
Embolization for Type Ia Endoleak after EVAR for Abdominal Aortic Aneurysms: A Systematic Review of the Literature

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Eligibility Criteria, Study Quality Assessment
2.3. Data Extraction and Statistical Analysis
2.4. Endpoint Definition
3. Results
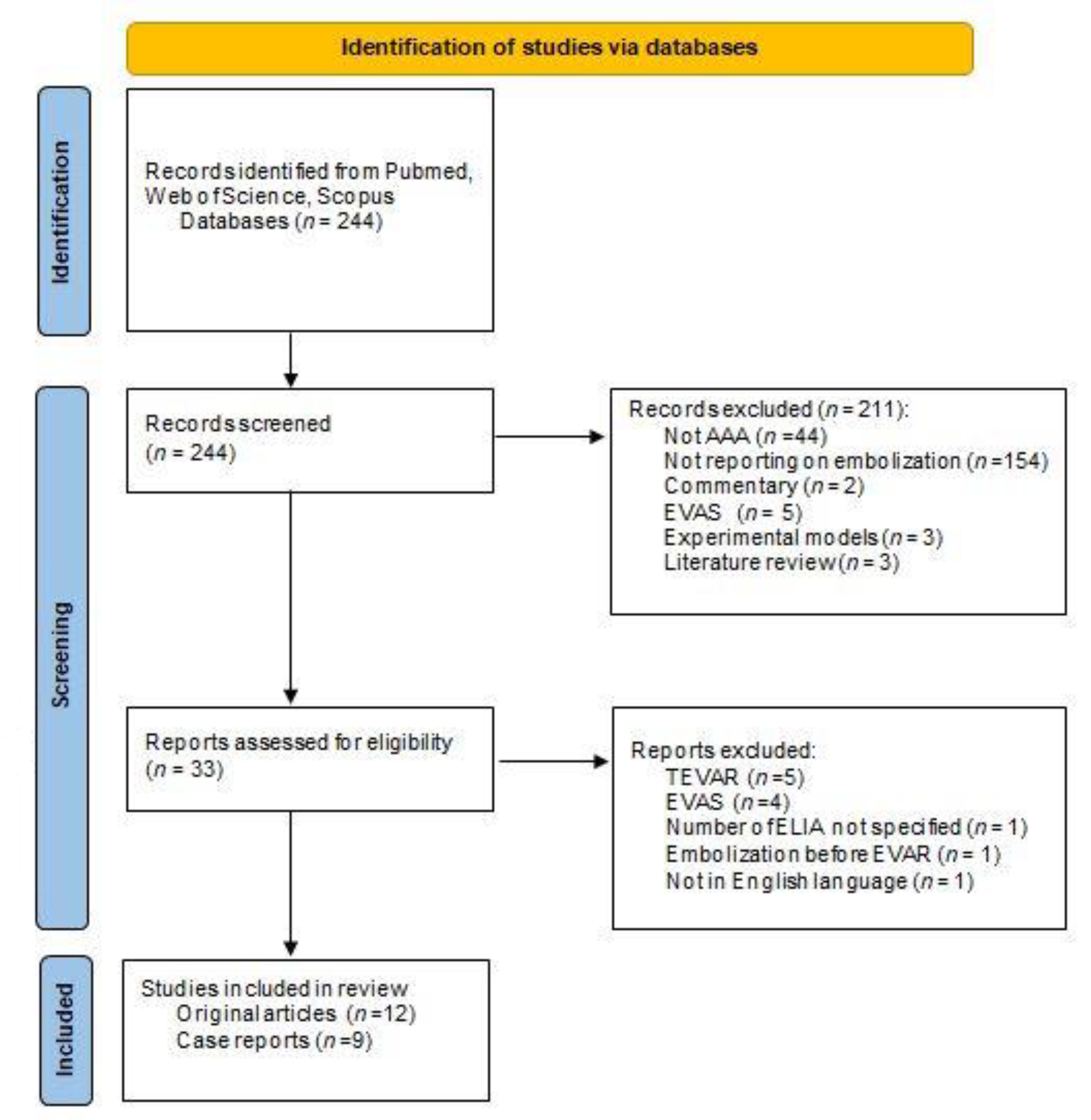
3.1. Search Results
3.2. Patients and Index-Procedure Characteristics
3.3. Embolization of ELIA
3.4. Endpoints, Outcomes and Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Debus, E.S. S3-Leitlinie zum Screening, Diagnostik Therapie und Nachsorge des Bauchaortenaneurysmas. Gefässchirurgie 2018, 23, 402–403. [Google Scholar] [CrossRef] [Green Version]
- Chaikof, E.L.; Dalman, R.L.; Eskandari, M.K.; Jackson, B.M.; Lee, W.A.; Mansour, M.A.; Mastracci, T.M.; Mell, M.; Murad, M.H.; Nguyen, L.L.; et al. The Society for Vascular Surgery Practice Guidelines on the Care of Patients with an Abdominal Aortic Aneurysm. J. Vasc. Surg. 2018, 67, 2–77.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wanhainen, A.; Verzini, F.; Herzeele, I.V.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-Iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarze, M.L.; Shen, Y.; Hemmerich, J.; Dale, W. Age-Related Trends in Utilization and Outcome of Open and Endovascular Repair for Abdominal Aortic Aneurysm in the United States, 2001-2006. J. Vasc. Surg. 2009, 50, 722–729.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giles, K.A.; Pomposelli, F.; Hamdan, A.; Wyers, M.; Jhaveri, A.; Schermerhorn, M.L. Decrease in Total Aneurysm-Related Deaths in the Era of Endovascular Aneurysm Repair. J. Vasc. Surg. 2009, 49, 543–550, discussion 550–551. [Google Scholar] [CrossRef] [Green Version]
- Nakai, M.; Sato, M.; Sato, H.; Sakaguchi, H.; Tanaka, F.; Ikoma, A.; Sanda, H.; Nakata, K.; Minamiguchi, H.; Kawai, N.; et al. Midterm Results of Endovascular Abdominal Aortic Aneurysm Repair: Comparison of Instruction-for-Use (IFU) Cases and Non-IFU Cases. Jpn. J. Radiol. 2013, 31, 585–592. [Google Scholar] [CrossRef]
- De Donato, G.; Pasqui, E.; Panzano, C.; Brancaccio, B.; Grottola, G.; Galzerano, G.; Benevento, D.; Palasciano, G. The Polymer-Based Technology in the Endovascular Treatment of Abdominal Aortic Aneurysms. Polymers 2021, 13, 1196. [Google Scholar] [CrossRef]
- Scali, S.T.; McNally, M.M.; Feezor, R.J.; Chang, C.K.; Waterman, A.L.; Berceli, S.A.; Huber, T.S.; Beck, A.W. Elective Endovascular Aortic Repair Conversion for Type Ia Endoleak Is Not Associated with Increased Morbidity or Mortality Compared with Primary Juxtarenal Aneurysm Repair. J. Vasc. Surg. 2014, 60, 286–294.e1. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological Quality of Case Series Studies: An Introduction to the JBI Critical Appraisal Tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef]
- Golzarian, J.; Struyven, J.; Abada, H.T.; Wery, D.; Dussaussois, L.; Madani, A.; Ferreira, J.; Dereume, J.P. Endovascular Aortic Stent-Grafts: Transcatheter Embolization of Persistent Perigraft Leaks. Radiology 1997, 202, 731–734. [Google Scholar] [CrossRef] [PubMed]
- Faries, P.L.; Cadot, H.; Agarwal, G.; Kent, K.C.; Hollier, L.H.; Marin, M.L. Management of Endoleak after Endovascular Aneurysm Repair: Cuffs, Coils, and Conversion. J. Vasc. Surg. 2003, 37, 1155–1161. [Google Scholar] [CrossRef] [Green Version]
- Maldonado, T.S.; Rosen, R.J.; Rockman, C.B.; Adelman, M.A.; Bajakian, D.; Jacobowitz, G.R.; Riles, T.S.; Lamparello, P.J. Initial Successful Management of Type I Endoleak after Endovascular Aortic Aneurysm Repair with N-Butyl Cyanoacrylate Adhesive. J. Vasc. Surg. 2003, 38, 664–670. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.Y.; Lee, D.Y.; Lee, K.-H.; Ko, Y.-G.; Choi, D.; Shim, W.-H.; Won, J.Y. Treatment of Type I Endoleaks after Endovascular Aneurysm Repair of Infrarenal Abdominal Aortic Aneurysm: Usefulness of N-Butyl Cyanoacrylate Embolization in Cases of Failed Secondary Endovascular Intervention. J. Vasc. Interv. Radiol. 2011, 22, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Henrikson, O.; Roos, H.; Falkenberg, M. Ethylene Vinyl Alcohol Copolymer (Onyx) to Seal Type 1 Endoleak. A New Technique. Vascular 2011, 19, 77–81. [Google Scholar] [CrossRef]
- Chun, J.-Y.; Morgan, R. Transcatheter Embolisation of Type 1 Endoleaks after Endovascular Aortic Aneurysm Repair with Onyx: When No Other Treatment Option Is Feasible. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 141–144. [Google Scholar] [CrossRef] [Green Version]
- Eberhardt, K.M.; Sadeghi-Azandaryani, M.; Worlicek, S.; Koeppel, T.; Reiser, M.F.; Treitl, M. Treatment of Type I Endoleaks Using Transcatheter Embolization with Onyx. J. Endovasc. Ther. 2014, 21, 162–171. [Google Scholar] [CrossRef]
- Ameli-Renani, S.; Pavlidis, V.; Morgan, R.A. Early and Midterm Outcomes after Transcatheter Embolization of Type I Endoleaks in 25 Patients. J. Vasc. Surg. 2017, 65, 346–355. [Google Scholar] [CrossRef] [Green Version]
- Graif, A.; Vance, A.Z.; Garcia, M.J.; Lie, K.T.; McGarry, M.K.; Leung, D.A. Transcatheter Embolization of Type I Endoleaks Associated with Endovascular Abdominal Aortic Aneurysm Repair Using Ethylene Vinyl Alcohol Copolymer. Vasc. Endovasc. Surg. 2017, 51, 28–32. [Google Scholar] [CrossRef]
- Marcelin, C.; Le Bras, Y.; Petitpierre, F.; Midy, D.; Grenier, N.; Ducasse, E.; Cornélis, F. Embolization for Persistent Type IA Endoleaks after Chimney Endovascular Aneurysm Repair with Onyx®. Diagn. Interv. Imaging 2017, 98, 849–855. [Google Scholar] [CrossRef]
- Ierardi, A.M.; Franchin, M.; Fontana, F.; Piffaretti, G.; Crippa, M.; Angileri, S.A.; Magenta Biasina, A.; Piacentino, F.; Tozzi, M.; Pinto, A.; et al. The Role of Ethylene-Vinyl Alcohol Copolymer in Association with Other Embolic Agents for the Percutaneous and Endovascular Treatment of Type Ia Endoleak. Radiol. Med. 2018, 123, 638–642. [Google Scholar] [CrossRef] [PubMed]
- Marchiori, E.; Herten, M.; Bosiers, M.; Schwindt, A.; Bisdas, T.; Austermann, M.; Torsello, G.; Stavroulakis, K. Effectiveness of Intra-Arterial Aneurysm Sac Embolization for Type Ia Endoleak after Endovascular Aneurysm Repair. J. Vasc. Interv. Radiol. 2019, 30, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Kirby, L.; Goodwin, J. Treatment of a Primary Type IA Endoleak with a Liquid Embolic System under Conditions of Aortic Occlusion. J. Vasc. Surg. 2003, 37, 456–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peynircioğlu, B.; Türkbey, B.; Ozkan, M.; Cil, B.E. Use of Glue and Microcoils for Transarterial Catheter Embolization of a Type 1 Endoleak. Diagn. Interv. Radiol. 2008, 14, 111–115. [Google Scholar] [PubMed]
- Grisafi, J.L.; Boiteau, G.; Detschelt, E.; Potts, J.; Kiproff, P.; Muluk, S.C. Endoluminal Treatment of Type IA Endoleak with Onyx. J. Vasc. Surg. 2010, 52, 1346–1349. [Google Scholar] [CrossRef] [Green Version]
- Loffroy, R.; Lin, M.; Ricolfi, F.; Steinmetz, E. Images in Vascular Medicine. Transarterial Microcoil Embolization of a Type Ia Endoleak after EVAR Using a Balloon Remodeling Technique. Vasc. Med. 2010, 15, 513–514. [Google Scholar] [CrossRef]
- Arici, V.; Quaretti, P.; Bozzani, A.; Moramarco, L.P.; Rossi, M.; Carlino, M. Neck-Targeted, Stand-Alone Coiling for Successful Treatment of Type 1A Endoleak Following Endovascular Repair. Vasc. Endovasc. Surg. 2014, 48, 61–64. [Google Scholar] [CrossRef]
- Gandini, R.; Del Giudice, C.; Abrignani, S.; Vasili, E.; Pampana, E.; Simonetti, G. Inexplicable Late Type Ia Endoleak Associated with the Low-Profile Ovation Endograft in a Patient with Favorable Neck Anatomy: Treatment with Transcaval Coil Embolization. J. Endovasc. Ther. 2015, 22, 426–430. [Google Scholar] [CrossRef]
- Igari, K.; Kudo, T.; Toyofuku, T.; Inoue, Y. A Case of Successful Coil Embolization for a Late-Onset Type Ia Endoleak after Endovascular Aneurysm Repair with the Chimney Technique. Case Rep. Vasc. Med. 2016, 2016, 5307416. [Google Scholar] [CrossRef] [Green Version]
- Massimi, T.M.; Kostun, Z.W.; Woo, E.Y. Transcaval Embolization of a Type I Gutter Endoleak after Three-Vessel Chimney Endovascular Aneurysm Repair. J. Vasc. Surg. 2017, 65, 1515–1517. [Google Scholar] [CrossRef] [Green Version]
- Belczak, S.Q.; Pedroso, G.D.; Ogawa, L.C.; Campos, P.T.; Padula, A.L.; Machado, G.P.; Dos Santos, M.Z.S.; Abrão, B.M. Treatment of Type 1A Endoleak Using Coil Embolization: A Case Report. J. Vasc. Bras. 2019, 18, e20180130. [Google Scholar] [CrossRef]
- Aburahma, A.F.; Campbell, J.E.; Mousa, A.Y.; Hass, S.M.; Stone, P.A.; Jain, A.; Nanjundappa, A.; Dean, L.S.; Keiffer, T.; Habib, J. Clinical Outcomes for Hostile versus Favorable Aortic Neck Anatomy in Endovascular Aortic Aneurysm Repair Using Modular Devices. J. Vasc. Surg. 2011, 54, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Abbruzzese, T.A.; Kwolek, C.J.; Brewster, D.C.; Chung, T.K.; Kang, J.; Conrad, M.F.; LaMuraglia, G.M.; Cambria, R.P. Outcomes Following Endovascular Abdominal Aortic Aneurysm Repair (EVAR): An Anatomic and Device-Specific Analysis. J. Vasc. Surg. 2008, 48, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Saratzis, A.N.; Goodyear, S.; Sur, H.; Saedon, M.; Imray, C.; Mahmood, A. Acute Kidney Injury after Endovascular Repair of Abdominal Aortic Aneurysm. J. Endovasc. Ther. 2013, 20, 315–330. [Google Scholar] [CrossRef]
- Valentin, J. Avoidance of Radiation Injuries from Medical Interventional Procedures. Ann. ICRP 2000, 30, 7–67. [Google Scholar] [CrossRef]
- Lu, Q.; Feng, J.; Yang, Y.; Nie, B.; Bao, J.; Zhao, Z.; Feng, X.; Pei, Y.; Yuan, L.; Mei, Z.; et al. Treatment of Type I Endoleak after Endovascular Repair of Infrarenal Abdominal Aortic Aneurysm: Success of Fibrin Glue Sac Embolization. J. Endovasc. Ther. 2010, 17, 687–693. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Type of Study | N Type I | N Type Ia | Age Range (Mean) [Years] | Male Sex [%] | Elective or Urgent | TEVAR | FEVAR | ch-EVAR | EVAS | MARS | Indication | Index Procedure or Reintervention | Diameter (Mean) [mm] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Golzarian [11] | 1997 | R | 7 | 3 | 58–80 * | 100% * | E | 0 | 0 | 0 | 0 | 0 | EL SAC | Re | NA |
| Faries [12] | 2003 | P | 8 | 7 | 76.4 | 86% | NA | 0 | 0 | 0 | 0 | 0 | UNSU UNFIT | Re | 59–82 (64) |
| Maldonado [13] | 2003 | R | 24 | 17 | NA | 83% | E | 0 | 0 | 0 | 0 | 0 | UNSU SAC EL SURG | both (53% index *) | NA |
| Choi [14] | 2011 | R | 7 | 6 | 58–81 (69.3) | 85.7% | both | 0 | 0 | 0 | 0 | 0 | UNSU UNFIT | Re | 58–117 |
| Henrikson [15] | 2011 | R | 6 | 5 | 62–88 (77) | 100% | NA | 1 | 0 | 4 | 0 | 0 | UNSU UNFIT | both (33% index) | 70–93 (83) |
| Chun [16] | 2013 | R | 6 | 4 | 62–82 | 83.3% | E | 2 | 1 | 0 | 0 | 0 | UNSU UNFIT | both (17% index) | NA |
| Eberhardt [17] | 2014 | P | 8 | 7 | 68–86 * | 57.1% | E | 5 | 0 | 0 | 0 | 1 | UNSU UNFIT | Re | NA |
| Ameli-Renani [18] | 2017 | R | 25 | 23 | 64–96 (80) | 80% | both | 1 | 0 | 0 | 11 | 0 | MULTI UNSU primary treatment for EVAS | Re | 53–129 (82) |
| Graif [19] | 2017 | R | 8 | 6 | 77–89 (78) | 75% | E | 0 | 0 | 0 | 0 | 0 | MULTI UNSU UNFIT | Re | NA |
| Marcelin [20] | 2017 | R | 9 | 9 | 62–87 (78.6) | 66.7% | NA | 1 | 0 | 9 | 0 | 0 | UNSU UNFIT MULTI EL + SAC | Re | 58–135 (81) |
| Ierardi [21] | 2018 | R | 8 | 8 | 65–83 (72.5) | 75% | both | 0 | 0 | NA | 0 | 0 | SAC RUP | Re | 54–70 |
| Marchiori [22] | 2019 | R | 22 | 22 | 68–90 (77) | 73% | both (23% urgent) | 0 | 0 | 9 | 1 | 0 | UNSU UNFIT SAC | both (18% index) | 56–117 (74) |
| Author | Year | N Type I | N Type Ia | Age [Years] | Sex | Elective or Urgent | TEVAR | FEVAR | ch-EVAR | EVAS | MARS | Indication | Index Procedure or Reintervention | Diameter [mm] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kirby [23] | 2003 | 1 | 1 | 76 | M | E | 0 | 0 | 0 | 0 | 0 | UNSU UNFIT | Reintervention | 90 |
| Peynicioglu [24] | 2008 | 1 | 1 | 70 | M | E | 0 | 0 | 0 | 0 | 0 | UNFIT EL | Reintervention | >110 |
| Grisafi [25] | 2010 | 1 | 1 | 92 | F | U | 0 | 0 | 0 | 0 | 0 | UNSU SYMPT PAT | Reintervention | 60 |
| Loffroy [26] | 2010 | 1 | 1 | 80 | M | E | 0 | 0 | 0 | 0 | 0 | EL | Reintervention | NA |
| Arici [27] | 2014 | 1 | 1 | 82 | M | E | 0 | 0 | 0 | 0 | 0 | UNSU UNFIT | Reintervention | 73 |
| Gandini [28] | 2015 | 1 | 1 | 82 | M | U | 0 | 0 | 0 | 0 | 0 | UNFIT RUPT | Reintervention | 57 |
| Igari [29] | 2016 | 1 | 1 | 77 | M | E | 0 | 0 | 1 | 0 | 0 | UNSU SAC+EL | Reintervention | 57 |
| Massimi [30] | 2017 | 1 | 1 | 77 | M | E | 0 | 0 | 1 | 0 | 0 | EL | Reintervention | 90 |
| Belczack [31] | 2019 | 1 | 1 | 72 | NA | U | 0 | 0 | 0 | 0 | 0 | UNSU | Index | 64 |
| Author | Time Interval Index to Embolization Procedure (Mean) [Months] | Approach | Embolic Agents | Adj. Type | Adj. % | Adj. Comments | Technical Success |
|---|---|---|---|---|---|---|---|
| Golzarian [11] | 3–8 * | F B | Coils (1 ELIA + gelatin sponge) | 0 | 0 | - | 100% * |
| Faries [12] | 14.5 ± 5.7 | A | Coils | 0 | 0 | - | 100% |
| Maldonado [13] | NA | F | LEA (N) Coils | extender cuff | 29.4% | Performed whenever possible | 92.3% |
| Choi [14] | 0–42 (9.6) | F T | LEA (N) Coils | extender cuff palmaz | 33.3% | - | 85.7% |
| Henrikson [15] | NA | F B | LEA (O) Coils | proximal extension | 40% | - | 100% |
| Chun [16] | 0–72 | A | LEA (O) | 0 | 0 | - | 100% |
| Eberhardt [17] | 0–108 | F B | LEA (O) Coils | endoanchors | 14.3% | - | 100% |
| Ameli-Renani [18] | 0–139 (22.5) | F B | LEA (O) Coils | 0 | 0 | - | 100% |
| Graif [19] | 1.6–106 | F T | LEA (O) Coils Plugs | 0 | 0 | - | 83.3% * |
| Marcelin [20] | 3–15 (6.8) | F | LEA (O) Coils | chimney extensions | NA | chimney extensions | 67% |
| Ierardi [21] | NA | F L | LEA (N,O) Coils | cuff | 50% | - | 100% |
| Marchiori [22] | 0–84 (26) | B | O,C,P | cuff, endoanchors chimney extensions | 54.5% | performed whenever possible | 100% |
| Author | Time Interval (Index to Embolization Procedure) | Approach | Embolic Agents | Adj. Type | Technical Success | Complications | Outcomes | Follow-Up Method | Months | Freedom from Sac Enlargement | Freedom from Endoleak | Recurrence rrence | Reinterventions | Ruptures |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kirby [23] | 2 days | F | LEA (N) | palmaz extender cuff | yes | 0 | Angio EL | CTA | 3 | NA | NA | 0 | 0 | 0 |
| Peynicioglu [24] | 11 days | F | LEA (N) Coils | 0 | yes | 0 | Angio, EL Sac | CTA clinical | 12 | NA | NA | 0 | 0 | 0 |
| Grisafi [25] | 2 years | F | LEA (O) | palmaz extender cuff | yes | 0 | Angio | CT | 12 | NA | NA | 0 | 0 | 0 |
| Loffroy [26] | 2 months | A | Coils | stent-graft extension | yes | 0 | NA | CTA | 6 | NA | yes | 0 | 0 | 0 |
| Arici [27] | 3 months | F | Coils | 0 | yes | 0 | EL Sac | CTA CEUS | 6 | Yes | Endoleak II | 0 | 0 | 0 |
| Gandini [28] | 7 months | C | Coils + thrombin | extender cuff | yes | temporary dialysis (recovery) | Angio EL Sac | NA | 12 | Yes | yes | 0 | 0 | 0 |
| Igari [29] | 2 years | B | Coils | 0 | yes | 0 | EL Sac | duplex | 3 | Yes | NA | 0 | 0 | 0 |
| Massimi [30] | 1 months | C | Coils | 0 | yes | 0 | Angio EL Sac | CTA | 1 | Yes | NA | 0 | 0 | 0 |
| Belczack [31] | intraoperative | NA | Coils | 0 | yes | 0 | Angio | clinical | 0,1 | NA | NA | 0 | 0 | 0 |
| Author | Complication < 30 Days Overall | Minor Complications % (N) | Major Complications % (N) | Procedure Related Complications % (N) | Comments | Deaths < 30 Days % (N) | Recurrences % (N) | N Reinterventions | N Expectant or Palliative | Reinterventions Success % (N) | Recurrences-Comments |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Golzarian [11] | 8.60% | 14.3% (1) | 14.3% (1) | NA | leg paresis, hemodialysis (recovered) sensory deficit (recovered) | 0 | 0 | 0 * | 0 * | - | - |
| Faries [12] | NA | 5.50% | 6.80% | NA | complications overall (not only embolization related) | 0 | 0 | 0 | 0 | - | - |
| Maldonado [13] | NA | NA | 4.2% (1) | NA | colon ischemia and sepsis (death) | 4.2% (1) | 25% (6) | 3 | 3 expectant | 66.7% (2/3) | 1 failed reintervention, underwent open conversion |
| Choi [14] | NA | NA | NA | NA | multiorgan failure in primary rAAA (death) | 14% (1) | 42.8% (3) | NA | NA | - | - |
| Henrikson [15] | NA | NA | 16.6% (1) | 0% | renal chimney and leg extensions occlusion, leg ischemia + renal failure (death) | 0 | NA | NA | NA | - | |
| Chun [16] | 0% | NA | NA | NA | - | 0 | 0 | 0 | 0 | - | |
| Eberhardt [17] | 0% | NA | NA | NA | - | 0 | 12.5% (1) | 1 | NA | 100% (1/1) | 1 failed re-embololization, endoanchors, success |
| Ameli-Renani [18] | 24% (6) | 4.0% (1) | 8% (2) | 12% (3) | puncture site hematomas (conservative or surgical revision) LEA dislocation (intervention, recovered) | 0 | 28% (7) | 5 | 2 palliative | 60% (3/5) | 5 reinterventions including 2 EVAS |
| Graif [19] | NA | NA | NA | NA | - | 0 | 0 | 0 | 0 | - | for ELIA no recurrences |
| Marcelin [20] | 0% | NA | NA | NA | - | 0 | 11.1% (1) | 1 | 0 | 100% (1/1) | |
| Ierardi [21] | 0% | NA | NA | NA | - | 0 | 0 | 0 | 0 | - | |
| Marchiori [22] | 13.5% (3) | 0% | 4.5% (1) | 9% (2) | LEA disclocation (intervention, recovered) chymney occlusion (intervention, recovered) acute coronary syndrome (death) | 4.5% (1) | 38% (8) | 6 | 4 (3 palliative, 1 refused) | 50% (3/6) | 1 failed reintervention, underwent FEVAR, success |
| Author | Outcome | Follow-Up Method | Follow-Up Length (Mean) [Months] | Follow-Up Protocol | Freedom from Sac Enlargement % (N) | Comment Sac Enlargement | Freedom from ELIA % (N) | Conversions | N Ruptures in Follow-Up (Time) | Comment Ruptures | Follow-Up Survival N (Non- Aneurysm Related Deaths) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Golzarian [11] | Sac | CT | 4–9 (7) | CT within 1 week and every 2 months | 100% | 100% | 0 | 0 | NA | ||
| Faries [12] | Sac | CTA | 1–60 (24.5) | CTA at 1–6–12, yearly | 100% | NA | 0 | 0 | NA | ||
| Maldonado [13] | Angio | CT | 0–40 (nBCA * mean 5.9, coils * means 25) | CTA within 1–6–12, yearly | 100% * | 92.30% | 1 | 1 (6 months) | refused reintervention (death) | (2) | |
| Choi [14] | Sac EL | CTA | 0–53 (18) | CTA at 3–6–12, yearly | 83.3% (5/6) | treated with open conversion (n = 1) | NA | 0 | 0 | (2) | |
| Henrikson [15] | NA | CT | 3–18 | CT before discharge and after 1 month | NA | NA | 1 | 1 (18 months) | stent-graft migration and ELIA recurrence, open conversion, recovery | (1) | |
| Chun [16] | Sac EL | CT Duplex | 1–10 | vary | 100% | 50% of patients follow-up with duplex | NA | 0 | 0 | 0 | |
| Eberhardt [17] | Angio Sac EL | CT Duplex | 8–14 | CTA at 6–12 months duplex at 3–6–12, yearly | 100% | 100% | 0 | NA | NA | ||
| Ameli-Renani [18] | Angio | CT Duplex | 0–44.6 (10.2) | NA | 85% | 80% | 0 | 3 (4, 5, 15 months) | ELIA recurrence, not suitable for further interventions | (1) | |
| Graif [19] | Angio EL | CTA Duplex | 0–10 * | CTA, duplex if CTA contraindicated | NA | 66.7 (4/6) | 1 | 1 (2.5 months) | refused reintervention (death) | NA | |
| Marcelin [20] | EL Sac | CTA | 3–35 (16) | CTA at 1–3, 6, 12, yearly | 100% | freedom from sac enlargement after reintervention (n = 1) | 78% including TEVAR | 0 | 0 | (2) | |
| Ierardi [21] | Angio EL Sac | CTA CEUS | 12–30 (16.5) | CEUS before discharge CTA 1–6, 12 months, yearly CT or CEUS at 6 months | 100% | NA | 0 | 0 | (2) | ||
| Marchiori [22] | Angio Sac EL | CTA Duplex MRA | 0–65 (15.4) | CTA within 1, 6, 12, yearly duplex at 6 months | 76% | 4 patients failed secondary procedure, 1 refused it | NA | 0 | 1 (6 months) | contained rupture confirmed at CT | (6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchiori, E.; Ibrahim, A.; Schäfers, J.F.; Oberhuber, A. Embolization for Type Ia Endoleak after EVAR for Abdominal Aortic Aneurysms: A Systematic Review of the Literature. Biomedicines 2022, 10, 1442. https://doi.org/10.3390/biomedicines10061442
Marchiori E, Ibrahim A, Schäfers JF, Oberhuber A. Embolization for Type Ia Endoleak after EVAR for Abdominal Aortic Aneurysms: A Systematic Review of the Literature. Biomedicines. 2022; 10(6):1442. https://doi.org/10.3390/biomedicines10061442
Chicago/Turabian StyleMarchiori, Elena, Abdulhakim Ibrahim, Johannes Frederik Schäfers, and Alexander Oberhuber. 2022. "Embolization for Type Ia Endoleak after EVAR for Abdominal Aortic Aneurysms: A Systematic Review of the Literature" Biomedicines 10, no. 6: 1442. https://doi.org/10.3390/biomedicines10061442
APA StyleMarchiori, E., Ibrahim, A., Schäfers, J. F., & Oberhuber, A. (2022). Embolization for Type Ia Endoleak after EVAR for Abdominal Aortic Aneurysms: A Systematic Review of the Literature. Biomedicines, 10(6), 1442. https://doi.org/10.3390/biomedicines10061442