
Prospective Risk of Type 2 Diabetes in Normal Weight Women with Polycystic Ovary Syndrome



Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Study Outcome
2.3. Exclusion Criteria
2.4. BMI and Body Composition
3. Results
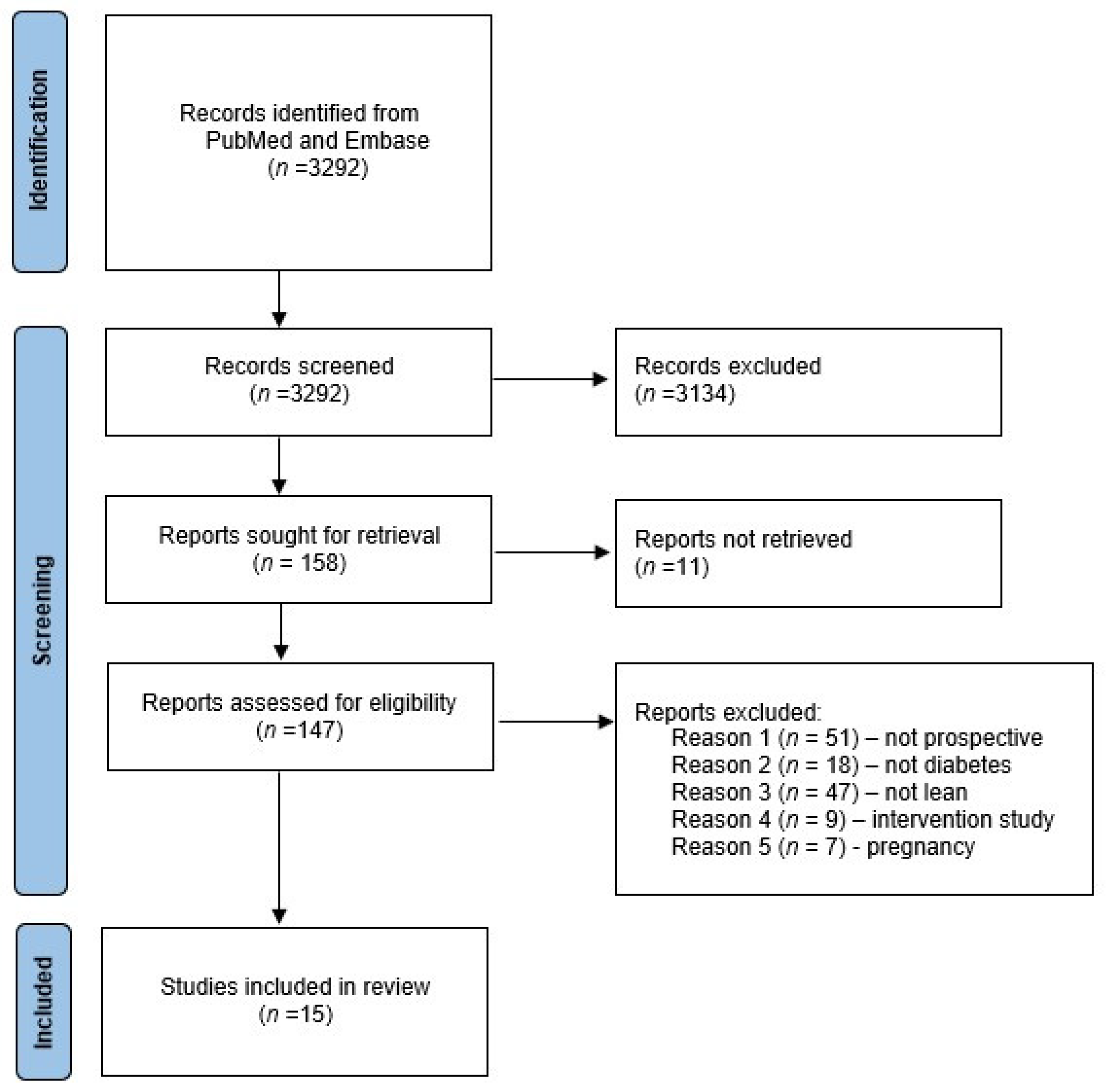
3.1. Study Selection and Descriptive Data
3.2. PCOS and Prospective Risk of T2D
3.2.1. Controlled Studies
3.2.2. Uncontrolled Studies
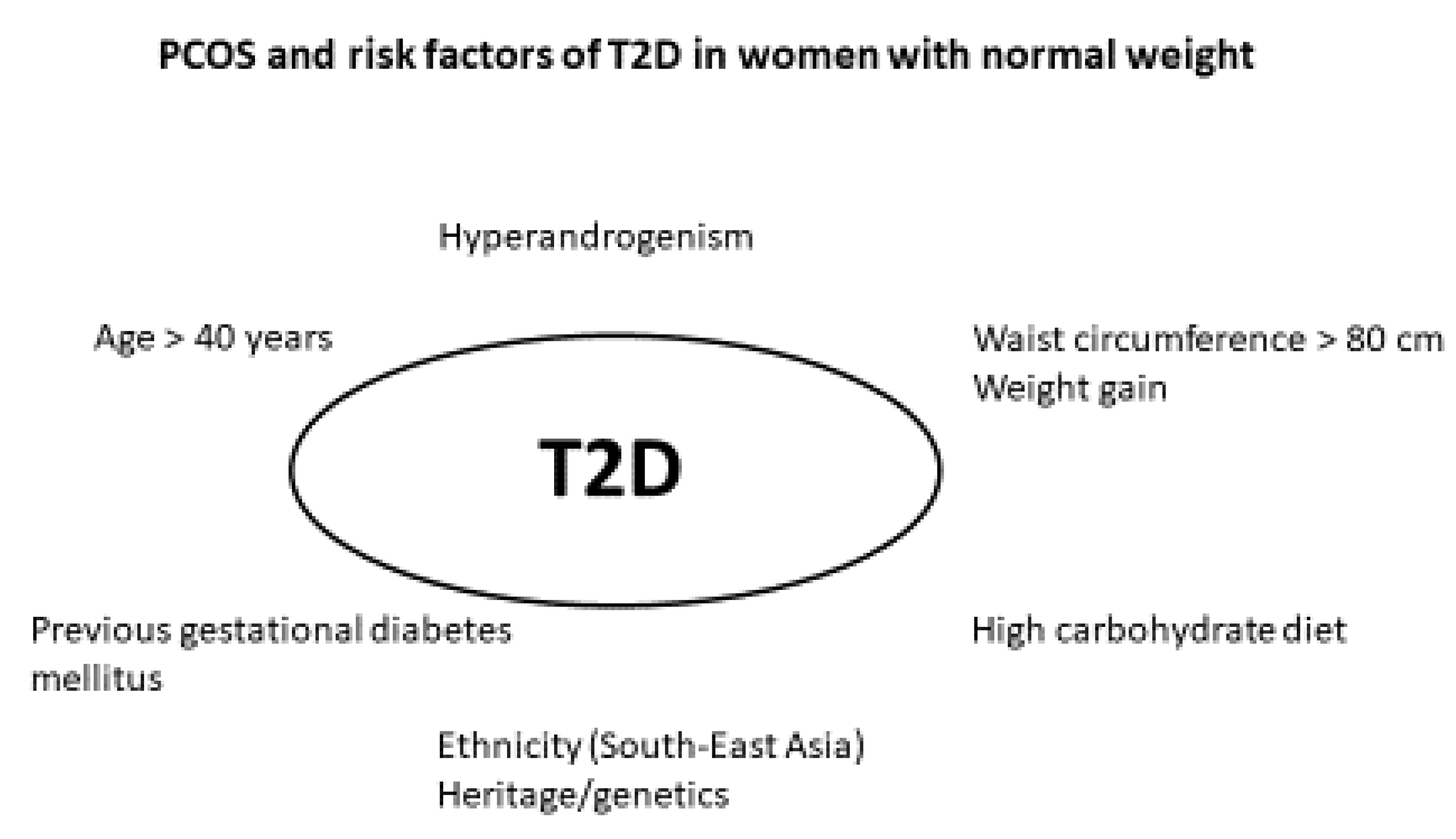
3.2.3. PCOS Phenotype and Risk of T2D
4. Discussion
4.1. Diagnosis of PCOS and Surveillance Bias
4.2. Hyperandrogenism and Metabolic Risk in PCOS
4.3. Menstrual Cycles and Metabolic Risk in PCOS
4.4. Oral Contraceptives and Metabolic Risk in PCOS
4.5. Metformin and Myoinositol in PCOS
4.6. Autoimmunity and Hypovitaminosis D
4.7. Depression
4.8. Ageing and β-Cell Function in PCOS
4.9. Pre-Diabetes and Method for T2D Diagnosis
4.10. Diet Intervention in PCOS
4.11. Ethnicity and T2D
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| FPG | Fasting plasma glucose |
| HbA1c | Hemoglobin A1c |
| HR | Hazard ratio |
| HOMA-IR | Homeostatic Model Assessment for Insulin Resistance |
| IGT | Impaired glucose tolerance |
| IR | Incidence rate |
| IRR | Incidence rate ratio |
| NGT | Normal glucose tolerance |
| NS | Not significant |
| N/A | Not available |
| OGTT | Oral glucose tolerance test, |
| PCOS | Polycystic ovary syndrome |
| PreDM | Prediabetes |
| PY | Person-years |
| T2D | Type 2 diabetes |
References
- Lauritsen, M.P.; Bentzen, J.G.; Pinborg, A.; Loft, A.; Forman, J.L.; Thuesen, L.L.; Cohen, A.; Hougaard, D.M.; Nyboe Andersen, A. The prevalence of polycystic ovary syndrome in a normal population according to the Rotterdam criteria versus revised criteria including anti-Mullerian hormone. Hum. Reprod. 2014, 29, 791–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ESHRE T R, ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Conway, G.; Dewailly, D.; Diamanti-Kandarakis, E.; Escobar-Morreale, H.F.; Franks, S.; Gambineri, A.; Kelestimur, F.; Macut, D.; Micic, D.; Pasquali, R.; et al. The polycystic ovary syndrome: A position statement from the European Society of Endocrinology. Eur. J. Endocrinol. 2014, 171, P1–P29. [Google Scholar] [CrossRef] [Green Version]
- Glintborg, D.; Andersen, M. Management of Endocrine Disease: Morbidity in polycystic ovary syndrome. Eur. J. Endocrinol. 2017, 176, R53–R65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamanti-Kandarakis, E.; Dunaif, A. Insulin resistance and the polycystic ovary syndrome revisited: An update on mechanisms and implications. Endocr. Rev. 2012, 33, 981–1030. [Google Scholar] [CrossRef]
- Lim, S.S.; Davies, M.J.; Norman, R.J.; Moran, L.J. Overweight, obesity and central obesity in women with polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. Update 2012, 18, 618–637. [Google Scholar] [CrossRef]
- Wekker, V.; van Dammen, L.; Koning, A.; Heida, K.Y.; Painter, R.C.; Limpens, J.; Laven, J.S.E.; Roeters van Lennep, J.E.; Roseboom, T.J.; Hoek, A. Long-term cardiometabolic disease risk in women with PCOS: A systematic review and meta-analysis. Hum. Reprod. Update 2020, 26, 942–960. [Google Scholar] [CrossRef]
- Ollila, M.E.; West, S.; Keinanen-Kiukaanniemi, S.; Jokelainen, J.; Auvinen, J.; Puukka, K.; Ruokonen, A.; Jarvelin, M.R.; Tapanainen, J.S.; Franks, S.; et al. Overweight and obese but not normal weight women with PCOS are at increased risk of Type 2 diabetes mellitus-a prospective, population-based cohort study. Hum. Reprod. 2017, 32, 423–431. [Google Scholar] [CrossRef] [Green Version]
- Rubin, K.H.; Glintborg, D.; Nybo, M.; Abrahamsen, B.; Andersen, M. Development and risk factors of type 2 diabetes in a nationwide population of women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2017, 102, 3848–3857. [Google Scholar] [CrossRef] [Green Version]
- Toosy, S.; Sodi, R.; Pappachan, J.M. Lean polycystic ovary syndrome (PCOS): An evidence-based practical approach. J. Diabetes Metab. Disord. 2018, 17, 277–285. [Google Scholar] [CrossRef]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut Off Points. In StatPearls; StatPearls Publishing Copyright© 2022; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Glintborg, D.; Petersen, M.H.; Ravn, P.; Hermann, A.P.; Andersen, M. Comparison of regional fat mass measurement by whole body DXA scans and anthropometric measures to predict insulin resistance in women with polycystic ovary syndrome and controls. Acta Obstet. Gynecol. Scand. 2016, 95, 1235–1243. [Google Scholar] [CrossRef]
- Glintborg, D. Endocrine and metabolic characteristics in polycystic ovary syndrome. Dan. Med. J. 2016, 63, B5232. [Google Scholar]
- Anagnostis, P.; Paparodis, R.D.; Bosdou, J.K.; Bothou, C.; Macut, D.; Goulis, D.G.; Livadas, S. Risk of type 2 diabetes mellitus in polycystic ovary syndrome is associated with obesity: A meta-analysis of observational studies. Endocrine 2021, 74, 245–253. [Google Scholar] [CrossRef]
- Kiconco, S.; Tay, C.T.; Rassie, K.L.; Azziz, R.; Teede, H.J.; Joham, A.E. Natural history of polycystic ovary syndrome: A systematic review of cardiometabolic outcomes from longitudinal cohort studies. Clin. Endocrinol. 2022, 96, 475–498. [Google Scholar] [CrossRef]
- Palm, C.V.B.; Glintborg, D.; Kyhl, H.B.; McIntyre, H.D.; Jensen, R.C.; Jensen, T.K.; Jensen, D.M.; Andersen, M. Polycystic ovary syndrome and hyperglycaemia in pregnancy. A narrative review and results from a prospective Danish cohort study. Diabetes Res. Clin. Pract. 2018. [Google Scholar] [CrossRef] [Green Version]
- Mustaniemi, S.; Vääräsmäki, M.; Eriksson, J.G.; Gissler, M.; Laivuori, H.; Ijäs, H.; Bloigu, A.; Kajantie, E.; Morin-Papunen, L. Polycystic ovary syndrome and risk factors for gestational diabetes. Endocr. Connect. 2018, 7, 859–869. [Google Scholar] [CrossRef]
- Persson, S.; Elenis, E.; Turkmen, S.; Kramer, M.S.; Yong, E.L.; Poromaa, I.S. Higher risk of type 2 diabetes in women with hyperandrogenic polycystic ovary syndrome. Fertil. Steril. 2021, 116, 862–871. [Google Scholar] [CrossRef]
- Pelanis, R.; Mellembakken, J.R.; Sundstrom-Poromaa, I.; Ravn, P.; Morin-Papunen, L.; Tapanainen, J.S.; Piltonen, T.; Puurunen, J.; Hirschberg, A.L.; Fedorcsak, P.; et al. The prevalence of Type 2 diabetes is not increased in normal-weight women with PCOS. Hum. Reprod. 2017, 32, 2279–2286. [Google Scholar] [CrossRef]
- Glintborg, D.; Rubin, K.H.; Nybo, M.; Abrahamsen, B.; Andersen, M. Cardiovascular disease in a nationwide population of Danish women with polycystic ovary syndrome. Cardiovasc. Diabetol. 2018, 17, 37. [Google Scholar] [CrossRef]
- Bryhni, B.; Arnesen, E.; Jenssen, T.G. Associations of age with serum insulin, proinsulin and the proinsulin-to-insulin ratio: A cross-sectional study. BMC Endocr. Disord. 2010, 10, 21. [Google Scholar] [CrossRef] [Green Version]
- Goodman, N.F.; Cobin, R.H.; Futterweit, W.; Glueck, J.S.; Legro, R.S.; Carmina, E. American Association of Clinical Endocrinologists, American College of Endocrinology, and Androgen Excess and Pcos Society Disease State Clinical Review: Guide to the Best Practices in the Evaluation and Treatment of Polycystic Ovary Syndr. Endocr. Pract. 2015, 21, 1415–1426. [Google Scholar] [CrossRef]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. 2018, 33, 1602–1618. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [Green Version]
- Kiconco, S.; Teede, H.J.; Earnest, A.; Loxton, D.; Joham, A.E. Menstrual cycle regularity as a predictor for heart disease and diabetes: Findings from a large population-based longitudinal cohort study. Clin. Endocrinol. 2022, 96, 605–616. [Google Scholar] [CrossRef]
- Ryu, K.J.; Kim, M.S.; Kim, H.K.; Kim, Y.J.; Yi, K.W.; Shin, J.H.; Hur, J.Y.; Kim, T.; Park, H. Risk of type 2 diabetes is increased in nonobese women with polycystic ovary syndrome: The National Health Insurance Service-National Sample Cohort Study. Fertil. Steril. 2021, 115, 1569–1575. [Google Scholar] [CrossRef]
- Kakoly, N.S.; Earnest, A.; Teede, H.J.; Moran, L.J.; Joham, A.E. The Impact of Obesity on the Incidence of Type 2 Diabetes Among Women with Polycystic Ovary Syndrome. Diabetes Care 2019, 42, 560–567. [Google Scholar] [CrossRef] [Green Version]
- Ng, N.Y.H.; Jiang, G.; Cheung, L.P.; Zhang, Y.; Tam, C.H.T.; Luk, A.O.Y.; Quan, J.; Lau, E.S.H.; Yau, T.T.L.; Chan, M.H.M.; et al. Progression of glucose intolerance and cardiometabolic risk factors over a decade in Chinese women with polycystic ovary syndrome: A case-control study. PLoS Med. 2019, 16, e1002953. [Google Scholar] [CrossRef]
- Glintborg, D.; Rubin, K.H.; Abrahamsen, B.; Andersen, M. Response to Letter to the Editor: “Development and Risk Factors of Type 2 Diabetes in a Nationwide Population of Women with Polycystic Ovary Syndrome”. J. Clin. Endocrinol. Metab. 2018, 103, 362–363. [Google Scholar] [CrossRef]
- Ramezani Tehrani, F.; Montazeri, S.A.; Hosseinpanah, F.; Cheraghi, L.; Erfani, H.; Tohidi, M.; Azizi, F. Trend of Cardio-Metabolic Risk Factors in Polycystic Ovary Syndrome: A Population-Based Prospective Cohort Study. PLoS ONE 2015, 10, e0137609. [Google Scholar] [CrossRef] [Green Version]
- Wang, E.T.; Calderon-Margalit, R.; Cedars, M.I.; Daviglus, M.L.; Merkin, S.S.; Schreiner, P.J.; Sternfeld, B.; Wellons, M.; Schwartz, S.M.; Lewis, C.E.; et al. Polycystic ovary syndrome and risk for long-term diabetes and dyslipidemia. Obstet. Gynecol. 2011, 117, 6–13. [Google Scholar] [CrossRef]
- Boudreaux, M.Y.; Talbott, E.O.; Kip, K.E.; Brooks, M.M.; Witchel, S.F. Risk of T2DM and impaired fasting glucose among PCOS subjects: Results of an 8-year follow-up. Curr. Diab. Rep. 2006, 6, 77–83. [Google Scholar] [CrossRef]
- Choi, Y.M.; Hwang, K.R.; Oh, S.H.; Lee, D.; Chae, S.J.; Yoon, S.H.; Kim, J.J. Progression to prediabetes or diabetes in young Korean women with polycystic ovary syndrome: A longitudinal observational study. Clin. Endocrinol. 2021, 94, 837–844. [Google Scholar] [CrossRef]
- Jacewicz-Święcka, M.; Kowalska, I. Changes in Metabolic Profile in the Women with a History of PCOS-A Long-Term Follow-Up Study. J. Clin. Med. 2020, 9, 3367. [Google Scholar] [CrossRef]
- Velija-Asimi, Z.; Burekovic, A.; Dujic, T.; Dizdarevic-Bostandzic, A.; Semiz, S. Incidence of prediabetes and risk of developing cardiovascular disease in women with polycystic ovary syndrome. Bosn. J. Basic Med. Sci. 2016, 16, 298–306. [Google Scholar] [CrossRef] [Green Version]
- Gambineri, A.; Patton, L.; Altieri, P.; Pagotto, U.; Pizzi, C.; Manzoli, L.; Pasquali, R. Polycystic ovary syndrome is a risk factor for type 2 diabetes: Results from a long-term prospective study. Diabetes 2012, 61, 2369–2374. [Google Scholar] [CrossRef] [Green Version]
- Andries, M.; Glintborg, D.; Andersen, M. Risk of impaired glucose tolerance in normal weight hirsute women during four years observation. Acta Obstet. Gynecol. Scand. 2010, 89, 1091–1095. [Google Scholar] [CrossRef]
- Jørgensen, M.E.; Ellervik, C.; Ekholm, O.; Johansen, N.B.; Carstensen, B. Estimates of prediabetes and undiagnosed type 2 diabetes in Denmark: The end of an epidemic or a diagnostic artefact? Scand. J. Public Health 2020, 48, 106–112. [Google Scholar] [CrossRef]
- Beagley, J.; Guariguata, L.; Weil, C.; Motala, A.A. Global estimates of undiagnosed diabetes in adults. Diabetes Res. Clin. Pract. 2014, 103, 150–160. [Google Scholar] [CrossRef]
- Moran, L.J.; Norman, R.J.; Teede, H.J. Metabolic risk in PCOS: Phenotype and adiposity impact. Trends Endocrinol. Metab. 2015, 26, 136–143. [Google Scholar] [CrossRef]
- Xu, Y.; Qiao, J. Association of Insulin Resistance and Elevated Androgen Levels with Polycystic Ovarian Syndrome (PCOS): A Review of Literature. J. Healthc. Eng. 2022, 2022, 9240569. [Google Scholar] [CrossRef]
- Oh, J.Y.; Sung, Y.A.; Lee, H.J. Clinical implications of menstrual cycle length in oligomenorrhoeic young women. Clin. Endocrinol. 2014, 80, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Panidis, D.; Tziomalos, K.; Papadakis, E. Metabolic syndrome in patients with the polycystic ovary syndrome. Expert Rev. Endocrinol. Metab. 2013, 8, 559–568. [Google Scholar] [CrossRef]
- Zhang, H.Y.; Guo, C.X.; Zhu, F.F.; Qu, P.P.; Lin, W.J.; Xiong, J. Clinical characteristics, metabolic features, and phenotype of Chinese women with polycystic ovary syndrome: A large-scale case-control study. Arch. Gynecol. Obstet. 2013, 287, 525–531. [Google Scholar] [CrossRef]
- Teede, H.; Tassone, E.C.; Piltonen, T.; Malhotra, J.; Mol, B.W.; Peña, A.; Witchel, S.F.; Joham, A.; McAllister, V.; Romualdi, D.; et al. Effect of the combined oral contraceptive pill and/or metformin in the management of polycystic ovary syndrome: A systematic review with meta-analyses. Clin. Endocrinol. 2019, 91, 479–489. [Google Scholar] [CrossRef]
- Glintborg, D.; Hass, R.K.; Nybo, M.; Abrahamsen, B.; Andersen, M. Morbidity and medicine prescriptions in a nationwide Danish population of patients diagnosed with polycystic ovary syndrome. Eur. J. Endocrinol. 2015, 172, 627–638. [Google Scholar] [CrossRef] [Green Version]
- de Medeiros, S.F. Risks, benefits size and clinical implications of combined oral contraceptive use in women with polycystic ovary syndrome. Reprod. Biol. Endocrinol. 2017, 15, 93. [Google Scholar] [CrossRef]
- Glintborg, D.; Altinok, M.L.; Mumm, H.; Hermann, A.P.; Ravn, P.; Andersen, M. Body composition is improved during 12 months treatment with metformin alone or combined with oral contraceptives compared to treatment with oral contraceptives in polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2014, 99, 2584–2591. [Google Scholar] [CrossRef] [Green Version]
- Glintborg, D.; Mumm, H.; Holst, J.J.; Andersen, M. Effect of oral contraceptives and/or metformin on GLP-1 secretion and reactive hypoglycemia in PCOS. Endocr. Connect. 2017, 6, 267–277. [Google Scholar] [CrossRef] [Green Version]
- Morin-Papunen, L.C.; Vauhkonen, I.; Koivunen, R.M.; Ruokonen, A.; Martikainen, H.K.; Tapanainen, J.S. Endocrine and metabolic effects of metformin versus ethinyl estradiol-cyproterone acetate in obese women with polycystic ovary syndrome: A randomized study. J. Clin. Endocrinol. Metab. 2000, 85, 3161–3168. [Google Scholar] [CrossRef]
- Christakou, C.; Kollias, A.; Piperi, C.; Katsikis, I.; Panidis, D.; Diamanti-Kandarakis, E. The benefit-to-risk ratio of common treatments in PCOS: Effect of oral contraceptives versus metformin on atherogenic markers. Hormones 2014, 13, 488–497. [Google Scholar] [CrossRef] [Green Version]
- Tay, C.T.; Joham, A.E.; Hiam, D.S.; Gadalla, M.A.; Pundir, J.; Thangaratinam, S.; Teede, H.J.; Moran, L.J. Pharmacological and surgical treatment of nonreproductive outcomes in polycystic ovary syndrome: An overview of systematic reviews. Clin. Endocrinol. 2018, 89, 535–553. [Google Scholar] [CrossRef] [Green Version]
- Zeng, L.; Yang, K. Effectiveness of myoinositol for polycystic ovary syndrome: A systematic review and meta-analysis. Endocrine 2018, 59, 30–38. [Google Scholar] [CrossRef]
- Wang, F.F.; Wu, Y.; Zhu, Y.H.; Ding, T.; Batterham, R.L.; Qu, F.; Hardiman, P.J. Pharmacologic therapy to induce weight loss in women who have obesity/overweight with polycystic ovary syndrome: A systematic review and network meta-analysis. Obes. Rev. 2018, 19, 1424–1445. [Google Scholar] [CrossRef]
- Pkhaladze, L.; Russo, M.; Unfer, V.; Nordio, M.; Basciani, S.; Khomasuridze, A. Treatment of lean PCOS teenagers: A follow-up comparison between Myo-Inositol and oral contraceptives. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 7476–7485. [Google Scholar] [CrossRef]
- Mobeen, H.; Afzal, N.; Kashif, M. Polycystic Ovary Syndrome May Be an Autoimmune Disorder. Scientifica 2016, 2016, 4071735. [Google Scholar] [CrossRef] [Green Version]
- Pergialiotis, V.; Konstantopoulos, P.; Prodromidou, A.; Florou, V.; Papantoniou, N.; Perrea, D.N. Management of Endocrine Disease: The impact of subclinical hypothyroidism on anthropometric characteristics, lipid, glucose and hormonal profile of PCOS patients: A systematic review and meta-analysis. Eur. J. Endocrinol. 2017, 176, R159–R166. [Google Scholar] [CrossRef] [Green Version]
- Glintborg, D.; Rubin, K.; Nybo, M.; Abrahamsen, B.; Andersen, M. Increased risk of thyroid disease in Danish women with polycystic ovary syndrome. Endocr. Connect. 2019, 8, 1405–1415. [Google Scholar] [CrossRef] [Green Version]
- Mogili, K.D.; Karuppusami, R.; Thomas, S.; Chandy, A.; Kamath, M.S.; Tk, A. Prevalence of vitamin D deficiency in infertile women with polycystic ovarian syndrome and its association with metabolic syndrome-A prospective observational study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 229, 15–19. [Google Scholar] [CrossRef]
- Joham, A.E.; Teede, H.J.; Cassar, S.; Stepto, N.K.; Strauss, B.J.; Harrison, C.L.; Boyle, J.; Court, D. Vitamin D in polycystic ovary syndrome: Relationship to obesity and insulin resistance. Mol. Nutr. Food Res. 2016, 60, 110–118. [Google Scholar] [CrossRef] [Green Version]
- Scott, D.; Joham, A.; Teede, H.; Gibson-Helm, M.; Harrison, C.; Cassar, S.; Hutchison, S.; Ebeling, P.R.; Stepto, N.; de Courten, B. Associations of Vitamin D with Inter- and Intra-Muscular Adipose Tissue and Insulin Resistance in Women with and without Polycystic Ovary Syndrome. Nutrients 2016, 8, 774. [Google Scholar] [CrossRef] [Green Version]
- Lagowska, K.; Bajerska, J.; Jamka, M. The Role of Vitamin D Oral Supplementation in Insulin Resistance in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2018, 10, 1637. [Google Scholar] [CrossRef] [Green Version]
- Cinar, N.; Kizilarslanoglu, M.C.; Harmanci, A.; Aksoy, D.Y.; Bozdag, G.; Demir, B.; Yildiz, B.O. Depression, anxiety and cardiometabolic risk in polycystic ovary syndrome. Hum. Reprod. 2011, 26, 3339–3345. [Google Scholar] [CrossRef] [Green Version]
- Lindekilde, N.; Rutters, F.; Erik Henriksen, J.; Lasgaard, M.; Schram, M.T.; Rubin, K.H.; Kivimäki, M.; Nefs, G.; Pouwer, F. Psychiatric disorders as risk factors for type 2 diabetes: An umbrella review of systematic reviews with and without meta-analyses. Diabetes Res. Clin. Pract. 2021, 176, 108855. [Google Scholar] [CrossRef]
- Salvi, V.; Grua, I.; Cerveri, G.; Mencacci, C.; Barone-Adesi, F. The risk of new-onset diabetes in antidepressant users - A systematic review and meta-analysis. PLoS ONE 2017, 12, e0182088. [Google Scholar] [CrossRef] [Green Version]
- Glintborg, D.; Altinok, M.L.; Ravn, P.; Stage, K.B.; Hojlund, K.; Andersen, M. Adrenal activity and metabolic risk during randomized escitalopram or placebo treatment in PCOS. Endocr. Connect. 2018, 7, 479–489. [Google Scholar] [CrossRef] [Green Version]
- Tabak, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimaki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef] [Green Version]
- Glintborg, D.; Mumm, H.; Ravn, P.; Andersen, M. Age associated differences in prevalence of individual rotterdam criteria and metabolic risk factors during reproductive age in 446 caucasian women with polycystic ovary syndrome. Horm. Metab. Res. 2012, 44, 694–698. [Google Scholar] [CrossRef]
- Tuomilehto, J.; Lindstrom, J.; Eriksson, J.G.; Valle, T.T.; Hamalainen, H.; Ilanne-Parikka, P.; Keinanen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef]
- Andersen, M.S.; Glintborg, D. Diagnosis and follow-up of type 2 diabetes in women with PCOS. A role of OGTT? Eur. J. Endocrinol. 2018, 179, D1–D14. [Google Scholar] [CrossRef]
- Velling, M.L.; Mumm, H.; Andersen, M.; Glintborg, D. Hemoglobin A1c as a tool for the diagnosis of type 2 diabetes in 208 premenopausal women with polycystic ovary syndrome. Fertil. Steril. 2011, 96, 1275–1280. [Google Scholar] [CrossRef]
- Rezaee, M.; Asadi, N.; Pouralborz, Y.; Ghodrat, M.; Habibi, S. A Review on Glycosylated Hemoglobin in Polycystic Ovary Syndrome. J. Pediatr. Adolesc. Gynecol. 2016, 29, 562–566. [Google Scholar] [CrossRef]
- Sinning, C.; Makarova, N.; Völzke, H.; Schnabel, R.B.; Ojeda, F.; Dörr, M.; Felix, S.B.; Koenig, W.; Peters, A.; Rathmann, W.; et al. Association of glycated hemoglobin A(1c) levels with cardiovascular outcomes in the general population: Results from the BiomarCaRE (Biomarker for Cardiovascular Risk Assessment in Europe) consortium. Cardiovasc. Diabetol. 2021, 20, 223. [Google Scholar] [CrossRef]
- Lim, S.S.; Hutchison, S.K.; Van Ryswyk, E.; Norman, R.J.; Teede, H.J.; Moran, L.J. Lifestyle changes in women with polycystic ovary syndrome. Cochrane Database Syst. Rev. 2019, 3, Cd007506. [Google Scholar] [CrossRef]
- Moran, L.J.; Tassone, E.C.; Boyle, J.; Brennan, L.; Harrison, C.L.; Hirschberg, A.L.; Lim, S.; Marsh, K.; Misso, M.L.; Redman, L.; et al. Evidence summaries and recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome: Lifestyle management. Obes. Rev. 2020, 21, e13046. [Google Scholar] [CrossRef]
- Hosseini, F.; Jayedi, A.; Khan, T.A.; Shab-Bidar, S. Dietary carbohydrate and the risk of type 2 diabetes: An updated systematic review and dose-response meta-analysis of prospective cohort studies. Sci. Rep. 2022, 12, 2491. [Google Scholar] [CrossRef]
- Kazemi, M.; Hadi, A.; Pierson, R.A.; Lujan, M.E.; Zello, G.A.; Chilibeck, P.D. Effects of Dietary Glycemic Index and Glycemic Load on Cardiometabolic and Reproductive Profiles in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Adv. Nutr. 2021, 12, 161–178. [Google Scholar] [CrossRef]
- Kulshreshtha, B.; Sharma, N.; Pant, S.; Sharma, L.; Pahuja, B.; Singh, P. PCOS patients differ in meal timings rather than total caloric or macronutrient intake in comparison to weight matched controls. Eur J. Obstet. Gynecol. Reprod. Biol. 2022, 270, 11–16. [Google Scholar] [CrossRef]
- Kakoly, N.S.; Khomami, M.B.; Joham, A.E.; Cooray, S.D.; Misso, M.L.; Norman, R.J.; Harrison, C.L.; Ranasinha, S.; Teede, H.J.; Moran, L.J. Ethnicity, obesity and the prevalence of impaired glucose tolerance and type 2 diabetes in PCOS: A systematic review and meta-regression. Hum. Reprod. Update 2018, 24, 455–467. [Google Scholar] [CrossRef]
- Zhao, Y.; Qiao, J. Ethnic differences in the phenotypic expression of polycystic ovary syndrome. Steroids 2013, 78, 755–760. [Google Scholar] [CrossRef]
- Guo, L.; Gordon, N.P.; Chandra, M.; Dayo, O.; Lo, J.C. The Risks of Polycystic Ovary Syndrome and Diabetes Vary by Ethnic Subgroup Among Young Asian Women. Diabetes Care 2021, 44, e129–e130. [Google Scholar] [CrossRef]
- Dumesic, D.A.; Oberfield, S.E.; Stener-Victorin, E.; Marshall, J.C.; Laven, J.S.; Legro, R.S. Scientific Statement on the Diagnostic Criteria, Epidemiology, Pathophysiology, and Molecular Genetics of Polycystic Ovary Syndrome. Endocr. Rev. 2015, 36, 487–525. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Study Descriptives | Total Population | Normal Weight Sub-Cohort | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Author, Year, Country | Design Study, Setting | Population (Number, Age, BMI (kg/m2)) | PCOS Definition | Follow-Up Duration | Definition, BMI (kg/m2) | T2D Definition | Results | Conclusion T2D Normal Weight PCOS vs. Controls | |
| PCOS | Control | ||||||||
| Persson et al., 2021 [18] | Register-based | n = 52,535 (12,362 lean) | n = 254,624 (83,120 lean) | Diagnosis code (ICD-10) | Maximum 19 years | Lean < 25 | Diagnosis code. Medicine prescriptions | HR 2.01 (1.29–3.12) normoandrogenic PCOS vs. controls, HR 4.27 (2.60–7.00) lean hyperandrogenic PCOS vs. controls | Increased risk of T2D in non-obese women with PCOS compared to non-obese controls. Hyperandrogenism independent risk factor in lean women with PCOS |
| Kiconco et al. 2021 Australia [25] | Prospective, birth cohort database | n = 1356 (lean N/A) Age 47.6 ± 1.5 | n = 11,740 (lean N/A) Age 47.6 ± 1.5 | Irregular menses (questionnaire) | 20 years | Healthy weight 18.5–24.9 | Self-reported T2D diagnosis | HR 0.95 (0.52–1.73) in healthy weight women with irregular menses vs. controls | Women with healthy weight did not have increased risk for T2D |
| Ryu et al., 2021 Korea [26] | Prospective, Population-based Register study | n = 1136 (818 lean) Age 15–44 (mean age not presented) BMI 21.79 ± 3.9 | n = 5675 (4.546 lean) Age 15–44 (mean age not presented) BMI 21.06 ± 3.0 | Diagnosis code (ICD-10) | 4.5 years (2.4–6.2) | Non-obese < 25 | Diagnosis code ICD10 | Non-obese PCOS vs. non-obese controls: Adjusted HR (95% CI) 2.3 (1.7–3.2) | Increased risk of T2D in non-obese women with PCOS compared to non-obese controls. |
| Kakoly et al., 2019 Australia [27] | Prospective, Population-based | n = 707 (lean N/A) | n = 7671 (lean N/A) | Self-reported (questionnaire) | 15 years | Lean < 25 | Self-reported T2D diagnosis | Lean PCOS vs. lean controls IRR (95% CI): 4.68 (2.66–7.91) | Increased risk of T2D in lean women with PCOS compared to lean controls. |
| Ng et al., 2019 China [28] | Prospective, Hospital clinic- and community-based | n = 199 (lean N/A) Age 30.6 ± 6.5 BMI 25.9 ± 5.6 | n = 225 (lean N/A) Age 42.6 ± 7.0 BMI 23.2 ± 3.8 | Rotterdam Clinical evaluation | 10.6 ± 1.3 years | Lean < 23 | OGTT | Rate ratio PCOS vs. controls: 1.84 (0.65; 5.25) | No significant difference between lean women and controls. |
| Glintborg et al., 2018 Denmark [9,29] | Prospective, National register and hospital clinic | n= 18,477 Embedded local cohort: n = 1165 (n= 421 lean) Age 29 (22–35) BMI 27.0 (23.0–32.4) | n = 54.680 (lean N/A) Age 29 (23–35) Median BMI N/A | Rotterdam Clinical evaluation (local sub- cohort) | 11.1 years (6.9–16.0) | Lean < 25 | Diagnosis code Medicine prescriptions | Lean PCOS vs. controls:HR 1.22 (0.58; 2.55) | No increased risk of T2D in lean women with PCOS compared to age- and BMI-matched controls. |
| Ollila et al., 2017 Finland [8] | Prospective, Population-based cohort | n = 279 (n = 62 lean) Age 14 (Birth cohort 1966) BMI 28.6 ± 6.3 (end of study) | n = 1577 (559 lean) Age 14 (Birth cohort 1966) BMI 26.3 ± 5.3 (end of study) | Self-report. NIH or diagnosis of PCO/PCOS | 32 years | Lean < 25 | OGTT | Lean PCOS: OR for T2D: 1.10 (0.31–3.80) NS | No significant difference between lean women with PCOS and controls |
| Tehrani et al., 2015 Iran [30] | Prospective, Population-based | n = 85 (normal BMI N/A) Age 29.8 ± 9.2 BMI 27.2 ± 5.3 | n = 552 (Normal BMI N/A) Age 29.3 ± 9.0 BMI 25.6 ± 5.0 | NIH Clinical evaluation | 9.4 years (8.7–10.4) | Normal BMI < 25 | Self-reported diabetes and FPG | Normal BMI PCOS vs. controls: FPG: NS | No significant difference between normal BMI women with PCOS and controls |
| Wang et al., 2011 USA [31] | Prospective, Population-based | n = 53 (n = 31 lean) Age 26.8 ± 3.7 Mean WC 78.5 ± 13.9 | n = 1074 (620 lean) Age 27.3 ± 3.6 Mean WC 77.0 ± 12.5 | Self-reported + testosterone measurement | 18 years | Lean < 25 | FPG | Lean PCOS vs. lean controls: OR T2D: 3.1 (1.2–8.0) | Increased risk of T2D in lean women with PCOS compared to lean controls |
| Boudreaux et al., 2006 USA [32] | Prospective, Hospital clinic | n = 97 (lean N/A) Age 38 ± 5.9 BMI 31.6 ± 9.6 | n = 95 (normal BMI N/A) Age 40 ± 5.2 BMI 26.22 ± 6.00 | NIH Clinical evaluation | 8 years | Lean < 25 (<35) | FPG | Women BMI < 35 kg/m2, PCOS vs. controls adjusted HR = 1.45; 95% CI, 0.41–5.08, p = 0.56. | No significant difference between women with PCOS and controls. |
| Choi et al., 2021 Korea [33] | Prospective, Hospital clinic | n = 252 (waist < 80 cm N = 212) Age 23.2 ± 5.7 BMI 22.7 ± 4.2 | None | Rotterdam Clinical examination | PCOS: 2.9 years (1.5–4.5) Controls: no follow-up | Lean WC < 80 | FPG HbA1c OGTT | Lean PCOS: IR T2D and prediabetes: 5.5 per 1000 PY | Increased risk of prediabetes and T2D in lean women with PCOS compared to general population. Waist circumference not associated with risk for T2D within PCOS group. |
| Jacewicz- Święcka et al., 2020 Poland [34] | Prospective, Outpatient clinic | n = 31 (n = 14 lean) Age 25.5 (21.5–29.2) BMI 25.6 (21.5–31.4) | None | Rotterdam Clinical examination | 10 years (8.9–10.6) | Lean < 25 | OGTT | No participants developed T2D at follow up. All women who developed preDM had WC ≥ 80 cm at follow up | No participants developed T2D |
| Velija-Asimi2016 Bosmia [35] | Prospective, Hospital clinic | n = 148 (n = 57 lean) Age 26 (21–39) | None | Rotterdam Clinical examination | 3 years | Lean < 25 | OGTT | 0/57 lean women developed T2D at follow up. | No development of T2D in lean women with PCOS |
| Gambineri et al., 2012 Italy [36] | Prospective, Hospital clinic | n = 249 (79 lean) Age 23.4 ± 6.3 BMI 29.1 ± 7.0 | None | NIH Clinical examination | 16.9 years | Lean < 25 | OGTT | Lean PCOS: 3/79 developed T2D Incidence rate 0.25 per 100 PY | No increased risk of T2D in lean women with PCOS compared to general population. |
| Andries et al., 2010 Denmark [37] | Prospective, Hospital clinic | n = 36 (69 PCOS and/or hirsutism, 36 lean) Age 31 (27–35) BMI 25.4 (23.0–30.0) | Non | Rotterdam Clinical examination | 4 years (range 2–7) | Lean ≤ 25 | OGTT | Lean PCOS T2D: 3/36 | Increased risk of T2D in lean women with PCOS compared to general population. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glintborg, D.; Kolster, N.D.; Ravn, P.; Andersen, M.S. Prospective Risk of Type 2 Diabetes in Normal Weight Women with Polycystic Ovary Syndrome. Biomedicines 2022, 10, 1455. https://doi.org/10.3390/biomedicines10061455
Glintborg D, Kolster ND, Ravn P, Andersen MS. Prospective Risk of Type 2 Diabetes in Normal Weight Women with Polycystic Ovary Syndrome. Biomedicines. 2022; 10(6):1455. https://doi.org/10.3390/biomedicines10061455
Chicago/Turabian StyleGlintborg, Dorte, Naja Due Kolster, Pernille Ravn, and Marianne Skovsager Andersen. 2022. "Prospective Risk of Type 2 Diabetes in Normal Weight Women with Polycystic Ovary Syndrome" Biomedicines 10, no. 6: 1455. https://doi.org/10.3390/biomedicines10061455
APA StyleGlintborg, D., Kolster, N. D., Ravn, P., & Andersen, M. S. (2022). Prospective Risk of Type 2 Diabetes in Normal Weight Women with Polycystic Ovary Syndrome. Biomedicines, 10(6), 1455. https://doi.org/10.3390/biomedicines10061455