
Diagnostic Value of AngioPLUS Microvascular Imaging in Thyroid Nodule Diagnosis Using Quantitative and Qualitative Vascularity Grading


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Type
2.2. Data Collection Procedures
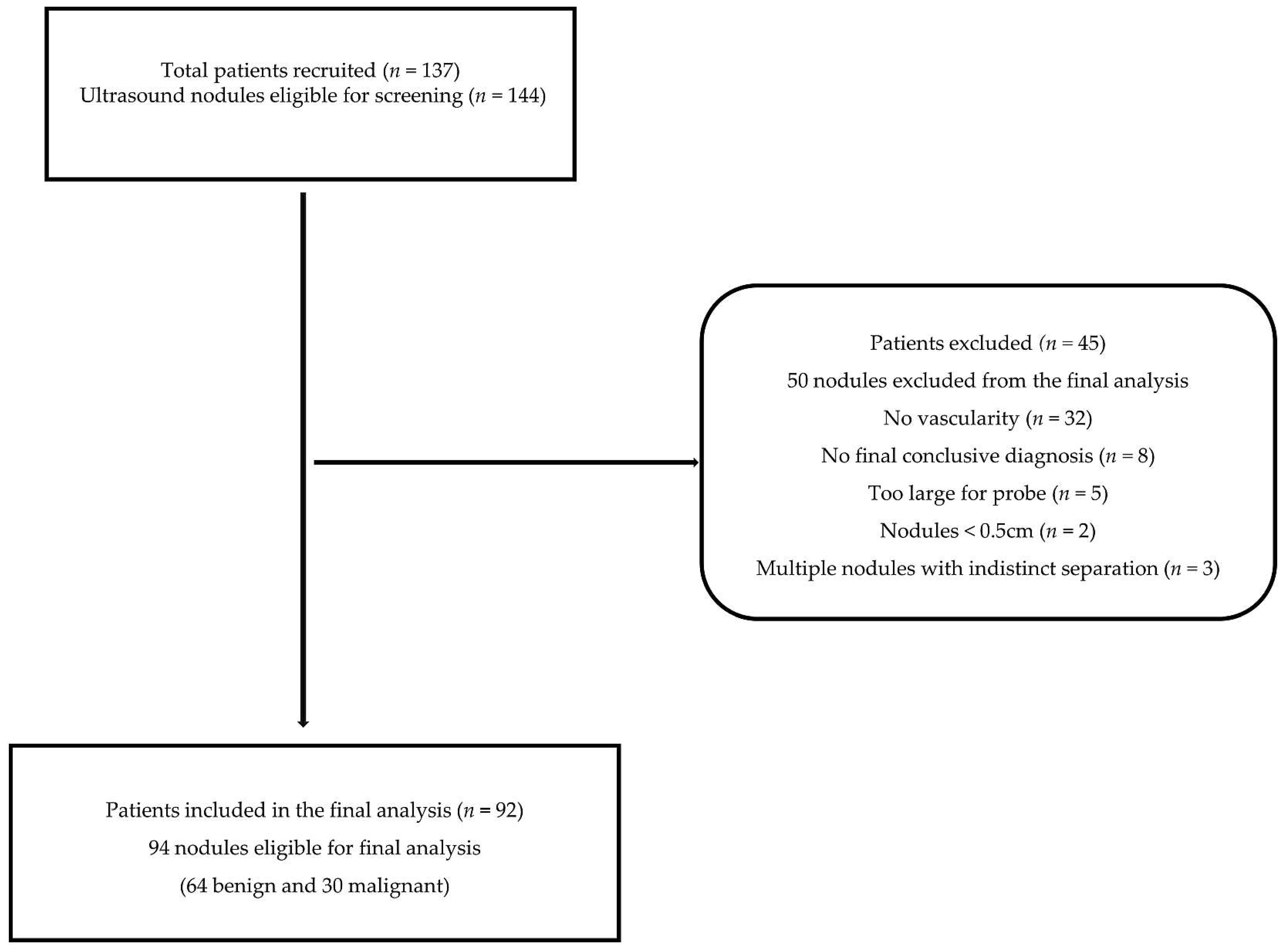
2.2.1. Inclusion and Exclusion Criteria
2.2.2. Ultrasound Imaging Procedures
2.2.3. Grey Scale Ultrasound Feature Assessment
2.2.4. Doppler Ultrasound Feature Assessment
Qualitative Vascularity Assessment
Quantitative Assessment
2.2.5. Data Analysis and Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Thyroid Nodule Vascularity Assessments
3.3. Diagnostic Performance Evaluation of EU TIRADS and Doppler Modes in Thyroid Nodule Malignancy Risk Stratification
3.3.1. Sole Diagnostic Performance Assessments
3.3.2. Combination Approach Diagnostic Performance Assessments
4. Discussion
4.1. Grey Scale Ultrasound Assessment with EU TIRADS
4.2. Qualitative Vascularity Assessment of AngioPLUS Combined with EU TIRADS
4.3. Quantitative Vascularity Assessment of AngioPLUS in Combination with EU TIRADS
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Li, H.; Wang, M.; Li, N.; Tian, T.; Wu, Y.; Xu, P.; Yang, S.; Zhai, Z.; Zhou, L.; et al. Global Burden of Thyroid Cancer From 1990 to 2017. JAMA Netw. Open 2020, 3, e208759. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Piao, J.; Li, M. Secular Trends in the Epidemiologic Patterns of Thyroid Cancer in China Over Three Decades: An Updated Systematic Analysis of Global Burden of Disease Study 2019 Data. Front. Endocrinol. 2021, 12, 707233. [Google Scholar] [CrossRef] [PubMed]
- Olson, E.; Wintheiser, G.; Wolfe, K.M.; Droessler, J.; Silberstein, P.T. Epidemiology of Thyroid Cancer: A Review of the National Cancer Database, 2000–2013. Cureus 2019, 11, e4127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda-Filho, A.; Lortet-Tieulent, J.; Bray, F.; Cao, B.; Franceschi, S.; Vaccarella, S.; Dal Maso, L. Thyroid cancer incidence trends by histology in 25 countries: A population-based study. Lancet Diabetes Endocrinol. 2021, 9, 225–234. [Google Scholar] [CrossRef]
- Li, M.; Maso, L.D.; Vaccarella, S. Global trends in thyroid cancer incidence and the impact of overdiagnosis. Lancet Diabetes Endocrinol. 2020, 8, 468–470. [Google Scholar] [CrossRef]
- Tamhane, S.; Gharib, H. Thyroid nodule update on diagnosis and management. Clin. Diabetes Endocrinol. 2016, 2, 17. [Google Scholar] [CrossRef] [Green Version]
- Perros, P.; Boelaert, K.; Colley, S.; Evans, C.; Evans, R.M.; Gerrard BA, G.; Gilbert, J.; Harrison, B.; Johnson, S.J.; Giles, T.E.; et al. Guidelines for the management of thyroid cancer. Clin. Endocrinol. 2014, 81, 1–122. [Google Scholar] [CrossRef]
- Lew, J.I.; Solorzano, C.C. Use of Ultrasound in the Management of Thyroid Cancer. Oncologist 2010, 15, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Russ, G.; Bonnema, S.J.; Erdogan, M.F.; Durante, C.; Ngu, R.; Leenhardt, L. European Thyroid Association Guidelines for Ultrasound Malignancy Risk Stratification of Thyroid Nodules in Adults: The EU-TIRADS. Eur. Thyroid J. 2017, 6, 225–237. [Google Scholar] [CrossRef] [Green Version]
- Carmeliet, P.; Jain, R.K. Angiogenesis in cancer and other diseases. Nature 2000, 407, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Ringel, M.D.; Burgun, S.J. Recombinant Human Thyrotropin. In Thyroid Cancer; Springer: Berlin/Heidelberg, Germany, 2016; pp. 119–129. [Google Scholar] [CrossRef]
- Rios, A.; Torregrosa, B.; Rodrίguez, J.M.; Rodrίguez, D.; Cepero, A.; Abellán, M.D.; Torregrosa, N.M.; Hernández, A.M.; Parrilla, P. Ultrasonographic risk factors of malignancy in thyroid nodules. Langenbeck’s Arch. Surg. 2016, 401, 839–849. [Google Scholar] [CrossRef] [PubMed]
- Papini, E.; Guglielmi, R.; Bianchini, A.; Crescenzi, A.; Taccogna, S.; Nardi, F.; Panunzi, C.; Rinaldi, R.; Toscano, V.; Pacella, C.M. Risk of Malignancy in Nonpalpable Thyroid Nodules: Predictive Value of Ultrasound and Color-Doppler Features. J. Clin. Endocrinol. Metab. 2002, 87, 1941–1946. [Google Scholar] [CrossRef]
- Frates, M.C.; Benson, C.B.; Doubilet, P.M.; Cibas, E.S.; Marqusee, E. Can color doppler sonography aid in the prediction of malignancy of thyroid nodules? J. Ultrasound Med. 2003, 22, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Anil, G.; Hegde, A.; Chong, F.H.V. Thyroid nodules: Risk stratification for malignancy with ultrasound and guided biopsy. Cancer Imaging 2011, 11, 209–223. [Google Scholar] [CrossRef] [PubMed]
- Rago, T.; Vitti, P.; Chiovato, L.; Mazzeo, S.; De Liperi, A.; Miccoli, P.; Viacava, P.; Bogazzi, F.; Martino, E.; Pinchera, A. Role of conventional ultrasonography and color flow-doppler sonography in predicting malignancy in ‘cold’ thyroid nodules. Eur. J. Endocrinol. 1998, 138, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Moon, H.J.; Kwak, J.Y.; Kim, M.J.; Son, E.J.; Kim, E.-K. Can Vascularity at Power Doppler US Help Predict Thyroid Malignancy? Radiology 2010, 255, 260–269. [Google Scholar] [CrossRef]
- Floridi, C.; Cellina, M.; Buccimazza, G.; Arrichiello, A.; Sacrini, A.; Arrigoni, F.; Pompili, G.; Barile, A.; Carrafiello, G. Ultrasound imaging classifications of thyroid nodules for malignancy risk stratification and clinical management: State of the art. Gland Surg. 2019, 8, S233–S244. [Google Scholar] [CrossRef]
- MacHado, P.; Segal, S.; Lyshchik, A.; Forsberg, F. A novel microvascular flow technique: Initial results in thyroids. Ultrasound Q. 2016, 32, 67–74. [Google Scholar] [CrossRef]
- Bercoff, J.; Tanter, M. Ultrasound Imaging Goes Ultrafast: A Change in Paradigm in Medical Ultrasound. Med. Phys. Int. 2015, 3, 109–119. [Google Scholar]
- Zhu, Y.-C.; Zhang, Y.; Deng, S.-H.; Jiang, Q. A Prospective Study to Compare Superb Microvascular Imaging with Grayscale Ultrasound and Color Doppler Flow Imaging of Vascular Distribution and Morphology in Thyroid Nodules. Med. Sci. Monit. 2018, 24, 9223–9231. [Google Scholar] [CrossRef] [PubMed]
- Cappelli, C.; Pirola, I.; Gandossi, E.; Marini, F.; Cristiano, A.; Casella, C.; Lombardi, D.; Agosti, B.; Ferlin, A.; Castellano, M. Ultrasound microvascular blood flow evaluation: A new tool for the management of thyroid nodule? Int. J. Endocrinol. 2019, 2019, 7874890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.; Liao, Q.; Wang, Y.; Hu, Y.; Zhu, Q.L.; Wang, L.; Liu, Q.Q.; Li, J.C.; Jiang, Y.X. A new tool for diagnosing parathyroid lesions: Angio plus ultrasound imaging. J. Thorac. Dis. 2019, 11, 4829–4834. [Google Scholar] [CrossRef] [PubMed]
- Russ, G.; Trimboli, P.; Buffet, C. The New Era of TIRADSs to Stratify the Risk of Malignancy of Thyroid Nodules: Strengths, Weaknesses and Pitfalls. Cancers 2021, 13, 4316. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Baek, J.H.; Chung, J.; Ha, E.J.; Kim, J.H.; Lee, Y.H.; Lim, H.K.; Moon, W.J.; Na, D.G.; Park, J.S.; et al. Ultrasonography diagnosis and imaging-based management of thyroid nodules: Revised Korean society of thyroid radiology consensus statement and recommendations. Korean J. Radiol. 2016, 17, 370–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chammas, M.C.; Gerhard, R.; Oliveira, I.R.S.D.; Widman, A.; Barros, N.D.; Durazzo, M.; Ferraz, A.; Cerri, G.G. Thyroid nodules: Evaluation with power Doppler and duplex Doppler ultrasound. Otolaryngol. Head Neck Surg. 2005, 132, 874–882. [Google Scholar] [CrossRef]
- Ying, M.; Ng, D.K.; Yung, D.M.; Lee, E.S. A semi-quantitative approach to compare high-sensitivity power Doppler sonography and conventional power Doppler sonography in the assessment of thyroid vascularity. Thyroid 2009, 19, 1265–1269. [Google Scholar] [CrossRef]
- Ying, M.; Cheng, S.C.H.; Ahuja, A.T. Diagnostic Accuracy of Computer-Aided Assessment of Intranodal Vascularity in Distinguishing Different Causes of Cervical Lymphadenopathy. Ultrasound Med. Biol. 2016, 42, 2010–2016. [Google Scholar] [CrossRef]
- Baig, F.N.; Van Lunenburg, J.T.J.; Liu, S.Y.W.; Yip, S.P.; Law, H.K.W.; Ying, M. Computer-aided assessment of regional vascularity of thyroid nodules for prediction of malignancy. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Lee, D.K. What is the proper way to apply the multiple comparison test? Korean J. Anesthesiol. 2018, 71, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Castellana, M.; Castellana, C.; Treglia, G.; Giorgino, F.; Giovanella, L.; Russ, G.; Trimboli, P. Performance of five ultrasound risk stratification systems in selecting thyroid nodules for FNA. A meta-analysis. J. Clin. Endocrinol. Metab. 2020, 105. [Google Scholar] [CrossRef] [PubMed]
- Koc, A.M.; Adıbelli, Z.H.; Erkul, Z.; Sahin, Y.; Dilek, I. Comparison of diagnostic accuracy of ACR-TIRADS, American Thyroid Association (ATA), and EU-TIRADS guidelines in detecting thyroid malignancy. Eur. J. Radiol. 2020, 133, 109390. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, P.; Ngu, R.; Royer, B.; Giovanella, L.; Bigorgne, C.; Simo, R.; Carroll, P.; Russ, G. A multicentre validation study for the EU-TIRADS using histological diagnosis as a gold standard. Clin. Endocrinol. 2019, 91, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Słowińska-Klencka, D.; Wysocka-Konieczna, K.; Klencki, M.; Popowicz, B. Diagnostic Value of Six Thyroid Imaging Reporting and Data Systems (TIRADS) in Cytologically Equivocal Thyroid Nodules. J. Clin. Med. 2020, 9, 2281. [Google Scholar] [CrossRef] [PubMed]
- Słowińska-Klencka, D.; Wysocka-Konieczna, K.; Klencki, M.; Popowicz, B. Usability of EU-TIRADS in the Diagnostics of Hürthle Cell Thyroid Nodules with Equivocal Cytology. J. Clin. Med. 2020, 9, 3410. [Google Scholar] [CrossRef]
- Chung, J.; Lee, Y.J.; Choi, Y.J.; Ha, E.J.; Suh, C.H.; Choi, M.; Baek, J.H.; Na, D.G. Clinical applications of Doppler ultrasonography for thyroid disease: Consensus statement by the Korean Society of Thyroid Radiology. Ultrasonography 2020, 39, 315–330. [Google Scholar] [CrossRef]
- Hong, Y.-r.; Wu, Y.-l.; Luo, Z.-y.; Wu, N.-b.; Liu, X.-m. Impact of nodular size on the predictive values of gray-scale, color-Doppler ultrasound, and sonoelastography for assessment of thyroid nodules. J. Zhejiang Univ. Sci. B 2012, 13, 707–716. [Google Scholar] [CrossRef] [Green Version]
- Wettasinghe, M.C.; Rosairo, S.; Ratnatunga, N.; Wickramasinghe, N.D. Diagnostic accuracy of ultrasound characteristics in the identification of malignant thyroid nodules. BMC Res. Notes 2019, 12, 193. [Google Scholar] [CrossRef]
- Kalantari, S. The Diagnostic Value of Color Doppler Ultrasonography in Predicting Thyroid Nodules Malignancy. Int. Tinnitus J. 2018, 22, 35–39. [Google Scholar] [CrossRef]
- Deng, S.; Jiang, Q.; Zhu, Y.; Zhang, Y. An analysis of the clinical value of high-frequency color Doppler ultrasound in the differential diagnosis of benign and malignant thyroid nodules. Int. J. Clin. Exp. Med. 2018, 11, 2331–2336. [Google Scholar]
- Rosario, P.W.; da Silva, A.L.; Borges, M.A.R.; Calsolari, M.R. Is Doppler ultrasound of additional value to gray-scale ultrasound in differentiating malignant and benign thyroid nodules? Arch. Endocrinol. Metab. 2015, 59, 79–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, J.; Li, J.-c.; Wang, H.-y.; Wang, Y.-h.; Zhao, R.-n.; Zhang, Y.; Jin, J. Role of Superb Micro-Vascular Imaging in the Preoperative Evaluation of Thyroid Nodules: Comparison With Power Doppler Flow Imaging. J. Ultrasound Med. 2017, 36, 1329–1337. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhan, J.; Diao, X.H.; Liu, Y.C.; Shi, Y.X.; Chen, Y.; Zhan, W.W. Additional Value of Superb Microvascular Imaging for Thyroid Nodule Classification with the Thyroid Imaging Reporting and Data System. Ultrasound Med. Biol. 2019, 45, 2040–2048. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Kim, E.-K.; Kwak, J.Y.; Park, V.Y.; Moon, H.J. Application of Various Additional Imaging Techniques for Thyroid Ultrasound: Direct Comparison of Combined Various Elastography and Doppler Parameters to Gray-Scale Ultrasound in Differential Diagnosis of Thyroid Nodules. Ultrasound Med. Biol. 2018, 44, 1679–1686. [Google Scholar] [CrossRef]
- Ahn, H.S.; Lee, J.B.; Seo, M.; Park, S.H.; Choi, B.I. Distinguishing benign from malignant thyroid nodules using thyroid ultrasonography: Utility of adding superb microvascular imaging and elastography. Radiol. Med. 2018, 123, 260–270. [Google Scholar] [CrossRef]
- Hong, M.J.; Ahn, H.S.; Ha, S.M.; Park, H.J.; Oh, J. Quantitative analysis of vascularity for thyroid nodules on ultrasound using superb microvascular imaging: Can nodular vascularity differentiate between malignant and benign thyroid nodules? Medicine 2022, 101, e28725. [Google Scholar] [CrossRef]
- Yoon, J.H.; Shin, H.J.; Kim, E.-K.; Moon, H.J.; Roh, Y.H.; Kwak, J.Y. Quantitative Evaluation of Vascularity Using 2-D Power Doppler Ultrasonography May Not Identify Malignancy of the Thyroid. Ultrasound Med. Biol. 2015, 41, 2873–2883. [Google Scholar] [CrossRef]
- Wu, M.H.; Chen, C.N.; Chen, K.Y.; Ho, M.C.; Tai, H.C.; Chung, Y.C.; Lo, C.P.; Chen, A.; Chang, K.J. Quantitative Analysis of Dynamic Power Doppler Sonograms for Patients with Thyroid Nodules. Ultrasound Med. Biol. 2013, 39, 1543–1551. [Google Scholar] [CrossRef]
- Sultan, L.R.; Xiong, H.; Zafar, H.M.; Schultz, S.M.; Langer, J.E.; Sehgal, C.M. Vascularity Assessment of Thyroid Nodules by Quantitative Color Doppler Ultrasound. Ultrasound Med. Biol. 2015, 41, 1287–1293. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Doppler Mode Pairs at Segmented Regions | Descriptive Statistics | Paired Sample t-Tests | |||||
|---|---|---|---|---|---|---|---|
| Mean VI | SD | SEM | t | df | p-Value (2-Tailed) | ||
| Peripheral VI | CFI | 44.92 | 16.05 | 1.66 | −8.89 | 93 | <0.001 |
| CFI + AngioPLUS | 55.29 | 16.74 | 1.73 | ||||
| PDI | 30.91 | 12.81 | 1.32 | −18.46 | 93 | <0.001 | |
| PDI + AngioPLUS | 57.34 | 17.82 | 1.84 | ||||
| Central VI | CFI | 36.70 | 19.88 | 2.05 | −7.64 | 93 | <0.001 |
| CFI + AngioPLUS | 48.07 | 19.20 | 1.98 | ||||
| PDI | 26.14 | 14.76 | 1.52 | −11.89 | 93 | <0.001 | |
| PDI + AngioPLUS | 49.55 | 21.29 | 2.20 | ||||
| EU TIRADS | ||
|---|---|---|
| Diagnostic Performance Measures | All Nodules (n = 94) | Equivocal Nodules (n = 40) |
| SEN (%) | 83.3 (65.3; 94.4) | 88.9 (51.8; 99.7) |
| SPEC (%) | 50.0 (37.2; 62.8) | 38.7 (21.8; 57.8) |
| PPV (%) | 43.9 (30.7; 57.6) | 29.6 (13.8; 50.2) |
| NPV (%) | 86.5 (71.2; 95.5) | 92.3 (64.0; 99.8) |
| AUROC | 0.67 (0.57; 0.76) | 0.62 (0.47; 0.78) |
| Qualitative Vascularity Grading Modes | |||||
|---|---|---|---|---|---|
| Nodules | Diagnostic Performance | CFI | ACFI | PDI | APDI |
| All (n = 94) | SEN (%) | 53.3 * (34.3; 71.7) | 80.0 (61.4; 92.3) | 46.7 ‡ (28.3; 65.7) | 83.3(65.3; 94.4) |
| SPEC (%) | 92.2 (82.7; 97.4) | 82.8 (71.3; 91.1) | 95.3 (86.9; 99.0) | 81.3 (69.5; 89.9) | |
| NPV (%) | 80.8 (69.9; 89.1) | 89.8 (79.2; 96.2) | 79.2 (68.5; 87.6) | 91.2 (80.7; 97.1) | |
| PPV (%) | 76.2 (52.8; 91.8) | 68.6 (50.7; 83.1) | 82.4 (56.6; 96.2) | 67.6 (50.2; 82.0) | |
| AUROC | 0.73 (0.63; 0.82) | 0.81 (0.73; 0.90) | 0.71 ‡ (0.62; 0.80) | 0.82(0.74; 0.91) | |
| Equivocal (n = 40) | SEN (%) | 66.7 * (29.9; 92.5) | 88.9 (51.8; 99.7) | 66.7 ‡ (29.9; 92.5) | 100 (66.4; 100) |
| SPEC (%) | 90.3 (74.2; 98.0) | 80.6 (62.5; 92.5) | 93.5 (78.6; 99.2) | 77.4 (58.9; 90.4) | |
| NPV (%) | 90.3 (74.2; 98.0) | 96.2 (80.4; 99.9) | 90.6 (75.0; 98.0) | 100 (.) | |
| PPV (%) | 66.7 (29.9; 92.5) | 57.1 (28.9; 82.3) | 75.0 (34.9; 96.8) | 56.3 (29.2; 80.2) | |
| AUROC | 0.79 (0.61; 0.96) | 0.85 (0.72; 0.98) | 0.80 (0.63; 0.97) | 0.89 (0.81; 0.96) | |
| Quantitative Vascularity Grading Modes | |||||
|---|---|---|---|---|---|
| Nodules | Diagnostic Performance | CFI | ACFI | PDI | APDI |
| All (n = 94) | SEN (%) | 56.7 (37.4 ; 74.5) | 60.0 (40.6 ; 77.3) | 46.7 (28.3 ; 65.7) | 66.7 (47.2 ; 82.7) |
| SPEC (%) | 81.3 (69.5 ; 89.9) | 73.4 (60.9 ; 83.7) | 65.6 (52.7 ; 77.1) §§ | 73.4 (60.9 ; 83.7) | |
| NPV (%) | 80.0 (68.2 ; 88.9) | 79.7 (67.2 ; 89.0) | 72.4 (59.1 ; 83.3) | 82.5 (70.1 ; 91.3) | |
| PPV (%) | 58.6 (38.9 ; 76.5) | 51.4 (34.0 ; 68.6) | 38.9 (23.1 ; 56.5) | 54.1 (36.9 ; 70.5) | |
| AUROC | 0.69 (0.59 ; 0.79) †† | 0.67 (0.56 ; 0.77) | 0.56 (0.45 ; 0.67) | 0.70 (0.60 ; 0.80) †† | |
| Equivocal (n = 40) | SEN (%) | 66.7 (29.9 ; 92.5) | 55.6 (21.2 ; 86.3) | 33.3 (7.5 ; 70.1) ᵻ | 77.8 (40.0 ; 97.2) ᵻ |
| SPEC (%) | 83.9 (66.3 ; 94.5) | 67.7 (48.6 ; 83.3) | 61.3 (42.2 ; 78.2) | 74.2 (55.4 ; 88.1) | |
| NPV (%) | 89.7 (72.6 ; 97.8) | 84.0 (63.9 ; 95.5) | 76.0 (54.9 ; 90.6) | 92.0 (74.0 ; 99.0) | |
| PPV (%) | 54.5 (23.4 ; 83.3) | 33.3 (11.8 ; 61.6) | 20.0 (4.3 ; 48.1) | 46.7 (21.3 ; 73.4) | |
| AUROC | 0.75 (0.58; 0.93) †† | 0.62 (0.43; 0.81) | 0.47 (0.29; 0.66) | 0.76 (0.60; 0.92) †† | |
| Nodules | Diagnostic Performance Measures | GSU | GSU + Qualitative Vascularity | GSU + Quantitative Vascularity |
|---|---|---|---|---|
| EU | EU + APDI_Qual | EU + APDI_RVI | ||
| All (n = 94) | SEN (%) | 83.3 (65.3 ; 94.4) | 76.7 (57.7 ; 90.1) | 58.1 (39.1 ; 75.5) * |
| SPEC (%) | 50.0 (37.2 ; 62.8) | 84.4 (73.1 ; 92.2) *** | 81.0 (69.1 ; 89.8) *** | |
| PPV (%) | 43.9 (30.7 ; 57.6) | 69.7 (51.3 ; 84.4) | 60.0 (40.6 ; 77.3) | |
| NPV (%) | 86.5 (71.2 ; 95.5) | 88.5 (77.8 ; 95.3) | 79.7 (67.8 ; 88.7) | |
| AUROC | 0.67 (0.57 ; 0.76) | 0.81 (0.72 ; 0.89) * | 0.70 (0.60 ; 0.80) | |
| Equivocal (n = 40) | SEN (%) | 88.9 (51.8 ; 99.7) | 88.9 (51.8 ; 99.7) | 66.7 (29.9 ; 92.5) |
| SPEC (%) | 38.7 (21.8 ; 57.8) | 77.4 (58.9 ; 90.4) *** | 74.2 (55.4 ; 88.1) *** | |
| PPV (%) | 29.6 (13.8 ; 50.2) | 53.3 (26.6 ; 78.7) | 42.9 (17.7 ; 71.1) | |
| NPV (%) | 92.3 (64.0 ; 99.8) | 96.0 (79.6 ; 99.9) | 88.5 (69.8 ; 97.6) | |
| AUROC | 0.62 (0.47; 0.78) | 0.83 (0.70; 0.96) *** | 0.70 (0.52; 0.89) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chambara, N.; Liu, S.Y.W.; Lo, X.; Ying, M. Diagnostic Value of AngioPLUS Microvascular Imaging in Thyroid Nodule Diagnosis Using Quantitative and Qualitative Vascularity Grading. Biomedicines 2022, 10, 1554. https://doi.org/10.3390/biomedicines10071554
Chambara N, Liu SYW, Lo X, Ying M. Diagnostic Value of AngioPLUS Microvascular Imaging in Thyroid Nodule Diagnosis Using Quantitative and Qualitative Vascularity Grading. Biomedicines. 2022; 10(7):1554. https://doi.org/10.3390/biomedicines10071554
Chicago/Turabian StyleChambara, Nonhlanhla, Shirley Yuk Wah Liu, Xina Lo, and Michael Ying. 2022. "Diagnostic Value of AngioPLUS Microvascular Imaging in Thyroid Nodule Diagnosis Using Quantitative and Qualitative Vascularity Grading" Biomedicines 10, no. 7: 1554. https://doi.org/10.3390/biomedicines10071554
APA StyleChambara, N., Liu, S. Y. W., Lo, X., & Ying, M. (2022). Diagnostic Value of AngioPLUS Microvascular Imaging in Thyroid Nodule Diagnosis Using Quantitative and Qualitative Vascularity Grading. Biomedicines, 10(7), 1554. https://doi.org/10.3390/biomedicines10071554