
Safety of FOLFIRI + Durvalumab +/− Tremelimumab in Second Line of Patients with Advanced Gastric Cancer: A Safety Run-In from the Randomized Phase II Study DURIGAST PRODIGE 59

 , , and
, , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Study Objectives
2.3. Study Population
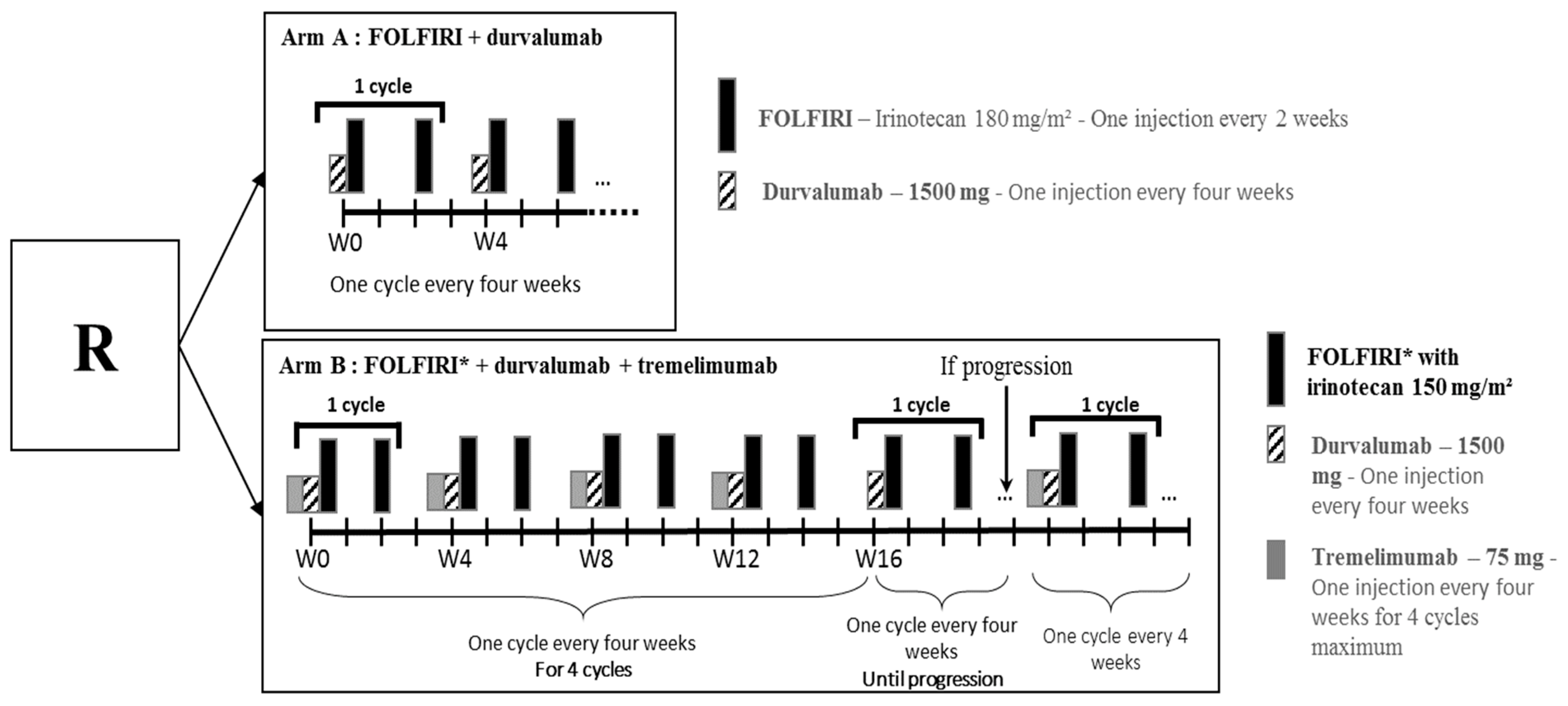
2.4. Treatment Scheme and Modalities
2.5. Safety Run-In Analysis
2.6. Statistical Analysis
3. Results
3.1. Patient and Tumour Characteristics
3.2. Adverse Events in Overall Population and in Each Arm
3.3. Modification of Treatment Related to Toxicity
3.4. Modification of the Protocol According to Safety Run-In Phase
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Cutsem, E.; Moiseyenko, V.; Tjulandin, S.; Majlis, A.; Constenla, M.; Boni, C.; Rodrigues, A.; Fodor, M.; Chao, Y.; Voznyi, E.; et al. Phase III Study of Docetaxel and Cisplatin Plus Fluorouracil Compared with Cisplatin and Fluorouracil as First-Line Therapy for Advanced Gastric Cancer: A Report of the V325 Study Group. J. Clin. Oncol. 2006, 24, 4991–4997. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Boni, C.; Tabernero, J.; Massuti, B.; Middleton, G.; Dane, F.; Reichardt, P.; Pimentel, F.L.; Cohn, A.; Follana, P.; et al. Docetaxel plus oxaliplatin with or without fluorouracil or capecitabine in metastatic or locally recurrent gastric cancer: A randomized phase II study. Ann. Oncol. 2014, 26, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Zaanan, A.; Samalin, E.; Aparicio, T.; Bouche, O.; Laurent-Puig, P.; Manfredi, S.; Michel, P.; Monterymard, C.; Moreau, M.; Rougier, P.; et al. Phase III randomized trial comparing 5-fluorouracil and oxaliplatin with or without docetaxel in first-line advanced gastric cancer chemotherapy (GASTFOX study). Dig. Liver Dis. 2018, 50, 408–410. [Google Scholar] [CrossRef] [PubMed]
- Ford, H.E.R.; Marshall, A.; Bridgewater, J.A.; Janowitz, T.; Coxon, F.Y.; Wadsley, J.; Mansoor, W.; Fyfe, D.; Madhusudan, S.; Middleton, G.W.; et al. Docetaxel versus active symptom control for refractory oesophagogastric adenocarcinoma (COUGAR-02): An open-label, phase 3 randomised controlled trial. Lancet Oncol. 2013, 15, 78–86. [Google Scholar] [CrossRef]
- Thuss-Patience, P.C.; Kretzschmar, A.; Bichev, D.; Deist, T.; Hinke, A.; Breithaupt, K.; Dogan, Y.; Gebauer, B.; Schumacher, G.; Reichardt, P. Survival advantage for irinotecan versus best supportive care as second-line chemotherapy in gastric cancer—A randomised phase III study of the Arbeitsgemeinschaft Internistische Onkologie (AIO). Eur. J. Cancer 2011, 47, 2306–2314. [Google Scholar] [CrossRef] [PubMed]
- Hironaka, S.; Ueda, S.; Yasui, H.; Nishina, T.; Tsuda, M.; Tsumura, T.; Sugimoto, N.; Shimodaira, H.; Tokunaga, S.; Moriwaki, T.; et al. Randomized, Open-Label, Phase III Study Comparing Irinotecan with Paclitaxel in Patients with Advanced Gastric Cancer Without Severe Peritoneal Metastasis After Failure of Prior Combination Chemotherapy Using Fluoropyrimidine Plus Platinum: WJOG 4007 Trial. J. Clin. Oncol. 2013, 31, 4438–4444. [Google Scholar] [CrossRef]
- Maugeri-Saccà, M.; Pizzuti, L.; Sergi, D.; Barba, M.; Belli, F.; Fattoruso, S.I.; Giannarelli, D.; Amodio, A.; Boggia, S.; Vici, P.; et al. FOLFIRI as a second-line therapy in patients with docetaxel-pretreated gastric cancer: A historical cohort. J. Exp. Clin. Cancer Res. 2013, 32, 67. [Google Scholar] [CrossRef]
- Fuchs, C.S.; Tomasek, J.; Yong, C.J.; Dumitru, F.; Passalacqua, R.; Goswami, C.; Safran, H.; dos Santos, L.V.; Aprile, G.; Ferry, D.R.; et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): An international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet Oncol. 2013, 383, 31–39. [Google Scholar] [CrossRef]
- Wilke, H.; Muro, K.; Van Cutsem, E.; Oh, S.-C.; Bodoky, G.; Shimada, Y.; Hironaka, S.; Sugimoto, N.; Lipatov, O.; Kim, T.-Y.; et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): A double-blind, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1224–1235. [Google Scholar] [CrossRef]
- Boku, N.; Ryu, M.H.; Kato, K.; Chung, H.C.; Minashi, K.; Lee, K.W.; Cho, H.; Kang, W.K.; Komatsu, Y.; Tsuda, M.; et al. Safety and efficacy of nivolumab in com-bination with S-1/capecitabine plus oxaliplatin in patients with previously untreated, unresectable, advanced, or recurrent gastric/gastroesophageal junction cancer: Interim results of a randomized, phase II trial (ATTRACTION-4). Ann. Oncol. 2019, 30, 250–258. [Google Scholar]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Bragagnoli, A.C.; et al. First-line nivolumab plus chemo-therapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 398, 27–40. [Google Scholar] [CrossRef]
- Shitara, K.; Van Cutsem, E.; Bang, Y.-J.; Fuchs, C.; Wyrwicz, L.; Lee, K.-W.; Kudaba, I.; Garrido, M.; Chung, H.C.; Lee, J.; et al. Efficacy and Safety of Pembrolizumab or Pembrolizumab Plus Chemotherapy vs Chemotherapy Alone for Patients with First-line, Advanced Gastric Cancer: The KEYNOTE-062 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.-J.; Ruiz, E.Y.; Van Cutsem, E.; Lee, K.W.; Wyrwicz, L.; Schenker, M.; Alsina, M.; Ryu, M.H.; Chung, H.C.; Evesque, L.; et al. Phase III, randomised trial of avelumab versus physician’s choice of chemotherapy as third-line treatment of patients with advanced gastric or gas-tro-oesophageal junction cancer: Primary analysis of JAVELIN Gastric 300. Ann. Oncol. 2018, 29, 2052–2060. [Google Scholar] [CrossRef] [PubMed]
- Janjigian, Y.Y.; Bendell, J.; Calvo, E.; Kim, J.W.; Ascierto, P.A.; Sharma, P.; Ott, P.A.; Peltola, K.; Jaeger, D.; Evans, J.; et al. CheckMate-032 Study: Efficacy and Safety of Nivolumab and Nivolumab Plus Ipilimumab in Patients with Metastatic Esophagogastric Cancer. J. Clin. Oncol. 2018, 36, 2836–2844. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.J.; Lee, J.; Bang, Y.J.; Almhanna, K.; Blum, M.M.; Catenacci, D.V.T.; Chung, H.C.; Wainberg, Z.A.; Gibson, M.K.; Lee, K.W.; et al. Safety and Efficacy of Durvalumab and Tremelimumab Alone or in Combination in Patients with Advanced Gastric and Gastroesophageal Junction Adenocar-cinoma. Clin. Cancer Res. 2020, 26, 846–854. [Google Scholar] [PubMed] [Green Version]
- Evrard, C.; Louvet, C.; Hajbi, F.E.; Fiore, F.D.; Malicot, K.L.; Aparicio, T.; Bouché, O.; Laurent-Puig, P.; Bibeau, F.; Lecomte, T.; et al. PRODIGE 59-DURIGAST trial: A randomised phase II study evaluating FOLFIRI + Durvalumab ± Tremelimumab in second-line of patients with advanced gastric cancer. Dig. Liver Dis. 2021, 53, 420–426. [Google Scholar] [CrossRef]
- Fumet, J.D.; Isambert, N.; Hervieu, A.; Zanetta, S.; Guion, J.-F.; Hennequin, A.; Rederstorff, E.; Bertaut, A.; Ghiringhelli, F. Phase Ib/II trial evaluating the safety, tolerability and immunological activity of durvalumab (MEDI4736) (anti-PD-L1) plus tremelimumab (anti-CTLA-4) combined with FOLFOX in patients with metastatic colorectal cancer. ESMO Open 2018, 3, e000375. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, Y.; Sunakawa, Y.; Inoue, E.; Kawabata, R.; Ishiguro, A.; Kito, Y.; Akamaru, Y.; Takahashi, M.; Yabusaki, H.; Matsuyama, J.; et al. Real-world effectiveness of nivolumab in advanced gastric cancer: The DELIVER trial (JACCRO GC-08). Gastric Cancer 2021, 25, 235–244. [Google Scholar] [CrossRef]
- Li, W.; Jiang, J.; Huang, L.; Long, F. Efficacy of PD-1/L1 inhibitors in brain metastases of non-small-cell lung cancer: Pooled analysis from seven randomized controlled trials. Future Oncol. 2022, 18, 403–412. [Google Scholar] [CrossRef]
- Flippot, R.; Dalban, C.; Laguerre, B.; Borchiellini, D.; Gravis, G.; Négrier, S.; Chevreau, C.; Joly, F.; Geoffrois, L.; Ladoire, S.; et al. Safety and Efficacy of Nivolumab in Brain Metastases from Renal Cell Carcinoma: Results of the GETUG-AFU 26 NIVOREN Multicenter Phase II Study. J. Clin. Oncol. 2019, 37, 2008–2016. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Forsyth, P.A.; Hodi, F.S.; Lao, C.D.; Moschos, S.J.; Hamid, O.; Atkins, M.B.; Lewis, K.; Thomas, R.P.; Glaspy, J.A.; et al. Safety and efficacy of the combination of nivolumab plus ipilimumab in patients with melanoma and asymptomatic or symptomatic brain metastases (CheckMate 204). Neuro-Oncol. 2021, 23, 1961–1973. [Google Scholar] [CrossRef] [PubMed]
- Roth, P.; Winklhofer, S.; Müller, A.M.; Dummer, R.; Mair, M.J.; Gramatzki, D.; Le Rhun, E.; Manz, M.G.; Weller, M.; Preusser, M. Neurological complications of cancer immunotherapy. Cancer Treat. Rev. 2021, 97, 102189. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Park, S.; Kim, H.; Kang, S.Y.; Ahn, S.; Kim, K.-M. Gastric Cancer: Mechanisms, Biomarkers, and Therapeutic Approaches. Biomedicines 2022, 10, 543. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | All Patients (n = 11) | Arm A (Folfiri + Durvalumab) (n = 8) | Arm B (Folfiri + Durvalumab + Tremelimumab) (n = 3) |
|---|---|---|---|
| Age (years, range) | 71 [42–78] | 72 [55–78] | 62 [42–70] |
| Female (n, %) | 4 (36.4%) | 3 (37.5%) | 1 (33.3%) |
| ECOG performance status (n, %) | |||
| 0 | 4 (36.4%) | 2 (25.0%) | 2 (66.7%) |
| 1 | 7 (63.6%) | 6 (75.0%) | 1 (33.3%) |
| Body Mass Index (kg/m2, range) | 26 [21–28] | 27 [21–28] | 23 [23–26] |
| Primary tumour site (n, %) | |||
| Gastro-oesophageal junction | 9 (81.8%) | 7 (87.5%) | 2 (67.7%) |
| Stomach | 2 (18.2%) | 1 (12.5%) | 1 (33.3%) |
| Tumour subtype (Lauren classification) (n, %) | |||
| Intestinal type | |||
| Diffuse type | 7 (70.0%) | 4 (57.1%) | 3 (100%) |
| Unknown | 3 (30.0%) | 3 (42.9%) | 0 |
| 1 | 1 | 0 | |
| Microsatellite instability | |||
| Deficient | 0 | 0 | 0 |
| Proficient | 11 (100%) | 8 (100%) | 3 (100%) |
| Delay of metastatic disease (n, %) | |||
| Metachronous | 2 (18.2%) | 1 (12.5%) | 1 (33.3%) |
| Synchronous | 9 (81.8%) | 7 (87.5%) | 2 (66.7%) |
| Resection of primary tumour (n, %) | |||
| No | 8 (72.7%) | 6 (75.0%) | 2 (66.7%) |
| Yes | 3 (27.3%) | 2 (25.0%) | 1 (33.3%) |
| Site of metastases (n, %) | 3 (37.5%) | 2 (66.7%) | |
| Liver | 5 (45.5%) | 1 (12.5%) | 1 (33.3%) |
| Lung | 2 (18.2%) | 3 (37.5%) | 0 |
| Peritoneal carcinomatosis | 3 (27.3%) | 5 (62.5%) | 1 (33.3%) |
| Lymph nodes | 6 (54.5%) | ||
| Prior first-line chemotherapy regimen (n, %) | 6 (75.0%) | 2 (66.7%) | |
| Doublet regimen * | 2 (25.0%) | 1 (33.3%) | |
| Triplet regimen ** | 8 (72.7%) | ||
| 3 (27.3%) |
| n, % | Arm A (Folfiri + Durvalumab) (n = 8) | Arm B (Folfiri + Durvalumab + Tremelimumab) (n = 3) | ||
|---|---|---|---|---|
| Grade 1–2 | Grade 3–4-5 | Grade 1–2 | Grade 3–4-5 | |
| Patients with at least one adverse event | 8 (100.0%) | 5 (62.5%) | 3 (100.0%) | 2 (66.7%) |
| Skin and subcutaneous tissue disorders | 5 (62.5%) | - | 1 (33.3%) | - |
| Pruritus | 1 (12.5%) | - | - | - |
| Acneiform rash | 2 (25.0%) | - | - | - |
| Dry skin | 1 (12.5%) | - | 1 (33.3%) | - |
| Palmar-plantar erythrodysesthesia | 2 (25.0%) | - | - | - |
| Renal and urinary disorders | - | 1 (12.5%) | - | - |
| Proteinuria | - | 1 (12.5%) | - | - |
| Nervous system disorders | 4 (50.0%) | 2 (25.0%) | 1 (33.3%) | - |
| Peripheral sensory neuropathy | 4 (50.0%) | 2 (25.0%) | 1 (33.3%) | - |
| Endocrine disorders | - | - | 1 (33.3%) | - |
| Hyperthyroidism | - | - | 1 (33.3%) | - |
| Gastrointestinal disorders | 8 (100.0%) | - | 2 (66.7%) | 1 (33.3%) |
| Constipation | 1 (12.5%) | - | 1 (33.3%) | - |
| Diarrhoea | 6 (75.0%) | - | - | - |
| Dysgeusia | 1 (33.3%) | - | ||
| Dyspepsia | 3 (37.5%) | - | - | - |
| Mucositis | 4 (50.0%) | - | - | - |
| Nausea | 7 (87.5%) | - | - | 1 (33.3%) |
| Vomiting | 3 (37.5%) | - | 1 (33.3%) | |
| Blood and lymphatic system disorders | 14 (100.0%) | 4 (50.0%) | 3 (100.0%) | 1 (33.3%) |
| Anaemia | 5 (62.5%) | 1 (12.5%) | 3 (100%) | |
| Neutropenia | 4 (50.0%) | 3 (37.5%) | 1 (33.3%) | 1 (33.3%) |
| Thrombocytopenia | 5 (62.5%) | - | - | - |
| Musculoskeletal conditions | 1 (12.5%) | - | 2 (66.7%) | - |
| Back pain | 1 (12.5%) | - | 2 (66.7%) | - |
| General disorder | 7 (87.5%) | 1 (12.5%) | 1 (33.3%) | 1 (33.3%) |
| Fatigue | 5 (62.5%) | 1 (12.5%) | 1 (33.3%) | 1 (33.3%) |
| Fever | 1 (12.5%) | - | - | - |
| Anorexia | 1 (12.5%) | - | - | - |
| n, % | n = 11 | Definitive Discontinuation of Treatments (n = 8) | |||
|---|---|---|---|---|---|
| Dose Reduction for Toxicities | Treatment Stop due to Toxicities | Treatment Stop due to Progression | Treatment Stop Planned by the Protocol | Treatment Stop for Other Reason(s) * | |
| Irinotecan (n = 11) | 2 (18.2%) | 1 (12.5%) | 6 (75.0%) | 0 | 1 (12.5%) |
| 5FU bolus (n = 11) | 2 (18.2%) | 0 | 7 (87.5%) | 0 | 1 (12.5%) |
| Continuous 5FU (n = 11) | 3 (27.3%) | 0 | 7 (87.5%) | 0 | 1 (12.5%) |
| Durvalumab (n = 11) | 0 | 0 | 7 (87.5%) | 0 | 1 (12.5%) |
| Tremelimumab (n = 3) | 0 | 0 | 2 (66.7%) | 1 (33.3%) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evrard, C.; Aparicio, T.; Soularue, E.; Le Malicot, K.; Desramé, J.; Botsen, D.; El Hajbi, F.; Gonzalez, D.; Lepage, C.; Bouché, O.; et al. Safety of FOLFIRI + Durvalumab +/− Tremelimumab in Second Line of Patients with Advanced Gastric Cancer: A Safety Run-In from the Randomized Phase II Study DURIGAST PRODIGE 59. Biomedicines 2022, 10, 1211. https://doi.org/10.3390/biomedicines10051211
Evrard C, Aparicio T, Soularue E, Le Malicot K, Desramé J, Botsen D, El Hajbi F, Gonzalez D, Lepage C, Bouché O, et al. Safety of FOLFIRI + Durvalumab +/− Tremelimumab in Second Line of Patients with Advanced Gastric Cancer: A Safety Run-In from the Randomized Phase II Study DURIGAST PRODIGE 59. Biomedicines. 2022; 10(5):1211. https://doi.org/10.3390/biomedicines10051211
Chicago/Turabian StyleEvrard, Camille, Thomas Aparicio, Emilie Soularue, Karine Le Malicot, Jérôme Desramé, Damien Botsen, Farid El Hajbi, Daniel Gonzalez, Come Lepage, Olivier Bouché, and et al. 2022. "Safety of FOLFIRI + Durvalumab +/− Tremelimumab in Second Line of Patients with Advanced Gastric Cancer: A Safety Run-In from the Randomized Phase II Study DURIGAST PRODIGE 59" Biomedicines 10, no. 5: 1211. https://doi.org/10.3390/biomedicines10051211
APA StyleEvrard, C., Aparicio, T., Soularue, E., Le Malicot, K., Desramé, J., Botsen, D., El Hajbi, F., Gonzalez, D., Lepage, C., Bouché, O., Tougeron, D., & on behalf of the DURIGAST—PRODIGE 59 Investigators/Collaborators. (2022). Safety of FOLFIRI + Durvalumab +/− Tremelimumab in Second Line of Patients with Advanced Gastric Cancer: A Safety Run-In from the Randomized Phase II Study DURIGAST PRODIGE 59. Biomedicines, 10(5), 1211. https://doi.org/10.3390/biomedicines10051211