


The Cerebellum Gets Social: Evidence from an Exploratory Study of Cerebellar, Neurodevelopmental, and Psychiatric Disorders

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Social Cognition Assessment
2.3. Data Analyses
2.4. Voxel-Based Morphometry
3. Results
3.1. Social Cognition Profile
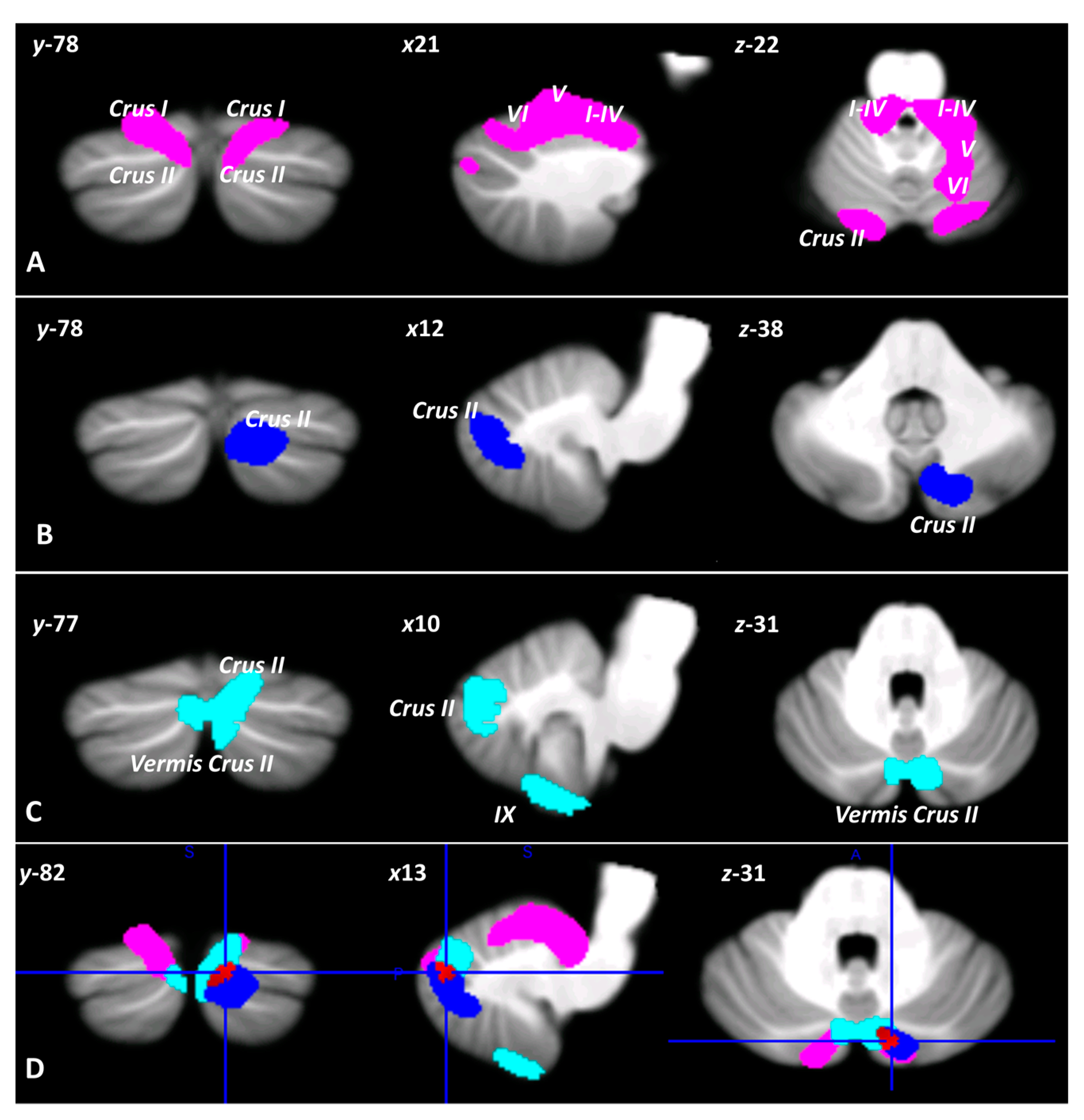
3.2. Voxel-Based Morphometry
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sapey-Triomphe, L.A.; Temmerman, J.; Puts, N.A.J.; Wagemans, J. Prediction Learning in Adults with Autism and Its Molecular Correlates. Mol. Autism 2021, 12, 64. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.C.; Brüne, M. The Role of Prediction in Social Neuroscience. Front. Hum. Neurosci. 2012, 6, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baillieux, H.; de Smet, H.J.; Paquier, P.F.; de Deyn, P.P.; Mariën, P. Cerebellar Neurocognition: Insights into the Bottom of the Brain. Clin. Neurol. Neurosurg. 2008, 110, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Buckner, R.L. The Cerebellum and Cognitive Function: 25 Years of Insight from Anatomy and Neuroimaging. Neuron 2013, 80, 807–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, S.; Nie, J.; Zhang, J.; Chen, C.; Wang, X.; Liu, Y.; Mo, Y.; Du, B.; Hu, Y.; Tian, Y.; et al. The Cerebellum Is Related to Cognitive Dysfunction in White Matter Hyperintensities. Front. Aging Neurosci. 2021, 13, 670463. [Google Scholar] [CrossRef] [PubMed]
- D’Mello, A.M.; Crocetti, D.; Mostofsky, S.H.; Stoodley, C.J. Cerebellar Gray Matter and Lobular Volumes Correlate with Core Autism Symptoms. NeuroImage Clin. 2015, 7, 631–639. [Google Scholar] [CrossRef] [Green Version]
- Frosch, I.R.; Mittal, V.A.; D’Mello, A.M. Cerebellar Contributions to Social Cognition in ASD: A Predictive Processing Framework. Front. Integr. Neurosci. 2022, 16, 810425. [Google Scholar] [CrossRef]
- Rapoport, M.; van Reekum, R.; Mayberg, H. The Role of the Cerebellum in Cognition and Behavior: A Selective Review. J. Neuropsychiatry Clin. Neurosci. 2000, 12, 193–198. [Google Scholar] [CrossRef]
- Sokolov, A.A. The Cerebellum in Social Cognition. Front. Cell Neurosci. 2018, 12, 145. [Google Scholar] [CrossRef] [Green Version]
- Sokolov, A.A.; Miall, R.C.; Ivry, R.B. The Cerebellum: Adaptive Prediction for Movement and Cognition. Trends Cogn. Sci. 2017, 21, 313–332. [Google Scholar] [CrossRef]
- Tamaš, O.; Kostić, M.; Kačar, A.; Stefanova, E.; Ðokić, B.S.; Stanisavljević, D.; Milovanović, A.; Ðorđević, M.; Glumbić, N.; Dragašević-Mišković, N. Social Cognition in Patients With Cerebellar Neurodegenerative Disorders. Front. Syst. Neurosci. 2021, 15, 664223. [Google Scholar] [CrossRef] [PubMed]
- Urgesi, C.; Butti, N.; Finisguerra, A.; Biffi, E.; Valente, E.M.; Romaniello, R.; Borgatti, R. Social Prediction in Pediatric Patients with Congenital, Non-Progressive Malformations of the Cerebellum: From Deficits in Predicting Movements to Rehabilitation in Virtual Reality. Cortex 2021, 144, 82–98. [Google Scholar] [CrossRef] [PubMed]
- van Overwalle, F.; Pu, M.; Ma, Q.; Li, M.; Haihambo, N.; Baetens, K.; Deroost, N.; Baeken, C.; Heleven, E. The Involvement of the Posterior Cerebellum in Reconstructing and Predicting Social Action Sequences. Cerebellum 2022, 21, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Ito, M. Cerebellar Circuitry as a Neuronal Machine. Prog. Neurobiol. 2006, 78, 272–303. [Google Scholar] [CrossRef] [PubMed]
- Ito, M. Control of Mental Activities by Internal Models in the Cerebellum. Nat. Rev. Neurosci. 2008, 9, 304–316. [Google Scholar] [CrossRef]
- Ramnani, N. The Primate Cortico-Cerebellar System: Anatomy and Function. Nat. Rev. Neurosci. 2006, 7, 511–522. [Google Scholar] [CrossRef]
- Miall, R.C.; Reckess, G.Z. The Cerebellum and the Timing of Coordinated Eye and Hand Tracking. Brain Cogn. 2002, 48, 212–226. [Google Scholar] [CrossRef] [Green Version]
- Leiner, H.C.; Leiner, A.L.; Dow, R.S. Does the Cerebellum Contribute to Mental Skills? Behav. Neurosci. 1986, 100, 443–454. [Google Scholar] [CrossRef]
- Clausi, S.; Olivito, G.; Lupo, M.; Siciliano, L.; Bozzali, M.; Leggio, M. The Cerebellar Predictions for Social Interactions: Theory of Mind Abilities in Patients with Degenerative Cerebellar Atrophy. Front. Cell Neurosci. 2019, 12, 510. [Google Scholar] [CrossRef]
- Heleven, E.; van Dun, K.; van Overwalle, F. The Posterior Cerebellum Is Involved in Constructing Social Action Sequences: An FMRI Study. Sci. Rep. 2019, 9, 11110. [Google Scholar] [CrossRef]
- Ploghaus, A.; Tracey, I.; Clare, S.; Gati, J.S.; Nicholas Rawlins, J.P.; Matthews, P.M. Learning about Pain: The Neural Substrate of the Prediction Error for Aversive Events. Proc. Natl. Acad. Sci. USA 2000, 97, 9281–9286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthoz, S.; Armony, J.L.; Blair, R.J.R.; Dolan, R.J. An FMRI Study of Intentional and Unintentional (Embarrassing) Violations of Social Norms. Brain 2002, 125, 1696–1708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szpunar, K.K.; Watson, J.M.; McDermott, K.B. Neural Substrates of Envisioning the Future. Proc. Natl. Acad. Sci. USA 2007, 104, 642–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckner, R.L.; Krienen, F.M.; Castellanos, A.; Diaz, J.C.; Thomas Yeo, B.T. The Organization of the Human Cerebellum Estimated by Intrinsic Functional Connectivity. J. Neurophysiol. 2011, 106, 2322–2345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krienen, F.M.; Buckner, R.L. Segregated Fronto-Cerebellar Circuits Revealed by Intrinsic Functional Connectivity. Cereb. Cortex 2009, 19, 2485–2497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivito, G.; Siciliano, L.; Clausi, S.; Lupo, M.; Romano, S.; Masciullo, M.; Molinari, M.; Cercignani, M.; Bozzali, M.; Leggio, M. Functional Changes of Mentalizing Network in SCA2 Patients: Novel Insights into Understanding the Social Cerebellum. Cerebellum 2020, 19, 235–242. [Google Scholar] [CrossRef]
- Schmahmann, J.D.; Pandyaf, D.N. The Cerebrocerebellar System. Int. Rev. Neurobiol. 1997, 41, 31–38. [Google Scholar] [CrossRef]
- van Overwalle, F.; D’aes, T.; Mariën, P. Social Cognition and the Cerebellum: A Meta-Analytic Connectivity Analysis. Hum. Brain Mapp. 2015, 36, 5137–5154. [Google Scholar] [CrossRef]
- van Overwalle, F.; Mariën, P. Functional Connectivity between the Cerebrum and Cerebellum in Social Cognition: A Multi-Study Analysis. Neuroimage 2016, 124, 248–255. [Google Scholar] [CrossRef]
- Clausi, S.; Olivito, G.; Siciliano, L.; Lupo, M.; Laghi, F.; Baiocco, R.; Leggio, M. The Cerebellum Is Linked to Theory of Mind Alterations in Autism. A Direct Clinical and MRI Comparison between Individuals with Autism and Cerebellar Neurodegenerative Pathologies. Autism Res. 2021, 14, 2300–2313. [Google Scholar] [CrossRef]
- D’Agata, F.; Caroppo, P.; Baudino, B.; Caglio, M.; Croce, M.; Bergui, M.; Tamietto, M.; Mortara, P.; Orsi, L. The Recognition of Facial Emotions in Spinocerebellar Ataxia Patients. Cerebellum 2011, 10, 600–610. [Google Scholar] [CrossRef]
- Hoche, F.; Guell, X.; Sherman, J.C.; Vangel, M.G.; Schmahmann, J.D. 139th Annual Meeting American Neurological Association. Ann. Neurol. 2014, 76, S1–S151. [Google Scholar] [CrossRef]
- Schmahmann, J.D. Dysmetria of Thought: Clinical Consequences of Cerebellar Dysfunction on Cognition and Affect. Trends Cogn. Sci. 1998, 2, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Schmahmann, J.D. Disorders of the Cerebellum: Ataxia, Dysmetria of Thought, and the Cerebellar Cognitive Affective Syndrome. J. Neuropsychiatr. 2004, 16, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Sokolovsky, N.; Cook, A.; Hunt, H.; Giunti, P.; Cipolotti, L. A Preliminary Characterisation of Cognition and Social Cognition in Spinocerebellar Ataxia Types 2, 1, and 7. Behav. Neurol. 2010, 23, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Gerschcovich, E.R.; Cerquetti, D.; Tenca, E.; Leiguarda, R. The Impact of Bilateral Cerebellar Damage on Theory of Mind, Empathy and Decision Making. Neurocase 2011, 17, 270–275. [Google Scholar] [CrossRef]
- Clausi, S.; Olivito, G.; Siciliano, L.; Lupo, M.; Bozzali, M.; Masciullo, M.; Molinari, M.; Romano, S.; Leggio, M. The Neurobiological Underpinning of the Social Cognition Impairments in Patients with Spinocerebellar Ataxia Type 2. Cortex 2021, 138, 101–112. [Google Scholar] [CrossRef]
- Becker, E.B.E.; Stoodley, C.J. Autism Spectrum Disorder and the Cerebellum, 1st ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2013; Volume 113, ISBN 9780124187009. [Google Scholar]
- Bora, E.; Bartholomeusz, C.; Pantelis, C. Meta-Analysis of Theory of Mind (ToM) Impairment in Bipolar Disorder. Psychol. Med. 2016, 46, 253–264. [Google Scholar] [CrossRef] [Green Version]
- Bora, E.; Berk, M. Theory of Mind in Major Depressive Disorder: A Meta-Analysis. J. Affect. Disord. 2016, 191, 49–55. [Google Scholar] [CrossRef]
- Fatemi, S.H. Cerebellar Pathology in Autism. In Essentials of Cerebellum and Cerebellar Disorders: A Primer for Graduate Students; Springer: Cham, Switzerland, 2016; Volume 11, pp. 539–543. [Google Scholar] [CrossRef]
- Kim, D.J.; Kent, J.S.; Bolbecker, A.R.; Sporns, O.; Cheng, H.; Newman, S.D.; Puce, A.; O’Donnell, B.F.; Hetrick, W.P. Disrupted Modular Architecture of Cerebellum in Schizophrenia: A Graph Theoretic Analysis. Schizophr. Bull. 2014, 40, 1216–1226. [Google Scholar] [CrossRef] [Green Version]
- Olivito, G.; Lupo, M.; Gragnani, A.; Saettoni, M.; Siciliano, L.; Pancheri, C.; Panfili, M.; Cercignani, M.; Bozzali, M.; Chiaie, R.D.; et al. Aberrant Cerebello-Cerebral Connectivity in Remitted Bipolar Patients 1 and 2: New Insight into Understanding the Cerebellar Role in Mania and Hypomania. Cerebellum 2022, 21, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Olivito, G.; Lupo, M.; Siciliano, L.; Gragnani, A.; Saettoni, M.; Pancheri, C.; Panfili, M.; Pignatelli, F.; Delle Chiaie, R.; Leggio, M. Theory of Mind Profile and Cerebellar Alterations in Remitted Bipolar Disorder 1 and 2: A Comparison Study. Front. Behav. Neurosci. 2022, 16, 366. [Google Scholar] [CrossRef] [PubMed]
- Cannon, J.; O’Brien, A.M.; Bungert, L.; Sinha, P. Prediction in Autism Spectrum Disorder: A Systematic Review of Empirical Evidence. Autism Res. 2021, 14, 604–630. [Google Scholar] [CrossRef] [PubMed]
- Ellis Weismer, S.; Saffran, J.R. Differences in Prediction May Underlie Language Disorder in Autism. Front. Psychol. 2022, 13, 897187. [Google Scholar] [CrossRef] [PubMed]
- Scholten, I.; Hartman, C.A.; Hendriks, P. Prediction Impairment May Explain Communication Difficulties in Autism. Front Psychol 2021, 12, 734024. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Kjelgaard, M.M.; Gandhi, T.K.; Tsourides, K.; Cardinaux, A.L.; Pantazis, D.; Diamond, S.P.; Held, R.M. Autism as a Disorder of Prediction. Proc. Natl. Acad. Sci. USA 2014, 111, 15220–15225. [Google Scholar] [CrossRef] [Green Version]
- van de Cruys, S.; Evers, K.; van der Hallen, R.; van Eylen, L.; Boets, B.; de-Wit, L.; Wagemans, J. Precise Minds in Uncertain Worlds: Predictive Coding in Autism. Psychol. Rev. 2014, 121, 649–675. [Google Scholar] [CrossRef] [Green Version]
- Olivito, G.; Lupo, M.; Laghi, F.; Clausi, S.; Baiocco, R.; Cercignani, M.; Bozzali, M.; Leggio, M. Lobular Patterns of Cerebellar Resting-State Connectivity in Adults with Autism Spectrum Disorder. Eur. J. Neurosci. 2018, 47, 729–735. [Google Scholar] [CrossRef] [PubMed]
- D’Mello, A.M.; Stoodley, C.J. Cerebro-Cerebellar Circuits in Autism Spectrum Disorder. Front. Neurosci. 2015, 9, 408. [Google Scholar] [CrossRef]
- Schmahmann, J.D.; Weilburg, J.B.; Sherman, J.C. The Neuropsychiatry of the Cerebellum - Insights from the Clinic. Cerebellum 2007, 6, 254–267. [Google Scholar] [CrossRef]
- Adamaszek, M.; D’Agata, F.; Ferrucci, R.; Habas, C.; Keulen, S.; Kirkby, K.C.; Leggio, M.; Mariën, P.; Molinari, M.; Moulton, E.; et al. Consensus Paper: Cerebellum and Emotion. Cerebellum 2017, 16, 552–576. [Google Scholar] [CrossRef] [PubMed]
- Moberget, T.; Ivry, R.B. Prediction, Psychosis, and the Cerebellum. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2019, 4, 820–831. [Google Scholar] [CrossRef] [PubMed]
- Merikangas, K.R.; Akiskal, H.S.; Angst, J.; Greenberg, P.E.; Hirschfeld, R.M.A.; Petukhova, M.; Kessler, R.C. Lifetime and 12-Month Prevalence of Bipolar Spectrum Disorder in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2007, 64, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Prieto, M.L.; Bobo, W.V.; Roger, V.L.; Bellivier, F.; West, C.P.; Frye, M.A.; Clinic, M.; Clinic, M.; Clinic, M.; Clinic, M.; et al. Risk of myocardial infarction and stroke in bipolar disorder: A systematic review and exploratory meta-analysis. Acta Psychiatr. Scand. 2014, 130, 342–353. [Google Scholar] [CrossRef] [Green Version]
- Bora, E.; Vahip, S.; Gonul, A.S.; Akdeniz, F.; Alkan, M.; Ogut, M.; Eryavuz, A. Evidence for Theory of Mind Deficits in Euthymic Patients with Bipolar Disorder. Acta Psychiatr. Scand. 2005, 112, 110–116. [Google Scholar] [CrossRef]
- Inoue, Y.; Tonooka, Y.; Yamada, K.; Kanba, S. Deficiency of Theory of Mind in Patients with Remitted Mood Disorder. J. Affect. Disord. 2004, 82, 403–409. [Google Scholar] [CrossRef]
- Lahera, G.; Montes, J.M.; Benito, A.; Valdivia, M.; Medina, E.; Mirapeix, I.; Sáiz-Ruiz, J. Theory of Mind Deficit in Bipolar Disorder: Is It Related to Aprevious History of Psychotic Symptoms? Psychiatry Res. 2008, 161, 309–317. [Google Scholar] [CrossRef]
- Olley, A.L.; Malhi, G.S.; Bachelor, J.; Cahill, C.M.; Mitchell, P.B.; Berk, M. Executive Functioning and Theory of Mind in Euthymic Bipolar Disorder. Bipolar Disord. 2005, 7, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Chen, G.; Jia, Y.; Gong, J.Y.; Qiu, S.; Zhong, S.; Zhao, L.; Chen, F.; Lai, S.; Qi, Z.; et al. Disrupted Cerebellar Connectivity With the Central Executive Network and the Default-Mode Network in Unmedicated Bipolar II Disorder. Front. Psychiatry 2018, 9, 705. [Google Scholar] [CrossRef]
- Lupo, M.; Olivito, G.; Gragnani, A.; Saettoni, M.; Siciliano, L.; Pancheri, C.; Panfili, M.; Bozzali, M.; Delle Chiaie, R.; Leggio, M. Comparison of Cerebellar Grey Matter Alterations in Bipolar and Cerebellar Patients: Evidence from Voxel-Based Analysis. Int. J. Mol. Sci. 2021, 22, 3511. [Google Scholar] [CrossRef] [PubMed]
- Baldaçara, L.; Guilherme, J.; Borgio, F.; Luiz, A.; de Lacerda, T.; Jackowski, A.P. Cerebellum and Psychiatric Disorders O Cerebelo e Os Transtornos Psiquiátricos. Braz. J. Psychiatry 2008, 30, 281–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delbello, M.P.; Strakowski, S.M.; Zimmerman, M.E.; Hawkins, J.M.; Sax, K.W. MRI Analysis of the Cerebellum in Bipolar Disorder: A Pilot Study. Neuropsychopharmacology 1999, 21, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Cho, H.B.; Dager, S.R.; Yurgelun-Todd, D.A.; Yoon, S.; Lee, J.H.; Lee, S.H.; Lee, S.; Renshaw, P.F.; Lyoo, I.K. Posterior Cerebellar Vermal Deficits in Bipolar Disorder. J. Affect. Disord. 2013, 150, 499–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mills, N.P.; Melissa DelBello, B.P.; Adler, C.M.; Strakowski, S.M. MRI Analysis of Cerebellar Vermal Abnormalities in Bipolar Disorder. Am. J. Psychiatry 2005, 162, 1530–1533. [Google Scholar] [CrossRef]
- Skokauskas, N.; Frodl, T. Overlap between Autism Spectrum Disorder and Bipolar Affective Disorder. Psychopathology 2015, 48, 209–216. [Google Scholar] [CrossRef]
- Schwarz, K.; Moessnang, C.; Schweiger, J.I.; Baumeister, S.; Plichta, M.M.; Brandeis, D.; Banaschewski, T.; Wackerhagen, C.; Erk, S.; Walter, H.; et al. Transdiagnostic Prediction of Affective, Cognitive, and Social Function Through Brain Reward Anticipation in Schizophrenia, Bipolar Disorder, Major Depression, and Autism Spectrum Diagnoses. Schizophr. Bull. 2020, 46, 592–602. [Google Scholar] [CrossRef]
- Cross-Disorder Group of the Psychiatric Genomics Consortium Identification of Risk Loci with Shared Effects on Five Major Psychiatric Disorders: A Genome-Wide Analysis. Lancet 2013, 381, 1371–1379. [CrossRef]
- Gandal, M.J.; Haney, J.R.; Parikshak, N.N.; Leppa, V.; Ramaswami, G.; Hartl, C.; Schork, A.J.; Appadurai, V.; Buil, A.; Werge, T.M.; et al. Shared Molecular Neuropathology across Major Psychiatric Disorders Parallels Polygenic Overlap. Science 2018, 359, 693–697. [Google Scholar] [CrossRef] [Green Version]
- Stahlberg, O.; Soderstrom, H.; Rastam, M.; Gillberg, C. Bipolar Disorder, Schizophrenia, and Other Psychotic Disorders in Adults with Childhood Onset AD/HD and/or Autism Spectrum Disorders. J. Neural. Transm. 2004, 111, 891–902. [Google Scholar] [CrossRef]
- Varcin, K.J.; Herniman, S.E.; Lin, A.; Chen, Y.; Perry, Y.; Pugh, C.; Chisholm, K.; Whitehouse, A.J.O.; Wood, S.J. Occurrence of Psychosis and Bipolar Disorder in Adults with Autism: A Systematic Review and Meta-Analysis. Neurosci. Biobehav. Rev. 2022, 134, 104543. [Google Scholar] [CrossRef]
- Borue, X.; Mazefsky, C.; Rooks, B.T.; Strober, M.; Keller, M.B.; Hower, H.; Yen, S.; Gill, M.K.; Diler, R.S.; Axelson, D.A.; et al. Longitudinal Course of Bipolar Disorder in Youth With High- Functioning Autism Spectrum Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 1064–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, Y.L.; Wu, C.S.; Tsai, H.J. The Comorbidity of Schizophrenia Spectrum and Mood Disorders in Autism Spectrum Disorder. Autism Res. 2021, 14, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Carpita, B.; Bertelloni, C.A.; Diadema, E.; Barberi, F.M.; Gesi, C.; Carmassi, C. Subthreshold Autism Spectrum in Bipolar Disorder: Prevalence and Clinical Correlates. Psychiatry Res. 2019, 281, 112605. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.M.; Khan, N.; Sultana, A.; Ma, P.; McKyer, E.L.J.; Ahmed, H.U.; Purohit, N. Prevalence of Comorbid Psychiatric Disorders among People with Autism Spectrum Disorder: An Umbrella Review of Systematic Reviews and Meta-Analyses. Psychiatry Res. 2020, 287, 112922. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, J.; Kamio, Y.; Takahashi, H.; Ota, M.; Teraishi, T.; Hori, H.; Nagashima, A.; Takei, R.; Higuchi, T.; Motohashi, N.; et al. Autistic-like Traits in Adult Patients with Mood Disorders and Schizophrenia. PLoS ONE 2015, 10, e0122711. [Google Scholar] [CrossRef] [Green Version]
- Hannon, G.; Taylor, E.P. Suicidal Behaviour in Adolescents and Young Adults with ASD: Findings from a Systematic Review. Clin. Psychol. Rev. 2013, 33, 1197–1204. [Google Scholar] [CrossRef] [Green Version]
- Sterling, L.; Dawson, G.; Estes, A.; Greenson, J. Characteristics Associated with Presence of Depressive Symptoms in Adults with Autism Spectrum Disorder. J. Autism Dev. Disord. 2008, 38, 1011–1018. [Google Scholar] [CrossRef]
- Clausi, S.; Lupo, M.; Olivito, G.; Siciliano, L.; Contento, M.P.; Aloise, F.; Pizzamiglio, L.; Molinari, M.; Leggio, M. Depression Disorder in Patients with Cerebellar Damage: Awareness of the Mood State. J. Affect. Disord. 2019, 245, 386–393. [Google Scholar] [CrossRef]
- Lupo, M.; Siciliano, L.; Leggio, M. From Cerebellar Alterations to Mood Disorders: A Systematic Review. Neurosci. Biobehav. Rev. 2019, 103, 21–28. [Google Scholar] [CrossRef]
- Romer, A.L.; Knodt, A.R.; Houts, R.; Brigidi, B.D.; Moffitt, T.E.; Caspi, A.; Hariri, A.R. Structural Alterations within Cerebellar Circuitry Are Associated with General Liability for Common Mental Disorders. Mol. Psychiatry 2018, 23, 1084–1090. [Google Scholar] [CrossRef] [Green Version]
- Siciliano, L.; Olivito, G.; Leggio, M. The Cerebellum Gains Weight: A Systematic Review of Alterations in Cerebellar Volume and Cerebro-Cerebellar Functional Alterations in Individuals with Eating Disorders. Neurosci. Biobehav. Rev. 2022, 141, 104863. [Google Scholar] [CrossRef] [PubMed]
- APA American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. SCID-5-CV. Intervista Clinica Strutturata per i Disturbi Del DSM-5, Versione per Il Clinico; Andrea Fossati e Serena Borroni, Ed.; Italiana; Raffaello Cortina Editore: Milano, Itlay, 2017. [Google Scholar]
- Hamilton, M. Development of a Rating Scale for Primary Depressive Illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–896. [Google Scholar] [CrossRef] [PubMed]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A Rating Scale for Mania: Reliability, Validity and Sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Raven, J.C. Progressive Matrices. Sets A, Ab, B: Board and Book Forms; Lewis: London, UK, 1949. [Google Scholar]
- Trouillas, P.; Takayanagi, T.; Hallett, M.; Currier, R.D.; Subramony, S.H.; Wessel, K.; Bryer, A.; Diener, H.C.; Massaquoi, S.; Gomez, C.M.; et al. International Cooperative Ataxia Rating Scale for pharmacological assessment of the cerebellar syndrome. J. Neurol. Sci. 1997, 145, 205–211. [Google Scholar] [CrossRef]
- Orsini, A.; Laicardi, C. Wais-r. Contributo Alla Taratura Italiana; Organizzazioni Speciali: Firenze, Italy, 1997. [Google Scholar]
- David, W. Wais-r. Wechsler Adult Intelligence Scale Revised; Psychological Corporation: New York, NY, USA, 1981. [Google Scholar]
- Ruta, L.; Mazzone, D.; Mazzone, L.; Wheelwright, S.; Baron-Cohen, S. The Autism-Spectrum Quotient - Italian Version: A Cross-Cultural Confirmation of the Broader Autism Phenotype. J. Autism Dev. Disord. 2012, 42, 625–633. [Google Scholar] [CrossRef]
- Blair, R.J.R.; Cipolotti, L. Impaired Social Response Reversal. A Case of “Acquired Sociopathy”. Brain 2000, 123, 1122–1141. [Google Scholar] [CrossRef] [Green Version]
- Prior, M.; Marchi, S.; Sartori, G. Cognizione Sociale e Comportamento. Vol. 1, Uno Strumento Per La Misurazione.; Upsel Domenghini Editore: Padova, Italy, 2003. [Google Scholar]
- Baron-Cohen, S.; Wheelwright, S.; Hill, J.; Raste, Y.; Plumb, I. The “Reading the Mind in the Eyes” Test Revised Version: A Study with Normal Adults, and Adults with Asperger Syndrome or High-Functioning Autism. J. Child Psychol. Psychiatry Allied Discip. 2001, 42, 241–251. [Google Scholar] [CrossRef]
- Serafin, M.; Surian, L. Il Test Degli Occhi: Uno Strumento per Valutare La “Teoria Della Mente”. Giornale Italiano di Psicologia 2004, 31, 839–862. [Google Scholar]
- Liverta Sempio, O.; Marchetti, A.; Lecciso, F. Faux Pas: Traduzione Italiana; Theory of Mind Research Unit; Department of Psychology, Catholic University of the Sacred Heart: Milan, Italy, 2005. [Google Scholar]
- Stone, V.E.; Baron-Cohen, S.; Knight, R.T. Frontal lobe contributions to theory of mind. J. Cogn. Neurosci. 1998, 10, 640–656. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Diedrichsen, J.; Balsters, J.H.; Flavell, J.; Cussans, E.; Ramnani, N. A Probabilistic MR Atlas of the Human Cerebellum. Neuroimage 2009, 46, 39–46. [Google Scholar] [CrossRef]
- Molinari, M.; Restuccia, D.; Leggio, M.G. State Estimation, Response Prediction, and Cerebellar Sensory Processing for Behavioral Control. Cerebellum 2009, 8, 399–402. [Google Scholar] [CrossRef] [PubMed]
- Kana, R.K.; Patriquin, M.A.; Black, B.S.; Channell, M.M.; Wicker, B. Altered Medial Frontal and Superior Temporal Response to Implicit Processing of Emotions in Autism. Autism Res. 2016, 9, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Lozier, L.M.; Vanmeter, J.W.; Marsh, A.A. Impairments in Facial Affect Recognition Associated with Autism Spectrum Disorders: A Meta-Analysis. Dev. Psychopathol. 2014, 26, 933–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siciliano, L.; Clausi, S. Implicit vs. Explicit Emotion Processing in Autism Spectrum Disorders: An Opinion on the Role of the Cerebellum. Front. Psychol. 2020, 11, 96. [Google Scholar] [CrossRef]
- Lartseva, A.; Dijkstra, T.; Buitelaar, J.K. Emotional Language Processing in Autism Spectrum Disorders: A Systematic Review. Front. Hum. Neurosci. 2015, 8, 991. [Google Scholar] [CrossRef]
- Klin, A.; Jones, W.; Schultz, R.T.; Volkmar, F.R. The Enactive Mind—from Actions to Cognition: Lessons from Autism. In Handbook of Autism and Pervasive Developmental Disorders; Volkmar, F.R., Paul, R., Klin, A., Cohen, D., Eds.; Wiley: Hoboken, NJ, USA, 2005. [Google Scholar]
- Saxe, R.; Carey, S.; Kanwisher, N. Understanding Other Minds: Linking Developmental Psychology and Functional Neuroimaging. Annu. Rev. Psychol. 2004, 55, 87–124. [Google Scholar] [CrossRef] [Green Version]
- Shamay-Tsoory, S.G.; Shur, S.; Barcai-Goodman, L.; Medlovich, S.; Harari, H.; Levkovitz, Y. Dissociation of Cognitive from Affective Components of Theory of Mind in Schizophrenia. Psychiatry Res. 2007, 149, 11–23. [Google Scholar] [CrossRef]
- van Overwalle, F.; van de Steen, F.; Mariën, P. Dynamic Causal Modeling of the Effective Connectivity between the Cerebrum and Cerebellum in Social Mentalizing across Five Studies. Cogn. Affect. Behav. Neurosci. 2019, 19, 211–223. [Google Scholar] [CrossRef] [Green Version]
- Keren-Happuch, E.; Chen, S.H.A.; Ho, M.H.R.; Desmond, J.E. A Meta-Analysis of Cerebellar Contributions to Higher Cognition from PET and FMRI Studies. Hum. Brain Mapp. 2014, 35, 593–615. [Google Scholar] [CrossRef] [Green Version]
- King, M.; Hernandez-castillo, C.R.; Poldrack, R.A.; Ivry, R.B.; Sciences, A. Functional boundaries in the human cerebellum revealed by a multi-domain task battery. Nat. Neurosci. 2021, 22, 1371–1378. [Google Scholar] [CrossRef]
- Cattaneo, Z.; Ferrari, C.; Ciricugno, A.; Heleven, E.; Schutter, D.J.L.G.; Manto, M.; van Overwalle, F. New Horizons on Non-Invasive Brain Stimulation of the Social and Affective Cerebellum. Cerebellum 2022, 21, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Pu, M.; Heleven, E.; Ma, Q.; Bylemans, T.; Baetens, K.; Haihambo, N.P.; Baeken, C.; Deroost, N.; van Overwalle, F. The Posterior Cerebellum and Social Action Sequences in a Cooperative Context. Cerebellum 2022. [Google Scholar] [CrossRef] [PubMed]
- Leggio, M.; Molinari, M. Cerebellar Sequencing: A Trick for Predicting the Future. Cerebellum 2015, 14, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, G. Cerebellar Motor Disorders. In Handbook of the Cerebellum and Cerebellar Disorders; Manto, M., Schmahmann, J.D., Rossi, F., Gruol, D.L., Koibuchi, N., Manto, M., Eds.; Springer: Dordrecht, The Netherlands, 2013. [Google Scholar]
- Kalbe, E.; Schlegel, M.; Sack, A.T.; Nowak, D.A.; Dafotakis, M.; Bangard, C.; Brand, M.; Shamay Tsoory, S.; Onur, O.A.; Kessler, J. Dissociating Cognitive from Affective Theory of Mind: A TMS Study. Cortex 2010, 46, 769–780. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, C.L.; McCrory, E.J.; Dadds, M.R.; Cecil, C.A.M.; Lockwood, P.L.; Hyde, Z.H.; de Brito, S.A.; Viding, E. Neural Responses to Fearful Eyes in Children with Conduct Problems and Varying Levels of Callous-Unemotional Traits. Psychol. Med. 2014, 44, 99–109. [Google Scholar] [CrossRef] [Green Version]
- Hiser, J.; Koenigs, M. The Multifaceted Role of the Ventromedial Prefrontal Cortex in Emotion, Decision Making, Social Cognition, and Psychopathology. Biol. Psychiatry 2018, 83, 638–647. [Google Scholar] [CrossRef]
- Narita, K.; Suda, M.; Takei, Y.; Aoyama, Y.; Majima, T.; Kameyama, M.; Kosaka, H.; Amanuma, M.; Fukuda, M.; Mikuni, M. Volume Reduction of Ventromedial Prefrontal Cortex in Bipolar II Patients with Rapid Cycling: A Voxel-Based Morphometric Study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 439–445. [Google Scholar] [CrossRef]
- Womer, F.Y.; Kalmar, J.H.; Wang, F.; Blumberg, H.P. A Ventral Prefrontal-Amygdala Neural System in Bipolar Disorder: A View from Neuroimaging Research. Acta Neuropsychiatr. 2009, 21, 228–238. [Google Scholar] [CrossRef] [Green Version]
- Allen, G.; McColl, R.; Barnard, H.; Ringe, W.K.; Fleckenstein, J.; Cullum, C.M. Magnetic Resonance Imaging of Cerebellar-Prefrontal and Cerebellar-Parietal Functional Connectivity. Neuroimage 2005, 28, 39–48. [Google Scholar] [CrossRef]
- Konarski, J.Z.; McIntyre, R.S.; Grupp, L.A.; Kennedy, S.H. Is the Cerebellum Relevant in the Circuitry of Neuropsychiatric Disorders? J. Psychiatry Neurosci. 2005, 30, 178–186. [Google Scholar]
- Leggio, M.G.; Chiricozzi, F.R.; Clausi, S.; Tedesco, A.M.; Molinari, M. The Neuropsychological Profile of Cerebellar Damage: The Sequencing Hypothesis. Cortex 2011, 47, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Moorhead, T.W.J.; McKirdy, J.; Sussmann, J.E.D.; Hall, J.; Lawrie, S.M.; Johnstone, E.C.; McIntosh, A.M. Progressive Gray Matter Loss in Patients with Bipolar Disorder. Biol. Psychiatry 2007, 62, 894–900. [Google Scholar] [CrossRef] [PubMed]
- Hafeman, D.M.; Chang, K.D.; Garrett, A.S.; Sanders, E.M.; Phillips, M.L. Effects of Medication on Neuroimaging Findings in Bipolar Disorder: An Updated Review. Bipolar. Disord. 2012, 14, 375–410. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Group | N | Sex F/M | Age Mean (SD) | Education Mean (SD) | Raven’s 47 Mean (SD) | IQ Mean (SD) | ICARS Mean (SD) | AQ Mean (SD) | HDRS Mean (SD) | YMRS Mean (SD) |
|---|---|---|---|---|---|---|---|---|---|---|
| CB | 32 | 17/15 | 46.71 (11.03) | 13.4 (3.45) | 29,29 (2,9) | 8662 (131) | 2626 (126) | - | - | - |
| ASD | 21 | 10/11 | 26.85 (8.66) | 13.76 (1.72) | - | 106.68 (20.7) | 2.46 (3.8) | 34.5 (9.9) | - | - |
| BD2 | 13 | 6/7 | 45.07 (11.22) | 14.53 (3.79) | 27.75 (7.75) | - | 1.08 (2.66) | - | 2.62 (3.23) | 1.77 (2.74) |
| HS-SC | 57 | 33/24 | 36.49 (13.15) | 13.78 (2.73) | 3120 (3.1) | 108.29 (10.8) | - | 16.3 (6.6) | - | - |
| Group | RMET | EA | “Faux Pas” Stories | “No-Faux Pas” Stories | Affective | Cognitive |
|---|---|---|---|---|---|---|
| CB | 21.77 (5.14) | 40.10 (6.00) | 38.77 (10.77) | 19.53 (0.73) | 6.30 (2.38) | 32.46 (8.81) |
| ASD | 21.14 (6.11) | 37.57 (8.98) | 39.33 (13.10) | 19.57 (0.98) | 5.71 (2.49) | 33.62 (10.99) |
| BD2 | 22.00 (5.40) | 43.10 (4.82) | 30.60 (13.55) | 19.60 (1.27) | 4.50 (2.64) | 26.10 (11.42) |
| HS-SC | 26.37 (3.19) | 43.86 (5.77) | 47.12 (9.57) | 19.19 (1.77) | 6.56 (2.08) | 40.56 (8.20) |
| Group | Size | Regions | Side | Coordinates (mm) | Peak Z-Scores | Peak-Level p Value (FWE) | ||
|---|---|---|---|---|---|---|---|---|
| x | y | z | ||||||
| CB | 17,013 | Lobule I–IV | L | −7 | −37 | −19 | 5.94 | 0.000 |
| Lobule I–IV | R | 12 | −37 | −22 | 5.82 | 0.000 | ||
| Lobule VI | R | 22 | −58 | −14 | 4.84 | 0.004 | ||
| 2731 | Crus-II | L | −12 | −86 | −29 | 4.88 | 0.003 | |
| Crus-I | L | −17 | −79 | −21 | 4.72 | 0.006 | ||
| ASD | 2702 | Crus-II | R | 12 | −76 | −39 | 4.28 | 0.026 |
| BD2 | 2972 | Lobule IX | R | 3 | −47 | −60 | 4.26 | 0.007 |
| Crus-II | R | 4 | −61 | −54 | 4.52 | 0.012 | ||
| 3148 | Crus-II | R | 6 | −79 | −34 | 4.23 | 0.008 | |
| Group | Size | Regions | Side | Coordinates (mm) | Peak Z-Scores | Peak-Level p Value (FWE) | ||
|---|---|---|---|---|---|---|---|---|
| x | y | z | ||||||
| CB < ASD | 2131 | Lobule VI | R | 24 | −59 | −27 | 4.64 | 0.002 |
| Loule V | R | 17 | −50 | −22 | 4.22 | 0.013 | ||
| Lobule I–IV | R | 12 | −38 | −22 | 4.18 | 0.015 | ||
| 1332 | Lobule VI | L | −26 | −52 | −25 | 4.51 | 0.004 | |
| L | −14 | −57 | −23 | 4.08 | 0.021 | |||
| CB < BD2 | 26,163 | VIIIb | R | 20 | −53 | −45 | 6.42 | 0.000 |
| Lobule VI | L | −21 | −52 | −24 | 5.61 | 0.000 | ||
| Lobule V | R | 18 | −48 | −23 | 5–60 | 0.000 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olivito, G.; Siciliano, L.; Clausi, S.; Lupo, M.; Baiocco, R.; Gragnani, A.; Saettoni, M.; Delle Chiaie, R.; Laghi, F.; Leggio, M. The Cerebellum Gets Social: Evidence from an Exploratory Study of Cerebellar, Neurodevelopmental, and Psychiatric Disorders. Biomedicines 2023, 11, 309. https://doi.org/10.3390/biomedicines11020309
Olivito G, Siciliano L, Clausi S, Lupo M, Baiocco R, Gragnani A, Saettoni M, Delle Chiaie R, Laghi F, Leggio M. The Cerebellum Gets Social: Evidence from an Exploratory Study of Cerebellar, Neurodevelopmental, and Psychiatric Disorders. Biomedicines. 2023; 11(2):309. https://doi.org/10.3390/biomedicines11020309
Chicago/Turabian StyleOlivito, Giusy, Libera Siciliano, Silvia Clausi, Michela Lupo, Roberto Baiocco, Andrea Gragnani, Marco Saettoni, Roberto Delle Chiaie, Fiorenzo Laghi, and Maria Leggio. 2023. "The Cerebellum Gets Social: Evidence from an Exploratory Study of Cerebellar, Neurodevelopmental, and Psychiatric Disorders" Biomedicines 11, no. 2: 309. https://doi.org/10.3390/biomedicines11020309
APA StyleOlivito, G., Siciliano, L., Clausi, S., Lupo, M., Baiocco, R., Gragnani, A., Saettoni, M., Delle Chiaie, R., Laghi, F., & Leggio, M. (2023). The Cerebellum Gets Social: Evidence from an Exploratory Study of Cerebellar, Neurodevelopmental, and Psychiatric Disorders. Biomedicines, 11(2), 309. https://doi.org/10.3390/biomedicines11020309