


The Association between Vitamin D and the Components of Male Fertility: A Systematic Review




Abstract
:1. Introduction
2. Background
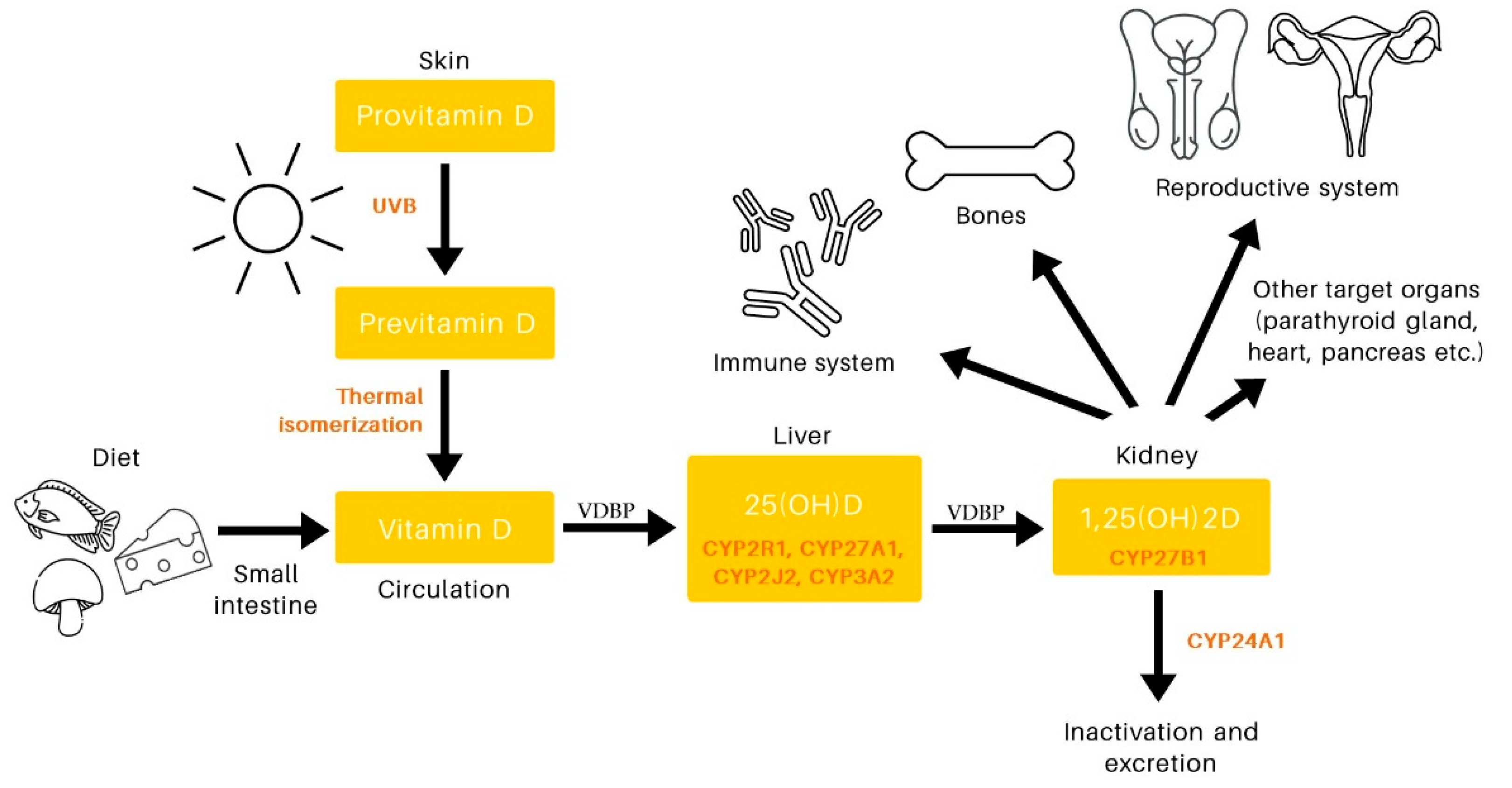
2.1. Vitamin D Physiology
2.2. Vitamin D in Male Reproductive System
3. Materials and Methods
4. Results
4.1. Vitamin D and Semen Parameters: Observational Studies
4.2. Vitamin D and Semen Prameters: Interventional Studies

{kind=link}
{kind=link}
| Study | Country | Study Design | Number of Patients | Age (Years) 1 | Characteristics of Patients | Vitamin D Measurement Method | Sperm Parameters | Adjustment | Level of Evidence |
|---|---|---|---|---|---|---|---|---|---|
| 2022 Güngör et al. [58] | Turkey | Cross-Sectional | 108 | F: 33.2 ± 4.1 I: 34.7 ± 4.0 | Fertile and infertile men | ECLIA | SC↑ TM↑ NM↑ DF↓ | Unadjusted | 3b |
| 2022 Holzer et al. [59] | Argentina | Cross-Sectional | 56 | 20–45 | Andrological patients | CLIA | SC→ TM↑ PM↑ NM→ | Unadjusted | 4 |
| 2022 Kamal et al. [67] | Egypt | Cross-Sectional | 100 | 35.0 ± 8.4 (20–50) | Andrological patients | ELISA | SC→ PM→ NM→ | Unadjusted | 4 |
| 2022 Rezayat et al. [60] | Iran | Cross-Sectional | 114 | F: 34.9 ± 13.5 I: 34.6 ± 12.2 (20–59) | Fertile and infertile men | ELISA | SC↑ TM↑ NM→ | Unadjusted | 3b |
| 2021 Ciccone et al. [57] | Brazil | Cross-Sectional | 260 | SA: 38.7 ± 8.5 NS: 38.0 ± 8.8 (18–60) | Men with semen abnormalities and normozoospermic men | ECLIA/HPLC | SC↑ TM↑ PM↑ NM↑ | Unadjusted | 3b |
| 2021 Hajianfar et al. [54] | Iran | Cross-Sectional | 350 | 34.8 ± 0.4 (20–50) | Andrological patients | ECLIA | SC↑ TM↑ NM↑ | Age, Educational Status, Smoking, Alcohol Consumption, Job, Varicocele, BMI, Total Energy Intake | 4 |
| 2021 Hussein et al. [55] | Egypt | Cross-Sectional | 100 | F: 31.4 ± 8.9 (19–58) I: 32.8 ± 6.9 (18–50) | Fertile and infertile men | ELFA | SC↑ PM↑ NM→ | Unadjusted | 3b |
| 2021 Kumari et al. [56] | India | Cross-Sectional | 224 | 18–45 | Men with semen abnormalities and normozoospermic men | CMIA | SC↑ TM↑ PM↑ NM↑ | Unadjusted | 3b |
| 2020 Derakhshan et al. [53] | Iran | Cross-Sectional | 70 | SVD: 33.7 ± 5.7 IVD: 36.3 ± 6.5 (18–60) | Andrological patients | HPLC | SC↑ TM↑ PM↑ NM↑ DF↓ | Unadjusted | 4 |
| 2020 Rudnicka et al. [66] | Spain | Cross-Sectional | 198 | 18–23 | Young men from general population | CLIA | SC→ TM→ NM→ | Age, BMI, Smoking, Physical activity, Season, Ejaculation Abstinence Time, Time to Start of Semen Analysis | 2b |
| 2019 Jueraitetibaike et al. [65] | China | Cross-Sectional | 222 | 30 | Andrological patients | ECLIA | SC→ TM→ PM→ NM→ | Unadjusted | 4 |
| 2018 Azizi et al. [51] | Iran | Cross-Sectional | 62 | NS: 34.1 ± 1.2 OAT: 33.0 ± 0.7 | Men with semen abnormalities and normozoospermic men | CLIA | SC→ TM↑ NM↑ DF→ | Unadjusted | 3b |
| 2018 Jóźków et al. [64] | Poland | Cross-Sectional | 177 | 24.6 ± 3.6 (20–35) | Young men from general population | ECLIA | SC→ PM→ | Smoking, Alcohol Consumption, Carrying a Telephone in a Pants Pockets, BMI, WHR, Caffeine Consumption, Physical Activity | 2b |
| 2018 Rehman et al. [52] | Pakistan | Cross-Sectional | 313 | 25–55 | Fertile and infertile men | Na | SC↑ TM↑ NM↑ | Vitamin D adjusted with BMI | 3b |
| 2017 Abbasihormozi et al. [49] | Iran | Cross-Sectional | 278 | 33.5 ± 4.8 (20–50) | Men with oligoasthenoteratozoospermia and normozoospermic men | ECLIA | SC→ TM↑ PM→ NM→ | Age, BMI, Season | 3b |
| 2017 Tirabassi et al. [50] | Italy | Cross-Sectional | 104 | 33.1 ± 4.8 | Andrological patients | CLIA | SC→ TM↑ PM↑ NM→ | Age, BMI, PTH, Varicocele | 4 |
| 2016 Blomberg Jensen et al. [48] | Denmark | Cross-Sectional | 1189 | 34.3 | Andrological patients | ID-LC-MS/MS | SC→ TM↑ PM↑ NM→ | Age, BMI, Smoking, Season, Abstinence, Time from Collection, Free Testosterone, Estradiol, Total Estradiol, Testosterone/Estradiol Ratio | 2b |
| 2016 Neville et al. [62] | Ireland | Cross-Sectional | 73 | 37.4 ± 4.4 | Men from couples undergoing IVF/ICSI | CPBA | SC→ TM→ PM→ NM→ | Unadjusted | 4 |
| 2016 Zhu et al. [63] | China | Case-Control | 265 | F: 28.22 ± 0.5 O: 28.8 ± 0.8 A: 28.3 ± 0.6 OA: 27.7 ± 0.6 AZ: 27.2 ± 0.6 NS: 28.4 ± 0.4 | Fertile and infertile men | ELISA | SC→ TM→ PM→ | Unadjusted | 3b |
| 2012 Hammound et al. [46] | USA | Cross-Sectional | 147 | 29.0 ± 8.5 (18–67) | General population | CLIA | SC↑ PM↑ NM→ | Age, BMI, Season, Alcohol Consumption, Smoking | 2b |
| 2012 Yang et al. [47] | China | Cross-Sectional | 559 | 20–40 | Fertile and infertile men | ELISA | TM↑ NM↑ | Season, Abstinence, Time from Collection | 3b |
| 2011 Blomber Jensen et al. [35] | Denmark | Cross-Sectional | 300 | 19.0 | General population | ID-LC-MS/MS | SC→ TM↑ PM↑ NM↑ | Abstinence, Season, Medication, Fever, Time from Ejaculation to Motility Assessment | 2b |
| 2011 Ramlau-Hansen et al. [61] | Denmark | Cross-Sectional | 307 | 18–21 | Young men from general population | ID-LC-MS/MS | SC→ TM→ NM→ | Season, History of Diseases of the Reproductive Organs, Smoking, Maternal Smoking During Pregnancy, Maternal Alcohol During Pregnancy, Abstinence, Spillage During Collection of The Sample | 2b |
| Study | Country | Study Design (Duration) | Vitamin D Dose | Number of Patients | Age (Years) 1 | Characteristics of Patients | Vitamin D Measurement Method | Sperm Parameters | Adjustment | Level of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|
| 2022 Padmapriya et al. [73] | India | DBRCT (3 months) | 28,000 IU of VD3 weekly | 120 | 30–40 | Men with oligoasthenoteratozoospermia | Na | SC↑ TM↑ PM↑ | Unadjusted | 1b |
| 2021 Bartl et al. [70] | Slovakia | Prospective interventional study (6 months) | 17,500 IU of VD3 weekly | 34 | 36.6 | Infertile men | HPLC | SC↑ PM↑ NM↑ | Unadjusted | 2b |
| 2021 Begum et al. [71] | Bangladesh | Prospective interventional study (3 months) | 40,000 IU of VD3 weekly for six weeks, 14,000 IU of VD3 weekly for another six weeks | 110 | 33.2 ± 5.8 (25–45) | Men with asthenozoospermia and vitamin D deficiency | CLIA | SC↑ TM↑ PM↑ | Unadjusted | 2b |
| 2021 Gheflati et al. [76] | Iran | DBRCT (3 months) | 50,000 IU of VD3 weekly for eight weeks and one maintenance dose of 50,000 IU for another four weeks | 44 | 18–45 | Men with asthenozoospermia | ELISA | SC→ PM→ NM→ | Unadjusted | 1b |
| 2021 Maghsoumi-Norouzabad et al. [72] | Iran | TBRCT (3 months) | 28,000 IU of VD3 weekly | 86 | VD: 35.1 ± 5.5 P: 34.4 ± 5.1 | Men with asthenozoospermia | ELISA | SC→ TM↑ PM↑ NM→ | Unadjusted | 1b |
| 2020 Amini et al. [75] | Iran | TBRCT (3 months) | 50,000 IU of VD3 weekly for eight weeks and one maintenance dose of 50,000 IU for another four weeks | 62 | 35–39 | Men with semen abnormalities | ELISA | SC→ TM→ PM→ NM→ | Unadjusted | 1b |
| 2020 Wadhwa et al. [69] | India | Prospective interventional study (6 months) | 60,000 IU of VD3 and 3500 mg of calcium weekly | 60 | 30.6 ± 4.0 (23–40) | Men with asthenozoospermia, oligozoospermia, or both | Na | SC↑ PM↑ | Unadjusted | 2b |
| 2018 Blomberg Jensen et al. [74] | Denmark | TBRCT (5 months) | single dose of 300,000 IU of VD3, then9800 IU of VD3 and 3500 mg of calcium weekly | 330 | 34.8 ± 6.6 | Men with semen abnormalities | ID-LC-MS/MS | SC→ TM→ PM→ NM→ | Unadjusted | 1b |
| 2017 Alzoubi et al. [68] | Jordan | Case-Control (2 months) | 35,000 IU of VD3 weekly | 34 | 20–45 | Men with semen abnormalities | ELISA | SC→ TM↑ PM↑ NM→ | Unadjusted | 2b |
4.3. Vitamin D and Sex Hormones: Observational Studies
4.4. Vitamin D and Sex Hormones: Interventional Studies
| Study | Country | Study Design | Number of Patients | Age (Years) 1 | Characteristics of Patients | Vitamin D Measurement Method | Hormones | Adjustment | Level of Evidence |
|---|---|---|---|---|---|---|---|---|---|
| 2022 Holzer et al. [59] | Argentina | Cross-Sectional | 56 | 20–45 | Andrological patients | CLIA | TT→ FT→ E2→ LH→ FSH→ SHBG ↑ | Unadjusted | 4 |
| 2022 Rezayat et al. [60] | Iran | Cross-Sectional | 114 | F:34.9 ± 13.5 I:34.6 ± 12.2 (20–59) | Fertile and infertile men | ELISA | TT↑ LH→ FSH→ | Unadjusted | 3b |
| 2022 Talebi et al. [81] | Iran | Cross-Sectional | 220 | 34.5 ± 5.6 (20–45) | Men with semen abnormalities | Na | TT→ FT→ LH→ FSH→ | Unadjusted | 4 |
| 2021 Ciccone et al. [57] | Brazil | Cross-Sectional | 260 | SA: 38.7 ± 8.5NS: 38.0 ± 8.8 (18–60) | Men with semen abnormalities and normospermic men | ECLIA/HPLC | TT↑ | Unadjusted | 3b |
| 2021 Książek et al. [80] | Poland | Cross-Sectional | 176 | 18–35 | Active young men from general population | ECLIA | TT→ FT→ LH→ FSH→ SHBG → | Age, BMI, Smoking, Alcohol Consumption, WHR | 2b |
| 2019 Chen et al. [97] | China | Cross-Sectional | 4254 | 18–93 | General population | CLIA | TT↑ | Age, Economic Status, Smoking, BMI, Hypertension, Diabetes | 2b |
| 2018 Rehman et al. [52] | Pakistan | Cross-Sectional | 313 | 25–55 | Fertile and infertile men | Na | TT↑ LH↓ FSH→ | Vitamin D adjusted with BMI | 3b |
| 2017 Abbasihormozi et al. [49] | Iran | Cross-Sectional | 278 | 33.5 ± 4.8 (20–50) | Men with oligoasthenoteratozoospermia and normospermic men | ECLIA | TT→ FT→ LH→ FSH→ | Age, BMI, Season | 3b |
| 2017 Tirabassi et al. [50] | Italy | Cross-Sectional | 104 | 33.1 ± 4.8 | Andrological patients | CLIA | TT→ | Age, BMI, PTH, Varicocele | 4 |
| 2017 Zhao et al. [79] | USA | Cross-Sectional | 3017 | 62.1 ± 10.2 (45–84) | General population | HPLC–tandem mass spectrometry | TT→ FT↓ E2↓ SHBG ↑ | Age, Race/Ethnicity, Study Site, BMI, Smoking, Education, Self-Reported Good Health Status, Intentional Physical Activity, Diabetes, Systolic Blood Pressure, Use of Antihypertensive Medications, eGFR, Total Cholesterol, HDL Cholesterol, Use of Lipid Lowering Medication Usage, C-Reactive Protein | 2b |
| 2016 Anic et al. [85] | USA | Cross-Sectional | 1633 | ≥20 | General population | RIA | TT↑ FT→ SHBG ↑ | Age, Race/Ethnicity, % Body Fat, Smoking | 2b |
| 2016 Barbonetti et al. [78] | Italy | Cross-Sectional | 49 | 47.5 ± 17.3 | Men with chronic spinal cord injury | CLIA | TT→ FT↑ | Age, Smoking, Alcohol Consumption, Coexisting Illness, Homeostatic Model Assessment of Insulin Resistance, Functional Independence Degree (Barthel Index), BMI, Weekly Leisure Time Physical Activity | 4 |
| 2016 Blomberg Jensen et al. [48] | Denmark | Cross-Sectional | 1189 | 34.3 | Andrological patients | ID-LC-MS/MS | TT→ FT↓ E2↓ LH→ FSH→ SHBG ↑ INHB↑ | Age, BMI, Smoking, Season, Abstinence, Time from Collection, Free Testosterone, Estradiol, Total Estradiol, Testosterone/Estradiol Ratio | 2b |
| 2016 Rafiq et al. [84] | Holland | Cohort Study | 643 | 65–89 | Older men from general population | CPBA | TT↑ FT→ E2→ LH→ FSH→ SHBG → | Age, BMI, Season, Alcohol Consumption, Smoking, Number of Chronic Diseases, Physical Function, Serum Creatinine | 2b |
| 2015 Chin et al. [77] | Malaysia | Cross-Sectional | 382 | 43.5 ± 15.5 | General population | ELISA | TT→ FT→ SHBG ↑ | Age, BMI, Race/Ethnicity | 2b |
| 2015 Tak et al. [82] | South Korea | Cross-Sectional | 652 | 56.7 ± 7.9 (40–80) | Men over 40 years old from general population | CLIA | TT↑ FT↑ | TT: Age, BMI, Waist Circumference, % Body Fat, Fasting Plasma Glucose, Diabetes, Dyslipidemia. FT: Age, Total Muscle Mass, Smooth Muscle Mass, Total Cholesterol, Diabetes, Dyslipidemia, Alcohol Consumption | 2b |
| 2015 Wang et al. [83] | China | Cross-Sectional | 2854 | 53.0 ± 13.5 | General population | CLIA | TT↑ FT→ E2↑ LH→ FSH→ SHBG → | Age, BMI, Residence Area, Economic Status, Smoking, HOMA-IR, Diabetes, Systolic Pressure | 2b |
| 2014 Lerchbaum et al. [88] | Austria | Cross-Sectional | 225 | 35 | Middle-aged men from general population | ID-LC-MS/MS | TT→ FT→ E2→ LH→ FSH→ SHBG → | Unadjusted | 4 |
| 2012 Hammound et al. [46] | USA | Cross-Sectional | 147 | 29.0 ± 8.5 (18–67) | General population | CLIA | TT→ FT→ E2→ LH→ FSH→ SHBG → | Age, BMI, Season, Alcohol Consumption, Smoking | 2b |
| 2012 Lee et al. [86] | Europe | Cross-Sectional | 3369 | 40–79 | General population | RIA | TT→ FT→ E2→ LH→ FSH→ SHBG → | Age, Centre, BMI, Smoking, Alcohol Consumption, Physical Activity, Physical Function, Heart Conditions, Hypertension, Diabetes, Depression | 2b |
| 2012 Nimptsch et al. [87] | USA | Cross-Sectional | 1362 | 40–75 | Participants selected for a nested case–control study on prostate cancer | RIA | TT↑ FT↑ E2↑ | Age, Batch, BMI, Season, Geographical Region, Smoking, Physical Activity, Time of Blood Collection. TT Further Adjusted for SHBG | 3b |
| 2011 Ramlau-Hansen et al. [61] | Denmark | Cross-Sectional | 307 | 18–21 | Young men from general population | ID-LC-MS/MS | TT→ E2→ LH→ FSH→ SHBG ↑ | Season, History of Diseases of the Reproductive Organs, Smoking, Maternal Smoking During Pregnancy, Maternal Alcohol During Pregnancy, Abstinence, Spillage During Collection of the Sample | 2b |
| Study | Country | Study Design (Duration) | Vitamin D Dose | Number of Patients | Age (Years) 1 | Characteristics of Patients | Vitamin D Measurement Method | Hormones | Adjustment | Level of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|
| 2021 Bartl et al. [70] | Slovakia | Prospective interventional study (6 months) | 17,500 IU of VD3 weekly | 34 | 36.6 | Infertile men | HPLC | TT→ FT→ E2→ LH→ FSH→ SHBG → | Unadjusted | 2b |
| 2021 Gheflati et al. [76] | Iran | DBRCT (3 months) | 50,000 IU of VD3 weekly for eight weeks and one maintenance dose of 50,000 IU for another four weeks | 44 | 18–45 | Men with asthenozoospermia | ELISA | TT→ SHBG → | Unadjusted | 1b |
| 2021 Maghsoumi-Norouzabad et al. [72] | Iran | TBRCT (3 months) | 28,000 IU of VD3 weekly | 86 | VD:35.1 ± 5.5 P:34.4 ± 5.1 | Men with asthenozoospermia | ELISA | TT→ E2→ LH→ FSH→ SHBG → | Unadjusted | 1b |
| 2021 Ulrich et al. [92] | Germany | DBRCT (3 months) | 5600 IU of VD3 weekly | 35 | 20–71 | General population | LC-MS/MS | TT→ | Unadjusted | 1b |
| Dose of VD3 adapted to patients VD serum levels | 18 | 20–71 | Hemodialysis patients | CLIA | TT→ | Unadjusted | 1b | |||
| 2020 Amini et al. [75] | Iran | TBRCT (3 months) | 50,000 IU of VD3 weekly for eight weeks and one maintenance dose of 50,000 IU for another four weeks | 62 | 35–39 | Men with semen abnormalities | ELISA | TT→ FT→ LH→ FSH→ SHBG ↓ | Unadjusted | 1b |
| 2019 Lerchbaum et al. [91] | Austria | DBRCT (3 months) | 20,000 IU of VD3 weekly | 94 | 47.0 ± 12.0 (18–70) | Men with serum TT levels < 10.4 nmol/L | ID-LC-MS/MS | TT→ FT→ E2→ LH→ FSH→ SBHG→ | Unadjusted | 1b |
| 2019 Zittermann et al. [96] | Germany | RCT (36 months) | 28,000 IU of VD3 weekly | 133 | 18–79 | Men with advanced heart failure, mean TT level of 11.2 nmol/L | CLIA | TT→ FT↓ SHBG → | Unadjusted | 1b |
| 2017 Canguven et al. [93] | Qatar | Prospective interventional study (12 months) | 150,000 IU of VD2 weekly; when serum 25(OH)D level reached 75 nmol/L, VD dose switched to 600,000 IU every eight weeks | 102 | 53.2 ± 10.5 (35–64) | Men with serum 25(OH)D levels < 30 ng/mL | ELISA | TT→ E2↓ LH→ | Unadjusted | 2b |
| 2017 Lerchbaum et al. [90] | Austria | DBRCT (3 months) | 20,000 IU of VD3 weekly | 98 | 18–70 | Men with serum 25(OH)D levels < 75 nmol/L and TT levels ≥ 10.4 nmol/L | ID-LC-MS/MS | TT→ FT→ E2↑ LH→ FSH→ SHBG↓ | Unadjusted | 1b |
| 2015 Heijboer et al. [89] | Holland | RCT (1.5 months) | 14,000 IU of VD3 weekly | 92 | 42–86 | Male patients with chronic heart failure | ID-LC-MS/MS | TT→ | Unadjusted | 1b |
| RCT (4 months) | 4200 IU of VD3 weekly | 49 | 71–97 | Male nursing home residents | RIA | TT→ | Unadjusted | 1b | ||
| RCT (4 months) | 8400 IU of VD3 daily | 43 | 20–70 | Vitamin D deficient male patients | ID-LC-MS/MS | TT→ | Unadjusted | 1b | ||
| 2013 Jorde et al. [95] | Norway | RCT (12 months) | 20,000–40,000 IU of VD3 and 3500 mg of calcium weekly | 129 | 48.9 ± 10.6 (21–70) | Men with BMI 28–47 kg/m2 | CLIA | TT→ FT→ LH→ FSH→ SHBG → | Unadjusted | 1b |
| RCT (6 months) | 40,000 IU of VD3 weekly | 53 | 51.2 ± 10.0 (30–75) | Men with serum 25(OH)D levels < 50 nmol/L | LC-MS/MS | TT→ FT→ SHBG → | Unadjusted | 1b | ||
| RCT (6 months) | 40,000 IU of VD3 weekly | 100 | 53.0 ±11.1 (30–75) | Men with serum 25(OH)D levels < 55 nmol/L | LC-MS/MS | TT→ FT→ SHBG→ | Unadjusted | 1b | ||
| 2011 Pilz et al. [94] | Austria | RCT (12 months) | 23,324 IU of VD3 weekly | 54 | VD:49.4 ± 10.2 P:46.8 ± 12.0 | Healthy, overweight men, mean TT level of 10.7 nmol/L | RIA | TT↑ FT↑ | Unadjusted | 1b |
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weinbauer, G.F.; Luetjens, C.M.; Simoni, M.; Nieschlag, E. Physiology of testicular function. In Andrology; Springer: Berlin/Heidelberg, Germany, 2010; pp. 11–59. [Google Scholar] [CrossRef]
- Mortimer, D.; Barratt, C.L.R.; Björndahl, L.; de Jager, C.; Jequier, A.M.; Muller, C.H. What should it take to describe a substance or product as “sperm-safe”. Hum. Reprod. Update 2013, 19 (Suppl. S1), i1–i45. [Google Scholar] [CrossRef] [Green Version]
- Battault, S.; Whiting, S.J.; Peltier, S.L.; Sadrin, S.; Gerber, G.; Maixent, J.M. Vitamin D metabolism, functions and needs: From science to health claims. Eur. J. Nutr. 2013, 52, 429–441. [Google Scholar] [CrossRef]
- Blomberg Jensen, M.; Nielsen, J.E.; Jørgensen, A.; Rajpert-De Meyts, E.; Kristensen, D.M.; Jørgensen, N.; Skakkebaek, N.E.; Juul, A.; Leffers, H. Vitamin D receptor and vitamin D metabolizing enzymes are expressed in the human male reproductive tract. Hum. Reprod. 2010, 25, 1303–1311. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F.; Maclaughlin, J.A.; Clark, M.B.; Holick, S.A.; Potts, J.T.; Anderson, R.R.; Blank, I.H.; Parrish, J.A.; Elias, P. Photosynthesis of Previtamin D3 in Human Skin and the Physiologic Consequences. Science 1980, 210, 203–205. [Google Scholar] [CrossRef]
- Chang, S.W.; Lee, H.C. Vitamin D and health—The missing vitamin in humans. Pediatr. Neonatol. 2019, 60, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Bouillon, R.; Schuit, F.; Antonio, L.; Rastinejad, F. Vitamin D Binding Protein: A Historic Overview. Front. Endocrinol. (Lausanne) 2020, 10, 910. [Google Scholar] [CrossRef]
- Cheng, J.B.; Motola, D.L.; Mangelsdorf, D.J.; Russell, D.W. De-orphanization of Cytochrome P450 2R1. J. Biol. Chem. 2003, 278, 38084–38093. [Google Scholar] [CrossRef] [Green Version]
- Schuster, I. Cytochromes P450 are essential players in the vitamin D signaling system. Biochim. Biophys. Acta 2011, 1814, 186–199. [Google Scholar] [CrossRef]
- Gil, Á.; Plaza-Diaz, J.; Mesa, M.D. Vitamin D: Classic and Novel Actions. Ann. Nutr. Metab. 2018, 72, 87–95. [Google Scholar] [CrossRef]
- McDuffie, J.R.; Calis, K.A.; Booth, S.L.; Uwaifo, G.I.; Yanovski, J.A. Effects of orlistat on fat-soluble vitamins in obese adolescents. Pharmacotherapy 2002, 22, 814–822. [Google Scholar] [CrossRef]
- Haussler, M.R.; Haussler, C.A.; Jurutka, P.W.; Thompson, P.D.; Hsieh, J.C.; Remus, L.S.; Selznick, S.H.; Whitfield, G.K. The vitamin D hormone and its nuclear receptor: Molecular actions and disease states. J. Endocrinol. 1997, 154 (Suppl. S3), S57–S73. [Google Scholar] [PubMed]
- Ramagopalan, S.V.; Heger, A.; Berlanga, A.J.; Maugeri, N.J.; Lincoln, M.R.; Burrell, A.; Handunnetthi, L.; Handel, A.E.; Disanto, G.; Orton, S.M.; et al. A ChIP-seq defined genome-wide map of vitamin D receptor binding: Associations with disease and evolution. Genome Res. 2010, 20, 1352–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dwivedi, P.P.; Hii, C.S.T.; Ferrante, A.; Tan, J.; Der, C.J.; Omdahl, J.L.; Morris, H.A.; May, B.K. Role of MAP kinases in the 1,25-dihydroxyvitamin D3-induced transactivation of the rat cytochrome P450C24 (CYP24) promoter. Specific functions for ERK1/ERK2 and ERK5. J. Biol. Chem. 2002, 277, 29643–29653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleet, J.C. Rapid, membrane-initiated actions of 1,25 dihydroxyvitamin D: What are they and what do they mean? J. Nutr. 2004, 134, 3215–3218. [Google Scholar] [CrossRef] [Green Version]
- Nutchey, B.K.; Kaplan, J.S.; Dwivedi, P.P.; Omdahl, J.L.; Ferrante, A.; May, B.K.; Hii, C.S.T. Molecular action of 1,25-dihydroxyvitamin D3 and phorbol ester on the activation of the rat cytochrome P450C24 (CYP24) promoter: Role of MAP kinase activities and identification of an important transcription factor binding site. Biochem. J. 2005, 389, 753–762. [Google Scholar] [CrossRef] [Green Version]
- Dwivedi, P.P.; Gao, X.H.; Tan, J.C.T.; Evdokiou, A.; Ferrante, A.; Morris, H.A.; May, B.K.; Hii, C.S.T. A role for the phosphatidylinositol 3-kinase--protein kinase C zeta--Sp1 pathway in the 1,25-dihydroxyvitamin D3 induction of the 25-hydroxyvitamin D3 24-hydroxylase gene in human kidney cells. Cell. Signal. 2010, 22, 543–552. [Google Scholar] [CrossRef]
- Doroudi, M.; Schwartz, Z.; Boyan, B.D. Membrane-mediated Actions of 1,25-Dihydroxy Vitamin D3: A Review of the Roles of Phospholipase A2 Activating Protein and Ca2+/Calmodulin-dependent Protein Kinase II. J. Steroid Biochem. Mol. Biol. 2015, 147, 81–84. [Google Scholar] [CrossRef] [Green Version]
- Hii, C.S.; Ferrante, A. The Non-Genomic Actions of Vitamin D. Nutrients 2016, 8, 135. [Google Scholar] [CrossRef] [Green Version]
- Norman, A.W. Minireview: Vitamin D receptor: New assignments for an already busy receptor. Endocrinology 2006, 147, 5542–5548. [Google Scholar] [CrossRef]
- Haussler, M.R.; Jurutka, P.W.; Mizwicki, M.; Norman, A.W. Vitamin D receptor (VDR)-mediated actions of 1α,25(OH)2vitamin D3: Genomic and non-genomic mechanisms. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 543–559. [Google Scholar] [CrossRef]
- Veldurthy, V.; Wei, R.; Campbell, M.; Lupicki, K.; Dhawan, P.; Christakos, S. 25-Hydroxyvitamin D3 24-Hydroxylase: A Key Regulator of 1,25(OH)2D3 Catabolism and Calcium Homeostasis. Vitam. Horm. 2016, 100, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Prosser, D.E.; Jones, G. Enzymes involved in the activation and inactivation of vitamin D. Trends Biochem. Sci. 2004, 29, 664–673. [Google Scholar] [CrossRef] [PubMed]
- Henry, H.L. Regulation of vitamin D metabolism. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Hollis, B.W. Assessment of circulating 25(OH)D and 1,25(OH)2D: Emergence as clinically important diagnostic tools. Nutr. Rev. 2007, 65 (Suppl. S2), S87–S90. [Google Scholar] [CrossRef]
- Hollis, B.W. Assessment of vitamin D status and definition of a normal circulating range of 25-hydroxyvitamin D. Curr. Opin. Endocrinol. Diabetes. Obes. 2008, 15, 489–494. [Google Scholar] [CrossRef]
- Cashman, K.D.; van den Heuvel, E.G.H.M.; Schoemaker, R.J.W.; Prévéraud, D.P.; Macdonald, H.M.; Arcot, J. 25-Hydroxyvitamin D as a Biomarker of Vitamin D Status and Its Modeling to Inform Strategies for Prevention of Vitamin D Deficiency within the Population. Adv. Nutr. 2017, 8, 947–957. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Dawson-Hughes, B.; Mithal, A.; Bonjour, J.P.; Boonen, S.; Burckhardt, P.; Fuleihan, G.E.H.; Josse, R.G.; Lips, P.; Morales-Torres, J.; Yoshimura, N. IOF position statement: Vitamin D recommendations for older adults. Osteoporos. Int. 2010, 21, 1151–1154. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Recommendations Abstracted from the American Geriatrics Society Consensus Statement on Vitamin D for Prevention of Falls and Their Consequences. J. Am. Geriatr. Soc. 2014, 62, 147–152. [CrossRef]
- Habib, F.K.; Maddy, S.Q.; Gelly, K.J. Characterisation of receptors for 1,25-dihydroxyvitamin D3 in the human testis. J. Steroid Biochem. 1990, 35, 195–199. [Google Scholar] [CrossRef]
- Corbett, S.T.; Hill, O.; Nangia, A.K. Vitamin D receptor found in human sperm. Urology 2006, 68, 1345–1349. [Google Scholar] [CrossRef] [PubMed]
- Aquila, S.; Guido, C.; Perrotta, I.; Tripepi, S.; Nastro, A.; Andò, S. Human sperm anatomy: Ultrastructural localization of 1alpha,25-dihydroxyvitamin D receptor and its possible role in the human male gamete. J. Anat. 2008, 213, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Blomberg Jensen, M.; Bjerrum, P.J.; Jessen, T.E.; Nielsen, J.E.; Joensen, U.N.; Olesen, I.A.; Petersen, J.H.; Juul, A.; Dissing, S.; Jørgensen, N. Vitamin D is positively associated with sperm motility and increases intracellular calcium in human spermatozoa. Hum. Reprod. 2011, 26, 1307–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blomberg Jensen, M.; Jørgensen, A.; Nielsen, J.E.; Steinmeyer, A.; Leffers, H.; Juul, A.; Meyts, E.R. De Vitamin D Metabolism and Effects on Pluripotency Genes and Cell Differentiation in Testicular Germ Cell Tumors In Vitro and In Vivo. Neoplasia 2012, 14, 952. [Google Scholar] [CrossRef] [Green Version]
- Foresta, C.; Strapazzon, G.; De Toni, L.; Perilli, L.; Di Mambro, A.; Muciaccia, B.; Sartori, L.; Selice, R. Bone Mineral Density and Testicular Failure: Evidence for a Role of Vitamin D 25-Hydroxylase in Human Testis. J. Clin. Endocrinol. Metab. 2011, 96, E646–E652. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Fernandez, R.; Alonso, M.; Segura, C.; Muñoz, I.; García-Caballero, T.; Diéguez, C. Vitamin D receptor gene expression in human pituitary gland. Life Sci. 1996, 60, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Eyles, D.W.; Smith, S.; Kinobe, R.; Hewison, M.; McGrath, J.J. Distribution of the vitamin D receptor and 1 alpha-hydroxylase in human brain. J. Chem. Neuroanat. 2005, 29, 21–30. [Google Scholar] [CrossRef]
- Johnson, J.A.; Grande, J.P.; Roche, P.C.; Kumar, R. Immunohistochemical detection and distribution of the 1,25-dihydroxyvitamin D3 receptor in rat reproductive tissues. Histochem. Cell Biol. 1996, 105, 7–15. [Google Scholar] [CrossRef]
- Sood, S.; Marya, R.K.; Reghunandanan, R.; Singh, G.P.; Jaswal, T.S.; Gopinalhan, K. Effect of vitamin D deficiency on testicular function in the rat. Ann. Nutr. Metab. 1992, 36, 203–208. [Google Scholar] [CrossRef]
- Uhland, A.M.; Kwiecinski, G.G.; DeLuca, H.F. Normalization of serum calcium restores fertility in vitamin D-deficient male rats. J. Nutr. 1992, 122, 1338–1344. [Google Scholar] [CrossRef]
- Kinuta, K.; Tanaka, H.; Moriwake, T.; Aya, K.; Kato, S.; Seino, Y. Vitamin D Is an Important Factor in Estrogen Biosynthesis of Both Female and Male Gonads. Endocrinology 2000, 141, 1317–1324. [Google Scholar] [CrossRef] [PubMed]
- Oxford Centre for Evidence-Based Medicine: Levels of Evidence (March 2009)—Centre for Evidence-Based Medicine (CEBM), University of Oxford. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009 (accessed on 15 November 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Hammoud, A.O.; Wayne Meikle, A.; Matthew Peterson, C.; Stanford, J.; Gibson, M.; Carrell, D.T. Association of 25-hydroxy-vitamin D levels with semen and hormonal parameters. Asian J. Androl. 2012, 14, 855–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, B.; Sun, H.; Wan, Y.; Wang, H.; Qin, W.; Yang, L.; Zhao, H.; Yuan, J.; Yao, B. Associations between testosterone, bone mineral density, vitamin D and semen quality in fertile and infertile Chinese men. Int. J. Androl. 2012, 35, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Blomberg Jensen, M.; Lawaetz, J.G.; Andersson, A.M.; Petersen, J.H.; Nordkap, L.; Bang, A.K.; Ekbom, P.; Joensen, U.N.; Prætorius, L.; Lundstrøm, P.; et al. Vitamin D deficiency and low ionized calcium are linked with semen quality and sex steroid levels in infertile men. Hum. Reprod. 2016, 31, 1875–1885. [Google Scholar] [CrossRef] [Green Version]
- Abbasihormozi, S.; Kouhkan, A.; Alizadeh, A.R.; Shahverdi, A.H.; Nasr-Esfahani, M.H.; Sadighi Gilani, M.A.; Salman Yazdi, R.; Matinibehzad, A.; Zolfaghari, Z. Association of vitamin D status with semen quality and reproductive hormones in Iranian subfertile men. Andrology 2017, 5, 113–118. [Google Scholar] [CrossRef]
- Tirabassi, G.; Cutini, M.; Muscogiuri, G.; delli Muti, N.; Corona, G.; Galdiero, M.; Pivonello, R.; Colao, A.; Balercia, G. Association between vitamin D and sperm parameters: Clinical evidence. Endocrine 2017, 58, 194–198. [Google Scholar] [CrossRef] [Green Version]
- Azizi, E.; Naji, M.; Shabani-Nashtaei, M.; Sobhani, A.; Najafi, A.; Amidi, F. Association of serum content of 25-hydroxy vitamin D with semen quality in normozoospermic and oligoasthenoteratozoospermic men. Int. J. Reprod. Biomed. 2018, 16, 689. [Google Scholar]
- Rehman, R.; Lalani, S.; Baig, M.; Nizami, I.; Rana, Z.; Gazzaz, Z.J. Association Between Vitamin D, Reproductive Hormones and Sperm Parameters in Infertile Male Subjects. Front. Endocrinol. (Lausanne) 2018, 9, 607. [Google Scholar] [CrossRef]
- Derakhshan, M.; Derakhshan, M.; Omidi, E.; Heidarpour, M. The association between serum vitamin D level and sperm parameters; A pilot study in a subset of Iranian infertile males. Immunopathol. Persa 2020, 6, e30. [Google Scholar] [CrossRef]
- Hajianfar, H.; Karimi, E.; Mollaghasemi, N.; Rezaei, S.; Arab, A. Is there a relationship between serum vitamin D and semen parameters? A cross-sectional sample of the Iranian infertile men. Basic Clin. Androl. 2021, 31, 29. [Google Scholar] [CrossRef] [PubMed]
- Hussein, T.M.; Eldabah, N.; Zayed, H.A.; Genedy, R.M. Assessment of serum vitamin D level and seminal vitamin D receptor gene methylation in a sample of Egyptian men with idiopathic infertility. Andrologia 2021, 53, e14172. [Google Scholar] [CrossRef]
- Kumari, S.; Singh, K.; Kumari, S.; Nishat, H.; Tiwary, B. Association of Vitamin D and Reproductive Hormones with Semen Parameters in Infertile Men. Cureus 2021, 13, e14511. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, I.; Costa, E.; Pariz, J.; Teixeira, T.; Drevet, J.; Gharagozloo, P.; Aitken, R.; Hallak, J. Serum vitamin D content is associated with semen parameters and serum testosterone levels in men. Asian J. Androl. 2021, 23, 52–58. [Google Scholar] [CrossRef]
- Güngör, K.; Güngör, N.D.; Başar, M.M.; Cengiz, F.; Erşahin, S.S.; Çil, K. Relationship between serum vitamin D levels semen parameters and sperm DNA damage in men with unexplained infertility. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 499–505. [Google Scholar] [CrossRef]
- Holzer, M.; Massa, E.; Ghersevich, S. Relationship between serum vitamin D concentration and parameters of gonadal function in infertile male patients. Curr. Urol. 2022, in press. [CrossRef]
- Rezayat, A.A.; Asadpour, A.A.; Yarahmadi, A.; Ahmadnia, H.; Hakkak, A.M.; Soltani, S. Association Between Serum Vitamin D Concentration with Spermiogram Parameters and Reproductive Hormones Among Infertile Iranian Males: A Cross-sectional Study. Reprod. Sci. 2022, 29, 270–276. [Google Scholar] [CrossRef]
- Ramlau-Hansen, C.H.; Moeller, U.K.; Bonde, J.P.; Olsen, J.; Thulstrup, A.M. Are serum levels of vitamin D associated with semen quality? Results from a cross-sectional study in young healthy men. Fertil. Steril. 2011, 95, 1000–1004. [Google Scholar] [CrossRef]
- Neville, G.; Martyn, F.; Kilbane, M.; O’Riordan, M.; Wingfield, M.; McKenna, M.; McAuliffe, F.M. Vitamin D status and fertility outcomes during winter among couples undergoing in vitro fertilization/intracytoplasmic sperm injection. Int. J. Gynaecol. Obstet. 2016, 135, 172–176. [Google Scholar] [CrossRef]
- Zhu, C.L.; Xu, Q.F.; Li, S.X.; Wei, Y.C.; Zhu, G.C.; Yang, C.; Shi, Y.C. Investigation of serum vitamin D levels in Chinese infertile men. Andrologia 2016, 48, 1261–1266. [Google Scholar] [CrossRef]
- Józków, P.; Slowinska-Lisowska, M.; Zagrodna, A.; Medras, M.; Lwow, F. Vitamin D and semen quality in urban, young, healthy men (Androls). J. Mens. Health 2018, 14, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Jueraitetibaike, K.; Ding, Z.; Wang, D.D.; Peng, L.P.; Jing, J.; Chen, L.; Ge, X.; Qiu, X.H.; Yao, B. The effect of vitamin D on sperm motility and the underlying mechanism. Asian J. Androl. 2019, 21, 400–407. [Google Scholar] [CrossRef]
- Rudnicka, A.; Adoamnei, E.; Noguera-Velasco, J.A.; Vioque, J.; Cañizares-Hernández, F.; Mendiola, J.; Jørgensen, N.; Chavarro, J.E.; Swan, S.H.; Torres-Cantero, A.M. Vitamin D status is not associated with reproductive parameters in young Spanish men. Andrology 2020, 8, 323–331. [Google Scholar] [CrossRef]
- Kamal, E.E.; Bakry, R.M.; Danyail, M.Y.; Badran, A.Y. Nonsignificant relation of seminal and serum vitamin D levels and semen parameters of males in Upper Egypt. Egypt. J. Dermatol. Venerol. 2022, 42, 27. [Google Scholar] [CrossRef]
- Alzoubi, A.; Mahdi, H.; Al Bashir, S.; Halalsheh, O.; Ebbini, M.A.; Alzarir, M.; Al-Ahmar, K.; Alfaqih, M.; Al-Hadidi, A.H. Normalization of Serum Vitamin D Improves Semen Motility Parameters in Patients with Idiopathic Male Infertility. Acta Endocrinol. (Bucharest Rom. 2005) 2017, 13, 180–187. [Google Scholar] [CrossRef]
- Wadhwa, L.; Priyadarshini, S.; Fauzdar, A.; Wadhwa, S.N.; Arora, S. Impact of Vitamin D Supplementation on Semen Quality in Vitamin D-Deficient Infertile Males with Oligoasthenozoospermia. J. Obstet. Gynaecol. India 2020, 70, 44–49. [Google Scholar] [CrossRef]
- Bartl, I.; Ondrušová, M.; Kužma, M.; Jackuliak, P.; Gažová, A.; Kyselovič, J.; Payer, J. Treatment With Cholecalciferol Leads to Increase Of Selected Semen Parameters in Young Infertile Males: Results of a 6-month Interventional Study. Physiol. Res. 2021, 70, S99–S107. [Google Scholar] [CrossRef]
- Amina Begum, M.; Ishrat, S.; Rani Saha, M.; Parveen, F.; Shah Alam, M.; Deeba, F.; Fatima, P.; Professor, A. Vitamin D Supplementation Improves Sperm Motility in Infertile Males with Asthenozoospermia: A Prospective Observational Study Scholars International Journal of Obstetrics and Gynecology Abbreviated Key Title: SchInt J ObstetGynec Vitamin D Supplementation Improves Sperm Motility in Infertile Males with Asthenozoospermia: A Prospective Observational Study. SchInt. J. Obs. 2021, 4, 331–336. [Google Scholar] [CrossRef]
- Maghsoumi-Norouzabad, L.; Zare Javid, A.; Mansoori, A.; Dadfar, M.; Serajian, A. The effects of Vitamin D3 supplementation on Spermatogram and endocrine factors in asthenozoospermia infertile men: A randomized, triple blind, placebo-controlled clinical trial. Reprod. Biol. Endocrinol. 2021, 19, 102. [Google Scholar] [CrossRef]
- Padmapriya, D.; Archana, R.; Sharma, N.; Vijayaraghavan, R. Effects of Vitamin D3 Supplementation in Male Reproductive Function: A Double-Blinded Randomized Controlled Trial. Curr. Top. Nutraceutical Res. 2022, 20, 334–339. [Google Scholar] [CrossRef]
- Blomberg Jensen, M.; Gerner Lawaetz, J.; Petersen, J.H.; Juul, A.; Jørgensen, N. Effects of Vitamin D Supplementation on Semen Quality, Reproductive Hormones, and Live Birth Rate: A Randomized Clinical Trial. J. Clin. Endocrinol. Metab. 2018, 103, 870–881. [Google Scholar] [CrossRef]
- Amini, L.; Mohammadbeigi, R.; Vafa, M.; Haghani, H.; Vahedian-Azimi, A.; Karimi, L.; Jahanfar, S.; Jamialahmadi, T.; Talebi, A.; Sahebkar, A. Evaluation of the effect of vitamin D3 supplementation on quantitative and qualitative parameters of spermograms and hormones in infertile men: A Randomized controlled trial. Complement. Ther. Med. 2020, 53, 102529. [Google Scholar] [CrossRef]
- Gheflati, A.; Mirjalili, S.A.M.; Kaviani, M.; Salehi-Abargouei, A.; Hosseini-Marnani, E.; Nadjarzadeh, A. Effects of Vitamin D Supplementation on Semen Quality and Reproductive Hormones in Patients with Asthenozoospermia: A Randomized Double-Blind Placebo-Controlled Clinical Trial. J. Nutr. Food Secur. 2021, 6, 31–42. [Google Scholar] [CrossRef]
- Chin, K.-Y.; Ima-Nirwana, S.; Wan Ngah, W.Z. Vitamin D is significantly associated with total testosterone and sex hormone-binding globulin in Malaysian men. Aging Male 2015, 18, 175–179. [Google Scholar] [CrossRef]
- Barbonetti, A.; Vassallo, M.R.C.; Felzani, G.; Francavilla, S.; Francavilla, F. Association between 25(OH)-vitamin D and testosterone levels: Evidence from men with chronic spinal cord injury. J. Spinal Cord Med. 2016, 39, 246–252. [Google Scholar] [CrossRef] [Green Version]
- Zhao, D.; Ouyang, P.; de Boer, I.H.; Lutsey, P.L.; Farag, Y.M.K.; Guallar, E.; Siscovick, D.S.; Post, W.S.; Kalyani, R.R.; Billups, K.L.; et al. Serum vitamin D and sex hormones levels in men and women: The Multi-Ethnic Study of Atherosclerosis (MESA). Maturitas 2017, 96, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Książek, A.; Mędraś, M.; Zagrodna, A.; Słowińska-Lisowska, M.; Lwow, F. Correlative studies on vitamin D and total, free bioavailable testosterone levels in young, healthy men. Sci. Rep. 2021, 11, 20198. [Google Scholar] [CrossRef]
- Talebi, A.; Amini, L.; Sahebkar, A.; Paper, R. Association between Serum Vitamin D3 Levels and Sex Hormones in Infertile Men. J. Babol Univ. Med. Sci. 2022, 24, 88–94. [Google Scholar]
- Tak, Y.J.; Lee, J.G.; Kim, Y.J.; Park, N.C.; Kim, S.S.; Lee, S.; Cho, B.M.; Kong, E.H.; Jung, D.W.; Yi, Y.H. Serum 25-hydroxyvitamin D levels and testosterone deficiency in middle-aged Korean men: A cross-sectional study. Asian J. Androl. 2015, 17, 324. [Google Scholar] [CrossRef]
- Wang, N.; Han, B.; Li, Q.; Chen, Y.; Chen, Y.; Xia, F.; Lin, D.; Jensen, M.D.; Lu, Y. Vitamin D is associated with testosterone and hypogonadism in Chinese men: Results from a cross-sectional SPECT-China study. Reprod. Biol. Endocrinol. 2015, 13, 74. [Google Scholar] [CrossRef]
- Rafiq, R.; van Schoor, N.M.; Sohl, E.; Zillikens, M.C.; Oosterwerff, M.M.; Schaap, L.; Lips, P.; de Jongh, R.T. Associations of vitamin D status and vitamin D-related polymorphisms with sex hormones in older men. J. Steroid Biochem. Mol. Biol. 2016, 164, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Anic, G.M.; Albanes, D.; Rohrmann, S.; Kanarek, N.; Nelson, W.G.; Bradwin, G.; Rifai, N.; McGlynn, K.A.; Platz, E.A.; Mondul, A.M. Association between serum 25-hydroxyvitamin D and serum sex steroid hormones among men in NHANES. Clin. Endocrinol. (Oxf.) 2016, 85, 258–266. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.M.; Tajar, A.; Pye, S.R.; Boonen, S.; Vanderschueren, D.; Bouillon, R.; O’Neill, T.W.; Bartfai, G.; Casanueva, F.F.; Finn, J.D.; et al. Association of hypogonadism with vitamin D status: The European Male Ageing Study. Eur. J. Endocrinol. 2012, 166, 77–85. [Google Scholar] [CrossRef] [Green Version]
- Nimptsch, K.; Platz, E.A.; Willett, W.C.; Giovannucci, E. Association between plasma 25-OH vitamin D and testosterone levels in men. Clin. Endocrinol. (Oxf.) 2012, 77, 106–112. [Google Scholar] [CrossRef] [Green Version]
- Lerchbaum, E.; Pilz, S.; Trummer, C.; Rabe, T.; Schenk, M.; Heijboer, A.C.; Obermayer-Pietsch, B. Serum vitamin D levels and hypogonadism in men. Andrology 2014, 2, 748–754. [Google Scholar] [CrossRef]
- Heijboer, A.C.; Oosterwerff, M.; Schroten, N.F.; Eekhoff, E.M.W.; Chel, V.G.M.; De Boer, R.A.; Blankenstein, M.A.; Lips, P. Vitamin D supplementation and testosterone concentrations in male human subjects. Clin. Endocrinol. (Oxf.) 2015, 83, 105–110. [Google Scholar] [CrossRef]
- Lerchbaum, E.; Pilz, S.; Trummer, C.; Schwetz, V.; Pachernegg, O.; Heijboer, A.C.; Obermayer-Pietsch, B. Vitamin D and Testosterone in Healthy Men: A Randomized Controlled Trial. J. Clin. Endocrinol. Metab. 2017, 102, 4292–4302. [Google Scholar] [CrossRef] [Green Version]
- Lerchbaum, E.; Trummer, C.; Theiler-Schwetz, V.; Kollmann, M.; Wölfler, M.; Heijboer, A.C.; Pilz, S.; Obermayer-Pietsch, B. Effects of vitamin D supplementation on androgens in men with low testosterone levels: A randomized controlled trial. Eur. J. Nutr. 2019, 58, 3135–3146. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, C.; Trojanowicz, B.; Fiedler, R.; Kraus, F.B.; Stangl, G.I.; Girndt, M.; Seibert, E. Serum Testosterone Levels Are Not Modified by Vitamin D Supplementation in Dialysis Patients and Healthy Subjects. Nephron 2021, 145, 481–485. [Google Scholar] [CrossRef]
- Canguven, O.; Talib, R.A.; El Ansari, W.; Yassin, D.J.; Al Naimi, A. Vitamin D treatment improves levels of sexual hormones, metabolic parameters and erectile function in middle-aged vitamin D deficient men. Aging Male 2017, 20, 9–16. [Google Scholar] [CrossRef]
- Pilz, S.; Frisch, S.; Koertke, H.; Kuhn, J.; Dreier, J.; Obermayer-Pietsch, B.; Wehr, E.; Zittermann, A. Effect of vitamin D supplementation on testosterone levels in men. Horm. Metab. Res. 2011, 43, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Jorde, R.; Grimnes, G.; Hutchinson, M.; Kjærgaard, M.; Kamycheva, E.; Svartberg, J. Supplementation with vitamin D does not increase serum testosterone levels in healthy males. Horm. Metab. Res. 2013, 45, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A.; Ernst, J.B.; Prokop, S.; Fuchs, U.; Dreier, J.; Kuhn, J.; Knabbe, C.; Berthold, H.K.; Gouni-Berthold, I.; Gummert, J.F.; et al. Vitamin D supplementation does not prevent the testosterone decline in males with advanced heart failure: The EVITA trial. Eur. J. Nutr. 2019, 58, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhai, H.; Cheng, J.; Weng, P.; Chen, Y.; Li, Q.; Wang, C.; Xia, F.; Wang, N.; Lu, Y. Causal Link Between Vitamin D and Total Testosterone in Men: A Mendelian Randomization Analysis. J. Clin. Endocrinol. Metab. 2019, 104, 3148–3156. [Google Scholar] [CrossRef]
- Arab, A.; Hadi, A.; Moosavian, S.P.; Askari, G.; Nasirian, M. The association between serum vitamin D, fertility and semen quality: A systematic review and meta-analysis. Int. J. Surg. 2019, 71, 101–109. [Google Scholar] [CrossRef]
- Nolan, M.A.; Babcock, D.F.; Wennemuth, G.; Brown, W.; Burton, K.A.; McKnight, G.S. Sperm-specific protein kinase A catalytic subunit Calpha2 orchestrates cAMP signaling for male fertility. Proc. Natl. Acad. Sci. USA 2004, 101, 13483–13488. [Google Scholar] [CrossRef] [Green Version]
- Banks, N.; Sun, F.; Krawetz, S.A.; Coward, R.M.; Masson, P.; Smith, J.F.; Trussell, J.C.; Santoro, N.; Zhang, H.; Steiner, A.Z. Male vitamin D status and male factor infertility. Fertil. Steril. 2021, 116, 973–979. [Google Scholar] [CrossRef]
- Cui, X.; Pertile, R.; Eyles, D.W. The vitamin D receptor (VDR) binds to the nuclear matrix via its hinge domain: A potential mechanism for the reduction in VDR mediated transcription in mitotic cells. Mol. Cell. Endocrinol. 2018, 472, 18–25. [Google Scholar] [CrossRef]
- Merino, O.; Sánchez, R.; Gregorio, B.M.; Sampaio, F.J.; Risopatrón, J. Effects of Diet-Induced Obesity and Deficient in Vitamin D on Spermatozoa Function and DNA Integrity in Sprague-Dawley Rats. Biomed Res. Int. 2018, 2018, 5479057. [Google Scholar] [CrossRef]
- Skakkebaek, N.E.; Rajpert-De Meyts, E.; Buck Louis, G.M.; Toppari, J.; Andersson, A.M.; Eisenberg, M.L.; Jensen, T.K.; Jørgensen, N.; Swan, S.H.; Sapra, K.J.; et al. Male Reproductive Disorders and Fertility Trends: Influences of Environment and Genetic Susceptibility. Physiol. Rev. 2016, 96, 55–97. [Google Scholar] [CrossRef]
- Hofer, D.; Münzker, J.; Schwetz, V.; Ulbing, M.; Hutz, K.; Stiegler, P.; Zigeuner, R.; Pieber, T.R.; Müller, H.; Obermayer-Pietsch, B. Testicular synthesis and vitamin D action. J. Clin. Endocrinol. Metab. 2014, 99, 3766–3773. [Google Scholar] [CrossRef] [Green Version]
- de Angelis, C.; Galdiero, M.; Pivonello, C.; Garifalos, F.; Menafra, D.; Cariati, F.; Salzano, C.; Galdiero, G.; Piscopo, M.; Vece, A.; et al. The role of vitamin D in male fertility: A focus on the testis. Rev. Endocr. Metab. Disord. 2017, 18, 285–305. [Google Scholar] [CrossRef] [PubMed]
- Hosseini Marnani, E.; Mollahosseini, M.; Gheflati, A.; Ghadiri-Anari, A.; Nadjarzadeh, A. The effect of vitamin D supplementation on the androgenic profile in men: A systematic review and meta-analysis of clinical trials. Andrologia 2019, 51, e13343. [Google Scholar] [CrossRef] [PubMed]
- Oury, F.; Ferron, M.; Huizhen, W.; Confavreux, C.; Xu, L.; Lacombe, J.; Srinivas, P.; Chamouni, A.; Lugani, F.; Lejeune, H.; et al. Osteocalcin regulates murine and human fertility through a pancreas-bone-testis axis. J. Clin. Investig. 2013, 123, 2421–2433. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.V.; Swami, S.; Peng, L.; Wang, J.; Moreno, J.; Feldman, D. Tissue-selective regulation of aromatase expression by calcitriol: Implications for breast cancer therapy. Endocrinology 2010, 151, 32–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenzen, M.; Boisen, I.M.; Mortensen, L.J.; Lanske, B.; Juul, A.; Blomberg Jensen, M. Reproductive endocrinology of vitamin D. Mol. Cell. Endocrinol. 2017, 453, 103–112. [Google Scholar] [CrossRef]
- Zamani, A.; Saki, F.; Hatami, N.; Koohpeyma, F. Stereological assessment of the effects of vitamin D deficiency on the rat testis. BMC Endocr. Disord. 2020, 20, 162. [Google Scholar] [CrossRef]
- Sonnenberg, J.; Christakos, S.; Krey, L.C. 1,25-Dihydroxyvitamin D3 treatment results in increased choline acetyltransferase activity in specific brain nuclei. Endocrinology 1986, 118, 1433–1439. [Google Scholar] [CrossRef] [PubMed]
- Zanatta, L.; Zamoner, A.; Zanatta, A.P.; Bouraïma-Lelong, H.; Delalande, C.; Bois, C.; Carreau, S.; Silva, F.R.M.B. Nongenomic and genomic effects of 1α,25(OH)2 vitamin D3 in rat testis. Life Sci. 2011, 89, 515–523. [Google Scholar] [CrossRef]
- Merino, O.; Sánchez, R.; Gregorio, M.B.; Sampaio, F.; Risopatrón, J. Effect of high-fat and vitamin D deficient diet on rat sperm quality and fertility. Theriogenology 2019, 125, 6–11. [Google Scholar] [CrossRef]
- Xu, Y.; Lou, Y.; Kong, J. VDR regulates energy metabolism by modulating remodeling in adipose tissue. Eur. J. Pharmacol. 2019, 865, 172761. [Google Scholar] [CrossRef]
- Wang, L.; Lu, H.; Wang, S.; Liu, H.; Guo, M.; Bai, H.; Zeng, W.; Zhang, T. Vitamin D Receptor affects male mouse fertility via regulation of lipid metabolism and testosterone biosynthesis in testis. Gene 2022, 834, 146589. [Google Scholar] [CrossRef]
- Blomberg Jensen, M. Vitamin D and male reproduction. Nat. Rev. Endocrinol. 2014, 10, 175–186. [Google Scholar] [CrossRef]
- Albahrani, A.A.; Rotarou, V.; Roche, P.J.; Greaves, R.F. A simultaneous quantitative method for vitamins A, D and E in human serum using liquid chromatography-tandem mass spectrometry. J. Steroid Biochem. Mol. Biol. 2016, 159, 41–53. [Google Scholar] [CrossRef]
- Agmon-Levin, N.; Theodor, E.; Segal, R.M.; Shoenfeld, Y. Vitamin D in systemic and organ-specific autoimmune diseases. Clin. Rev. Allergy Immunol. 2013, 45, 256–266. [Google Scholar] [CrossRef]
- de Lorenzo, A.; Noce, A.; Moriconi, E.; Rampello, T.; Marrone, G.; di Daniele, N.; Rovella, V. MOSH Syndrome (Male Obesity Secondary Hypogonadism): Clinical Assessment and Possible Therapeutic Approaches. Nutrients 2018, 10, 474. [Google Scholar] [CrossRef] [Green Version]
- Santos, H.O.; Howell, S.; Nichols, K.; Teixeira, F.J. Reviewing the Evidence on Vitamin D Supplementation in the Management of Testosterone Status and Its Effects on Male Reproductive System (Testis and Prostate): Mechanistically Dazzling but Clinically Disappointing. Clin. Ther. 2020, 42, e101–e114. [Google Scholar] [CrossRef]


| Hypothesis | Supported | Not Supported | |
|---|---|---|---|
| VD has a positive effect on sperm motility | observational studies | [35,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60] | [61,62,63,64,65,66,67] |
| interventional studies | [68,69,70,71,72,73] | [74,75,76] | |
| VD increases sperm concentration | observational studies | [46,52,53,54,55,56,57,58,60] | [35,48,49,50,51,59,61,62,63,64,65,66,67] |
| interventional studies | [69,70,71,73] | [68,72,74,75,76] | |
| VD improves sperm morphology | observational studies | [35,51,52,53,54,56,57,58] | [46,48,49,50,55,59,60,61,62,65,67] |
| interventional studies | [70] | [68,72,73,74,75,76] | |
| VD reduces sperm DNA fragmentation | observational studies | [53,58] | [51] |
| interventional studies | Na | Na | |
| VD positively influences testosterone levels | observational studies | [52,57,60,78,82,83,84,85,87,97] | [46,48,59,61,77,80,81,86,88] |
| interventional studies | [94] | [70,72,75,76,91,92,93,95,96] | |
| VD affects the bioavailability of androgens by increasing the level of SHBG | observational studies | [48,59,61,77,79,85] | [46,49,50,79,80,83,84,86,88] |
| interventional studies | Na | [70,72,75,76,89,90,91,95,96] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adamczewska, D.; Słowikowska-Hilczer, J.; Walczak-Jędrzejowska, R. The Association between Vitamin D and the Components of Male Fertility: A Systematic Review. Biomedicines 2023, 11, 90. https://doi.org/10.3390/biomedicines11010090
Adamczewska D, Słowikowska-Hilczer J, Walczak-Jędrzejowska R. The Association between Vitamin D and the Components of Male Fertility: A Systematic Review. Biomedicines. 2023; 11(1):90. https://doi.org/10.3390/biomedicines11010090
Chicago/Turabian StyleAdamczewska, Daria, Jolanta Słowikowska-Hilczer, and Renata Walczak-Jędrzejowska. 2023. "The Association between Vitamin D and the Components of Male Fertility: A Systematic Review" Biomedicines 11, no. 1: 90. https://doi.org/10.3390/biomedicines11010090
APA StyleAdamczewska, D., Słowikowska-Hilczer, J., & Walczak-Jędrzejowska, R. (2023). The Association between Vitamin D and the Components of Male Fertility: A Systematic Review. Biomedicines, 11(1), 90. https://doi.org/10.3390/biomedicines11010090