
Paper-Based Interleukin-6 Test Strip for Early Detection of Wound Infection



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. CRP
2.3. Enzyme-Linked Immunosorbent Assay (ELISA) for IL-6 Measurement in Wound Samples
2.4. Lateral Flow Immunoassay-Based IL-6 Test Strip with Reflectance Spectral Analysis
2.5. Performance of IL-6 Test Strip
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study
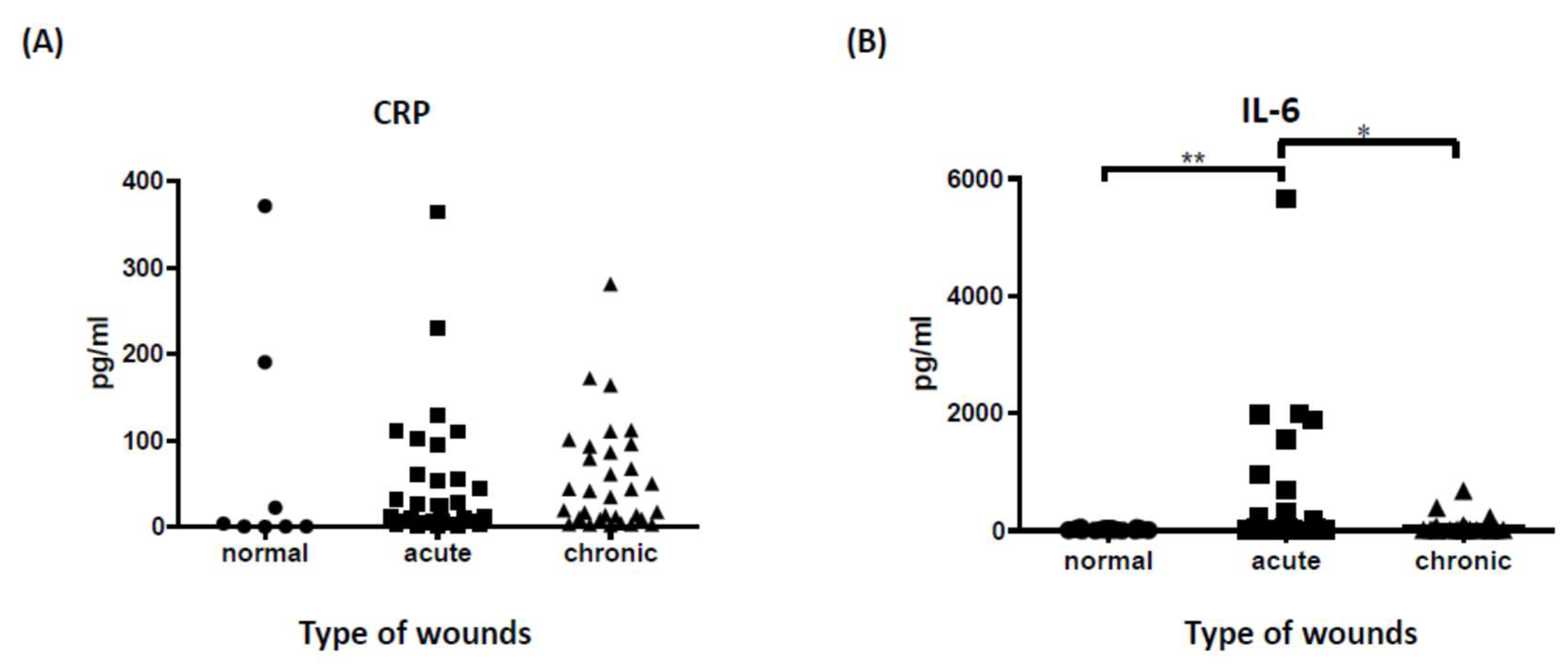
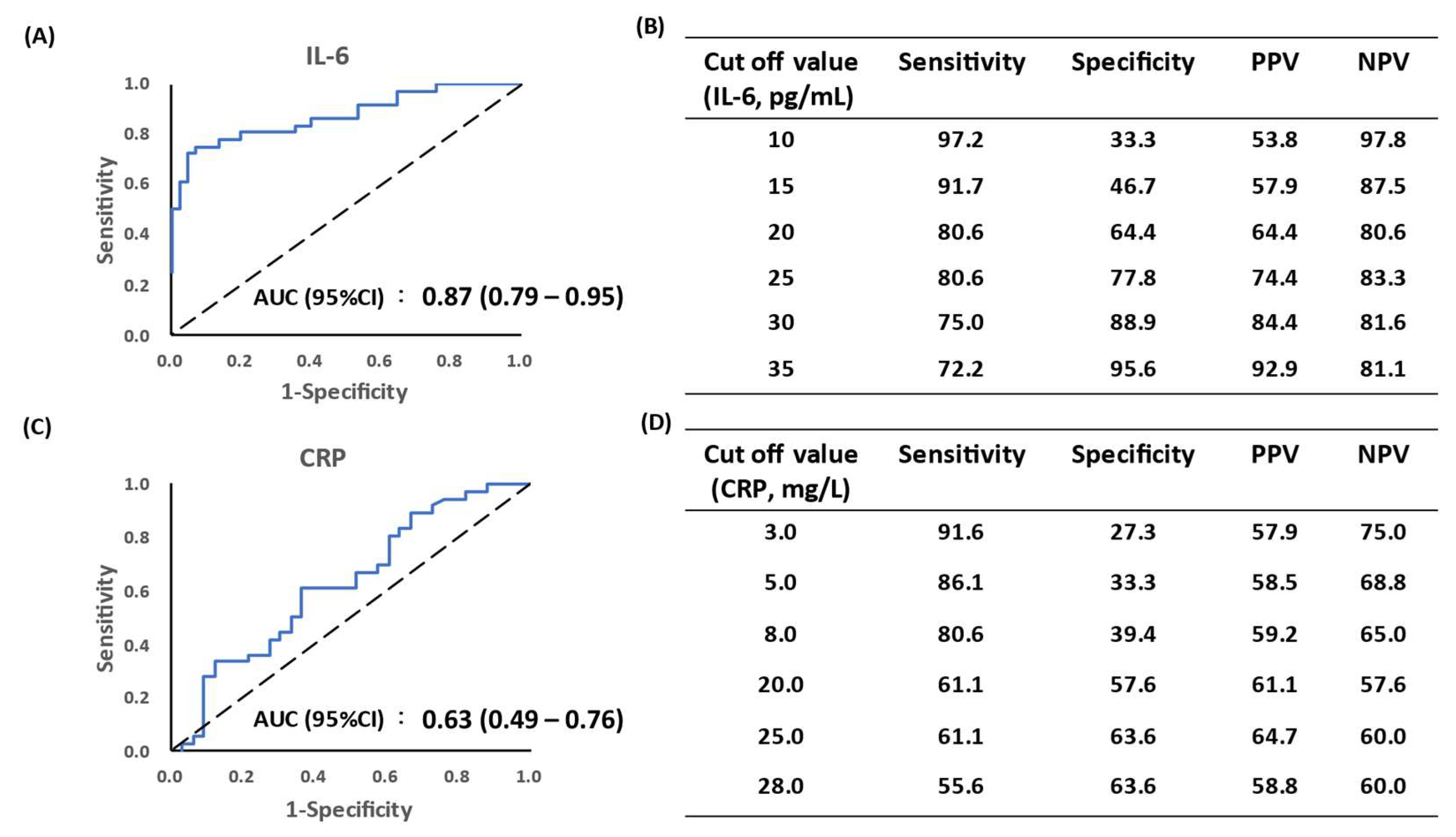
3.2. Tissue IL-6 Is a Superior Prognostic Marker to Predict Wound Infection Status
3.3. Predictive Role of IL-6 in Local Wound Status
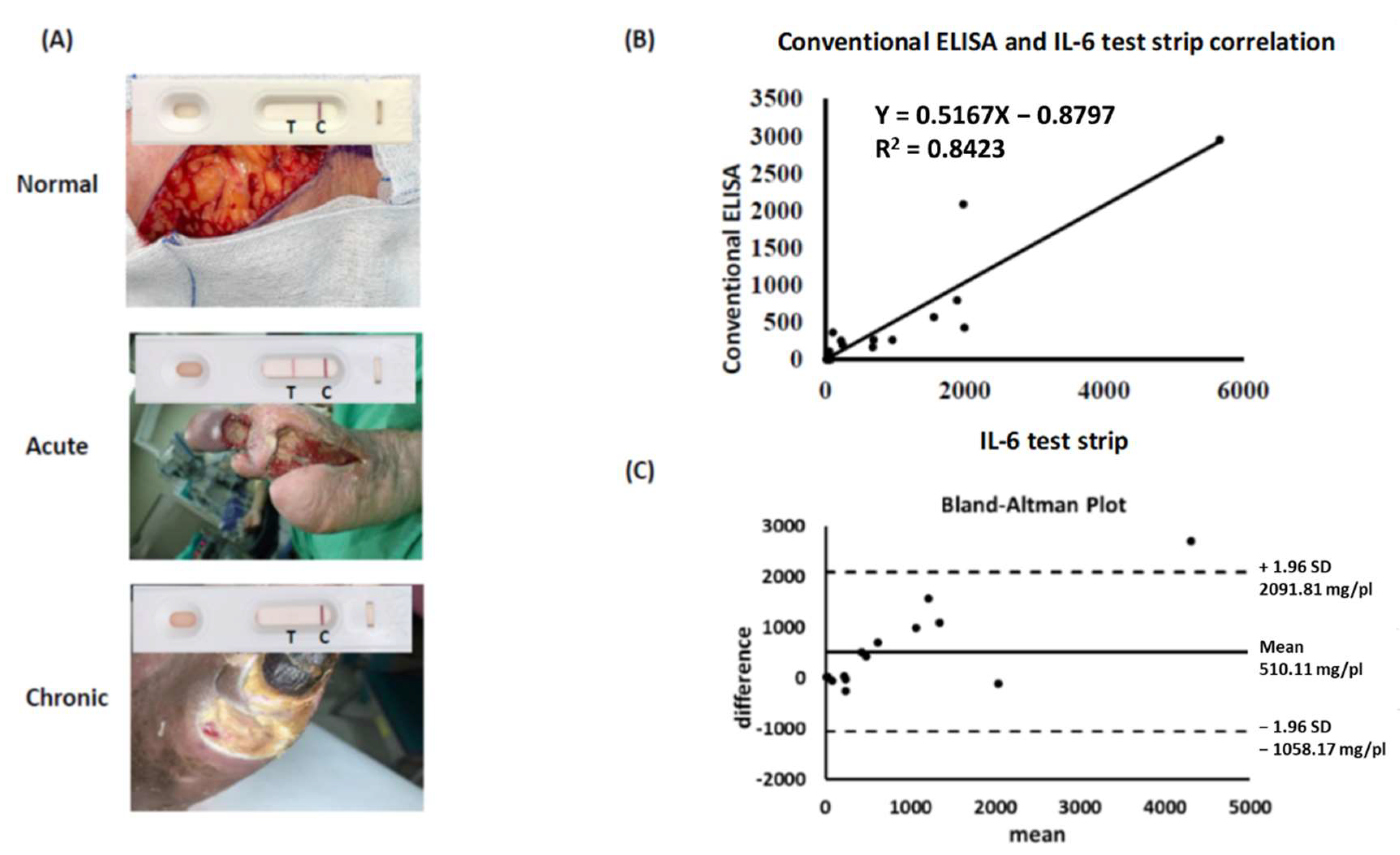
3.4. IL-6 Test Strip Provides a Reliable and Convenient Tool for Identification of IL-6
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hess, C.T. Checklist for factors affecting wound healing. Adv. Skin Wound Care 2011, 24, 192. [Google Scholar] [CrossRef] [PubMed]
- Saleh, K.; Strömdahl, A.-C.; Riesbeck, K.; Schmidtchen, A. Inflammation Biomarkers and Correlation to Wound Status after Full-Thickness Skin Grafting. Front. Med. 2019, 6, 159. [Google Scholar] [CrossRef] [PubMed]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef] [PubMed]
- Pope, J.E.; Choy, E.H. C-reactive protein and implications in rheumatoid arthritis and associated comorbidities. Semin. Arthritis Rheum 2021, 51, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Laino, A.S.; Woods, D.; Vassallo, M.; Qian, X.; Tang, H.; Wind-Rotolo, M.; Weber, J. Serum interleukin-6 and C-reactive protein are associated with survival in melanoma patients receiving immune checkpoint inhibition. J. Immunother. Cancer 2020, 8, e000842. [Google Scholar] [CrossRef]
- Lagrand, W.K.; Visser, C.A.; Hermens, W.T.; Niessen, H.W.; Verheugt, F.W.; Wolbink, G.J.; Hack, C.E. C-reactive protein as a cardiovascular risk factor: More than an epiphenomenon? Circulation 1999, 100, 96–102. [Google Scholar] [CrossRef] [Green Version]
- Trengove, N.J.; Bielefeldt-Ohmann, H.; Stacey, M.C. Mitogenic activity and cytokine levels in non-healing and healing chronic leg ulcers. Wound Repair Regen. 2001, 8, 13–25. [Google Scholar] [CrossRef]
- Del Giudice, M.; Gangestad, S.W. Rethinking IL-6 and CRP: Why they are more than inflammatory biomarkers, and why it matters. Brain Behav. Immun. 2018, 70, 61–75. [Google Scholar] [CrossRef]
- Krzyszczyk, P.; Schloss, R.; Palmer, A.; Berthiaume, F. The Role of Macrophages in Acute and Chronic Wound Healing and Interventions to Promote Pro-wound Healing Phenotypes. Front. Physiol. 2018, 9, 419. [Google Scholar] [CrossRef]
- Nagaraja, S.; Wallqvist, A.; Reifman, J.; Mitrophanov, A.Y. Computational Approach to Characterize Causative Factors and Molecular Indicators of Chronic Wound Inflammation. J. Immunol. 2014, 192, 1824–1834. [Google Scholar] [CrossRef] [Green Version]
- Hirano, T. IL-6 in inflammation, autoimmunity and cancer. Int. Immunol. 2021, 33, 127–148. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Pan, S.-C.; Cheng, C.-M. Paper-based human neutrophil elastase detection device for clinical wound monitoring. Lab Chip 2020, 20, 2709–2716. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.W.; Shen, C.F.; Liu, C.C.; Cheng, C.M. A Paper-Based IL-6 Test Strip Coupled with a Spectrum-Based Optical Reader for Differentiating Influenza Severity in Children. Front. Bioeng. Biotechnol. 2021, 9, 752681. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Lin, S.W.; Wang, I.J.; Yang, C.Y.; Hong, C.; Sun, J.R.; Feng, P.H.; Lee, M.H.; Shen, C.F.; Lee, Y.T. Interleukin-6 Test Strip Combined with a Spectrum-Based Optical Reader for Early Recognition of COVID-19 Patients with Risk of Respiratory Failure. Front. Bioeng. Biotechnol. 2022, 10, 796996. [Google Scholar] [CrossRef]
- Johnson, B.Z.; Stevenson, A.W.; Prêle, C.M.; Fear, M.W.; Wood, F.M. The Role of IL-6 in Skin Fibrosis and Cutaneous Wound Healing. Biomedicines 2020, 8, 101. [Google Scholar] [CrossRef]
- Landry, A.; Docherty, P.; Ouellette, S.; Cartier, L.J. Causes and outcomes of markedly elevated C-reactive protein levels. Can. Fam. Physician 2017, 63, e316–e323. [Google Scholar]
- Blomgren, L.; Johansson, G.; Siegbahn, A.; Bergqvist, D. Coagulation and fibrinolysis in chronic venous insufficiency. Vasa 2001, 30, 184–187. [Google Scholar] [CrossRef]
- Trengove, N.J.; Langton, S.R.; Stacey, M.C. Biochemical analysis of wound fluid from nonhealing and healing chronic leg ulcers. Wound Repair Regen. 1996, 4, 234–239. [Google Scholar] [CrossRef]
- Fahey, T.J., 3rd; Sadaty, A.; Jones, W.G., 2nd; Barber, A.; Smoller, B.; Shires, G.T. Diabetes impairs the late inflammatory response to wound healing. J. Surg Res. 1991, 50, 308–313. [Google Scholar] [CrossRef]
- Cruz, A.S.; Mendes-Frias, A.; Oliveira, A.I.; Dias, L.; Matos, A.R.; Carvalho, A.; Capela, C.; Pedrosa, J.; Gil Castro, A.; Silvestre, R. Interleukin-6 Is a Biomarker for the Development of Fatal Severe Acute Respiratory Syndrome Coronavirus 2 Pneumonia. Front. Immunol. 2021, 12, 613422. [Google Scholar] [CrossRef]
- Yeh, F.; Lin, W.; Shen, H.; Fang, R. Changes in circulating levels of interleukin 6 in burned patients. Burns 1999, 25, 131–136. [Google Scholar] [CrossRef]
- Gille, J.; Jocovic, J.; Kremer, T.; Sablotzki, A. The predictive role of Interleukin 6 in burn patients with positive blood cultures. Int. J. Burn. Trauma 2021, 11, 123–130. [Google Scholar]
- Meloni, M.; Izzo, V.; Giurato, L.; Brocco, E.; Ferrannini, M.; Gandini, R.; Uccioli, L. Procalcitonin Is a Prognostic Marker of Hospital Outcomes in Patients with Critical Limb Ischemia and Diabetic Foot Infection. J. Diabetes Res. 2019, 2019, 4312737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christ-Crain, M.; Müller, B. Procalcitonin in bacterial infections--hype, hope, more or less? Swiss Med Wkly. 2005, 135, 451–460. [Google Scholar]
- Becker, K.L.; Snider, R.; Nylen, E.S. Procalcitonin assay in systemic inflammation, infection, and sepsis: Clinical utility and limitations. Crit. Care Med. 2008, 36, 941–952. [Google Scholar] [CrossRef]
- Jonaidi Jafari, N.; Safaee Firouzabadi, M.; Izadi, M.; Safaee Firouzabadi, M.S.; Saburi, A. Can procalcitonin be an accurate diagnostic marker for the classification of diabetic foot ulcers? Int. J. Endocrinol. Metab. 2014, 12, e13376. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Acute | Chronic | Normal | |
|---|---|---|---|
| Case No. | 31 | 32 | 19 |
| Infection (No.) | 22 | 15 | 0 |
| Non-infection (No.) | 9 | 17 | 19 |
| Age (y/o, mean ± SD) | 62.8 ± 9.5 | 64.3 ± 8.9 | 50.3 ± 11.8 |
| CRP (mg/L, mean ± SD) | 51.28 ± 77.79 (IQR: 6.9–61.1) | 59.14 ± 63.44 (IQR: 11.7–93) | 74 ± 136.87 (IQR: 0.8–106.65) |
| IL-6 (pg/mL, mean ± SD) | 522.33 ± 1142.77 (IQR: 19.1–308.88) | 51.95 ± 123.47 (IQR: 12.5–36.44) | 18.46 ± 14.76 (IQR: 3.49–25.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, S.-C.; Wu, Y.-F.; Lin, Y.-C.; Lin, S.-W.; Cheng, C.-M. Paper-Based Interleukin-6 Test Strip for Early Detection of Wound Infection. Biomedicines 2022, 10, 1585. https://doi.org/10.3390/biomedicines10071585
Pan S-C, Wu Y-F, Lin Y-C, Lin S-W, Cheng C-M. Paper-Based Interleukin-6 Test Strip for Early Detection of Wound Infection. Biomedicines. 2022; 10(7):1585. https://doi.org/10.3390/biomedicines10071585
Chicago/Turabian StylePan, Shin-Chen, Yu-Feng Wu, Yu-Chen Lin, Sheng-Wen Lin, and Chao-Min Cheng. 2022. "Paper-Based Interleukin-6 Test Strip for Early Detection of Wound Infection" Biomedicines 10, no. 7: 1585. https://doi.org/10.3390/biomedicines10071585
APA StylePan, S. -C., Wu, Y. -F., Lin, Y. -C., Lin, S. -W., & Cheng, C. -M. (2022). Paper-Based Interleukin-6 Test Strip for Early Detection of Wound Infection. Biomedicines, 10(7), 1585. https://doi.org/10.3390/biomedicines10071585