
Predictive Value of Serum Uric Acid to HDL Cholesterol Ratio for Incident Ischemic Heart Disease in Non-Diabetic Koreans



Abstract
:1. Introduction
2. Materials and Methods
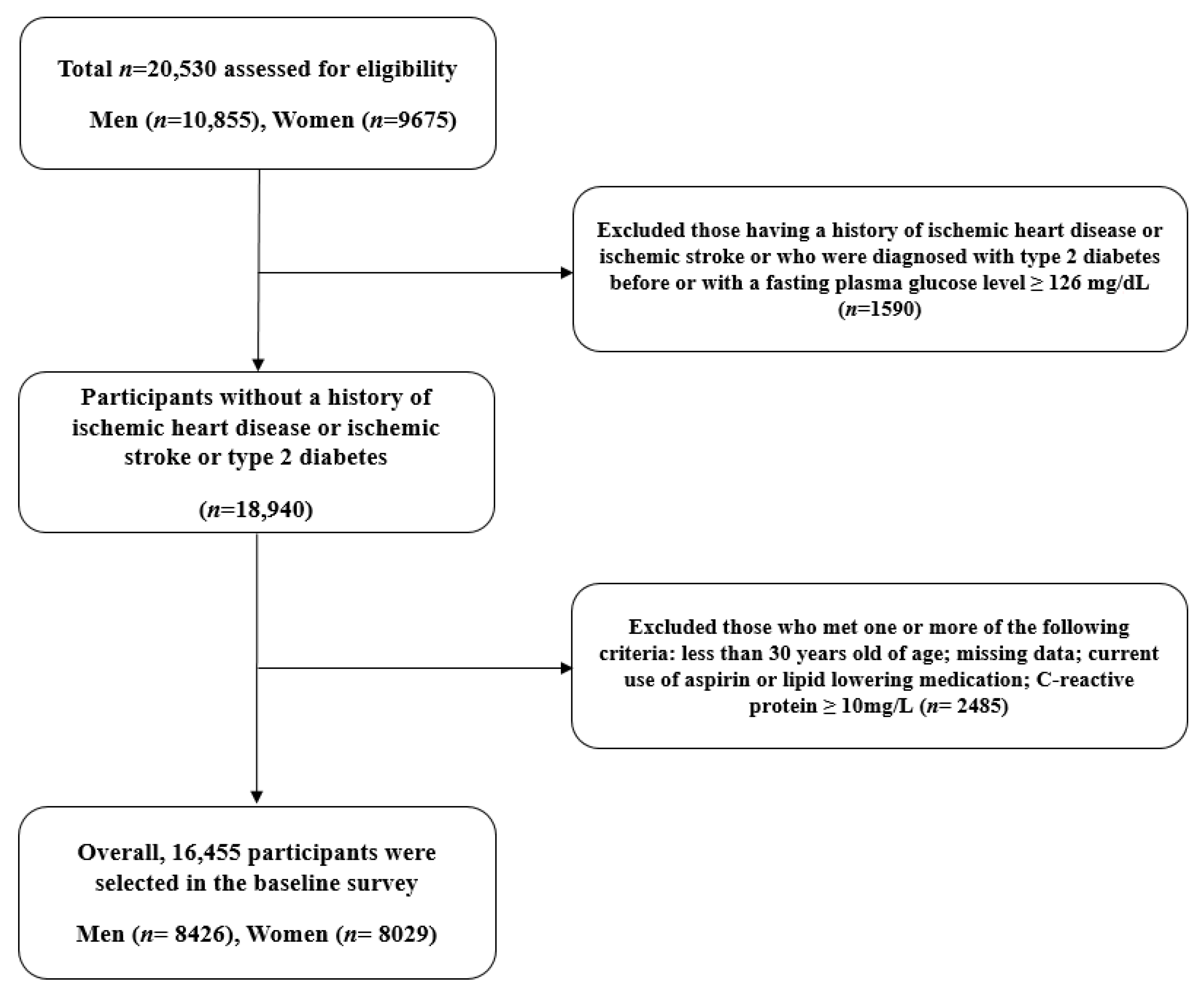
2.1. Participants and Data Collection
2.2. Outcomes and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Julve, J.; Escolà-Gil, J.C. High-density lipoproteins and cardiovascular disease: The good, the bad, and the future. Int. J. Mol. Sci. 2021, 22, 7488. [Google Scholar] [CrossRef] [PubMed]
- Navab, M.; Reddy, S.T.; Van Lenten, B.J.; Fogelman, A.M. Hdl and cardiovascular disease: Atherogenic and atheroprotective mechanisms. Nat. Rev. Cardiol. 2011, 8, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Kou, T.; Luo, H.; Yin, L. Relationship between neutrophils to hdl-c ratio and severity of coronary stenosis. BMC Cardiovasc. Disord 2021, 21, 127. [Google Scholar] [CrossRef]
- Voight, B.F.; Peloso, G.M.; Orho-Melander, M.; Frikke-Schmidt, R.; Barbalic, M.; Jensen, M.K.; Hindy, G.; Hólm, H.; Ding, E.L.; Johnson, T. Plasma hdl cholesterol and risk of myocardial infarction: A mendelian randomisation study. Lancet 2012, 380, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Maiuolo, J.; Oppedisano, F.; Gratteri, S.; Muscoli, C.; Mollace, V. Regulation of uric acid metabolism and excretion. Int. J. Cardiol. 2016, 213, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Ndrepepa, G. Uric acid and cardiovascular disease. Clin. Chim. Acta 2018, 484, 150–163. [Google Scholar] [CrossRef]
- Kivity, S.; Kopel, E.; Maor, E.; Abu-Bachar, F.; Segev, S.; Sidi, Y.; Olchovsky, D. Association of serum uric acid and cardiovascular disease in healthy adults. Am. J. Cardiol. 2013, 111, 1146–1151. [Google Scholar] [CrossRef]
- Muiesan, M.L.; Agabiti-Rosei, C.; Paini, A.; Salvetti, M. Uric acid and cardiovascular disease: An update. Eur. Cardiol. Rev. 2016, 11, 54. [Google Scholar] [CrossRef]
- Yoo, T.W.; Sung, K.C.; Shin, H.S.; Kim, B.J.; Kim, B.S.; Kang, J.H.; Lee, M.H.; Park, J.R.; Kim, H.; Rhee, E.J. Relationship between serum uric acid concentration and insulin resistance and metabolic syndrome. Circ. J. 2005, 69, 928–933. [Google Scholar] [CrossRef] [Green Version]
- Feig, D.I.; Kang, D.-H.; Nakagawa, T.; Mazzali, M.; Johnson, R.J. Uric acid and hypertension. Curr. Hypertens. Rep. 2006, 8, 111–115. [Google Scholar] [CrossRef]
- Bellomo, G. Uric acid and chronic kidney disease: A time to act? World J. Nephrol. 2013, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Tsukui, D.; Kono, H. Uric acid in inflammation and the pathogenesis of atherosclerosis. Int. J. Mol. Sci. 2021, 22, 12394. [Google Scholar] [CrossRef] [PubMed]
- Feig, D.I.; Kang, D.H.; Johnson, R.J. Uric acid and cardiovascular risk. N. Engl. J. Med. 2008, 359, 1811–1821. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Wei, Q.; Long, J.; Gong, L.; Chen, H.; Luo, R.; Ren, W.; Wang, Y. Gender-specific association of serum uric acid levels and cardio-ankle vascular index in chinese adults. Lipids Health Dis. 2018, 17, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aktas, G.; Kocak, M.Z.; Bilgin, S.; Atak, B.M.; Duman, T.T.; Kurtkulagi, O. Uric acid to hdl cholesterol ratio is a strong predictor of diabetic control in men with type 2 diabetes mellitus. Aging Male 2020, 23, 1098–1102. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-N.; Wang, Q.-Q.; Chen, Y.-S.; Shen, C.; Xu, C.-F. Association between serum uric acid to hdl-cholesterol ratio and nonalcoholic fatty liver disease in lean chinese adults. Int. J. Endocrinol. 2020, 2020, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Cholesterol Education Program (NCEP). Expert Panel on Detection; Treatment of High Blood Cholesterol in Adults. Third Report of the National Cholesterol Education Program (Ncep) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Baweja, P.S.; Sandesara, P.B.; Ashraf, M.J. Asymptomatic coronary artery disease in type ii diabetes. Mo. Med. 2014, 111, 73. [Google Scholar]
- Jung, D.H.; Park, B.; Lee, Y.J. Longitudinal effects of serum calcium and phosphate levels and their ratio on incident ischemic heart disease among korean adults. Biomolecules 2022, 12, 103. [Google Scholar] [CrossRef]
- Yoon, J.; Jung, D.; Lee, Y.; Park, B. The metabolic score for insulin resistance (mets-ir) as a predictor of incident ischemic heart disease: A longitudinal study among korean without diabetes. J. Pers. Med. 2021, 11, 742. [Google Scholar] [CrossRef]
- Kocak, M.Z.; Aktas, G.; Erkus, E.; Sincer, I.; Atak, B.; Duman, T. Serum uric acid to hdl-cholesterol ratio is a strong predictor of metabolic syndrome in type 2 diabetes mellitus. Rev. Assoc. Med. Bras. (1992) 2019, 65, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Yazdi, F.; Baghaei, M.H.; Baniasad, A.; Naghibzadeh-Tahami, A.; Najafipour, H.; Gozashti, M.H. Investigating the relationship between serum uric acid to high-density lipoprotein ratio and metabolic syndrome. Endocrinol. Diabetes Metab. 2022, 5, e00311. [Google Scholar] [CrossRef] [PubMed]
- Kosekli, M.A.; Kurtkulagii, O.; Kahveci, G.; Duman, T.T.; Tel, B.M.A.; Bilgin, S.; Demirkol, M.E.; Aktas, G. The association between serum uric acid to high density lipoprotein-cholesterol ratio and non-alcoholic fatty liver disease: The abund study. Rev. Assoc. Med. Bras. (1992) 2021, 67, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Kurtkulagi, O.; Tel, B.M.A.; Kahveci, G.; Bilgin, S.; Duman, T.T.; Ertürk, A.; Balci, B.; Aktas, G. Hashimoto’s thyroiditis is associated with elevated serum uric acid to high density lipoprotein-cholesterol ratio. Rom. J. Intern. Med. 2021, 59, 403–408. [Google Scholar] [CrossRef]
- Lee, S.J.; Oh, B.K.; Sung, K.C. Uric acid and cardiometabolic diseases. Clin. Hypertens. 2020, 26, 13. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, W.; McRae, S.; Marek, G.; Wymer, D.; Pannu, V.; Baylis, C.; Johnson, R.J.; Sautin, Y.Y. Hyperuricemia as a mediator of the proinflammatory endocrine imbalance in the adipose tissue in a murine model of the metabolic syndrome. Diabetes 2011, 60, 1258–1269. [Google Scholar] [CrossRef] [Green Version]
- Adachi, S.I.; Yoshizawa, F.; Yagasaki, K. Hyperuricemia in type 2 diabetic model kk-a(y)/ta mice: A potent animal model with positive correlation between insulin resistance and plasma high uric acid levels. BMC Res. Notes 2017, 10, 577. [Google Scholar] [CrossRef] [Green Version]
- Waheed, Y.; Yang, F.; Sun, D. Role of asymptomatic hyperuricemia in the progression of chronic kidney disease and cardiovascular disease. Korean J. Intern. Med. 2021, 36, 1281–1293. [Google Scholar] [CrossRef]
- Takir, M.; Kostek, O.; Ozkok, A.; Elcioglu, O.C.; Bakan, A.; Erek, A.; Mutlu, H.H.; Telci, O.; Semerci, A.; Odabas, A.R.; et al. Lowering uric acid with allopurinol improves insulin resistance and systemic inflammation in asymptomatic hyperuricemia. J. Investig. Med. 2015, 63, 924–929. [Google Scholar] [CrossRef]
- Perez-Pozo, S.E.; Schold, J.; Nakagawa, T.; Sánchez-Lozada, L.G.; Johnson, R.J.; Lillo, J.L. Excessive fructose intake induces the features of metabolic syndrome in healthy adult men: Role of uric acid in the hypertensive response. Int. J. Obes. 2010, 34, 454–461. [Google Scholar] [CrossRef] [Green Version]
- Barter, P. The role of hdl-cholesterol in preventing atherosclerotic disease. Eur. Heart J. Suppl. 2005, 7, F4–F8. [Google Scholar] [CrossRef] [Green Version]
- Barter, P.J.; Nicholls, S.; Rye, K.-A.; Anantharamaiah, G.; Navab, M.; Fogelman, A.M. Antiinflammatory properties of hdl. Circ. Res. 2004, 95, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Rong, J.X.; Li, J.; Reis, E.D.; Choudhury, R.P.; Dansky, H.M.; Elmalem, V.I.; Fallon, J.T.; Breslow, J.L.; Fisher, E.A. Elevating high-density lipoprotein cholesterol in apolipoprotein e-deficient mice remodels advanced atherosclerotic lesions by decreasing macrophage and increasing smooth muscle cell content. Circulation 2001, 104, 2447–2452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garner, B.; Witting, P.K.; Waldeck, A.R.; Christison, J.K.; Raftery, M.; Stocker, R. Oxidation of high density lipoproteins. I. Formation of methionine sulfoxide in apolipoproteins ai and aii is an early event that accompanies lipid peroxidation and can be enhanced by alpha-tocopherol. J. Biol. Chem. 1998, 273, 6080–6087. [Google Scholar] [CrossRef] [Green Version]
- Einhorn, D.; Reaven, G.M.; Cobin, R.H.; Ford, E.; Ganda, O.P.; Handelsman, Y.; Hellman, R.; Jellinger, P.S.; Kendall, D.; Krauss, R.M.; et al. American college of endocrinology position statement on the insulin resistance syndrome. Endocr. Pract. 2003, 9, 237–252. [Google Scholar] [CrossRef]
- Persky, V.W.; Dyer, A.R.; Idris-Soven, E.; Stamler, J.; Shekelle, R.; Schoenberger, J.; Berkson, D.; Lindberg, H. Uric acid: A risk factor for coronary heart disease? Circulation 1979, 59, 969–977. [Google Scholar] [CrossRef] [Green Version]
- Freedman, D.S.; Williamson, D.F.; Gunter, E.W.; Byers, T. Relation of serum uric acid to mortality and ischemic heart disease. The nhanes i epidemiologic follow-up study. Am. J. Epidemiol. 1995, 141, 637–644. [Google Scholar] [CrossRef]
- Rathmann, W.; Hauner, H.; Dannehl, K.; Gries, F.A. Association of elevated serum uric acid with coronary heart disease in diabetes mellitus. Diabete Metab. 1993, 19, 159–166. [Google Scholar]
- Chou, P.; Lin, K.C.; Lin, H.Y.; Tsai, S.T. Gender differences in the relationships of serum uric acid with fasting serum insulin and plasma glucose in patients without diabetes. J. Rheumatol. 2001, 28, 571–576. [Google Scholar]



{kind=link}
{kind=link}
| Q1 (n = 4113) | Q2 (n = 4114) | Q3 (n = 4114) | Q4 (n = 4114) | p Value 1 | Post Hoc 2 | |
|---|---|---|---|---|---|---|
| UHR (%) | ≤6.8 | ~9.3 | ~12.6 | ≥12.6 | ||
| Age (years) | 45.2 ± 9.1 | 46.6 ± 9.7 | 46.8 ± 9.6 | 45.7 ± 9.5 | <0.001 | a,b,e,f |
| Male sex (%) | 9.7 | 32.8 | 70.2 | 92.2 | <0.001 | - |
| Body mass index (kg/m2) | 21.6 ± 2.6 | 22.7 ± 2.7 | 23.9 ± 2.7 | 25.2 ± 2.7 | <0.001 | a,b,c,d,e,f |
| Systolic blood pressure (mmHg) | 116.3 ± 15.0 | 120.0 ± 15.5 | 124.3 ± 14.7 | 127.2 ± 14.5 | <0.001 | a,b,c,d,e,f |
| Diastolic blood pressure (mmHg) | 72.2 ± 9.6 | 74.9 ± 10.0 | 77.9 ± 9.6 | 79.9 ± 9.4 | <0.001 | a,b,c,d,e,f |
| Fasting plasma glucose (mg/dL) | 88.3 ± 8.7 | 90.2 ± 9.2 | 92.9 ± 10.0 | 94.3 ± 10.0 | <0.001 | a,b,c,d,e,f |
| Uric acid (mg/dL) | 3.6 ± 0.7 | 4.4 ± 0.7 | 5.4 ± 0.8 | 6.5 ± 1.0 | <0.001 | a,b,c,d,e,f |
| Total cholesterol (mg/dL) | 187.9 ± 31.7 | 188.3 ± 33.4 | 192.2 ± 33.8 | 192.6 ± 34.0 | <0.001 | b,c,d,e |
| Triglyceride (mg/dL) | 81.6 ± 35.7 | 102.2 ± 50.1 | 131.4 ± 72.0 | 181.6 ± 119.4 | <0.001 | a,b,c,d,e,f |
| HDL cholesterol (mg/dL) | 66.3 ± 11.3 | 55.7 ± 8.9 | 49.5 ± 7.6 | 41.4 ± 6.4 | <0.001 | a,b,c,d,e,f |
| Log C-reactive protein (mg/L) | −1.0 ± 1.0 | −0.7 ± 1.0 | −0.4 ± 1.0 | 0.0 ± 0.9 | <0.001 | a,b,c,d,e,f |
| Current smoker (%) | 8.0 | 16.2 | 31.2 | 42.6 | <0.001 | - |
| Alcohol drinking 3 (%) | 30.3 | 36.2 | 50.0 | 56.4 | <0.001 | - |
| Regular exercise 4 (%) | 31.3 | 32.0 | 32.1 | 28.3 | <0.001 | - |
| Impaired fasting glucose (%) | 9.2 | 14.3 | 22.0 | 26.5 | <0.001 | - |
| Metabolic syndrome (%) | 2.3 | 7.7 | 13.4 | 25.1 | <0.001 | - |
| Hypertension (%) | 11.1 | 17.4 | 22.9 | 29.9 | <0.001 | - |
| Q1 | Q2 | Q3 | Q4 | p for Trend | ||
|---|---|---|---|---|---|---|
| New cases of ischemic heart disease, n | 56 | 52 | 98 | 115 | ||
| Mean follow-up, years | 2.4 ± 1.1 | 2.4 ± 1.1 | 2.4 ± 1.1 | 2.4 ± 1.1 | ||
| Pearson–years of follow-up | 9778 | 9713 | 9716 | 9825 | ||
| Incidence rate/1000 person–years | 5.7 | 5.4 | 10.1 | 11.7 | ||
| Model 1 | HR (95% CI) | 1.00 (reference) | 0.88 (0.58–1.34) | 1.55 (1.04–2.31) | 1.78 (1.17–2.70) | 0.001 |
| p value | - | 0.548 | 0.031 | 0.006 | ||
| Model 2 | HR (95% CI) | 1.00 (reference) | 0.84 (0.55–1.29) | 1.43 (0.95–2.15) | 1.57 (1.01–2.44) | 0.009 |
| p value | - | 0.425 | 0.089 | 0.044 | ||
| Model 3 | HR (95% CI) | 1.00 (reference) | 0.85 (0.55–1.29) | 1.42 (0.94–2.13) | 1.57 (1.01–2.45) | 0.011 |
| p value | - | 0.436 | 0.097 | 0.045 | ||
| Men | Q1 (≤9.8) | Q2 (~12.2) | Q3 (~14.9) | Q4 (≥14.9) | p for Trend | |
|---|---|---|---|---|---|---|
| Model 1 | HR (95% CI) | 1.00 (reference) | 1.44 (0.94–2.22) | 1.73 (1.14–2.63) | 1.71 (1.12–2.61) | 0.045 |
| p value | - | 0.096 | 0.009 | 0.013 | ||
| Model 2 | HR (95% CI) | 1.00 (reference) | 1.38 (0.90–2.14) | 1.61 (1.05–2.45) | 1.54 (0.98–2.40) | 0.156 |
| p value | - | 0.143 | 0.029 | 0.059 | ||
| Model 2 | HR (95% CI) | 1.00 (reference) | 1.38 (0.89–2.14) | 1.61 (1.05–2.47) | 1.55 (0.99–2.43) | 0.155 |
| p value | - | 0.145 | 0.029 | 0.056 | ||
| Women | Q1 (≤5.7) | Q2 (~7.0) | Q3 (~8.7) | Q4 (≥8.7) | p for Trend | |
| Model 1 | HR (95% CI) | 1.00 (reference) | 1.53 (0.78–3.01) | 1.38 (0.70–2.72) | 2.07 (1.12–3.85) | 0.113 |
| p value | - | 0.216 | 0.350 | 0.021 | ||
| Model 2 | HR (95% CI) | 1.00 (reference) | 1.53 (0.78–3.00) | 1.38 (0.70–2.73) | 2.02 (1.06–3.84) | 0.167 |
| p value | - | 0.221 | 0.355 | 0.032 | ||
| Model 3 | HR (95% CI) | 1.00 (reference) | 1.52 (0.77–2.99) | 1.39 (0.70–2.76) | 2.01 (1.06–3.84) | 0.180 |
| p value | - | 0.225 | 0.342 | 0.033 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, B.; Jung, D.-H.; Lee, Y.-J. Predictive Value of Serum Uric Acid to HDL Cholesterol Ratio for Incident Ischemic Heart Disease in Non-Diabetic Koreans. Biomedicines 2022, 10, 1422. https://doi.org/10.3390/biomedicines10061422
Park B, Jung D-H, Lee Y-J. Predictive Value of Serum Uric Acid to HDL Cholesterol Ratio for Incident Ischemic Heart Disease in Non-Diabetic Koreans. Biomedicines. 2022; 10(6):1422. https://doi.org/10.3390/biomedicines10061422
Chicago/Turabian StylePark, Byoungjin, Dong-Hyuk Jung, and Yong-Jae Lee. 2022. "Predictive Value of Serum Uric Acid to HDL Cholesterol Ratio for Incident Ischemic Heart Disease in Non-Diabetic Koreans" Biomedicines 10, no. 6: 1422. https://doi.org/10.3390/biomedicines10061422
APA StylePark, B., Jung, D. -H., & Lee, Y. -J. (2022). Predictive Value of Serum Uric Acid to HDL Cholesterol Ratio for Incident Ischemic Heart Disease in Non-Diabetic Koreans. Biomedicines, 10(6), 1422. https://doi.org/10.3390/biomedicines10061422