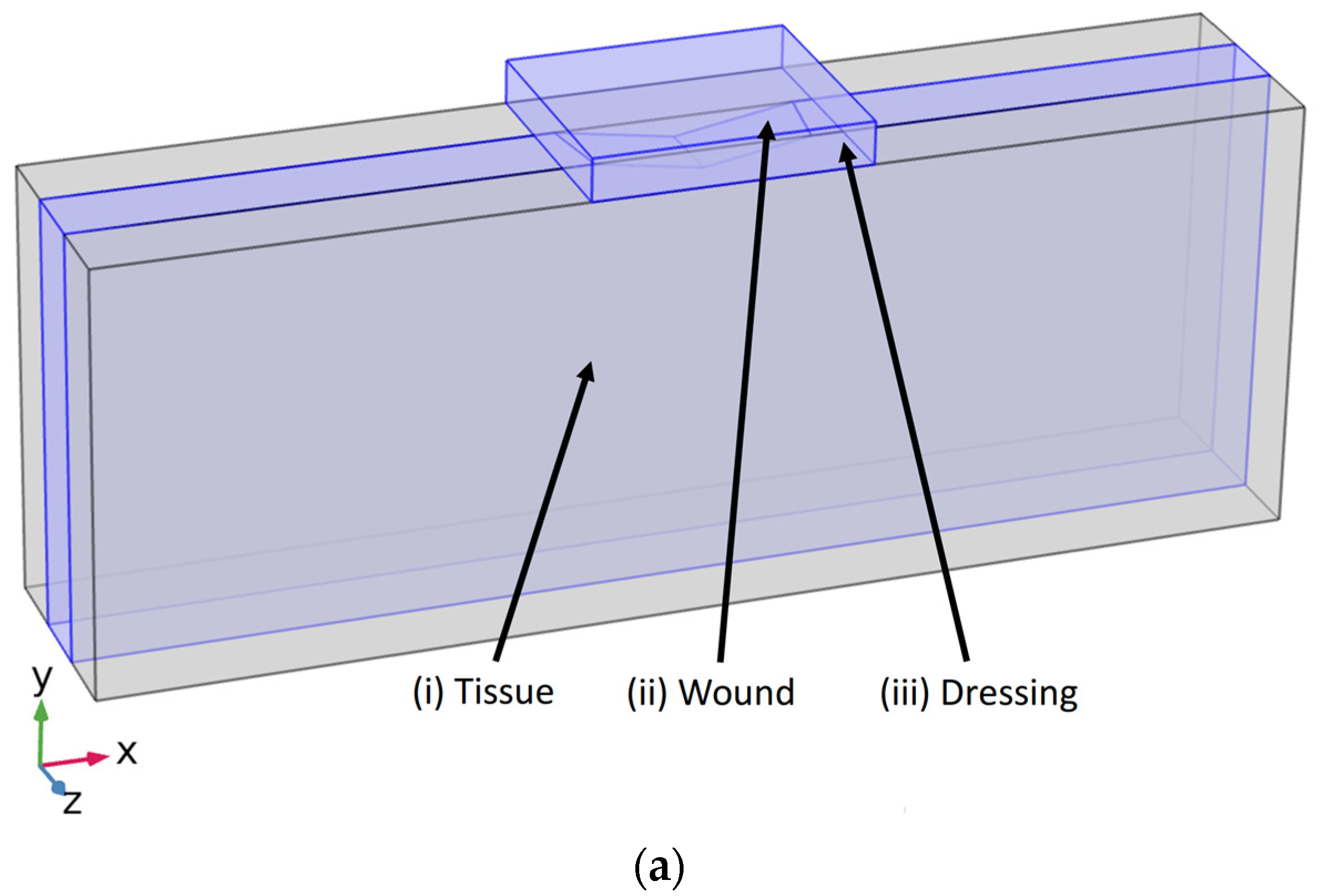
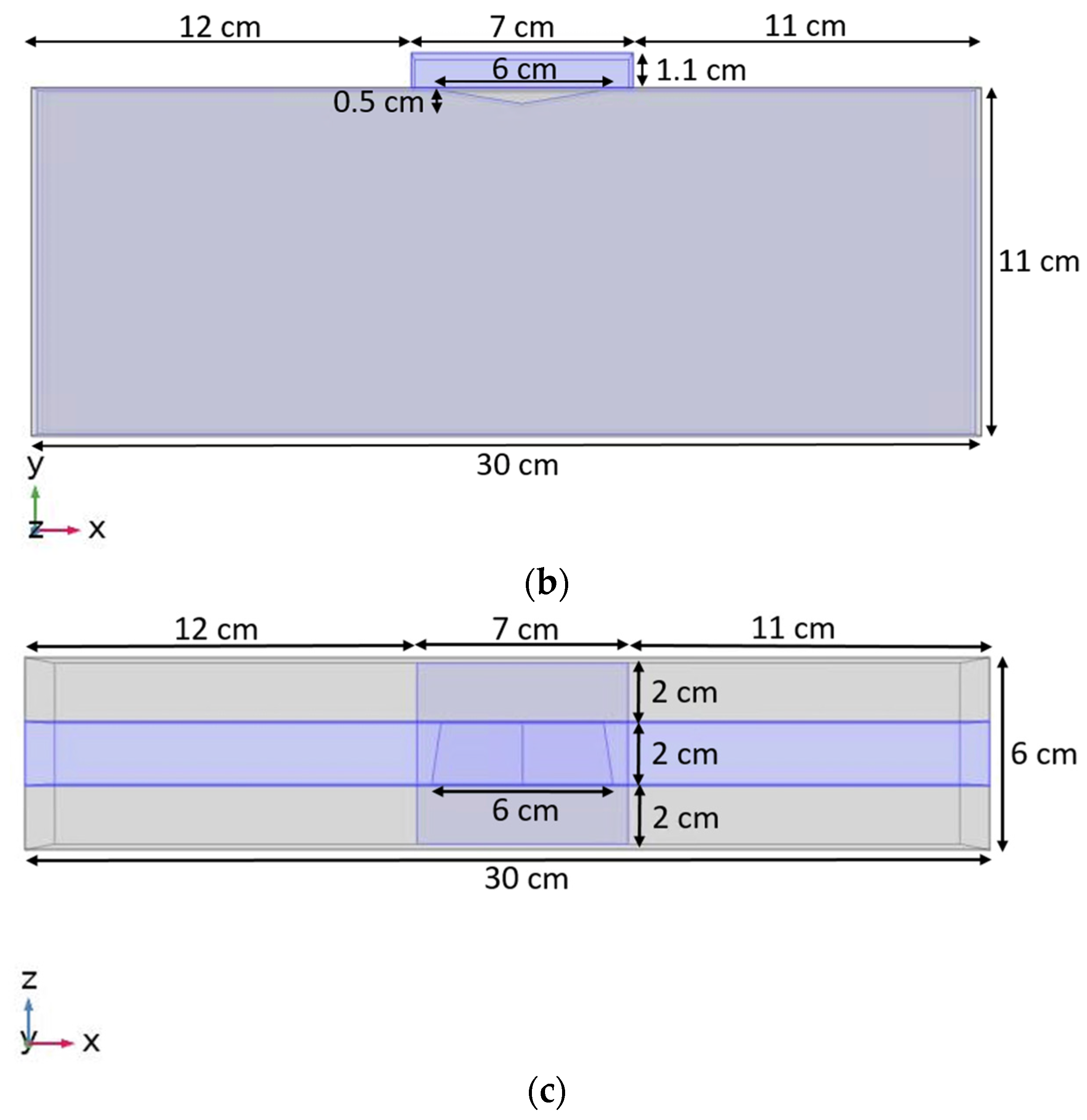
2. Materials and Methods
3. Results
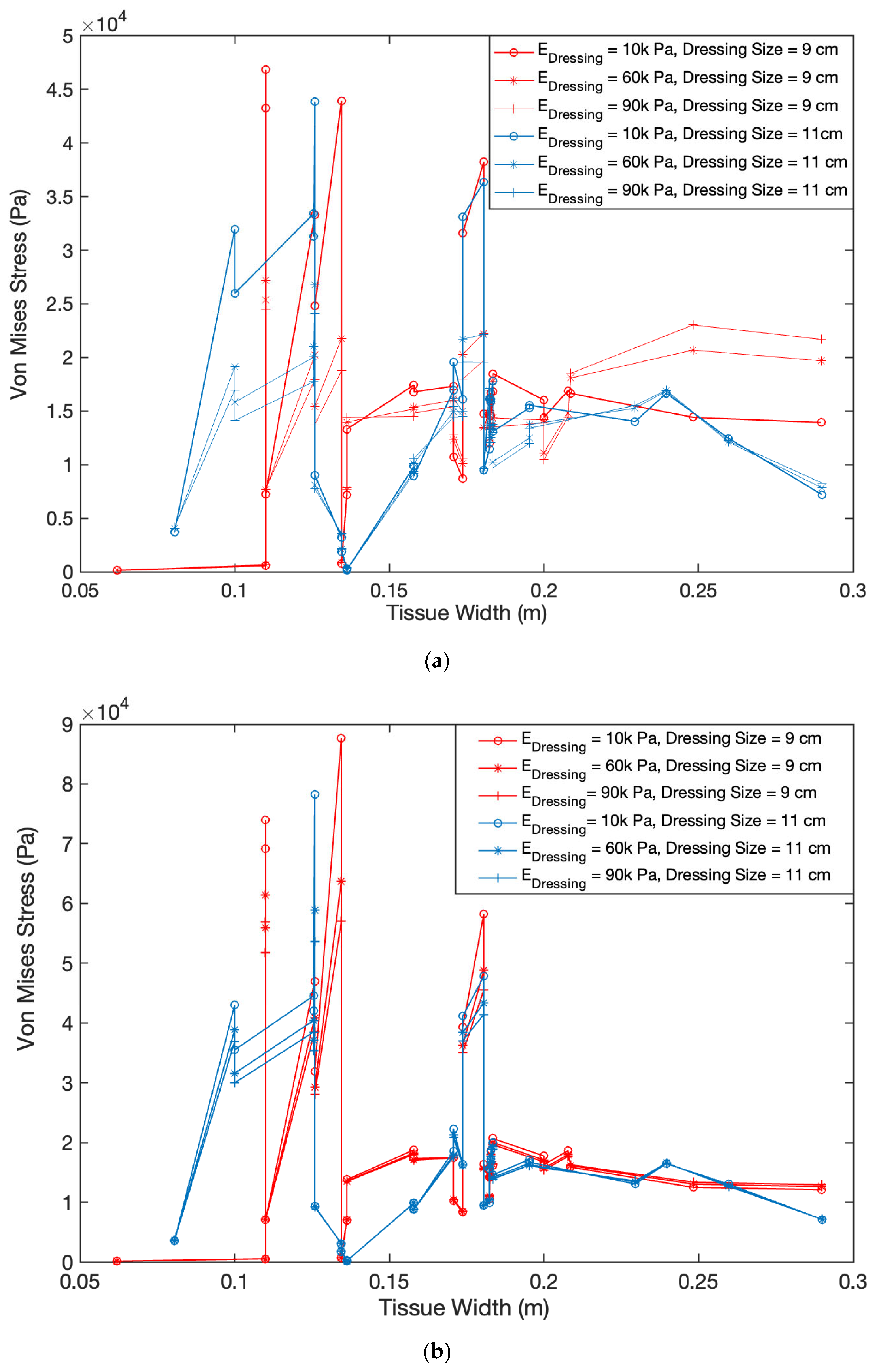
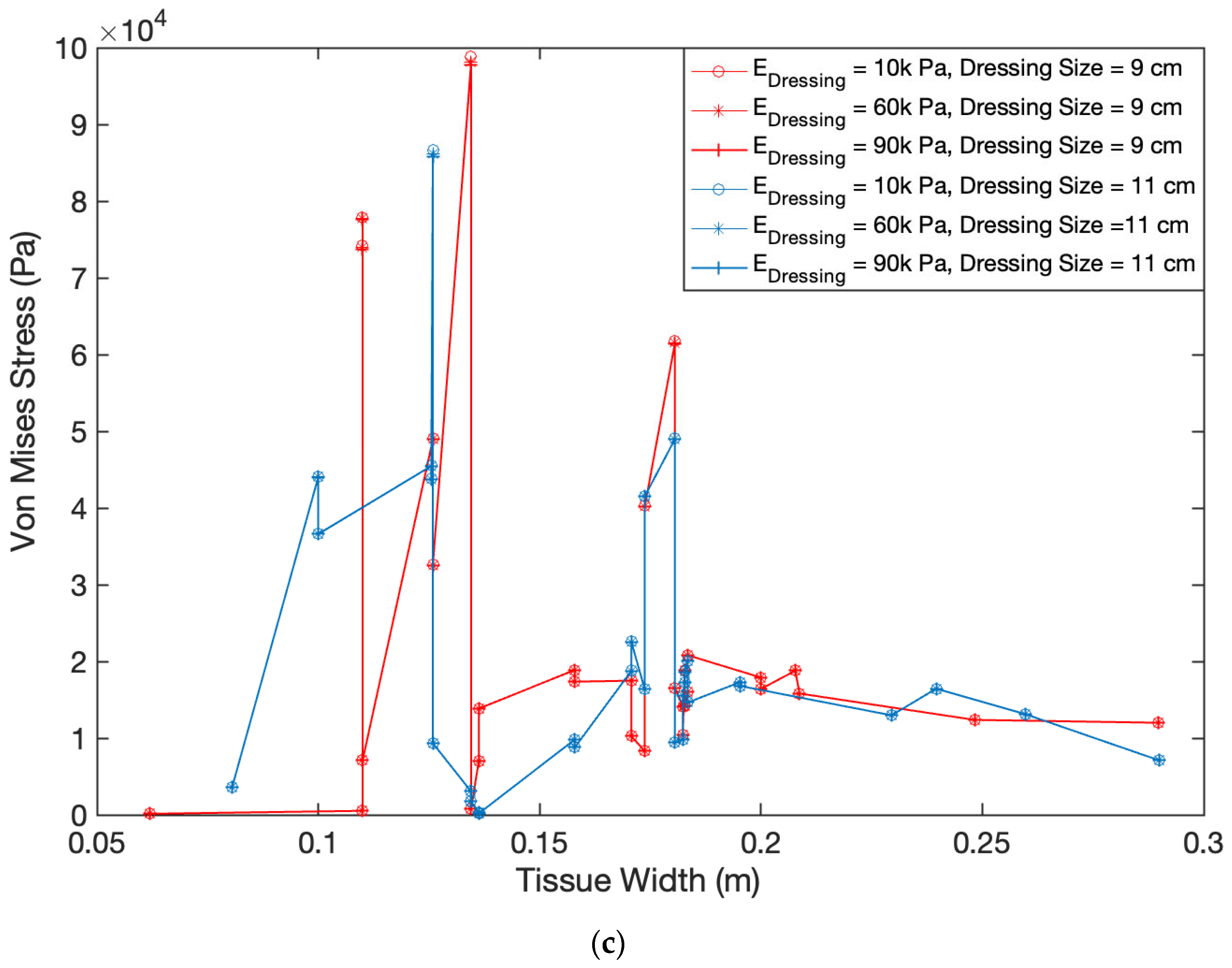
3.1. Impact of Dressing Stiffness and Tissue Stiffness on von Mises Stress within Wound Tissue
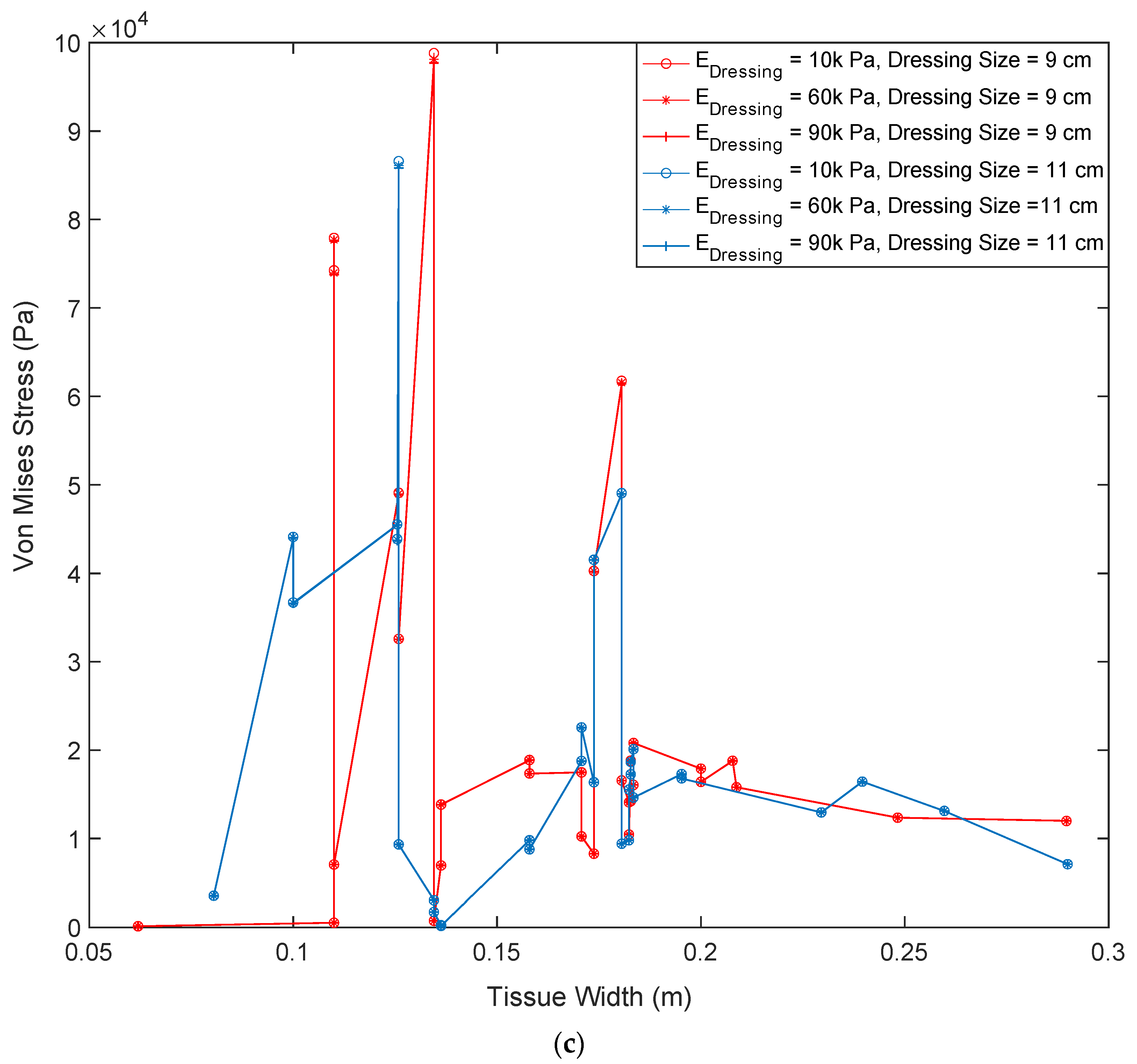
3.2. Impact of Dressing Size on von Mises Stress within Wound Tissue
3.3. Impact of Various Dressing and Tissue Properties on Maximum Force Transmission within Wound Tissue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuehlmann, B.; Bonham, C.A.; Zucal, I.; Prantl, L.; Gurtner, G.C. Mechanotransduction in Wound Healing and Fibrosis. J. Clin. Med. 2020, 9, 1423. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes since 1980, a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet 2016, 387, 1513–1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stockl, K.; Vanderplas, A.; Tafesse, E.; Chang, E. Costs of lower-extremity ulcers among patients with diabetes. Diabetes Care 2004, 27, 2129–2134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, H.N.; Hardman, M.J. Wound healing: Cellular mechanisms and pathological outcomes. Open Biol. 2020, 10, 200223. [Google Scholar] [CrossRef]
- Silver, F.H. A Matter of gravity–mechanotransduction: How mechanical forces influence biological materials. Mater. Sci. Eng. Int. J. 2017, 1, 66–68. [Google Scholar] [CrossRef]
- Tonnesen, M.G.; Feng, X.; Clark, R.A. Angiogenesis in wound healing. J. Investig. Derm. Symp. Proc. 2000, 5, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Yang, L. Computational Modeling and Simulation Study of Dermal Wound Healing Proliferative Phase. In Theses and Dissertations; Virginia Commonwealth University: Richmond, VA, USA, 2011; Available online: https://scholarscompass.vcu.edu/etd/278 (accessed on 28 November 2022).
- Dhivya, S.; Padma, V.V.; Santhini, E. Wound dressings—A review. BioMed 2015, 5, 22. [Google Scholar] [CrossRef]
- Mehrvar, S.; Rymut, K.T.; Foomani, F.H.; Mostaghimi, S.; Eells, J.T.; Ranji, M.; Gopalakrishnan, S. Fluorescence Imaging of Mitochondrial Redox State to Assess Diabetic Wounds. IEEE J. Transl. Eng. Health Med. 2019, 7, 1800809. [Google Scholar] [CrossRef]
- Mehrvar, S.; Mostaghimi, S.; Foomani, F.H.; Abroe, B.; Eells, J.T.; Gopalakrishnan, S.; Ranji, M. 670 nm photobiomodulation improves the mitochondrial redox state of diabetic wounds. Quant Imaging Med. Surg. 2021, 11, 107–118. [Google Scholar] [CrossRef]
- Geris, L.; Schugart, R.; Van Oosterwyck, H. In silico design of treatment strategies in wound healing and bone fracture healing. Philos. Trans. A Math. Phys. Eng. Sci. 2010, 368, 2683–2706. [Google Scholar] [CrossRef]
- Geris, L.; Gerisch, A.; Schugart, R. Mathematical modeling in wound healing, bone regeneration and tissue engineering. ActaBiotheor. 2010, 58, 355–367. [Google Scholar] [CrossRef]
- Mantzaris, N.V.; Webb, S.; Othmer, H.G. Mathematical modeling of tumor-induced angiogenesis. J. Math. Biol. 2004, 49, 111–187. [Google Scholar] [CrossRef] [PubMed]
- Addison-Smith, B.; McElwain, D.L.; Maini, P.K. A simple mechanistic model of sprout spacing in tumour-associated angiogenesis. J. Biol. 2008, 250, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Alarcón, T.; Byrne, H.M.; Maini, P.K. A multiple scale model for tumor growth. Multi. Model Simul. 2005, 3, 440–475. [Google Scholar] [CrossRef] [Green Version]
- Alarcón, T.; Byrne, H.M.; Maini, P.K.; Panovska, J. Mathematical modelling of angiogenesis and vascular adaptation. In Multidisciplinary Approaches to Theory in Medicine; Paton, R., McNamara, L., Eds.; Elsevier: Amsterdam, The Netherlands, 2006; Volume 3, pp. 369–387. [Google Scholar]
- Alarcón, T.; Owen, M.R.; Byrne, H.M.; Maini, P.K. Multiscale modelling of tumour growth and therapy: The influence of vesselnormalisation on chemotherapy. Comput. Math Methods Med. 2006, 7, 85–119. [Google Scholar] [CrossRef] [Green Version]
- Chaplain, M.A.; Byrne, H.M. Mathematical modelling of wound healing and tumour growth: Two sides of the same coin. Wounds A Compend. Clin. Res. Pract. 1996, 8, 42–48. [Google Scholar]
- Chaplain, M.A.; Giles, S.M.; Sleeman, B.D.; Jarvis, R.J. A mathematical analysis of a model for tumour angiogenesis. J. Math Biol. 1995, 33, 744–770. [Google Scholar] [CrossRef]
- Ziraldo, C.; Mi, Q.; An, G.; Vodovotz, Y. Computational Modeling of Inflammation and Wound Healing. Adv. Wound Care 2013, 2, 527–537. [Google Scholar] [CrossRef] [Green Version]
- Sherratt, J.A.; Dallon, J.C. Theoretical models of wound healing: Past successes and future challenges. C. R. Biol. 2002, 325, 557–564. [Google Scholar] [CrossRef]
- Viji Babu, P.K.; Radmacher, M. Mechanics of Brain Tissues Studied by Atomic Force Microscopy: A Perspective. Front. Neurosci. 2019, 13, 600. [Google Scholar] [CrossRef] [Green Version]
- Gouget, C.L.M.; Hwang, Y.; Barakat, A.I. Model of cellular mechanotransduction via actin stress fibers. Biomech. Model. Mechanobiol. 2015, 15, 331–344. [Google Scholar] [CrossRef]
- Barakat, A.I. A model for shear stress-induced deformation of a flow sensor on the surface of vascular endothelial cells. J. Biol. 2001, 210, 221–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.H.; Choi, J.H.; Kim, J.; Chung, Y.K. Fasciotomy in compartment syndrome from snakebite. Arch Plast. Surg. 2019, 46, 69–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, Y.; Gouget, C.L.; Barakat, A.I. Mechanisms of cytoskeleton-mediated mechanical signal transmission in cells. Commun. Integr. Biol. 2012, 5, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Hwang, Y.; Barakat, A.L. Dynamics of mechanical signal transmission through prestressed stress fibers. PLoS ONE 2012, 7, 10. [Google Scholar] [CrossRef]
- Dabagh, M.; Jalali, P.; Butler, P.J.; Tarbell, J.M. Shear-Induced force transmission in a multicomponent, multicell model of endothelium. J. R Soc. Interf. 2014, 11, 20140431. [Google Scholar] [CrossRef] [Green Version]
- Flegg, J.A.; Menon, S.N.; Maini, P.K.; McElwain, D.L. On the mathematical modeling of wound healing angiogenesis in skin as a reaction-transport process. Front. Physiol. 2015, 6, 262. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.; Nordquist, A.; Zhou, J.; Feng, Y. Computational Modeling of Wound Healing Based on Continuum Mixture Theory. In Center for Simulation, Visualization, and Real Time Prediction (SiViRT); The University of Texas at San Antonio: San Antonio, TX, USA, 2014. [Google Scholar]
- Pensalfini, M.; Buganza-Tepole, A. Mechano-biological and bio-mechanical pathways in cutaneous wound healing. Biorxiv 2022, 12, 1–43. [Google Scholar] [CrossRef]
- Vogt, P.M.; Andree, C.; Breuing, K.; Liu, P.Y.; Slama, J.; Helo, G.; Eriksson, E. Dry, moist, and wet skin wound repair. Ann. Plast. Surg. 1995, 34, 493–499. [Google Scholar] [CrossRef]
- Wang, J.H.C.; Thampatty, B.P.; Lin, J.S.; Im, H.J. Mechanoregulation of gene expression in fibroblasts. Gene 2007, 391, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Niezgoda, J.A.; Niezgoda, J.A.; Gopalakrishnan, S. In Vitro Characterization of Pressure Redistribution Among Commercially Available Wound Dressings. Adv. Ski. Wound Care 2021, 34, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Nussbaum, S.R.; Carter, M.J.; Fife, C.E.; DaVanzo, J.; Haught, R.; Nusgart, M.; Cartwright, D. An Economic Evaluation of the Impact, Cost, and Medicare Policy Implications of Chronic Nonhealing Wounds. Value Health 2018, 21, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sen, C.K. Human Wounds and Its Burden: An Updated Compendium of Estimates. Adv. Wound Care 2019, 8, 39–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, A.R.; Chaplain, M.A. Continuous and discrete mathematical models of tumor-induced angiogenesis. Bull. Math Biol. 1998, 60, 857–899. [Google Scholar] [CrossRef] [PubMed]
- Chaplain, M.A. The mathematical modelling of tumour angiogenesis and invasion. Acta Biotheor. 1995, 43, 387–402. [Google Scholar] [CrossRef]
- Chaplain, M.A. Mathematical modelling of angiogenesis. J. Neurooncol. 2000, 50, 37–51. [Google Scholar] [CrossRef]
- Chaplain, M.A.; McDougall, S.R.; Anderson, A.R. Mathematical modeling of tumor-induced angiogenesis. Annu. Rev. Biomed. Eng. 2006, 8, 233–257. [Google Scholar] [CrossRef] [Green Version]
- Mehidizadeh, H.; Brey, E.; Cinar, A. Modeling vascularization in tissue engineering scaffolds. In Vascularization: Regenerative Medicine and Tissue Engineering, 1st ed.; Brey, E.M., Ed.; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Spill, F.; Guerrero, P.; Alarcon, T.; Maini, P.K.; Byrne, H.M. Mesoscopic and continuum modelling of angiogenesis. J. Math Biol. 2015, 70, 485–532. [Google Scholar] [CrossRef] [Green Version]
- Dabagh, M.; Jalali, P.; Butler, P.J.; Randles, A.; Tarbell, J.M. Mechanotransmission in endothelial cells subjected to oscillatory and multi-directional shear flow. J. R. Soc. Interf. 2017, 14, 20170185. [Google Scholar] [CrossRef] [Green Version]
- Dabagh, M.; Randles, A. Role of deformable cancer cells on wall shear stress-associated-VEGF secretion by endothelium in microvasculature. PLoS ONE 2019, 14, e0211418. [Google Scholar] [CrossRef]
- Korenczuk, C.E.; Votava, L.E.; Dhume, R.Y.; Kizilski, S.B.; Brown, G.E.; Narain, R.; Barocas, V.H. Isotropic Failure Criteria Are Not Appropriate for Anisotropic Fibrous Biological Tissues. J. Biomech. Eng. 2017, 139, 0710081. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Dressing Size (cm) | Dressing Stiffness (Pa) | ECM-Stiffness (Pa) |
|---|---|---|---|
| 1 | 7 | 10,000 | 50,000 |
| 2 | 7 | 10,000 | 200,000 |
| 3 | 7 | 10,000 | 1,000,000 |
| 4 | 7 | 10,000 | 100 × 106 |
| 5 | 7 | 60,000 | 50,000 |
| 6 | 7 | 60,000 | 200,000 |
| 7 | 7 | 60,000 | 1,000,000 |
| 8 | 7 | 60,000 | 100 × 106 |
| 9 | 7 | 90,000 | 50,000 |
| 10 | 7 | 90,000 | 200,000 |
| 11 | 7 | 90,000 | 1,000,000 |
| 12 | 7 | 90,000 | 100 × 106 |
| 13 | 9 | 10,000 | 50,000 |
| 14 | 9 | 10,000 | 1,000,000 |
| 15 | 9 | 10,000 | 100 × 106 |
| 16 | 9 | 60,000 | 50,000 |
| 17 | 9 | 60,000 | 1,000,000 |
| 18 | 9 | 60,000 | 100 × 106 |
| 19 | 9 | 90,000 | 50,000 |
| 20 | 9 | 90,000 | 1,000,000 |
| 21 | 9 | 90,000 | 100 × 106 |
| 22 | 11 | 10,000 | 50,000 |
| 23 | 11 | 10,000 | 1,000,000 |
| 24 | 11 | 10,000 | 100 × 106 |
| 25 | 11 | 60,000 | 50,000 |
| 26 | 11 | 60,000 | 1,000,000 |
| 27 | 11 | 60,000 | 100 × 106 |
| 28 | 11 | 90,000 | 50,000 |
| 29 | 11 | 90,000 | 1,000,000 |
| 30 | 11 | 90,000 | 100 × 106 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McElvain, K.; Klister, J.; Ebben, A.; Gopalakrishnan, S.; Dabagh, M. Impact of Wound Dressing on Mechanotransduction within Tissues of Chronic Wounds. Biomedicines 2022, 10, 3080. https://doi.org/10.3390/biomedicines10123080
McElvain K, Klister J, Ebben A, Gopalakrishnan S, Dabagh M. Impact of Wound Dressing on Mechanotransduction within Tissues of Chronic Wounds. Biomedicines. 2022; 10(12):3080. https://doi.org/10.3390/biomedicines10123080
Chicago/Turabian StyleMcElvain, Kelly, Joshua Klister, Alessandra Ebben, Sandeep Gopalakrishnan, and Mahsa Dabagh. 2022. "Impact of Wound Dressing on Mechanotransduction within Tissues of Chronic Wounds" Biomedicines 10, no. 12: 3080. https://doi.org/10.3390/biomedicines10123080
APA StyleMcElvain, K., Klister, J., Ebben, A., Gopalakrishnan, S., & Dabagh, M. (2022). Impact of Wound Dressing on Mechanotransduction within Tissues of Chronic Wounds. Biomedicines, 10(12), 3080. https://doi.org/10.3390/biomedicines10123080