
A Review on Music Interventions for Frontotemporal Aphasia and a Proposal for Alternative Treatments




Abstract
:1. Introduction
2. Materials and Methods
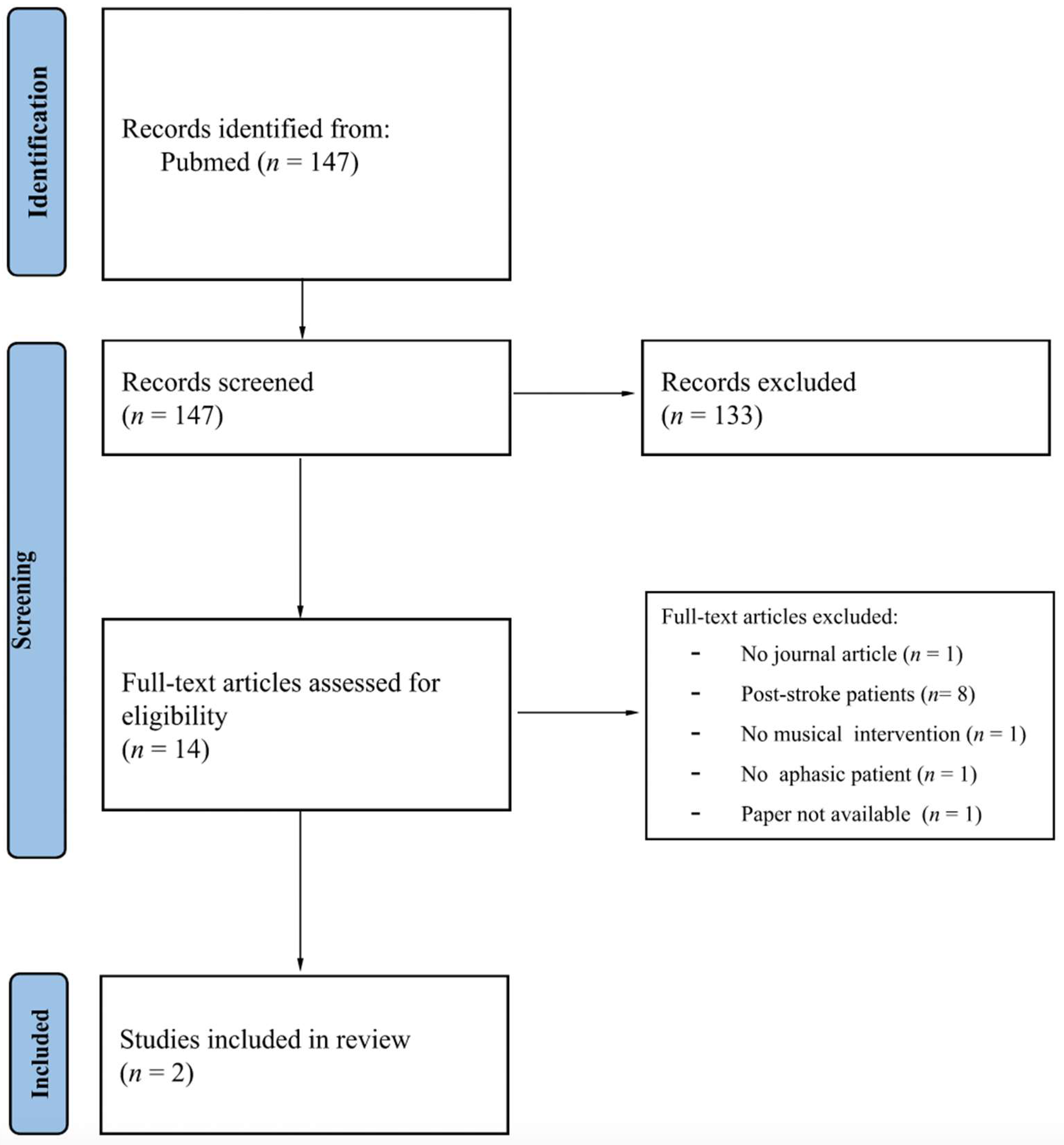
2.1. Literature Search and Study Eligibility
2.2. Data Extraction
3. Results
3.1. Study Characteristics
3.1.1. Sociodemographic Variables
3.1.2. Assessment and Treatments
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benussi, A.; Padovani, A.; Borroni, B. Phenotypic heterogeneity of monogenic frontotemporal dementia. Front. Aging Neurosci. 2015, 7, 171. [Google Scholar] [CrossRef] [PubMed]
- Rohrer, J.D.; Lashley, T.; Schott, J.M.; Warren, J.E.; Mead, S.; Isaacs, A.M.; Beck, J.; Hardy, J.; de Silva, R.; Warrington, E.; et al. Clinical and neuroanatomical signatures of tissue pathology in frontotemporal lobar degeneration. Brain 2011, 13, 2565–2581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borroni, B.; Graff, C.; Hardiman, O.; Ludolph, A.C.; Moreno, F.; Otto, M.; Piccininni, M.; Remes, A.M.; Rowe, J.B.; Seelaar, H.; et al. FRONTotemporal dementia Incidence European Research Study—FRONTIERS: Rationale and design. Alzheimer’s Dement. 2022, 18, 498–506. [Google Scholar] [CrossRef]
- Younes, K.; Miller, B.L. Frontotemporal dementia: Neuropathology, genetics, neuroimaging, and treatments. Psychiatr. Clin. 2020, 43, 331–344. [Google Scholar]
- Logroscino, G.; Piccininni, M.; Binetti, G.; Zecca, C.; Turrone, R.; Capozzo, R.; Tortelli, R.; Battista, P.; Bagoj, E.; Barone, R.; et al. Incidence of frontotemporal lobar degeneration in Italy: The Salento-Brescia Registry study. Neurology 2019, 92, e2355–e2363. [Google Scholar] [CrossRef]
- Laforce, R., Jr. Behavioral and language variants of frontotemporal dementia: A review of key symptoms. Clin. Neurol. Neurosurg. 2013, 115, 2405–2410. [Google Scholar] [CrossRef]
- Mesulam, M.-M.; Rogalski, E.J.; Wieneke, C.; Hurley, R.S.; Geula, C.; Bigio, E.H.; Thompson, C.K.; Weintraub, S. Primary progressive aphasia and the evolving neurology of the language network. Nat. Rev. Neurol. 2014, 10, 554–569. [Google Scholar] [CrossRef] [Green Version]
- Mesulam, M.M. Primary progressive aphasia. Ann. Neurol. 2001, 49, 425–432. [Google Scholar] [CrossRef]
- Pick, A. Beiträge zur Lehre von den Störungen der Sprache. Arch. Psychiatr. Nervenkrankh. 1892, 23, 896–918. [Google Scholar] [CrossRef]
- Sérieux, P. Sur un cas de surdite verbale pure. Rev. Med. 1893, 13, 733–750. [Google Scholar]
- Mesulam, M.M. Slowly progressive aphasia without generalized dementia. Ann. Neurol. 1982, 11, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Mesulam, M.M. Primary progressive aphasia—A language-based dementia. N. Engl. J. Med. 2003, 349, 1535–1542. [Google Scholar] [CrossRef] [PubMed]
- Gorno-Tempini, L.M.; Hillis, E.A.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volkmer, A.; Cartwright, J.; Ruggero, L.; Beales, A.; Gallée, J.; Grasso, S.; Henry, M.; Jokel, R.; Kindell, J.; Khayum, R.; et al. Principles and philosophies for speech and language therapists working with people with primary progressive aphasia: An international expert consensus. Disabil. Rehabil. 2022. [Google Scholar] [CrossRef] [PubMed]
- Carthery-Goulart, M.T.; Silveira, A.D.C.D.; Machado, T.H.; Mansur, L.L.; Parente, M.A.D.M.P.; Senaha, M.L.H.; Brucki, S.M.D.; Nitrini, R. Nonpharmacological interventions for cognitive impairments following primary progressive aphasia: A systematic review of the literature. Dement. Neuropsychol. 2013, 7, 122–131. [Google Scholar] [CrossRef] [Green Version]
- Henry, M.L.; Hubbard, H.I.; Grasso, S.M.; Mandelli, M.L.; Wilson, S.M.; Sathishkumar, M.T.; Fridriksson, J.; Daigle, W.; Boxer, A.L.; Miller, B.L.; et al. Retraining speech production and fluency in non-fluent/agrammatic primary progressive aphasia. Brain 2018, 141, 1799–1814. [Google Scholar] [CrossRef] [Green Version]
- Jokel, R.; Graham, N.L.; Rochon, E.; Leonard, C. Word retrieval therapies in primary progressive aphasia. Aphasiology 2014, 28, 1038–1068. [Google Scholar] [CrossRef]
- Coemans, S.; Struys, E.; Vandenborre, D.; Wilssens, I.; Engelborghs, S.; Paquier, P.; Tsapkini, K.; Keulen, S. A Systematic Review of Transcranial Direct Current Stimulation in Primary Progressive Aphasia: Methodological Considerations. Front. Aging 2021, 13, 710818. [Google Scholar] [CrossRef]
- Nissim, N.R.; Moberg, P.J.; Hamilton, R.H. Efficacy of noninvasive brain stimulation (tDCS or TMS) paired with language therapy in the treatment of primary progressive aphasia: An exploratory meta-analysis. Brain Sci. 2020, 10, 597. [Google Scholar] [CrossRef]
- Thaut, M.H.; Rice, R.R.; Braun Janzen, T.; Hurt-Thaut, C.P.; McIntosh, G.C. Rhythmic auditory stimulation for reduction of falls in Parkinson’s disease: A randomized controlled study. Clin. Rehabil. 2019, 33, 34–43. [Google Scholar] [CrossRef]
- Sihvonen, A.J.; Leo, V.; Ripollés, P.; Lehtovaara, T.; Ylönen, A.; Rajanaro, P.; Laitinen, S.; Forsblom, A.; Saunavaara, J.; Autti, T.; et al. Vocal music enhances memory and language recovery after stroke: Pooled results from two RCTs. Ann. Clin. Transl. Neurol. 2020, 7, 2272–2287. [Google Scholar] [CrossRef] [PubMed]
- Särkämö, T.; Tervaniemi, M.; Laitinen, S.; Forsblom, A.; Soinila, S.; Mikkonen, M.; Autti, T.; Silvennoinen, H.M.; Erkkilä, J.; Laine, M.; et al. Music listening enhances cognitive recovery and mood after middle cerebral artery stroke. Brain 2008, 131, 866–876. [Google Scholar] [CrossRef] [PubMed]
- Schlaug, G.; Marchina, S.; Norton, A. From singing to speaking: Why singing may lead to recovery of expressive language function in patients with Broca’s aphasia. Music. Percept. 2008, 25, 315–323. [Google Scholar] [CrossRef] [Green Version]
- Särkämö, T.; Tervaniemi, M.; Laitinen, S.; Numminen, A.; Kurki, M.; Johnson, J.K.; Rantanen, P. Cognitive, emotional, and social benefits of regular musical activities in early dementia: Randomized controlled study. Gerontologist 2014, 54, 634–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leggieri, M.; Thaut, M.H.; Fornazzari, L.; Schweizer, T.A.; Barfett, J.; Munoz, D.G.; Fischer, C.E. Music intervention approaches for Alzheimer’s disease: A review of the literature. Front. Neurosci. 2019, 13, 132. [Google Scholar] [CrossRef] [Green Version]
- Van der Steen, J.T.; Smaling, H.J.; Van der Wouden, J.C.; Bruinsma, M.S.; Scholten, R.J.; Vink, A.C. Music-based therapeutic interventions for people with dementia. Cochrane Database Syst. Rev. 2018, 7, CD003477. [Google Scholar] [CrossRef] [Green Version]
- Sihvonen, A.J.; Särkämö, T.; Leo, V.; Tervaniemi, M.; Altenmüller, E.; Soinila, S. Music-based interventions in neurological rehabilitation. Lancet Neurol. 2017, 16, 648–660. [Google Scholar] [CrossRef] [Green Version]
- Thaut, M.H.; McIntosh, G.C.; Hoemberg, V. Neurobiological foundations of neurologic music therapy: Rhythmic entrainment and the motor system. Front. Psychol. 2015, 5, 1185. [Google Scholar] [CrossRef] [Green Version]
- Särkämö, T.; Soto, D. Music listening after stroke: Beneficial effects and potential neural mechanisms. Ann. N. Y. Acad. Sci. 2012, 1252, 266–281. [Google Scholar] [CrossRef]
- Thaut, M.H. The future of music in therapy and medicine. Ann. N. Y. Acad. Sci. 2005, 1060, 303–308. [Google Scholar] [CrossRef]
- Norton, A.; Zipse, L.; Marchina, S.; Schlaug, G. Melodic intonation therapy: Shared insights on how it is done and why it might help. Ann. N. Y. Acad. Sci. 2009, 1169, 431–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sparks, R.; Helm, N.; Albert, M. Aphasia rehabilitation resulting from melodic intonation therapy. Cortex 1974, 10, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.L.; Sparks, R.W.; Helm, N.A. Melodic intonation therapy for aphasia. Arch. Neurol. 1973, 29, 130–131. [Google Scholar] [CrossRef] [PubMed]
- Merrett, D.L.; Peretz, I.; Wilson, S.J. Neurobiological, cognitive, and emotional mechanisms in melodic intonation therapy. Front. Hum. Neurosci. 2014, 8, 401. [Google Scholar] [CrossRef] [Green Version]
- García-Casares, N.; Barros-Cano, A.; García-Arnés, J.A. Melodic Intonation Therapy in Post-Stroke Non-Fluent Aphasia and Its Effects on Brain Plasticity. J. Clin. Med. 2022, 11, 3503. [Google Scholar] [CrossRef]
- Haro-Martínez, A.; Pérez-Araujo, C.M.; Sanchez-Caro, J.M.; Fuentes, B.; Díez-Tejedor, E. Melodic intonation therapy for post-stroke non-fluent aphasia: Systematic review and meta-analysis. Front. Neurol. 2021, 12, 700115. [Google Scholar] [CrossRef]
- Zumbansen, A.; Peretz, I.; Hébert, S. Melodic intonation therapy: Back to basics for future research. Front. Neurol. 2014, 5, 7. [Google Scholar] [CrossRef] [Green Version]
- Ogar, J.; Slama, H.; Dronkers, N.; Amici, S.; Luisa Gorno-Tempini, M. Apraxia of speech: An overview. Neurocase 2005, 11, 427–432. [Google Scholar] [CrossRef]
- Ballard, K.J.; Granier, J.P.; Robin, D.A. Understanding the nature of apraxia of speech: Theory, analysis, and treatment. Aphasiology 2000, 14, 969–995. [Google Scholar] [CrossRef]
- McNeil, M.R.; Robin, D.A.; Schmidt, R.A. Apraxia of speech: Definition, differentiation, and treatment. Clin. Manag. Sens. Speech Disord. 1997, 311–344. [Google Scholar]
- Cortese, M.D.; Riganello, F.; Arcuri, F.; Pignataro, L.M.; Buglione, I. Rehabilitation of aphasia: Application of melodic-rhythmic therapy to Italian language. Front. Hum. Neurosci. 2015, 9, 520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.D. Language, music, syntax and the brain. Nat. Neurosci. 2003, 6, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Altenmüller, E.; Schlaug, G. Neurologic music therapy: The beneficial effects of music making on neurorehabilitation. Acoust. Sci. Technol. 2013, 34, 5–12. [Google Scholar] [CrossRef]
- Brancatisano, O.; Baird, A.; Thompson, W.F. Why is music therapeutic for neurological disorders? The Therapeutic Music Capacities Model. Neurosci. Biobehav. Rev. 2020, 112, 600–615. [Google Scholar] [CrossRef]
- Kumfor, F.; Sapey-Triomphe, L.A.; Leyton, C.E.; Burrell, J.R.; Hodges, J.R.; Piguet, O. Degradation of emotion processing ability in corticobasal syndrome and Alzheimer’s disease. Brain 2014, 137, 3061–3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Stock, J.; Peretz, I.; Grezes, J.; de Gelder, B. Instrumental music influences recognition of emotional body language. Brain Topogr. 2009, 21, 216–220. [Google Scholar] [CrossRef] [Green Version]
- Anderson, A.J.; Lin, F. How pattern information analyses of semantic brain activity elicited in language comprehension could contribute to the early identification of Alzheimer’s disease. NeuroImage Clin. 2019, 22, 101788. [Google Scholar] [CrossRef]
- Szatloczki, G.; Hoffmann, I.; Vincze, V.; Kalman, J.; Pakaski, M. Speaking in Alzheimer’s disease, is that an early sign? Importance of changes in language abilities in Alzheimer’s disease. Front. Aging Neurosci. 2015, 7, 195. [Google Scholar] [CrossRef] [Green Version]
- Verma, M.; Howard, R.J. Semantic memory and language dysfunction in early Alzheimer’s disease: A review. Int. J. Geriatr. Psychiatry 2012, 27, 1209–1217. [Google Scholar] [CrossRef]
- Nelissen, N.; Vandenbulcke, M.; Fannes, K.; Verbruggen, A.; Peeters, R.; Dupont, P.; Laere, K.V.; Bormans, G.; Vandenberghe, R. Aβ amyloid deposition in the language system and how the brain responds. Brain 2007, 130, 2055–2069. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Casares, N.; Moreno-Leiva, R.M.; Garcia-Arnes, J.A. Music therapy as a non-pharmacological treatment in Alzheimer’s disease. A systematic review. Rev. Neurol. 2017, 65, 529–538. [Google Scholar]
- Ridder, H.M.; Wigram, T.; Ottesen, A.M. A pilot study on the effects of music therapy on frontotemporal dementia–developing a research protocol. Nord. J. Music. Ther. 2009, 18, 103–132. [Google Scholar] [CrossRef]
- Ridder, H.M.; Aldridge, D. Individual music therapy with persons with frontotemporal dementia: Singing dialogue. Nord. J. Music Ther. 2005, 14, 91–106. [Google Scholar] [CrossRef]
- Grube, M.; Bruffaerts, R.; Schaeverbeke, J.; Neyens, V.; De Weer, A.S.; Seghers, A.; Bergmans, B.; Dries, E.; Griffiths, D.; Vandenberghe, R. Core auditory processing deficits in primary progressive aphasia. Brain 2016, 139, 1817–1829. [Google Scholar] [CrossRef] [PubMed]
- Rohrer, J.D.; Sauter, D.; Scott, S.; Rossor, M.N.; Warren, J.D. Receptive prosody in nonfluent primary progressive aphasias. Cortex 2012, 48, 308–316. [Google Scholar] [CrossRef] [Green Version]
- Maruta, C.; Makhmood, S.; Downey, L.E.; Golden, H.L.; Fletcher, P.D.; Witoonpanich, P.; Rohrer, J.D.; Warren, J.D. Delayed auditory feedback simulates features of nonfluent primary progressive aphasia. J. Neurol. Sci. 2014, 347, 345–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goll, J.C.; Crutch, S.J.; Loo, J.H.; Rohrer, J.D.; Frost, C.; Bamiou, D.E.; Warren, J.D. Non-verbal sound processing in the primary progressive aphasias. Brain 2010, 133, 272–285. [Google Scholar] [CrossRef]
- Sihvonen, A.J.; Särkämö, T. Clinical and Neural Predictors of Treatment Response to Music Listening Intervention after Stroke. Brain Sci. 2021, 11, 1576. [Google Scholar] [CrossRef]
- Haro-Martínez, A.M.; Lubrini, G.; Madero-Jarabo, R.; Díez-Tejedor, E.; Fuentes, B. Melodic intonation therapy in post-stroke nonfluent aphasia: A randomized pilot trial. Clin. Rehabil. 2019, 33, 44–53. [Google Scholar] [CrossRef]
- Raglio, A.; Oasi, O.; Gianotti, M.; Rossi, A.; Goulene, K.; Stramba-Badiale, M. Improvement of spontaneous language in stroke patients with chronic aphasia treated with music therapy: A randomized controlled trial. Int. J. Neurosci. 2016, 126, 235–242. [Google Scholar] [CrossRef]
- Van Der Meulen, I.; De Sandt-Koenderman, V.; Mieke, W.M.E.; Heijenbrok, M.H.; Visch-Brink, E.; Ribbers, G.M. Melodic intonation therapy in chronic aphasia: Evidence from a pilot randomized controlled trial. Front. Hum. Neurosci. 2016, 10, 533. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Elie, A.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Stahl, B.; Kotz, S.A. Facing the music: Three issues in current research on singing and aphasia. Front. Psychol. 2014, 5, 1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jungblut, M.; Mais, C.; Binkofski, F.C.; Schüppen, A. The efficacy of a directed rhythmic-melodic voice training in the treatment of chronic non-fluent aphasia—Behavioral and imaging results. J. Neurol. 2022, 269, 5070–5084. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.; Saxena, S.; Sheppard, S.M.; Hillis, A.E. Selective impairments in components of affective prosody in neurologically impaired individuals. Brain Cogn. 2018, 124, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Brotons, M.; Koger, S.M. The impact of music therapy on language functioning in dementia. J. Music Ther. 2000, 37, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Liechty, J.A. On the Tip of My Tongue: Living with aphasia. J. Christ. Nurs. 2006, 23, 32–33. [Google Scholar] [CrossRef]
- Jungblut, M.; Huber, W.; Mais, C.; Schnitker, R. Paving the way for speech: Voice-training-induced plasticity in chronic aphasia and apraxia of speech—Three single cases. Neural Plast. 2014, 2014, 841982. [Google Scholar] [CrossRef] [Green Version]
- Tomaino, C.M. Effective music therapy techniques in the treatment of nonfluent aphasia. Ann. N. Y. Acad. Sci. 2012, 1252, 312–317. [Google Scholar] [CrossRef]
- Wambaugh, J.L.; Nessler, C.; Cameron, R.; Mauszycki, S.C. Acquired apraxia of speech: The effects of repeated practice and rate/rhythm control treatments on sound production accuracy. Am. J. Speech-Lang. Pathol. 2012, 21, S5. [Google Scholar] [CrossRef]
- Stahl, B.; Kotz, S.A.; Henseler, I.; Turner, R.; Geyer, S. Rhythm in disguise: Why singing may not hold the key to recovery from aphasia. Brain 2011, 134, 3083–3093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breier, J.I.; Randle, S.; Maher, L.M.; Papanicolaou, A.C. Changes in maps of language activity activation following melodic intonation therapy using magnetoencephalography: Two case studies. J. Clin. Exp. Neuropsychol. 2010, 32, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Tomaino, C.M. Protocol evaluation for effective music therapy for persons with nonfluent aphasia. Top. Stroke Rehabil. 2008, 15, 555–569. [Google Scholar] [CrossRef] [PubMed]
- Belin, P.; Eeckhout, P.V.; Zilbovicius, M.; Remy, P.; Francois, C.; Guillaume, S.; Chain, F.; Rancurel, G.; Samson, Y. Recovery from nonfluent aphasia after melodic intonation therapy: A PET study. Neurology 1996, 47, 1504–1511. [Google Scholar] [CrossRef]
- Beber, B.C.; Berbert, M.C.B.; Grawer, R.S.; Cardoso, M.C.D.A.F. Rate and rhythm control strategies for apraxia of speech in nonfluent primary progressive aphasia. Dement. Neuropsychol. 2018, 12, 80–84. [Google Scholar] [CrossRef]
- Raglio, A.; Bellandi, D.; Baiardi, P.; Gianotti, M.; Ubezio, M.C.; Granieri, E. Music therapy in frontal temporal dementia: A case report. J. Am. Geriatr. Soc. 2012, 60, 1578–1579. [Google Scholar] [CrossRef]
- Volkmer, A.; Rogalski, E.; Henry, M.; Taylor-Rubin, C.; Ruggero, L.; Khayum, R.; Kindell, J.; Gorno-Tempini, M.L.; Warren, J.D.; Rohrer, J.D. Speech and language therapy approaches to managing primary progressive aphasia. Pract. Neurol. 2020, 20, 154–161. [Google Scholar] [CrossRef]
- Montagut, N.; Borrego-Écija, S.; Castellví, M.; Rico, I.; Reñé, R.; Balasa, M.; Lladó, A.; Sánchez-Valle, R. Errorless learning therapy in semantic variant of primary progressive aphasia. J. Alzheimer’s Dis. 2021, 79, 415–422. [Google Scholar] [CrossRef]
- Krajenbrink, T.; Croot, K.; Taylor-Rubin, C.; Nickels, L. Treatment for spoken and written word retrieval in the semantic variant of primary progressive aphasia. Neuropsychol. Rehabil. 2018, 30, 915–947. [Google Scholar] [CrossRef]
- Fried-Oken, M.; Rowland, C.; Gibbons, C. Providing augmentative and alternative communication treatment to persons with progressive nonfluent aphasia. Perspect. Neurophysiol. Neurogenic Speech Lang. Disord. 2010, 20, 21–25. [Google Scholar] [CrossRef]
- Hausen, M.; Torppa, R.; Salmela, V.R.; Vainio, M.; Särkämö, T. Music and speech prosody: A common rhythm. Front. Psychol. 2013, 4, 566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boccalini, C.; Carli, G.; Tondo, G.; Polito, C.; Catricalà, E.; Berti, V.; Bessi, V.; Sorbi, S.; Iannaccone, S.; Esposito, V.; et al. Brain metabolic connectivity reconfiguration in the semantic variant of primary progressive aphasia. Cortex 2022, 154, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Neri, F.; Romanella, S.M.; Pitinca, M.L.T.; Taddei, S.; Monti, L.; Benocci, S.; Santarnecchi, E.; Cappa, S.F.; Rossi, S. rTMS-induced language improvement and brain connectivity changes in logopenic/phonological variant of Primary progressive Aphasia. Clin. Neurophysiol. 2021, 132, 2481–2484. [Google Scholar] [CrossRef] [PubMed]
- Battista, P.; Capozzo, R.; Rizzo, G.; Zecca, C.; Anastasia, A.; De Blasi, R.; Logroscino, G. Early pathological gambling in co-occurrence with semantic variant primary progressive aphasia: A case report. Clin. Interv. Aging 2019, 14, 727. [Google Scholar] [CrossRef]
- Battista, P.; Catricalà, E.; Piccininni, M.; Copetti, M.; Esposito, V.; Polito, C.; Miozzo, A.; Gobbi, E.; Cuoco, S.; Boschi, V.; et al. Screening for aphasia in neurodegeneration for the diagnosis of patients with primary progressive aphasia: Clinical validity and psychometric properties. Dement. Geriatr. Cogn. Disord. 2018, 46, 243–252. [Google Scholar] [CrossRef]
- Catricalà, E.; Gobbi, E.; Battista, P.; Miozzo, A.; Polito, C.; Boschi, V.; Esposito, V.; Cuoco, S.; Barone, P.; Sorbi, S.; et al. SAND: A Screening for Aphasia in NeuroDegeneration. Development and normative data. Neurol. Sci. 2017, 38, 1469–1483. [Google Scholar] [CrossRef]
- Iaccarino, L.; Crespi, C.; Della Rosa, P.A.; Catricala, E.; Guidi, L.; Marcone, A.; Tagliarvini, F.; Magnani, G.; Cappa, S.; Perani, D. The semantic variant of primary progressive aphasia: Clinical and neuroimaging evidence in single subjects. PLoS ONE 2015, 10, e0120197. [Google Scholar] [CrossRef] [Green Version]
- Cerami, C.; Marcone, A.; Galimberti, D.; Villa, C.; Fenoglio, C.; Scarpini, E.; Cappa, S.F. Novel missense progranulin gene mutation associated with the semantic variant of primary progressive aphasia. J. Alzheimer’s Dis. 2013, 36, 415–420. [Google Scholar] [CrossRef]
- Riello, R.; Frisoni, G.B. Music therapy in Alzheimer’s disease: Is an evidence-based approach possible? Recenti Progress. Med. 2001, 92, 317–321. [Google Scholar]
- Cicconetti, P.; Fionda, A.; Zannino, G.; Ettorre, E.; Marigliano, V. Rehabilitation in Alzheimer’s dementia. Recenti Progress. Med. 2000, 91, 450–454. [Google Scholar]
- Grossman, M.; Irwin, D.J. Primary progressive aphasia and stroke aphasia. Continuum 2018, 24, 745–767. [Google Scholar] [CrossRef] [PubMed]
- Canu, E.; Agosta, F.; Battistella, G.; Spinelli, E.G.; DeLeon, J.; Welch, A.E.; Mandelli, M.L.; Hubbard, H.I.; Moro, A.; Magnani, G.; et al. Speech production differences in English and Italian speakers with nonfluent variant PPA. Neurology 2020, 94, e1062–e1072. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No Journal Articles | Post-Stroke Patients | No Musical Intervention | No Aphasic Patient | Paper Not Available |
|---|---|---|---|---|
| Stahl et al., 2014 [63] | Jungblut et al., 2022 [64] | Wright et al., 2018 [65] | Brotons et al. [66] | Liechty, 2006 [67] |
| Jungblut et al., 2014 [68] | ||||
| Tomaino, 2012 [69] | ||||
| Wambaugh et al., 2012 [70] | ||||
| Stahl et al., 2011 [71] | ||||
| Breier et al., 2010 [72] | ||||
| Kim et al., 2008 [73] | ||||
| Belin et al., 1996 [74] |
| Study | Disease | Age | Intervention | Responsible | Duration (m) | Frequency (per Week) |
|---|---|---|---|---|---|---|
| Beber et al. (2018) [75] | non-fluent PPA | 72 | rhythm-based on apraxia of speech | speech therapist | 45 | once |
| Raglio et al. (2012) [76] | FTD with global aphasia | 58 | active music-therapy | music therapist | 30 | twice |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spinosa, V.; Vitulli, A.; Logroscino, G.; Brattico, E. A Review on Music Interventions for Frontotemporal Aphasia and a Proposal for Alternative Treatments. Biomedicines 2023, 11, 84. https://doi.org/10.3390/biomedicines11010084
Spinosa V, Vitulli A, Logroscino G, Brattico E. A Review on Music Interventions for Frontotemporal Aphasia and a Proposal for Alternative Treatments. Biomedicines. 2023; 11(1):84. https://doi.org/10.3390/biomedicines11010084
Chicago/Turabian StyleSpinosa, Vittoria, Alessandra Vitulli, Giancarlo Logroscino, and Elvira Brattico. 2023. "A Review on Music Interventions for Frontotemporal Aphasia and a Proposal for Alternative Treatments" Biomedicines 11, no. 1: 84. https://doi.org/10.3390/biomedicines11010084
APA StyleSpinosa, V., Vitulli, A., Logroscino, G., & Brattico, E. (2023). A Review on Music Interventions for Frontotemporal Aphasia and a Proposal for Alternative Treatments. Biomedicines, 11(1), 84. https://doi.org/10.3390/biomedicines11010084